
Abstract
Private and public social services, including social work centers, are limited to disadvantaged Vietnamese people, such as orphans and people with HIV/AIDS. Buddhism-based organizations (BBOs) have been acknowledged as an avenue to extend social services in Vietnam. This article reviews the social service system and BBOs in Vietnam using secondary data and findings from an empirical study on Buddhist charitable giving. A proposed model linking BBOs to social work centers seeks to improve the efficacy and effectiveness of service delivery.
Introduction
The Vietnamese government has identified various social problems, such as poverty, vulnerable children and older adults without family assistance, and so on, and sought to create an accessible and resilient social welfare system (Hugman et al., 2007). Recently, the social welfare system, which has long depended on the public sector, was expanded through private social work centers (Ministry of Labour, Invalids and Social Affairs [MOLISA], 2015a). Yet both public and private social services have limited resources to meet the needs of vulnerable populations (ILSSA and GIZ, 2013). Social work centers are new and unfamiliar to most Vietnamese citizens. Faith-based organizations become a more accessible and affordable solution to underserved populations.
In Vietnam, Buddhism-based organizations (BBOs) serve as the most common alternative social services in the community (Tu, 2017). Buddhism has a more than 2000 year-old tradition in Vietnam (Nguyen and Doan, 2015; Thich, 2016), and currently it is estimated that 54.6 million Vietnamese people identify with this religious tradition (Thich, 2016). Buddhism is acknowledged as the most influential religion in Vietnam, which impacts individual help-seeking behaviors and almsgiving (Nguyen, 1985). BBOs have provided shelter, food, clothes, medical care, and basic education for orphans, children with disabilities, older adults without family care, people with HIV/AIDS, and others. The budget for these services comes from community-based charitable donations. A cultural barrier to the extension of services is long-held stigma concerning distrust toward public and private philanthropic organizations (Center for Community Development, 2012; The Asia Foundation [TAF] and Vietnam Asia Pacific Economic Center [VAPEC], 2011). Faith-based organizations, especially BBOs, therefore became alternative recipients of almsgiving. Empirical studies show that the amount of almsgiving targeting faith-based organizations was much higher than charitable and philanthropic organizations run by the government (TAF and VAPEC, 2011).
It is worth mentioning that a majority of the current staff working in the Vietnamese welfare system, especially in faith-based organizations including BBOs, do not have social work backgrounds. According to MOLISA (2010), only 23.4 percent of social welfare system workers held a Bachelor’s degree, while 19.45 percent of practitioners held lower degrees, such as high school or a 2-year degree (Nguyen and Bui, 2012: 4). These numbers are surprising, given social work was reintroduced to Vietnam more than two decades ago (Hugman et al., 2007; Nguyen, 2015a; Nguyen, 2002, 2010; (Nguyen and Bui, 2012: 4); United Nations Children’s Fund [UNICEF], 2005: 15).
Social work was approved by the Vietnamese government as a training degree within the higher education system in 2004 (Ministry of Education and Training [MOET], 2004). Most social work schools in Vietnam adopted the curriculum and syllabus from Western countries, such as the United States, the United Kingdom, Australia, and so on (Hugman et al., 2007). In 2010, the Vietnamese government approved a national plan on social work professional development for the period of 2011–2020 (Decree 32) which aimed to train 35,000 new social workers and provide in-service training to 25,000 practitioners (The Vietnamese Government, 2010). After 5 years, there were 55 undergraduate social work, 21 vocational social work, and 3 graduate social work programs. In total, 13,391 students received social work training at different levels (Nguyen, 2017). With this rapid growth, social workers were expected to lead the workforce of all sectors of the social welfare system, including BBOs.
Acknowledging the limitations of both public and private sectors in providing accessible and affordable social services for vulnerable and disadvantaged groups, as well as the contribution of BBOs and the participation of the new social work labor force to those services, Vietnamese scholars explored ways to incorporate Buddhism into social work (Hoang, 2012; Nguyen, 2012; Nguyen et al., 2012). However, few studies discuss how to engage stakeholders. In order to address this knowledge gap, we first review the current state of social services in Vietnam. Second, we review Buddhism-based charity and philanthropy in the Vietnamese social welfare system. Third, we propose a model of linking BBOs to social work centers in the Vietnamese context with a discussion on its rationale and collaboration mechanism.
In order to support our argument, we used different literature and data sources. The primary sources are from the literature on the Vietnamese social welfare system. In addition, findings from our empirical study (project NAFOSTED VIII1.1-2012.05) on Buddhist ethics and entrepreneurship of Vietnamese urban people in the market economy will be used to support the argument on the willingness of Vietnamese Buddhists to participate in almsgiving. Last but not least, we review the database of the Vietnam Buddhist Sangha (VBS) to acquire an overview of the foundation of the VBS and the results of its charitable and philanthropic programs.
Current situations of social services in Vietnam
Prior to 1989, only public educational and medical services were available in Vietnam. The financial constraints of the 1980s, however, led to the decentralization of these systems. The Vietnamese government called for the participation of the private sector in the social welfare system while maintaining its primary role in orienting and managing the systems (Vietnamese government, n.d.). After entering the market economy in 1986, the socioeconomic position of citizens significantly changed. In 2009, Vietnam reached the goal of becoming one of the average-income countries (United Nations Development Programme [UNDP], 2011: 24). Along with economic gains, the social welfare system is experiencing many changes, including a greater role of the private and faith-based sectors (MOLISA, 2015b).
Public social services
For a long time, the Vietnamese government played a dominant role in regulating the social welfare system in Vietnam. The Vietnamese government developed the social welfare system based on risk management and basic social service delivery through four main social policy sectors. These include (1) vocational policies aiming for a minimum income and poverty reduction, (2) social security policy, (3) social assistance policies, and (4) basic social service policies (UNDP, 2011). Regarding the social assistance system, there are different types of social welfare programs targeting children with special needs, older adults, people with disabilities, people with mental disorders, as well as general social welfare centers and social work centers (MOLISA, 2015b).
In the public sector, the social work center is a new type of social service center. Social work centers are district-level centers that provide professional services, such as counseling, interventions, and other social work services, for different clients. Potential clients are older adults; people with disabilities, mental disorders, or HIV/AIDS; those suffering from poverty or substance abuse; caregivers, and so on (MOLISA and Ministry of Home Affairs [MOHA], 2013). Up to 2014, there have been 30 major cities or provinces establishing social work centers at the district level (MOLISA, 2014).
Despite efforts and changes in the social welfare system, in general, public services are limited, especially in the educational and medical areas (ILSSA and GIZ, 2013: 42). Limited health literacy and significant health disparities are acknowledged across regions and geographic areas. Vulnerable populations, such as those with low-income, ethnic minorities, and people with disabilities, confront challenges in accessing necessary health care and educational services due to geographical isolation, limited transportation, unavailability or unaffordability of services, and discrimination (UNDP, 2011: 78). For example, in 2008, only 34 percent of Vietnamese people could access basic health care services. In 2006, only 40 percent of ethnic minority children, compared to 61 percent of Kinh or Hoa children – the major ethnicities in Vietnam, could access kindergarten services (UNDP, 2011). A similar situation is acknowledged among migrant workers, as 99 percent of them have no social insurance and are at high risk of sickness, unemployment, and so on (Oxfam, 2015). Although the government has established new social work centers since 2013, there has not been a systematic evaluation of these centers in the social welfare system.
Private social services
Since the Vietnamese government has implemented policies that encourage the participation of private services in the social welfare system, there have been an increasing number of private agencies providing educational and medical services (UNDP, 2011). Some private agencies provide basic services for those with special needs, such as children with autism, older adults, and people with disabilities (MOLISA, 2015b). As an emerging sector in the social welfare system, private services have some limitations. First, private social services have been developed only since 1986. Limited experience challenges service organizers in developing culturally competent services. Second, private services, particularly in educational and medical areas, mostly target stable- and high-income middle-class residents. Those services are mostly provided in highly urbanized areas with high fees to maximize their profits. In other words, private services are out of reach of low-income and vulnerable populations. Third, the mechanism to manage, regulate, and evaluate service delivery and quality appears to be missing in the private sector (UNDP, 2011). That said, clients’ rights are not fully protected when they use private services.
Faith-based social services
Addressing the limitations of both public and private sectors in providing necessary social services for those in need, in 2013, the Vietnamese government issued the governmental decree 693/QD-TTg on tax and fee reduction and credit benefits for faith-based organizations which provide services for underserved populations. Of the 413 social service agencies nationwide, 218 of them are non-public agencies. Half of these non-public agencies are run by faith-based organizations and accredited by the Vietnamese government. In addition, approximately 50 unaccredited faith-based organizations have been providing care for at least 10 clients (MOLISA, 2017). Approximately, each year, faith-based organizations with an estimated 2600 employees provide services for 11,800 clients, accounting for one-third of the total people in need across the country. Their services include (1) direct care for vulnerable subjects identified in the social welfare law, such as children with specific needs, older adults without family care, and so on; (2) rehabilitation, vocational therapy, training, and orientation; (3) social work services; and (4) community reintegration (MOLISA, 2017). In short, since the public sector has exposed numerous limitations, non-public services, particularly faith-based organizations, have participated more actively in the Vietnamese welfare system.
Buddhism-based charity and philanthropy in the Vietnamese social welfare system
In situations where accessible and affordable public or private social services are hard to reach, faith-based organizations become a solution for underserved populations. Buddhism is acknowledged as the most influential religion in the country; BBOs are considered a major source of alternative social services in the community (Tu, 2017). Major strengths of BBOs in Vietnamese social welfare are having strong community connections, great fundraising capacity, and open access to vulnerable populations. In the following sections we examine Vietnamese Buddhists and their practice of giving to charity and philanthropy and charitable and philanthropic activities of BBOs.
Vietnamese Buddhists and their practice of giving to charity and philanthropy
The fundraising capacity of BBOs largely depends on Buddhists’ intention of giving. According to ancient Buddhist scriptures (sutras), ‘giving’ (Dana in Pali) is an important practice of Buddhists. Giving consists of two primary forms, including material giving (amisa-dana), such as money and goods donation, and Buddhist doctrine giving, or sharing of Buddha’s teaching (Dhamma-dana) (Thich, n.d.). Buddhists believe that constant giving will bring unlimited rewards to givers (Hue Quang Center for Sino-Nom Translation, 2013). Between material giving and Dharma giving, material giving is likely the easiest form to practice. In Vietnamese society, contributing to charity and philanthropic activities (material giving) is seen as a practice of not only Buddha’s teaching but also social responsibility (Nguyen, 2013).
Recent studies show that the practice of giving among Vietnamese citizens is significant. TAF and VAPEC (2011) report that 87 and 59 percent of the household representatives in rural and urban areas, respectively, are interested in some form of giving, while 73 percent of those in rural areas and 51 percent in urban areas express the need for contribution to charity and philanthropy (TAF and VAPEC, 2011). The giving of Vietnamese individuals and enterprises includes monetary and time contributions to official and unofficial charitable and philanthropic agencies or organizations (Dang and Tri, 2013; TAF and VAPEC, 2011; Vien Nghien cuu xa hoi kinh te va moi truong [iSEE], 2015).
The practice of giving confronts some obstacles in the Vietnamese context. Lack of trust, lack of understanding, and limited giving channels are identified as three main obstacles that contribute to the reluctance of Vietnamese people regarding charitable giving (Center for Community Development, 2012; TAF and VAPEC 2011). Due to ‘a lack of transparency and trust’ in how their giving will be used, as well as what may be donated besides money and where to find trustworthy and appropriate organizations to donate to, Vietnamese people may not contribute as much as they intend (TAF and VAPEC, 2011). In this situation, giving to faith-based organizations becomes a preferred option when people wish to donate for a charitable purpose.
Buddhists have a high potential for charitable giving since giving is a core practice of Buddhists. The study NAFOSTED VIII1.1-2012.05 examines the practice of charitable giving among Vietnamese Buddhists. In this study, 685 participants in two major metropolitan areas in Vietnam (433 from Hanoi city and 252 from Hue city) were asked to take part in a survey using convenient and snowball sampling. In total, 391 of them responded to the question ‘Assuming that after spending on basic needs for you and your family and you have 10 Vietnamese Dong [VND] left, how will you spend these VND 10?’. Approximately 67.4 and 44.5 percent of the participants reported they would be willing to spend their extra budget of VND10 on charitable and dakkhina giving, respectively, compared to 61.6 percent of them who planned to save and 46.2 percent who planned to shop, among other things.
This study showed the significant differences of the intended budget for charity among different groups of participants’ occupations and levels of Buddhist self-identification. To be more specific, the study results suggested significant differences in the intended budget for charity among paid officers/workers, self-employed, and unemployed participants. In particular, the groups of self-employed and unemployed individuals were more likely to contribute to charity compared to paid officers/workers. Regarding the level of Buddhist self-identification, the study also suggested significant differences of the intended budget for charity among four groups of non-Buddhists: from those who strongly self-identify as Buddhists. to those who have a weaker attachment to the Buddhist identity. People who self-identified as Buddhists are more likely to contribute more to charity compared to those who self-identified as non-Buddhists. The Buddhists tradition of giving partly explains why BBOs have advantages in community connection and resource mobilization, including fundraising.
Charitable and philanthropic activities of BBOs
Under the influence of Buddhism, Buddhist temples are acknowledged as the most popular channel for charitable giving among Vietnamese people (iSEE, 2015; TAF and VAPEC, 2011). Since its establishment in 1981, the VBS has actively participated in charitable and philanthropic activities. Over the period 2012–2017, through Buddhist temples the VBS collected approximately 6838 billion dong (US$284 million), including more than 100 billion dong mobilized by BBOs, to provide shelter, food, clothes, medical care, and sometimes basic education for orphans, children with disabilities, older adults without family care, and underserved workers nationwide (VBS, 2017). Recently, due to the mass effects of HIV/AIDS on Vietnam citizens, some BBOs have welcomed and provided care, including end-of-life care for people with HIV/AIDS. Among a wide range of activity categories receiving Buddhism-based contributions, public health, such as charitable clinics and clinics of traditional medicine for vulnerable people, outnumbered others in the report. Other activities, such as providing care for older adults and individuals with HIV/AIDS, started emerging recently (Table 1).
Basic Buddhism-based charitable activities.
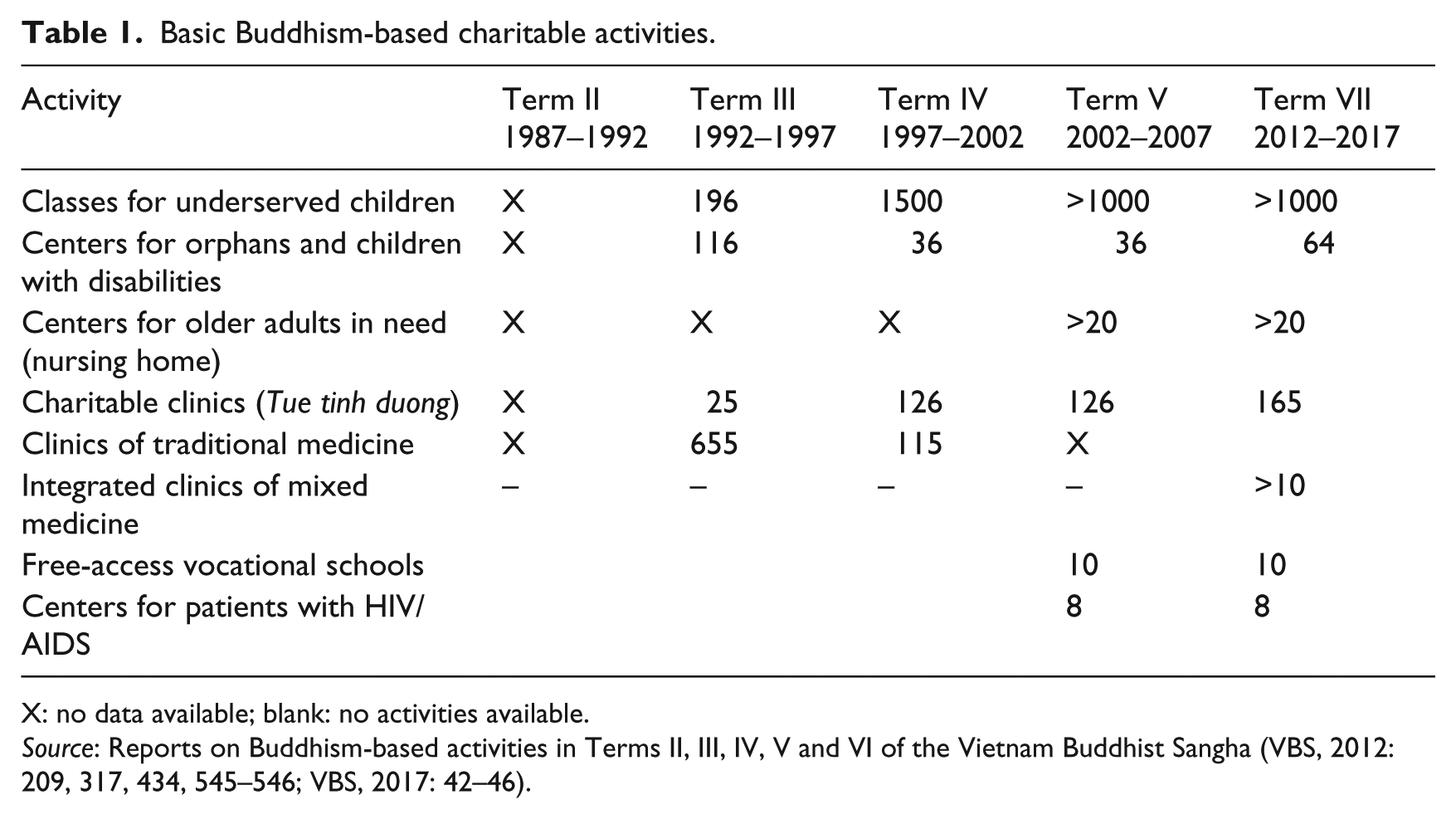
X: no data available; blank: no activities available.
Source: Reports on Buddhism-based activities in Terms II, III, IV, V and VI of the Vietnam Buddhist Sangha (VBS, 2012: 209, 317, 434, 545–546; VBS, 2017: 42–46).
Based on reviewing the major charitable activities and their results as mentioned above, we argue that the VBS and its branches function as both charitable and philanthropic organizations. Charitable activities undertaken by these organizations often include emergency assistance through the giving of money, food, and clothes to those in need. Currently, BBOs focus more on community development emphasizing long-term effects, such as building and renovating roads; establishing charitable schools and clinics of traditional medicine; and running Buddhism-based shelters for orphans, seniors without family support, and people with HIV/AIDS. One of the major strengths of BBOs is their open access to vulnerable populations, which reaches more beneficiaries than public and private services. For example, Buddhism-based Nhan Ai Phat Quang kindergarten provided free childcare for poor parents who did not qualify for financial support from public services. This free service helped 85 percent of involved households to increase their income by spending more time working (Tu, 2017).
Despite many achievements, the Superior Buddhist Monk Thich Nhu Niem (2011) demonstrates three main challenges of BBOs. First, BBOs lack a systematic mechanism of operation at every level. Up to 2011, the VBS had 40 out of 56 charitable/philanthropic departments at the provincial level, yet there were no consistent regulations shared by these departments. Second, there was no stable funding, except for donations from Buddhists, to run philanthropic activities in these departments. Third, most current staff in BBOs are unqualified to provide social service delivery. He therefore advocates the transformation of BBOs into scientific philanthropy and social work. Responding to this, VBS collaborated with some educational institutions to provide training in childcare, medical care, and social work for 140 monks and nuns in Ho Chi Minh City (VBS, 2012). It is likely that the development of Vietnamese Buddhism-based charity and philanthropy is progressing toward social work.
Linking BBOs to social work centers in the Vietnamese context
The discussion above emphasizes the limitation of both public and private sectors in providing accessible and affordable social services for vulnerable and disadvantaged groups. Meanwhile, BBOs have successfully mobilized resources from communities to address the needs of underserved groups. Addressing a similar situation in the United States, Tangenberg (2005) points out the important role of social work in faith-based organizations, as well as the great potential of these organizations in social service delivery and political advocacy targeting marginalized communities. Hence, Tangenberg (2005) argues for the benefits of collaboration between faith-based organizations and social work. In Vietnam, incorporating Buddhism into social work is also suggested as a new trend of indigenous social work in Vietnam (Hoang, 2012; Nguyen, 2012; Nguyen et al., 2012).
Based on all these reasons, we propose a model which links BBOs to social work centers (Figure 1). This model is adapted from the model of policy-based profession (Popple and Leighninger, 2011) and the model of service delivery in mental health in Vietnam (Nguyen, 2013). The policy-based profession model (Popple and Leighninger, 2011) lays out the connection between policy, professional (social work), and client systems. The model of service delivery in mental health in Vietnam (Nguyen, 2013), on the other hand, conceptualizes the proposed collaboration between Buddhist temples and social work services in mental health in Vietnam. While the former model (Popple and Leighninger, 2011) approaches social work as a public service sector only, the latter model (Nguyen, 2013) addresses the role of BBOs (Buddhist temples) in social service delivery in Vietnam. Therefore, adapting and combining these two models provides a strong foundation for the proposed model (Figure 1).
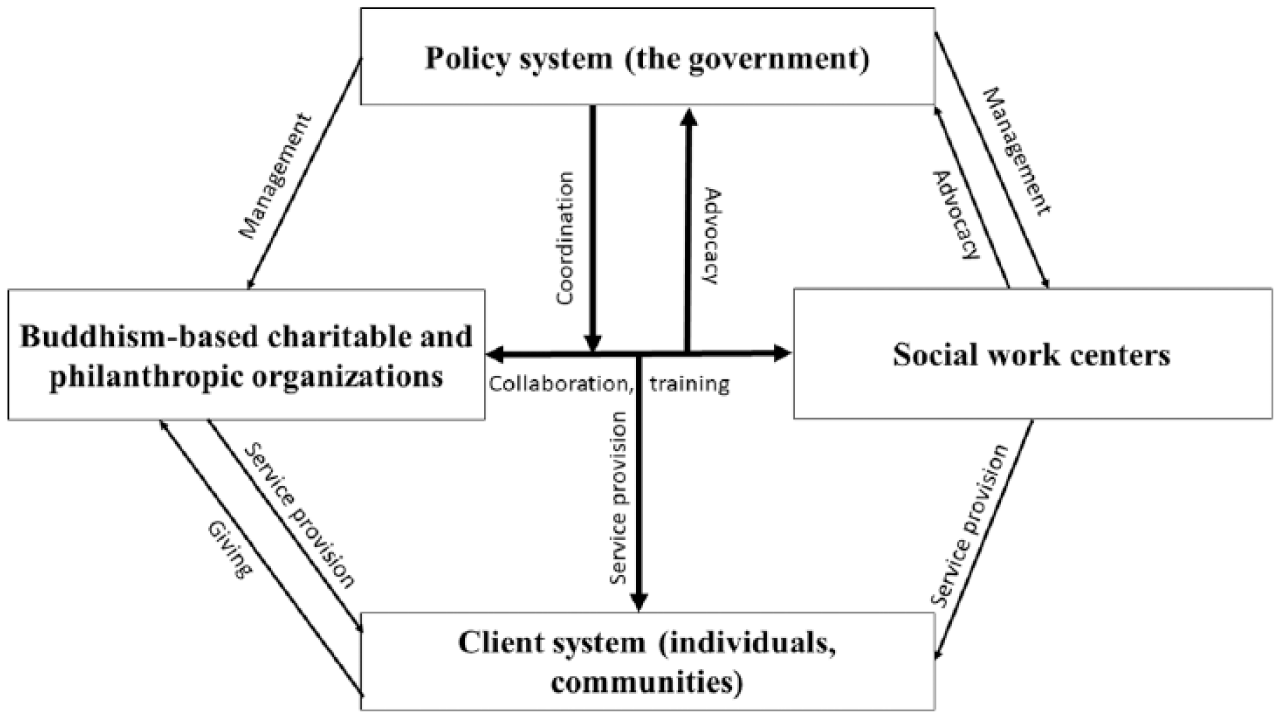
A model for linking Buddhism-based charitable and philanthropic organizations and social work centers.
Rationale of the linkage between BBOs and social work centers
We propose the model of linking BBOs to social work centers (Figure 1) to address the current issues in a Vietnamese context. First, Vietnamese people prefer to seek help for their problems and needs from Buddhist temples and Buddhist monks rather than social work centers (Nguyen, 2013). Social work is a new profession in Vietnam, and public perception of social work is limited. Most Vietnamese people perceive social work as charitable work that everyone with goodwill can do (Nguyen, 2002, 2015a, 2017). Although social work centers have received political and financial support from the government, they likely confront a great obstacle to bridge their services to target beneficiaries in communities (Nguyen, 2013). With the support of BBOs, including 47,237 monks and nuns, 17,287 Buddhist temples (VBS, 2012), and their capacity of fundraising, social work centers may reach and provide services to those in need in communities.
Second, the international literature shows that BBOs, including Buddhist temples, with great resources and trust from communities, can serve as both official and unofficial social service centers in addition to their religious purposes (Canda and Furman, 2010). For example, Thai Buddhist temples have been identified as ‘centers for education, local social welfare, and community activities’ (Gerald et al., 2013: 276). In Western countries, Buddhist temples provide various social services, such as psychological counseling, palliative care, end-of-life care, and others for Asian immigrants (Sherwood, 2001). In Vietnam, many Buddhist temples have also hosted, fed, and provided medicine and counseling for people having difficulties, such as poor people, orphans, widows, people with disabilities, and others in the community (Nguyen, 2015b).
Third, current Buddhist-run social welfare units are serving diverse disadvantaged and vulnerable populations through their own infrastructure, yet they lack scientific methods to operate their centers effectively. BBOs have run numerous orphanages, nursing homes, free-access vocational training centers, charitable schools, charitable clinics, and others. Many of them do not have sustainable funds and effective operation mechanisms to maintain their services (Thich, 2011). In addition, staff serving in those social service units do not have professional training in social services (Thich, 2011). These limitations lead to the termination of many Buddhism-based social service units, such as the clinic of traditional medicine at Phap Hoa Buddhist Temple in Ho Chi Minh City (Thich, 2011).
The current situation of BBOs and social work centers suggests a need for collaboration between these two service systems. This suggestion is also based on lessons from other countries, such as England and the United States, where social work development is rooted in religion-based charity and philanthropy, including scientific philanthropy (Bremner, 1956; Marx, 2013; Richmond, 2012; Science Encyclopedia, n.d.). The transitions from religion-based charity to philanthropy, scientific philanthropy, and social work are marked by (1) the expansive mission from poverty relief only to distress prevention and (2) changing methods from pure giving to scientific and evidence-based practice (Bremner, 1956; Marx, 2013; Richmond, 2012; Science Encyclopedia, n.d.). Vietnamese social work has a strong foundation built upon collectivism, community orientation, and Buddhism-based giving, which is important for the development of indigenous social work (Dang, 2011; Nguyen, 1985, 2002, 2015a). There is high potential for collaboration between BBOs and social work centers, yet the need for a feasible collaboration mechanism is pressing. We suggest a collaboration mechanism as follows.
Collaboration mechanism of BBOs and social work centers
Stakeholders
In the proposed model, we present four key systems: the client system (individuals and communities), the policy system (the government), and two main units providing social services, including Buddhism-based charitable and philanthropic organizations (informal social service units) and social work centers (formal social service units). BBOs refer to Buddhist temples and charitable service centers which are undertaken by Buddhist temples or VBS. These units are under the management and regulation of the Vietnamese government. Currently, each service unit has provided social services or advocated for clients independently (MOLISA, 2013; Nguyen, 2013). The collaboration between BBOs and social work centers is currently supported by the Vietnamese government. Specifically, the Vietnamese government aims to support and improve the quantity and quality of non-public services until this sector reaches at least 60 percent of total service agencies/centers in the country (MOLISA, 2015b).
In the proposed model, social workers will play a key role in the partnership between BBOs and social work centers. It is likely that the number of social workers consulting with and practicing in the BBO setting will increase (Cnaan and Boddie, 2002). Cnaan and Boddie (2002) argue that ‘social workers offer a broad set of skills (for example, proposal writing, case management, program evaluation, and counseling) that can compliment faith-based organizations’ (p. 231). In addition, social workers are considered the appropriate leaders of the partnership between BBOs and social work centers because their professional values and practice ethics will guide them to find common ground between the two service systems (Cnaan and Boddie, 2002).
Target clients, problems, and services
BBOs and social work centers have many characteristics in common. First, they both aim to serve underserved children, lonely elders, the poor, and people affected by dioxins and HIV/AIDS. Second, Buddhist temples and social work centers share functions such as service coordination and provision, education, training, communication, community development, and policy advocacy (Nguyen, 2015a). In fact, both service systems already set up and implement their own centers and services. For example, BBOs have already run centers for orphans and children with disabilities, older adults in need, patients with HIV/AIDS, clinics of traditional medicine, and so on, along with interventions, counseling, and others provided by social work centers (MOLISA and MOHA, 2013). Therefore, in the proposed model, we suggest that BBOs and social work center can collaborate to refer clients to appropriate services available at both service systems.
Implementation
The partnership between BBOs and social work centers can be performed in different areas. In the proposed model, we suggest four main functions in which these service systems can collaborate with each other: joint service provision, mutual training, policy advocacy, and fundraising. In order to improve the efficacy and effectiveness of social service delivery, we suggest in the model a mutual, cooperative partnership between the two units for joint functions. One of the first forms of the collaboration is that service staff from BBOs (including Buddhist monks, paid staff, and volunteers) and social work centers (trained social workers) can conduct the intake of new clients, provide necessary services, or refer them to the other if appropriate. Furthermore, both units may develop joint interventions, such as a counseling service and treatment (e.g. meditation class) at Buddhist temples.
Mutual training
BBO staff, including Buddhist monks and social workers, have their unique strengths to offer in mutual training. Social workers can offer training in case management, program evaluation, and counseling skills for BBO staff and Buddhist monks as many clients prefer to ask Buddhist monks for advice for their problems. They also can train Buddhist monks to provide some specific treatments to clients. On the other hand, religion and spiritual dimensions are considered a key cultural competence of social workers. Buddhist monks can provide great insight, philosophies, and techniques to social workers regarding roles of religion and specific Buddhism-based mindfulness practice, such as meditation.
Policy advocacy
Policy advocacy is one of the roles of social workers, while BBO staff merely participate in policy advocacy. However, BBO staff, especially Buddhist monks, often have a strong connection with communities and critically understand people’s circumstances and needs. With specific training in advocacy and leadership skills, social workers can collaborate with BBO staff to advocate for vulnerable people in the community. In addition, they can also advocate for culturally competent practice and services incorporating Buddhism into social work.
Fundraising
Fundraising is a strength of BBOs. Social work centers run on limited government budgets, and not all people in need can qualify for free services and support from those centers. In this situation, BBOs may be a solution as they have significant potential for resource mobilization. The giving potential from the community to BBOs will likely promote the success of fundraising for services and aids which may cover larger beneficiaries. For example, when a natural disaster happens in Vietnam, such as a major flood, BBOs often call for donation of food, money, clothes, and so on immediately. They tend to be among the first organizations with substantial aids to support communities. Collaborating with BBOs in fundraising, social work centers are more likely to successfully deliver their programs and services to communities.
Conclusion
Buddhism-based charity and philanthropy have significantly contributed to supporting vulnerable people in Vietnamese society. Based on the relationship of charity, philanthropy, and social work and as well as current situation in Vietnam, we argue that Buddhism-based charity and philanthropy are progressing toward a social work model of service delivery. Therefore, linking BBOs to social work centers potentially addresses the limitations of BBOs, as well as of social work centers, which are new to Vietnamese people. The informal and formal social service units can collaborate to train each other, assess needs, provide services, and advocate for their clients. They can also work on joint fundraising activities to mobilize resources from communities. In order to implement the model for linking the two units, we recommend two main strategies. First, providing social work training to BBO staff, including Vietnamese Buddhist monks, will increase the cooperation between the two units, as well as improve the effectiveness of service delivery. Second, social work with religious and spiritual beliefs needs to be a core component of social work education in Vietnam. Linking Buddhism-based charitable and philanthropic organizations to social work centers will contribute to addressing diverse social problems in Vietnam, as well as promote an indigenous and culturally appropriate approach to Vietnamese social work.
Footnotes
Funding
This research is funded by Vietnam National Foundation for Science and Technology Development (NAFOSTED) under grant number VIII1.1-2012.05