
Abstract
This study identifies the cultural values affecting near-lethal suicide attempters’ help-seeking behaviours. Six Chinese survivors of intentional near-lethal self-poisoning were interviewed and their medical records examined. Interviewees with strong suicidal intentions had less demand for healthcare services and were resistant to care. Non-contact with services was associated with perceived service irrelevance, unhelpfulness and personal need to maintain self-reliance and dignity. Service providers should be trained to be sensitive to these individual values to allow the delivery of a culturally-appropriate service for this population. Social work empowerment models that focus on users’ self-reliance should be adopted in practice for this high-risk group.
Introduction
Suicide and suicide attempts are closely associated with emotional vulnerability, although those with non-psychotic symptoms tend not to contact mental healthcare service providers prior to their suicidal acts (Law et al., 2010, 2015). Survivors of near-lethal suicide attempts are likely to have a high suicide intent, so may serve as a valid proxy for those who complete suicide (Hawton, 2001). A number of barriers have been found to be associated with not seeking help related to factors such as the helpfulness, accessibility and availability of relevant services (National Collaborating Centre for Mental Health [NCCMH], 2012). These include dissatisfaction with healthcare professionals, discouraging compliance with treatment (Cooper et al., 2011), a lack of confidence among clinical staff (Gibb et al., 2010) combined with providers’ negativity towards repeated episodes of self-harm (Saunders et al., 2012). Yet there is a lack of in-depth personal accounts about factors shaping a preference for death over professional help to solve problems. Suicide prevention requires identifying what determined suicide attempters go through, their rationalizations and the causes of ambivalence towards service use before and after the attempt. This information could inform relevant and acceptable service design and access.
Several explanatory theoretical models have been developed to account for people’s decisions about access to healthcare services. These focus not only on the association with individual needs or vulnerabilities, but also on different forces behind these decisions and their interaction with the surrounding structural or non-structural barriers. The Behavioural Model (Andersen, 1995; Babitsch et al., 2012) emphasizes how inequitable access to healthcare is largely determined by individuals’ social and demographic backgrounds, needs, health beliefs and enabling resources. The Network-Episode Model (NEM) discusses how the pathway to care for people with a mental illness is a muddling-through process mainly shaped by the influences exerted by surrounding social and cultural networks (Pescosolido et al., 1998). The Health Belief Model and Cognitivist Theory focus on why people do or do not use services, including subjective perceptions of potential benefits of medical care for health problems (Rosenstock, 2005) and the positive gains of non-attendance, not ceding control of self to professional advice and not giving up priorities that are treasured more than health Boudon, 1996, 2017; Buetow, 2007). The Cycle of Avoidance (COA) model shows how not seeking help was considered a viable strategy by young people who normalized emotional distress to accommodate or deny their problems (Biddle et al., 2007). COA suggests that interpretation of lay diagnoses of problems and meanings attached to help-seeking should be central to understanding non-help-seeking behaviours (Biddle et al., 2007). In Chinese societies, disparities between the need for and use of mental health treatment have been found in comparison with other ethnic groups. This is partly attributable to cultural beliefs emphasizing the maintenance of personal and family ‘face’. Disclosing emotional distress shows weakness and a lack of family harmony (Mak and Chen, 2010). Features from these models structure this qualitative in-depth study. These models suggest that services designed for people with particular health or emotional vulnerabilities have to pay special attention to a number of dimensions. These include accessibility, affordability, association with stigma, loss of self-autonomy and lack of respect for clients and their families.
Suicide has been ranked as the 11th leading cause of death in Europe and the 15th globally (Gjertsen et al., 2016). The annual global age-standardized suicide rate in 2015 was 10.7 per 100,000 persons (World Health Organization, 2017). All 7.4 million people in Hong Kong (Census and Statistics Department, 2018) have access to affordable primary and specialized healthcare services (Food and Health Bureau, 2012). The age-standardized suicide rate fell from 14.7 per 100,000 persons in 2003 to 8.9 in 2016 (Centre for Suicide Research and Prevention, 2017). Yet over half of those known to have psychiatric illnesses received no psychiatric care prior to their suicide (Law et al., 2010). Examining this pattern of denying mental illness and service avoidance before making near-lethal suicide attempts will allow more effective service design.
Method
Grounded theory (Glaser, 2014; Strauss and Corbin, 1997) was adopted for this qualitative study to extract and examine meaning from the personal accounts of participants’ subjective reality. Grounded theory was applied because the study operated inductively to draw links among repeated ideas or concepts that were grounded on the qualitative data, through which it might lead to the formulation of a new perspective or theory that could be different from existing theories on service use patterns prior to suicide. Through semi-structured interviews, participants were asked about suicide attempts, the interaction between themselves and their networks prior to the near-lethal act, and details of service use. Three areas were covered: (a) How did individuals perceive their need for healthcare or other psychosocial services to ameliorate their distress and what meaning did they attribute to their decisions on service use? (b) What barriers to care did participants identify and how did they try to overcome these barriers? (c) How were cultural values related to ambivalences about suicide which might have shaped their decision with regard to using services related to emotional distress?
Sampling and participants
Since survivors of near-lethal suicide attempts are ‘hard to reach’, purposive sampling was used to identify participants who met a list of inclusion criteria in order to maximize the richness of the data (Abrams, 2010) about this group of patients. The setting where potential and surviving participants could be more conveniently found was a public hospital’s poisoning information centre. It has a list comprising 4,177 Hong Kong residents who had reported intentional self-harm using poison from 1 July 2008 to 30 June 2011. Of these, 17.2 percent, 57.2 percent, 0.3 percent, 14.9 percent, 7.8 percent and 1.4 percent were rated as no effect, minor, mild, moderate, major and fatal, respectively. The sampling was purposively screened among a total of 287 acts of intentional self-harm that had happened within the preceding 12 months and resulted in a major outcome (106 men and 181 women aged 18–59), requiring treatment in an intensive care unit. Out of the 287 people who received phone calls requesting their participation, 16 were successfully contacted. Six (three men and three women) gave their written consent to attend a 60- to 90-minute audio-recorded semi-structured interview. Background information on their attempted suicides and service use was collected using a form based on the Oxford Monitoring System (Hawton et al., 2003), the Beck Suicide Intent Scale, Chinese version (SIS; Beck et al., 1974; Zhang and Jia, 2007) and a checklist of service use. Clinical records, including their history of previous self-harm and psychiatric diagnoses, treatment compliance and other related information, were retrieved. Assessment of the lethality of the suicide attempts and clinical outcomes was divided into five levels: no effect, mild, moderate, major (life-threatening signs or symptoms or significant residual disability or disfigurement) and fatal (Chan et al., 2016). All were rated as ‘major’; their suicide attempts were near-lethal and they were unconscious upon hospital admission. During the interviews, participants were asked to share their views on (a) the process of suicide attempt(s), (b) their interaction with networks (i.e. families and friends, healthcare and psychosocial service providers) in shaping their service use decisions, (c) experiences of previous service use prior to the indexed near-lethal attempt and (d) values, beliefs and perceptions in accessing care. Ethical approval was obtained from the Hong Kong Hospital Authority, Kowloon Central/East Clinical Research Ethics Review panel (Ref: KC/KE-11-0076/ER-2).
Data analysis
All of the interview records were transcribed verbatim in Cantonese. A thematic approach comprising open, axial and selective coding and core themes (Glaser, 2014; Strauss and Corbin, 1997) was adopted. Using constant comparative analysis, themes were compared, conceptualized and operationalized simultaneously to support the ongoing formulation of new questions and observations during the data collection process. A core set of analytical codes was generated in each one of the three areas of exploration, and then continually compared and revised based on similarities and differences until a number of prominent themes or concepts had emerged that were sufficiently comprehensive to illustrate the variety of the results. New codes were assigned to alternative aspects of interpretations or meaning raised by the participants. Memos were written to link these themes/concepts (Glaser, 2014; Strauss and Corbin, 1997), showing how the participants made sense of their views and behaviour. The qualitative data was triangulated by participants’ basic demographic and socioeconomic characteristics, service use records, SIS scores and clinical data, which were documented in detailed case summaries. NVivo10 software was used for analysing qualitative data.
Results
Background of the six participants
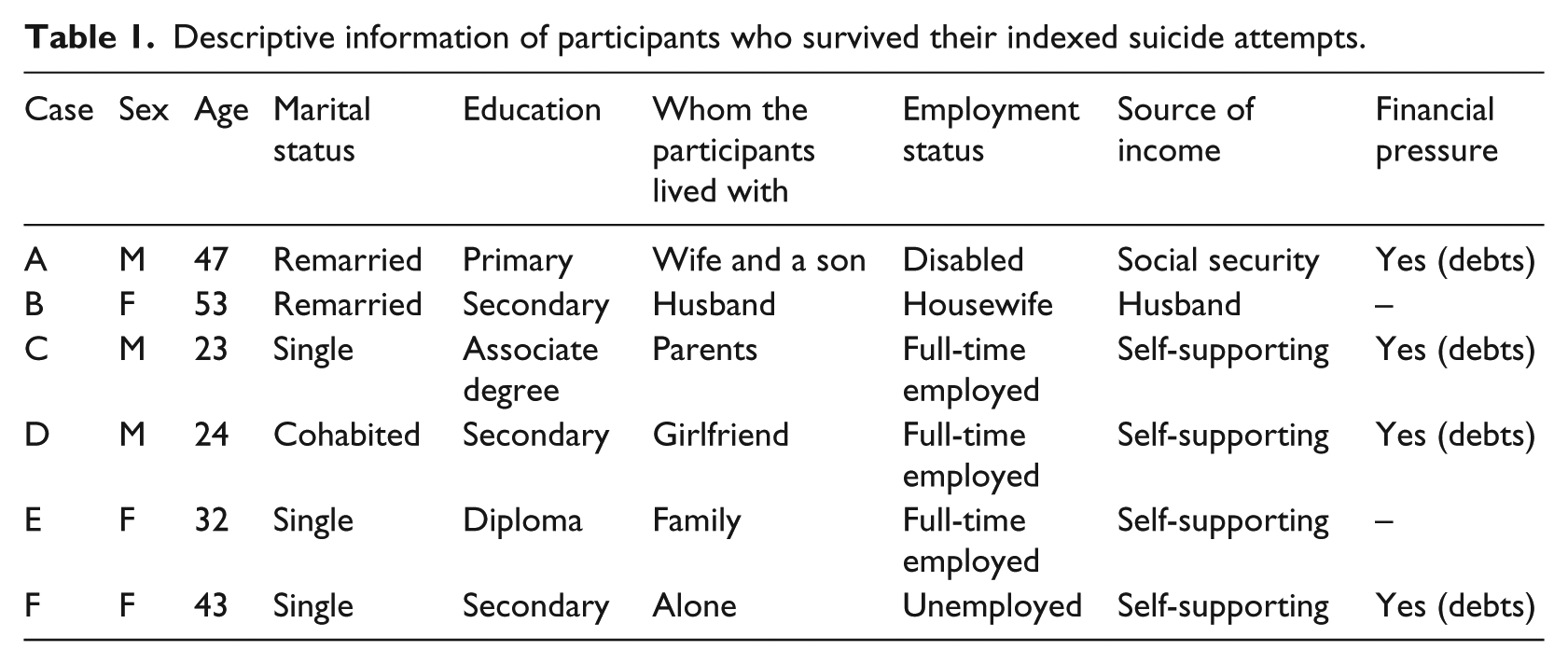
Tables 1 and 2 give an overview of the participants’ basic demographic and socioeconomic characteristics, psychiatric diagnoses at the indexed and any previous attempt(s), SIS scores, medical outcomes, previous service use, and help sought from family and friends before the indexed attempt. All had experienced negative life events (e.g. work pressure, relationship issues, debts) triggering/worsening their mental illnesses/emotional problems. Four had previously attempted suicide and tried to hide the current attempt from others.
Descriptive information of participants who survived their indexed suicide attempts.
Clinical conditions of indexed attempt and service use history.
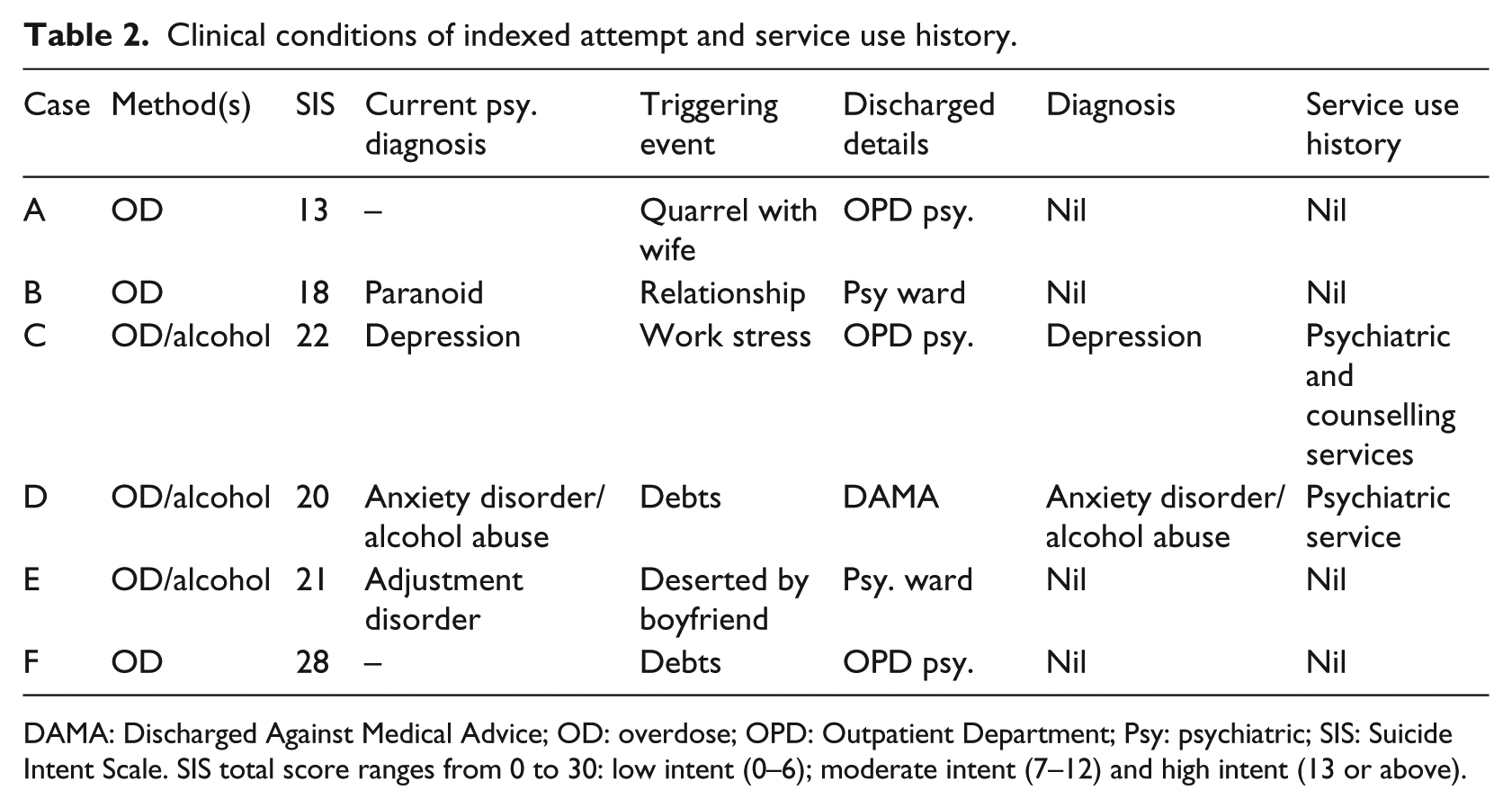
DAMA: Discharged Against Medical Advice; OD: overdose; OPD: Outpatient Department; Psy: psychiatric; SIS: Suicide Intent Scale. SIS total score ranges from 0 to 30: low intent (0–6); moderate intent (7–12) and high intent (13 or above).
Participant A: Male, remarried, aged 47, bankrupt; no previous suicide attempt. He had suffered from kidney disease for several years after closing his business. He removed his Tenckhoff catheter (for his kidney condition) and swallowed all of his medication when his second wife left him. He was admitted to a hospital intensive care unit (ICU) and later sent to a closed psychiatric ward for observation. He had moderate to high suicide intent (SIS: 13), and refused to be helped by anyone around him.
Participant B: Female, housewife, aged 53, remarried; no previous suicide attempt. Having overdosed at home, she was taken to the hospital by her husband. She was admitted to the ICU and then to a closed psychiatric ward for 1 month of treatment. She believed her husband was having an affair and was diagnosed with ‘delusional disorder’. Her suicide intent was high (SIS: 18) and she rejected her husband’s suggestion that she needed professional help. She believed suicide in her situation was inevitable and trusted no one to render appropriate help.
Participant C: 23-year-old male, single, employed full-time, living with parents; a number of previous suicide attempts. He had persistent suicidal thoughts and self-cutting behaviour when he was a teenager, sought help from a school counsellor and a psychiatrist, but was discouraged by poor treatment outcomes despite regular psychiatric follow-up. In the indexed attempt (SIS: 22) he overdosed at home, was discovered unconscious and sent to hospital by his family. He was admitted to the ICU, then treated for depression at a psychiatric hospital for a month.
Participant D: 24-year-old male, cohabiting with girlfriend, employed full-time; several previous suicide attempts. He saw a psychiatrist in a community-based clinic and was diagnosed with ‘alcohol abuse’ and ‘anxiety disorder’. He was deeply stressed from having to pay off his father’s debts. He took all accessible medication together with alcohol (SIS: 20), was found by his girlfriend and admitted to the ICU. When he regained consciousness, he felt ashamed of himself and refused all help.
Participant E: 32-year-old female, single, full-time professional nurse; no previous suicide attempt. She decided to end her life (SIS: 21) after breaking up with her boyfriend. She took patients’ medications with alcohol at work. She was admitted to an ICU unconscious, and then to a closed psychiatric ward for observation, diagnosed with ‘adjustment disorder’. She described herself as optimistic, a good problem-solver, and knowledgeable about services and crisis helplines. She thought none of these resources were relevant to her own suicide.
Participant F: 43-year-old female, single, left a long-term position as a healthcare worker after her father’s death; had made three suicide attempts prior to the indexed one. She was upset by her unemployment and found it difficult to get another job. As the financial pressure from paying off her mortgage built up, she overdosed by taking all accessible medication before a scheduled visit from her friends and a social worker. She was rescued, sent to hospital and treated in the ICU (SIS: 28). F’s previous contacts with social workers and suicide prevention services were unhelpful. She strongly believed that everyone should solve their own problems, just as she had managed to look after herself and her father following her mother’s death decades ago.
Intentional disengagement from networks’ help and non-disclosure
All six participants had familial and/or friendship networks that offered both tangible and intangible support. Some of these networks had explicitly facilitated their contact with helping services, so were able to have a positive influence on suicide attempters’ perceptions of health and social services. Whether or not they had a high intention to die, all participants displayed intentional avoidance of or disengagement from both formal and informal networks. They adopted an attitude of strict non-disclosure concerning their suicidal intentions as the following excerpts show.
Participant E’s desire to commit suicide was focused and clear: It might sound ridiculous that I went to work as usual, yet that was exactly what I did – without a second thought. I knew I had to finish what I had to [at work], and I would do it [commit suicide] afterwards. In between, I did not struggle at all.
Prior to his indexed attempt, Participant C had a history of psychiatric treatment for depression, but saw no sign of recovery and attempted suicide as a result. After lengthy but ineffective treatment, he wanted to end his life using a more lethal method than in previous attempts: I thought it’s extremely lethal . . . I wanted to die. I thought if I was sent to hospital, I would still die.
Participant F had previously attempted suicide and wanted to do it again before her friends could offer help. She was fully aware of their intentions and purposefully avoided them: One of them [my friends] was very smart, and said I talked strangely as if I was departing. So, during her next few visits, I was smart too. I knew they might have discovered something, so I had to expedite my departure from this world. I did not want anybody to rescue me.
The participants deliberately kept their plans to themselves before the indexed attempt and had no intention of disclosing them, as Participant C’s remarks indicate: I made sure I didn’t tell my family, or my friends either. Actually I told no one.
Regardless of the participants’ suicidal thoughts prior to their indexed attempts, none had sought help or considered that they needed medical treatment or professional psychosocial services. Three themes were drawn from participants’ interpretation of their non-contact pattern:
Theme 1: Irrelevance
The participants did not consider accessing services a viable option. There was a gap between their perceptions of their problems and their use of services. Participant E was well-educated, and explicitly stated that she could have sought help easily knowing the what, where and how of service access. Yet she saw the help they offered as irrelevant to her own problems, and thus did not see herself as a service target, as her comments show: I didn’t think I needed it . . . not afraid of being labelled, but I had never thought of making those calls [to a psychiatrist].
Participant D had seen a psychiatrist several times, but never considered seeing one when he wanted to end his life, even though he knew how to do so: When you talk to a stranger, he doesn’t know you; he will just ask you not to do anything stupid. It is just the psychiatrist’s job. He may not understand you or your situation, so talking to a psychiatrist doesn’t help.
Participant F was also convinced that she did not need healthcare services, believing that they were appropriate only for those with more pronounced psychiatric symptoms: They [people needing psychiatric treatment] have hallucinations, delusions. I think they require psychiatric treatment . . . I didn’t talk to myself, and I didn’t feel mentally deranged and so I did not need to see a psychiatrist.
Theme 2: Perceived unhelpfulness
All six participants believed that healthcare services would be ineffective for their problems, which were interpreted as non-medical issues. Participant E claimed that she was quite resourceful in obtaining support from her own networks, including various kinds of mental health assistance, but was unsure that any of it was helpful: I wasn’t sure if they [mental health services] could help me at all. I have a very good friend who is a doctor, and I often seek help from him when I have problems and if I think he can help. [If I had any problem], I would find someone who is competent.
Participant C had not found psychiatric treatment very helpful in stopping his suicidal thoughts. He was left frustrated, and simply felt like ‘ending it all’: I realized the problem could not be completely resolved. Seeing a psychiatrist could calm me down for a short period of time, but the negative feelings would come back sooner or later. When I reached that critical point, I would do it anyway.
As noted earlier, Participant B believed that her husband was having an affair. She rejected her husband’s suggestion that she see a social worker. She did not want to reveal her true thoughts and feelings to a psychiatrist because he or she would not believe her about the affair: They [social workers] usually said that I was ruminating, that nothing had actually happened, and that there was no evidence for it. The doctor(s) said the same thing, so I stopped telling them about my feelings’.
They [psychiatrists] just thought that since I looked more dominant than my husband, he could not have … gotten into an affair.
Theme 3: Self-reliance
Overloaded with emotional distress, participants preferred a self-help approach instead of reaching out for help. This was driven by a desire to retain their dignity, to avoid repeating a previous negative experience of service use, or to accept responsibility for problems to avoid burdening family or friends. Participant A expressed a strong desire for self-reliance and to maintain his identity as a useful person within his social network: I think it’s fine to help others, but asking for others’ help . . .? I [prefer to] rely on myself. I would rather try [to be self-reliant]; I would force myself. I have my dignity even though I am poor. This is no joke.
Participant F’s previous experience of seeking help from social workers had been so negative, she said that being self-reliant was better than enduring such ‘help’. Rather than be disappointed again, she preferred engaging in a lethal act without seeking any help: [Social workers] simply said there was no way they could help . . . That means I had to solve [my problems] myself.
Many Chinese place a high value on being the giver of help in their families and resist role reversal. This is demonstrated in Participant F’s comment that she would rather find ways to pay off her debts without seeking help from her family network: I was so afraid, and I didn’t want to hurt my family . . . I didn’t want them to pay off my debts . . . I didn’t want to disturb them with my problems.
Participant C said that death was better than receiving others’ help again. His desire not to bother others was intense.
Was there any other option? What’s the point of help? Isn’t it better to let it happen? If one wants to die, better let him/her die . . . I’d rather let it happen [death].
Participant F, too, said she would rather have died than receive help from friends: [My friend] asked me not to act stupidly. Maybe she sensed that I was unhappy, and so we cried together. I said my life was not satisfactory, and I did not want to carry on. She asked me not to think that way, and said there would always be a solution . . . I was in a panic that night . . . frightened [by the offer of help]. I wanted to expedite my departure from this world as soon as possible. I could not let them help.
Discussion
Detours from pathways to care through intentional disengagement
The pathway to care is a process with direction and duration that starts with the initiation of help-seeking and contact by people who are in distress (Bhui et al., 2014; Rogler and Cortes, 1993). However, assumptions about rationality in seeking appropriate care, as suggested by the Behavioural Model (Andersen, 1995; Babitsch et al., 2012), may not be applicable to people with a strong intent to die. The experiences of the six participants, particularly during extreme distress, were more consistent with the Cognitivist Theory (Boudon, 1996, 2017; Buetow, 2007); people do not naturally strive for better health and actively seek relevant support. The participants with a stronger suicide intent had less motivation to seek care because they saw help as irrelevant and ineffective, even believing it would make things worse. This led away from the pathway to care and towards near-lethal suicide attempts. They intentionally detached themselves from their social and healthcare networks and declined offered help because they felt that healthcare, psychosocial services and even friendship had no relevance to their intention to die. Some of them tried to solve their problems alone despite access to and previous use of professional help. Some of this resistance can be attributed to their previous negative experiences of service use and is, within its own terms, a logical response.
It is a matter of value judgement
Previous research on mentally ill patients’ service utilization has focused primarily on the barriers and benefits along the pathways to care, the services being delivered and professional judgements. Recognized barriers include patients’ lack of awareness of their mental health needs (Pagura et al., 2009), stigma (Morgan and Jorm, 2009) and pessimism about treatment effectiveness (Van Voorhees et al., 2006). The prolonged avoidance of healthcare is a way of normalizing the experience of emotional distress and is not based on ignorance of their problems (Biddle et al., 2007). This study has illustrated a dimension of non-contact behaviour that is based not only on avoidance, but also on a sense that contacting healthcare or psychosocial services prior to self-harm would be irrelevant. When there is no link between a service and an attempter’s perceived needs, it is unlikely that a pathway to care will be established. This was particularly noticeable among the participants with a strong suicidal intention in this study.
Although non-contact behaviours are often attributed to patients’ irresponsibility or the inability to initiate the pathway to care, these decisions should not be seen as irrational. Their reasons are meaningful to them (Buetow, 2007). They choose death over treatment that requires relinquishing control of one’s life and loss of dignity and respect. The participants’ non-contact with healthcare services at their indexed attempts was a value judgement made not necessarily as a result of barriers to service access. It seems to have been based on cultural values about self-reliance in times of distress, rendering professional help an undesirable option. Furthermore, self-reliance was preferable to services they did not trust due to previous negative encounters and ineffectiveness of offered interventions.
Self-reliance
The value placed on self-reliance, as we have seen, is associated with a fear of losing control, loss of dignity and being seen as weak, vulnerable and incompetent, where previously there had been strength and competence. Control over their own lives and reputations is the priority, not accessing care (Buetow, 2007). Relying on oneself and not burdening others is an affirmative act and a cultural value that poses a major barrier to seeking help (Griffiths et al., 2011). This has been discussed in both the Chinese (Cheng et al., 2010) and Western contexts (Gulliver et al., 2010). Handling life’s difficulties independently is highly valued. Children with low social initiative but high social control and emotional restraint are more praised in traditional Chinese societies (Chen, 2010). The introverted inclinations, which suggest self-absorption or self-demand, instead of being demanding of others and demanding of changes to the external environment, have been deep-rooted in Chinese dominant schools of thought, such as traditional Chinese medicine, Confucianism and Taoism, about ways to acquire an ideal state of mental health (Yip, 2005). Managing one’s own problems without burdening others or bringing shame to one’s family is related to positive personal characteristics such as being reliable and mature (Wiklander et al., 2003). Suicidal behaviour is considered honourable in certain contexts in Chinese culture. The suicide of Qu-yuan (332–295 B.C.) is glorified as an altruistic act. He drowned in a river to prove his loyalty to the emperor and to demonstrate publicly that the emperor had made a mistake in listening to the advice of his corrupt ministers rather than to that of Qu-yuan. Even today a public holiday celebrates his action (Ji et al., 2001).
The Western practice of psychotherapy, which emphasizes the development of insight into one’s inner psychological processes and thus freeing oneself to make informed choices (Bond, 1994; Chong and Liu, 2002), is not compatible with Chinese culture. The disclosure of personal problems may bring shame on the family and its networks, and therapeutic changes may conflict with the traditional value placed on harmony in long-term familial relationships. In Chinese, the term for help-seeking means ‘begging for help’, suggesting a condescending relationship between provider and recipient. The stigma associated with help-seeking reinforces non-contact behavioural patterns among people at risk of suicide. Data collected from this study indicate that the participants in a Chinese cultural context made sense of their suicide attempts as a natural option via which they took responsibility for their problems, which they saw as preferable to seeking external help from others such as professionals or at times even their social networks.
Implications for social work practice
Seeking help for mental distress specifically during critical life-and-death moments can be positively framed in the Chinese context as the most responsible act for self and family. Yip (2004) suggests that the use of the empowerment model of social work, tailored for Chinese culture, may offer a way forward by encouraging practitioners to frame help as a means of empowering the individual and family as an organic whole, thus reducing the risk of losing face, which was so obviously a concern for our participants.
Social work practitioners who have been trained to establish a collaborative alliance with clients are knowledgeable in trying to understand the client’s perspective (Levin, 2015). Respect for the individual’s self-reliance and dignity must be preserved throughout the entire service delivery process, particularly for those at high suicidal risk. Individuals at risk of suicide are often referred to emergency medical services, which often focus more on physical conditions without attending to individuals’ interpretation about the services’ relevance to their emotional distress, particularly when their issues, for example debts and relationship problems, are difficult to disentangle from a series of contextual factors. Social work practitioners whose expertise is built upon a biopsychosocial model should become involved at the early stage of care so as to offer a comprehensive psychosocial-environmental assessment (Doherty and DeVylder, 2016) using proactive engagement approaches that may allow more options of care. For example, community care or online forums (Owens et al., 2015) for people in distress might allow a relatively higher level of anonymity. Social workers could also take up a lead role among different healthcare professionals for coordinated care (Joubert et al., 2012) that builds links between clinical and community services specifically for alleviating these psychosocial stressors. A study by Petrakis and Joubert (2013) showed potential effects of assertive brief psychotherapy and community linkage in improving the psychosocial functioning among self-harm patients. Law et al. (2016) also found promising evidence on the brief contacts offered by trained volunteers that could help to alleviate self-harm patients’ depressive symptoms and the level of hopelessness in a quasi-experimental design. Yet the role of social work intervention in bridging the chain of care is very much under-researched, particularly for self-harm patients after their discharge from clinical settings.
Services offered on the basis of evaluated needs are unlikely to reach individuals at high risk of suicide, but contact with them is not impossible. Ideas include campaigns using innovative communication strategies to replace stigmatized terms such as ‘begging for help’ with more neutral ones, for example ‘service utilization’; redefining how to be self-reliant in a responsible way, for example ‘to care for yourself is the smartest way to care for your loved ones’; reaching out to individuals with potential high suicide risk in settings such as primary healthcare centres or community mental health programmes involving family caregivers (Ng et al., 2017); allowing community-based social workers a more active role in caring for discharged clients with seamless care and safety plans involving families and friends (Griffin et al., 2017), who may also experience feelings of shame and reluctance to receive services.
A local study has shown promising evidence that online social work engagement and empowerment services could alleviate emotional distress and social withdrawal behaviours among a group of young Internet users (Chan et al., 2017; Law et al., submitted). Given that young people are increasingly active in various online platforms, in comparison with conventional community-based services, social work practices can be designed to allow higher levels of accessibility, affordability, anonymity, autonomy and equality between helper and the helped through online simultaneous interactions. With such features, social workers might be more relevant, timely and acceptable when engaging with people at serious risk of suicide.
Limitations
Given the challenges of identifying survivors of near-lethal suicide attempts, only six cases were interviewed. The small sample size is the major limitation of this study. Yet with the rich data related to the participants’ subjective reality prior to the lethal acts, one can have an in-depth understanding of the factors that impeded their access to service use. In addition, the narratives about the suicide attempts revealed by the participants might be subjectively recalled or interpreted more than a year after the recovery of the incidents. All six participants had positive feelings about having been rescued, and viewed their suicide attempts as mistakes or acts of stupidity. This reaction greatly contrasted with how they felt at the time of the attempt. Their changes in perception could have been caused by the perceived usefulness of the post-discharge care. The reliability and authenticity of the data constituted another major limitation of this study: those individuals who continued to resist external help following a suicide attempt were likely to remain at risk and unlikely to consent to be interviewed for this study. Thus their views cannot be included.
Conclusion
Participants in this study were, at the time of their near-lethal suicide attempt, uninterested in mental health and psychosocial services. They generally saw no hope of finding a way out of being in an extreme state of distress, which is typically found among suicide attempters. To cope with such a devastating condition, they decided to be self-reliant to retain control over their lives (and death), avoiding the potential loss of dignity arising from being perceived as weak, or burdensome to family members or others. The cultural values of self-reliance and individual and family shame avoidance further exacerbated their non-contact behaviours. Preventing acts of near-lethal suicide is difficult as many suicide attempters plan carefully to avoid detection. The study affirms the role of individuals’ values in affecting judgements related to seeking professional help prior to near-lethal suicide attempts. Although all six participants intentionally distanced themselves from their supportive networks, they survived partly due to the care and support from those same networks. One way of establishing care pathways for those at high risk of suicide is to raise awareness of self-harm and suicide prevention and to encourage the use of healthcare services among the families and friends of high-risk individuals. Despite initial reluctance to be helped, vulnerable individuals could be reached if proper care plans were in place as well as coordinated implementation among families, friends and service providers. The results of this qualitative study are not meant to be generalized to all Chinese populations, but indicate a fruitful direction for studying non-contact behaviours that offers sensitive approaches for designing prevention programmes valuing self-reliance, dignity and responsibility.
Footnotes
Funding
This study was completed with funding support from The HKJC Centre for Suicide Research and Prevention of The University of Hong Kong.