
Abstract
Living with dignity until the end is one of the important values in life among older adults as Taiwan enters a super-aged society. This study used a dataset of 4890 participants from a teaching hospital by comparing the differences between group-based and individual-based consultations on advance care planning. The results showed that group-based consultations had a higher advance directive completion rate. Factors such as religion, self-perceived health, and consultation format influenced completion. In conclusion, group-based consultation was an effective innovation with cultural sensitivity for social workers to assist and support diverse populations needing end-of-life planning.
Keywords
Introduction
Advance care planning (ACP) is a critical process for formalizing advance directives and ensuring that individuals’ medical preferences are respected (Emanuel et al., 1995). Over the past three decades, ACP has been extensively studied across multiple countries, with growing research exploring its definition, conceptual development, and influencing factors, highlighting its increasing global relevance (Jimenez et al., 2018; Van der Steen et al., 2024). The topic is more recognized in western societies but most Asian countries have been catching up quickly in order to face the end-of-life needs in super-aged societies (Lin and Lwin, 2026). In many Asian societies where filial piety and paternalistic traditions prevail, family members often find it difficult to accept the withdrawal of life-sustaining treatments for their parents (Akhtar et al., 2025; Cheng et al., 2020; Lee et al., 2024; Pan et al., 2025). In this context, Taiwan enacted the Patient Right to Autonomy Act (PRAA) in 2016, becoming the first country in Asia to establish comprehensive legislation protecting patient autonomy. The Act allows individuals, under specific clinical conditions, to sign advance decisions (ADs) after ACP consultations in which medical social workers often play a coordinating and advocacy role (Chen, 2019; Chin and Fang-ho, 2018; Wu et al., 2023).
Medical social workers play a crucial role in safeguarding clients’ rights. Guided by the person-in-environment perspective, social workers facilitate communication among patients, families, and the healthcare system by navigating family dynamics, interprofessional teamwork, and legal considerations, thereby supporting a balanced decision-making process across different designs for consultation models (Cowles and Lefcowitz, 1992). In addition, from the life course perspective, the aging process involves multiple decision-making challenges, particularly those related to medical care (Hutchison, 2010). ACP offers a structured framework for addressing these issues. Therefore, this study explores whether social worker-led interventions and the consultation model developed in the study can promote ACP engagement and the AD completion.
Role of social workers in ACP
The role of social workers in ACP has been widely discussed in various studies. Rodriguez and Gomez (2020) reviewed past research on the role of social workers in ACP from 2009 to 2019 and found that social workers could serve as effective initiators of ACP discussions during the ACP process. Social workers acted as mediators within the medical team, assisting patients in obtaining relevant information, providing guidance, assisting with administrative tasks and assessing their needs to ensure comprehensive care. In addition, social workers played a crucial role at the end-of-life (EOL) care by offering spiritual support to patients. In other research on renal disease, the author had highlighted another essential function of social workers, including helping patients address psychosocial issues and facilitating health behavior changes through emotional support at an early stage of ACP. At the EOL, social workers trained in motivational interviewing techniques can help clarify their true preferences through structured conversations, thereby enhancing the quality of EOL care (Senteio and Callahan, 2020). Promoting ACP was considered one of the primary responsibilities of social workers (Chan and Yu, 2021). Past research that collected data from the perspective of social workers found that most of them viewed themselves as a facilitator in the ACP process, inspiring patients and their families to engage in discussions about EOL planning (Wang et al., 2018; Werner et al., 2004).
In Taiwan, social workers were facilitators and mediators who not only managed the administrative aspects of the process, but were also tasked with promoting awareness and advocating for the PRAA. They emphasized that ACP is not merely a procedural step to sign an AD, but a meaningful process that allows individuals to fully contemplate and articulate their preferences (Hsu et al., 2022; Lin et al., 2020).
Some studies suggested that ACP benefits social workers’ professional development. By facilitating discussions between patient, their families, and the medical team, ACP helped social workers lay the foundation for long-term care (LTC) services (Payne, 2010). It also presented an opportunity for social workers to take on a leadership role within medical institutions (Otis-Green et al., 2019). Although there is no universally defined role for social workers in ACP today, the existing research suggests that the goals, objectives, and values of ACP align with the philosophy of medical social work and the hospitals’ expectations of social workers (Gagliardi and Morassaei, 2019; Jimenez, 2020; Rodriguez and Gomez, 2020). In addition, social workers possess the ability to assess needs and design intervention programs and advocacy strategies tailored to different demographic groups (Otis-Green et al., 2019). This positions them as highly suitable facilitators in developing and promoting ACP consultation programs. Therefore, it is essential for social workers to continue developing innovative approaches to effectively promote and implement ACP.
Implementation and advantages of ACP group-based consultation
ACP group-based consultation models, first introduced in the United States and Canada, had shown promising results particularly among veterans and older adult populations. One notable approach was Lum’s model, which involved two sessions led by geriatric specialists and social workers, significantly enhancing participants’ willingness to complete ACP documents (Lum et al., 2015). The benefits of group-based ACP discussions were well-supported by various studies. For instance, heart failure patients and their caregivers reported feeling more comfortable engaging in ACP within a group format, which enhanced their understanding of care options and personal values, while also creating a supportive environment for sharing experiences (Bandini et al., 2021). Similarly, some research reported that group discussions among individuals with mild cognitive impairment and their families provided valuable information and recommendations, encouraging participants to contemplate future healthcare decisions collectively (Daddato et al., 2022).
Disease-specific support groups further amplified these benefits by enabling patients and families to discuss care expectations and future plans within a shared experience context, thereby enhancing their comfort and understanding (Ahluwalia et al., 2021). Sharing illness experiences and treatment perspectives in these groups helped reinforce disease knowledge and clarified personal values and expectations (Bandini et al., 2021).
Group ACP is not widely implemented in Taiwan. Yang et al. (2020) were the first to introduce a group-based consultation model in which participants registered by family units, with a total of 5 to 15 individuals taking part in each session. The group-based consultation consisted of two phases. In the first phase, a physician provided an overview of the PRAA, including a lecture on the five specific clinical conditions and care options. In the second phase, the families were divided into smaller groups, each facilitated by a social worker, nurse, or psychologist. This setting allowed participants to share their motivations and life values in a more private and supportive environment. Another study found that group-based consultations could be implemented in community care stations alongside health education activities, particularly for specific populations such as veterans and individuals with cerebellar disorders. These sessions were typically held at community care stations, with an average of eight participants per session (Hsu et al., 2022).
Clearly, the group-based consultation model for ACP maximizes the benefits of ACP discussions while reducing the time and labor costs associated with individual consultations. In addition, this group-based model serves as an effective approach for promoting ACP engagement.
Factors influencing the willingness to sign an AD: The Behavioral Model of Health Services Use
The primary objective of promoting ACP was to increase public participation in ACP consultations and the completion of ADs, thereby ensuring that individuals can experience EOL care aligned with their preferences. To examine the factors that influence individuals’ willingness to engage in ACP and complete ADs, the Behavioral Model of Health Services Use (BM) offers a valuable theoretical framework. Widely applied in public health research, this model sought to explain and predict the determinants of healthcare utilization at both the individual and family levels.
According to Andersen’s framework, healthcare utilization and health status were interrelated, with each influencing the other over time. The BM categorized determinants into three domains: (1) predisposing factors included demographic characteristics such as gender, age, and occupation; (2) enabling factors encompassing practical aspects such as travel time to healthcare facilities, hospital density, and waiting times for services; and (3) need factors referring to the individuals’ or family’s perceived necessity for healthcare. These categories highlighted the multifaceted nature of healthcare decision-making and emphasize that individuals’ health behaviors result from the dynamic interaction of multiple influences rather than a single determinant (Andersen, 2008).
This study aimed to assess whether different approaches to ACP consultations influence individuals’ willingness to sign ADs and to explore how predisposing, enabling, and need factors contribute to this willingness. Insights from this analysis may inform strategies to increase AD completion rates and advance more patient-centered EOL care planning.
Method
Study design
This study employed a retrospective secondary data analysis to compare demographic differences between participants in group-based and individual-based ACP consultations. Variables analyzed included gender, age, welfare status (based on welfare identity), religion, self-perceived health status, and consultation format. The data were organized into two primary categories: (1) type of intervention (group-based vs individual-based) and (2) key demographic characteristics from the basic medical records that were related to decision-making, including older adults’ age, self-rated health status, gender, and welfare eligibility. Given the sociocultural context of Asia, religion was also included as a relevant analytical factor. This quantitative approach was chosen because few studies have compared the demographic profiles of declarants across consultation formats, and quantitative methods provide a systematic means to identify such differences and ensure the reliability of secondary data.
Participants and data collection
This study was conducted at a public hospital in Taipei City, Taiwan. In accordance with the PRAA, ACP was implemented through a multidisciplinary team consisting of physicians, nurses, and social workers. Within this team, social workers played a central role in coordinating and facilitating the ACP process. First, individuals interested in ACP were referred for consultation, during which social workers conducted preliminary ACP discussions and explained the differences between group-based and individual-based consultation formats. Based on these discussions, individuals were supported in selecting their preferred consultation approach. Social workers were responsible for organizing and facilitating group-based consultations, addressing administrative inquiries, and serving as the primary point of contact for subsequent ACP-related communication. Their role focused on supporting understanding, clarifying values, and ensuring smooth coordination throughout the consultation process, complementing the medical decision-making roles of physicians and nurses. A total of 4890 individuals participated in ACP consultations between 2021 and 2022. At the conclusion of each ACP session, participants completed a consultation record form assessing their comprehension of the discussion, their decision regarding the signing of an AD, and their motivations for participation. These forms were completed by the facilitating social workers, integrated into participants’ medical records, and securely archived by the Department of Social Work.
The dataset for this study spans the years 2019 to 2022. However, as the ACP program was in its pilot phase during the initial years, data from earlier periods were relatively incomplete and were therefore used only for preliminary analyses. Given that the proportions of group-based and individual-based consultations became more balanced in the last 2 years, this study focused on data from 2021 to 2022 for primary analysis. All records were reviewed by responsible case administrators to ensure data completeness and minimize the risk of recording bias.
Reflexivity
All members of the research team have professional backgrounds in social work, have completed comprehensive training on the PRAA, and possess practical experience in ACP consultations. While these qualifications enhanced the researchers’ ability to understand the consultation process and contextualize the findings, they also carried the potential risk of overinterpreting the results through the lens of personal counseling experience. To mitigate this, the team adhered to an agreed analytic approach that focused solely on comparing signing rates and demographic characteristics, avoiding speculative interpretations regarding the underlying reasons for signing decisions.
Data analysis
This study employed Andersen’s Behavioral Model as the conceptual framework by incorporating operational definitions across three core dimensions: predisposing factors (gender, age, religion, and welfare status), enabling factors (consultation type: group vs individual), and need factors (self-perceived health) (Andersen, 1995). All statistical analyses were conducted using SPSS version 20.01.
Prior to analysis, cases with missing values on any of the variables included in the analysis were removed using a listwise deletion approach. No outlying or deviant cases were identified that contradicted the overall interpretation of the study findings. Descriptive statistics were first applied to examine the distribution of participants’ characteristics and their motivations for engaging in ACP consultations. Chi-square tests (χ²) were used to compare demographic and clinical differences between participants in group-based versus individual-based ACP consultations, and to assess variations in willingness to sign an AD across the independent variables. Subsequently, binary logistic regression was performed to identify the predictive effect of these variables on participants’ willingness to complete an AD. In addition, stratified analyses were conducted to further explore potential interaction effects and subgroup-specific patterns associated with consultation type and decision-making behaviors (Figure 1).
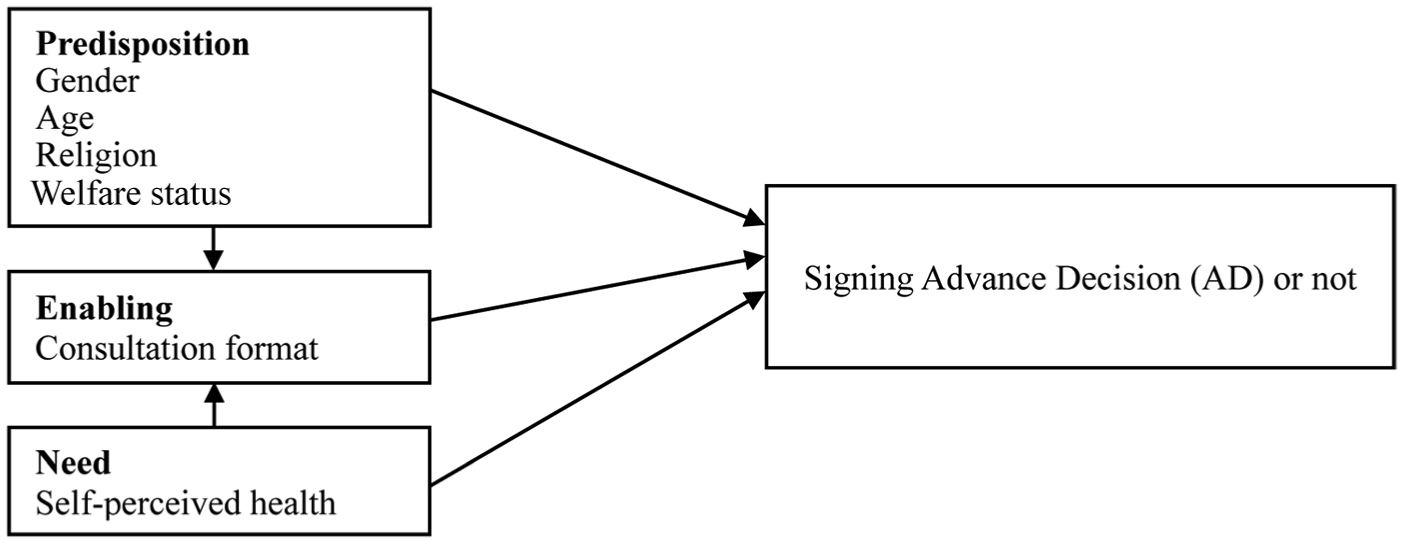
Research framework for examining factors influencing AD completion among participants in group-based and individual-based ACP consultations in Taiwan (2021–2022).
Ethical considerations
The research protocol was reviewed and approved by the Institutional Review Board of Taipei City Hospital (IRB No. TCHIRB-11305017-E). This study adopted a retrospective medical record analysis, conducted in accordance with medical ethical procedures, and received permission from the data management unit to access the required data. All data were fully de-identified prior to analysis, ensuring that no individual participant could be identified. The research data were accessible only by the research team and were securely stored. As this study was retrospective in nature, it utilized only existing data and did not involve any direct intervention or risk to participants. Data collection was concluded once all necessary information had been obtained, without the need for premature termination.
Results
Descriptive statistics
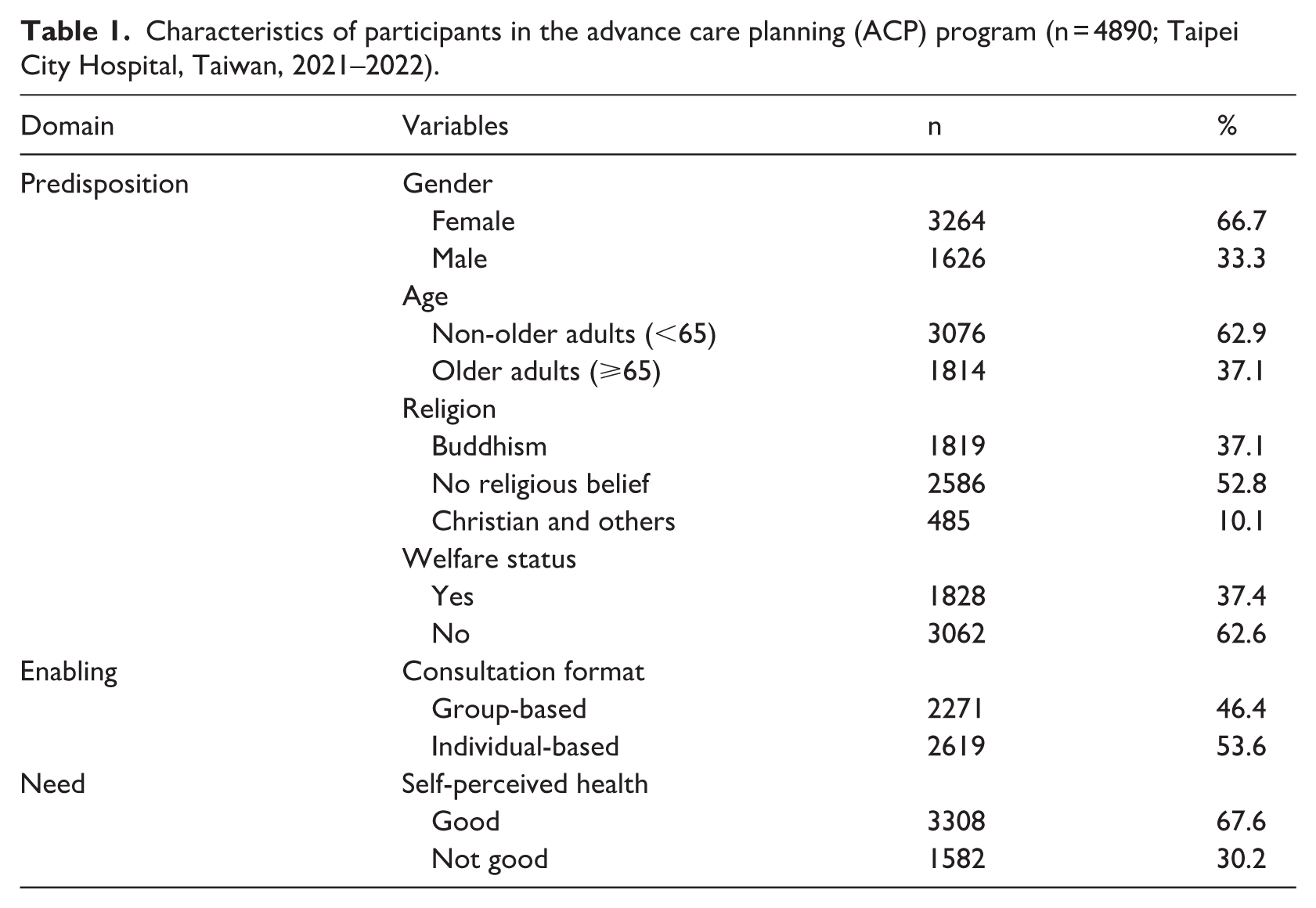
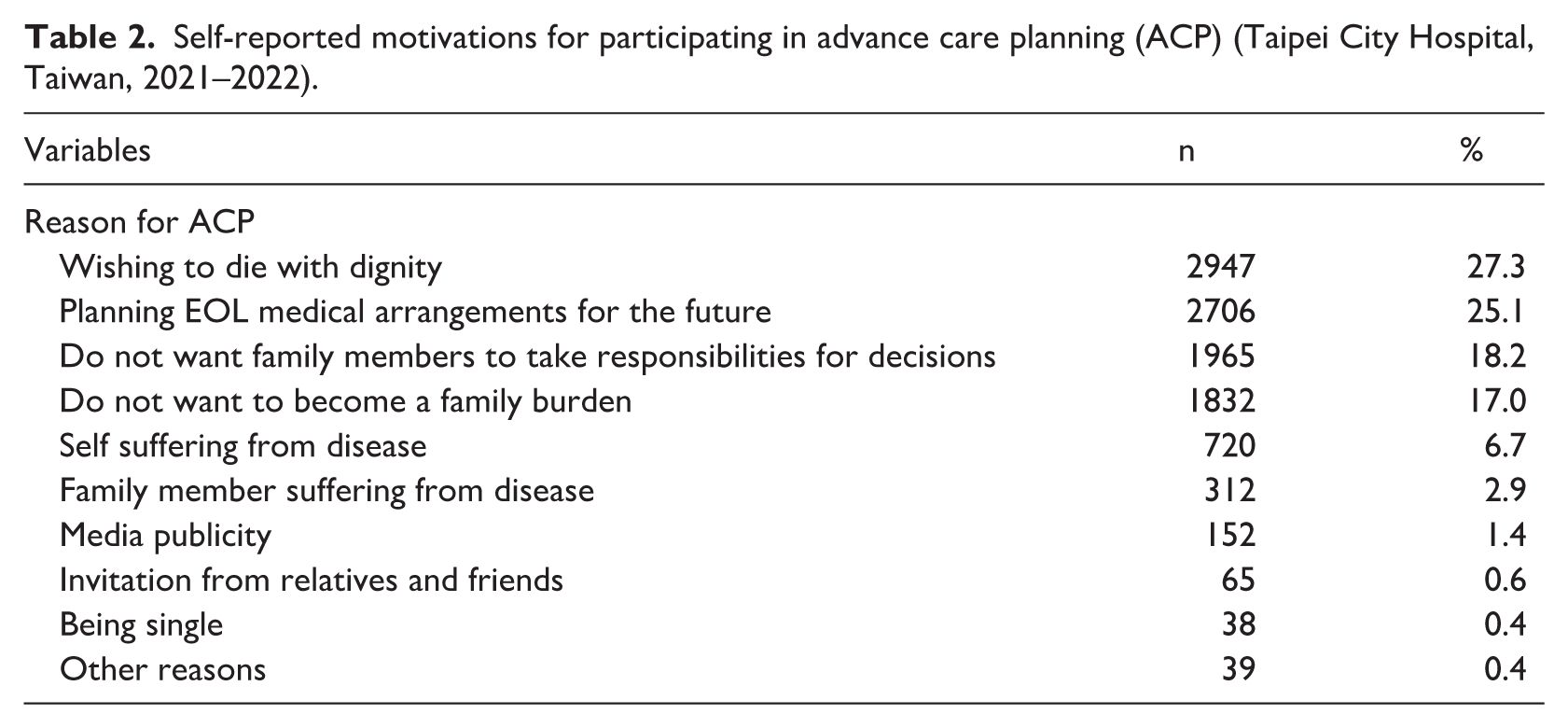
The study sample comprised 4890 participants who completed ACP consultations. The majority were female (66.7%) and non-older adults (62.9%). Over half of the participants reported having no religious belief (52.8%), while Buddhism was the most common religion (37.1%) among those with religious belief. Participants without registered welfare status accounted for 62.6% of the sample. In terms of consultation format, 53.6% attended individual-based sessions, whereas 46.4% participated in group-based consultations. Most participants (67.6%) perceived their health status as good (Table 1). The study also explored participants’ motivations for engaging in ACP consultations. The most commonly cited reason was the desire to die with dignity, followed by the intention to plan for future EOL medical arrangements (Table 2).
Characteristics of participants in the advance care planning (ACP) program (n = 4890; Taipei City Hospital, Taiwan, 2021–2022).
Self-reported motivations for participating in advance care planning (ACP) (Taipei City Hospital, Taiwan, 2021–2022).
Bivariate analysis
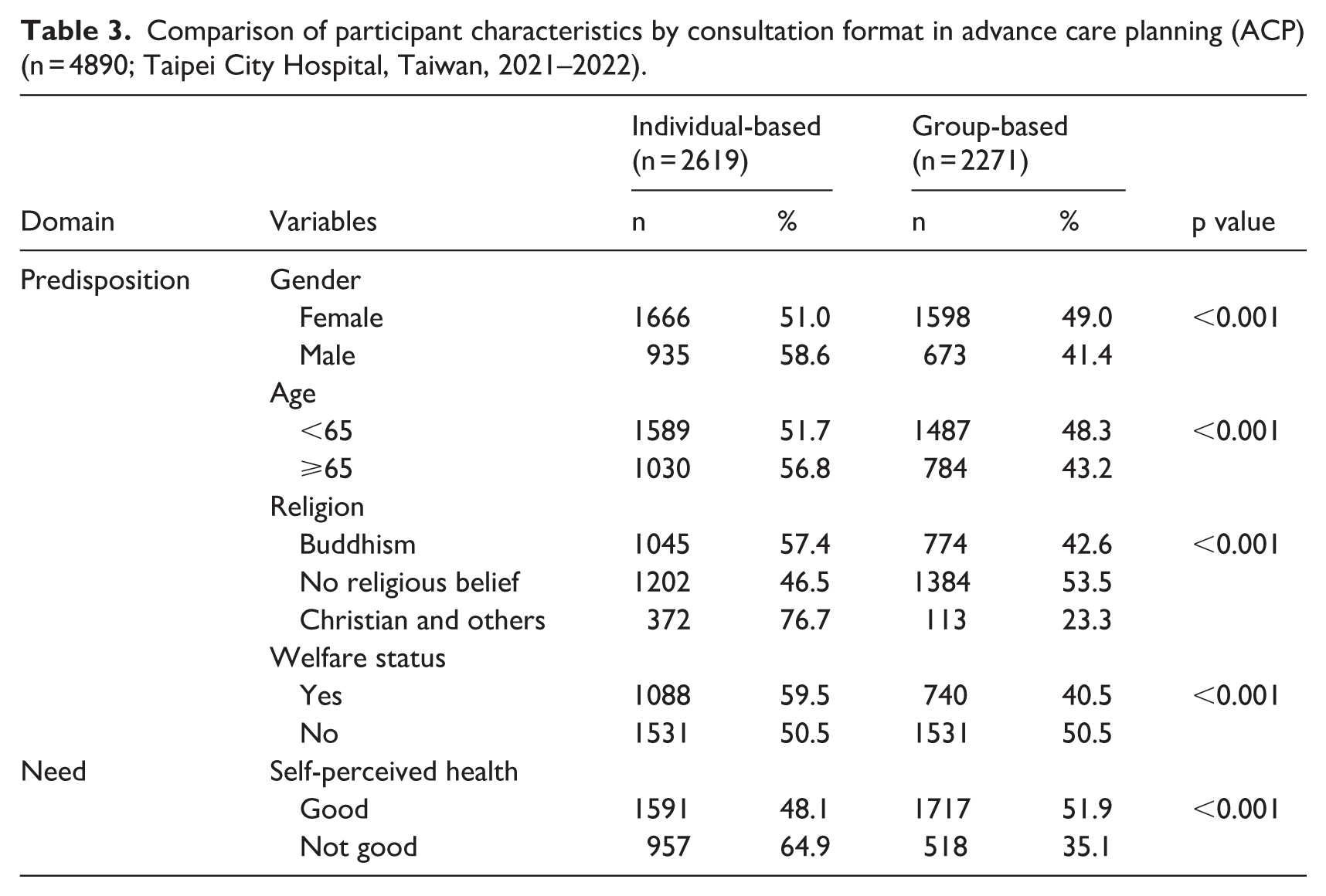
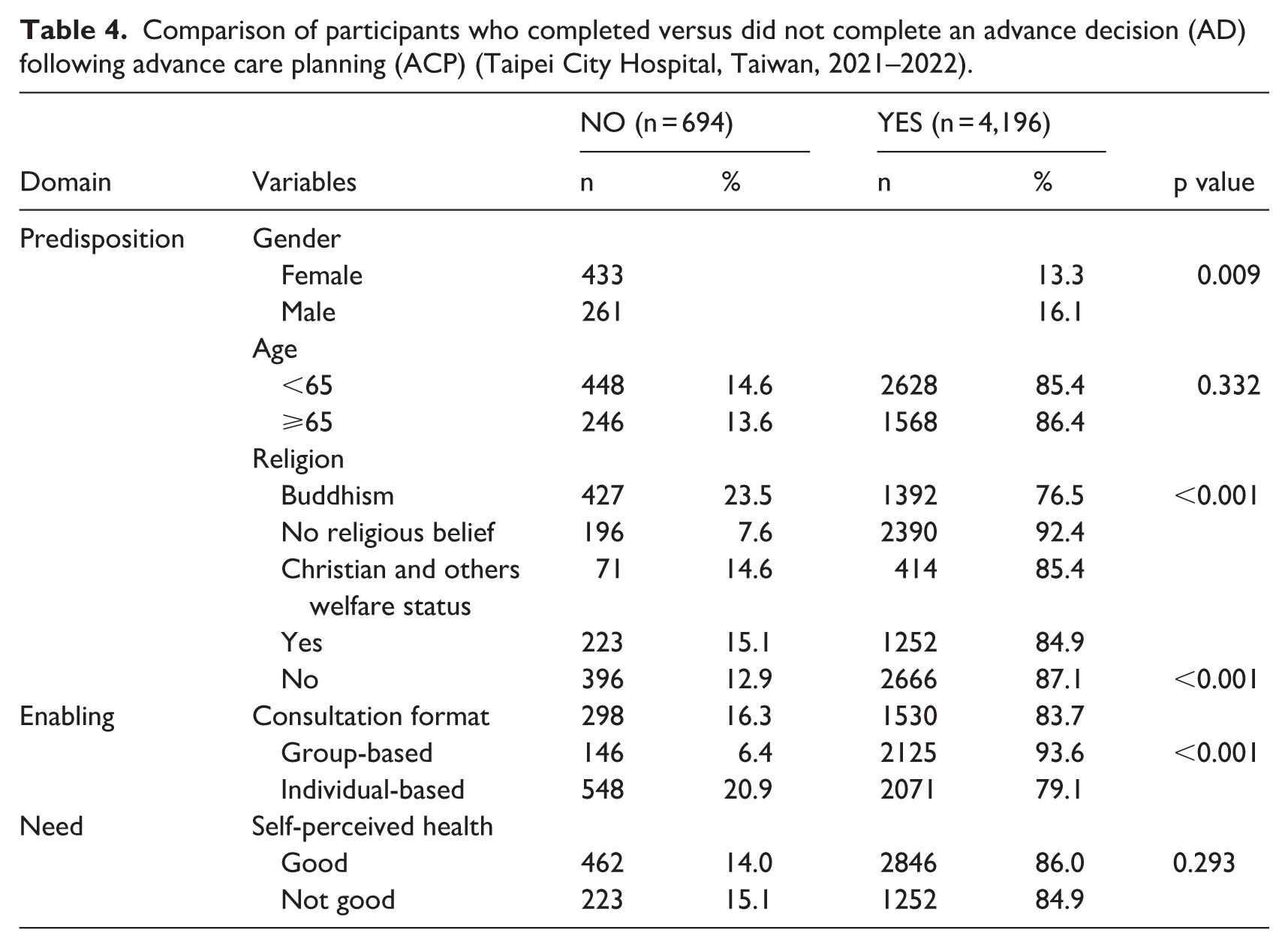
Bivariate analysis using chi-square tests was conducted to examine five variables related to predisposing and need factors. The results revealed significant differences across all examined variables between participants who attended group-based consultations and those who participated in individual consultations, indicating distinct demographic characteristics associated with the choice of consultation type (Table 3). In addition, comparisons were made between participants who completed an AD and those who did not. Significant differences were found in all predisposing variables, except age, as to whether the AD was completed. However, perceived health did not play a notable role in the decision-making process regarding the completion of an AD in this study (Table 4).
Comparison of participant characteristics by consultation format in advance care planning (ACP) (n = 4890; Taipei City Hospital, Taiwan, 2021–2022).
Comparison of participants who completed versus did not complete an advance decision (AD) following advance care planning (ACP) (Taipei City Hospital, Taiwan, 2021–2022).
Logistic regression analysis
To examine the influence of various factors on the completion of ADs and to explore differences across participant characteristics, logistic regression analyses were conducted. The sample was divided into two groups—group-based consultation and individual-based with separate models estimated for each group followed by a model of the overall sample. In the group-based consultation analysis, religion and gender emerged as significant predictors of AD completion (p < 0.001). Specifically, men were 1.6 times more likely to complete an AD than women. In terms of religion, Buddhists showed a significantly higher likelihood of completing an AD, compared to individuals without religious affiliation or those of other faiths.
For the individual-based consultation, religion, age, and welfare status were significant predictors. Consistent with the group consultation, Buddhists demonstrated the highest completion rates. Non-older adults were 0.83 times as likely to complete an AD compared to the older adults. In addition, individuals without welfare status were 1.26 times more likely to complete an AD than those receiving welfare support.
In the analysis of the overall sample, religion remained a highly significant factor. Moreover, participants who attended group-based consultations were 3.83 times more likely to complete an AD compared to those in individual-based consultations, signifying the stronger influence of the group setting on AD completion.
Two predictive models were constructed to assess the impact of these factors. Model 1, which included predisposing and need factors, yielded statistically significant results across all groups, though the explanatory power was modest. The individual-based consultation showed the lowest R² (0.035), followed by the overall sample (0.046), while the group-based consultation demonstrated a slightly higher R² (0.050). In Model 2, which incorporated enabling factors, the overall explanatory power increased notably, with an R² value of 0.134. These findings suggested that group-based consultations played a meaningful role in influencing participants’ decisions to complete an AD (Table 5).
Logistic regression analysis of factors associated with willingness to sign an advance decision (AD), stratified by consultation format (Taipei City Hospital, Taiwan, 2021–2022).
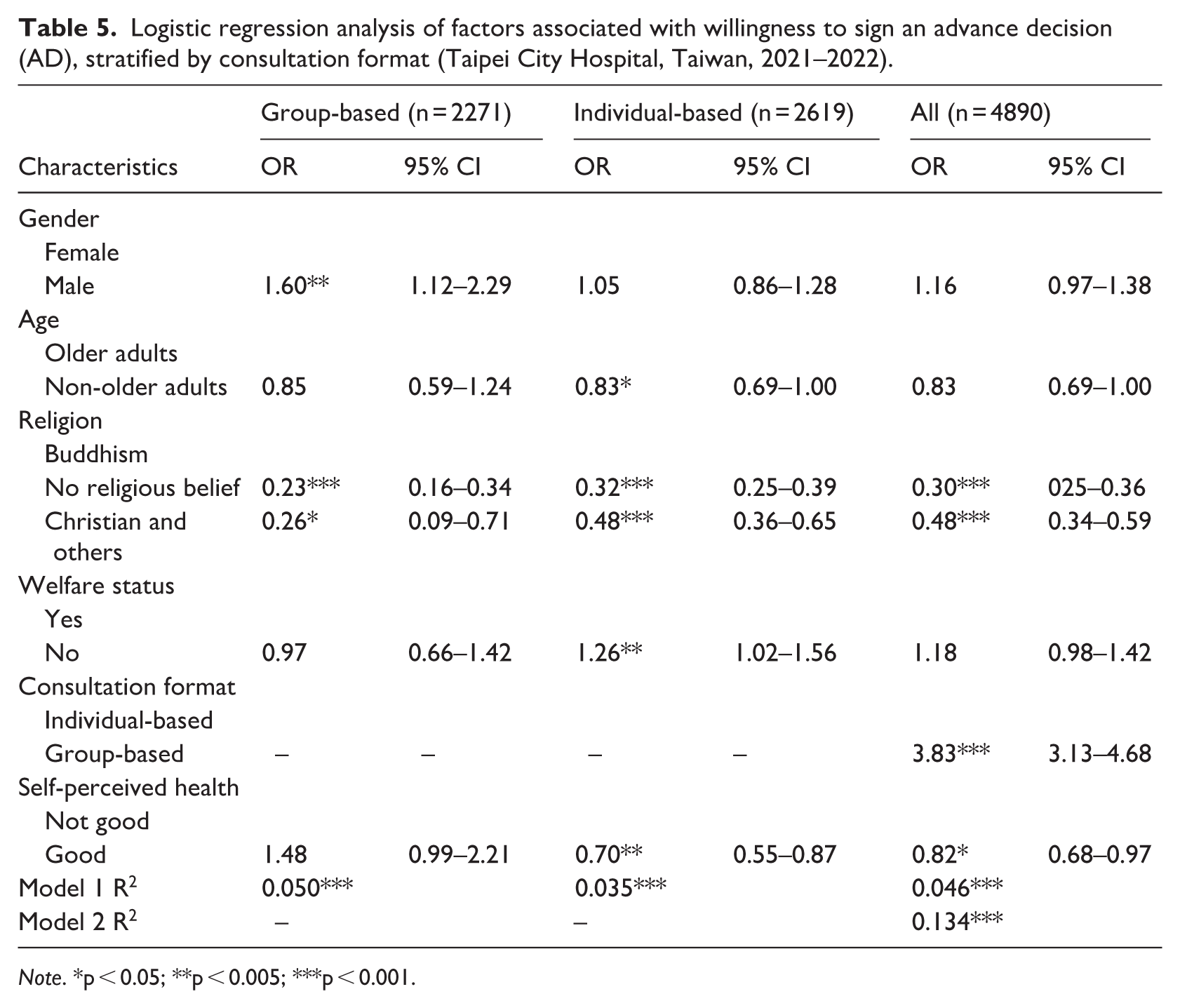
Note. *p < 0.05; **p < 0.005; ***p < 0.001.
Discussion
Results on predisposing factors for ACP participation
The study’s findings revealed that a significant proportion of participants in ACP group-based consultation were female, non-older adults, individuals without welfare status and those with good self-perceived health. The higher participation rate among women aligned with previous research, which indicated that women were generally more proactive in health-related planning and discussions (Inoue, 2016; Lum et al., 2017). Similarly, the greater willingness of non-older adults to engage in ACP was consistent with prior studies. Younger adults tended to be more receptive to ACP-related knowledge and were more interested in discussing autonomous medical decision-making (Kavalieratos et al., 2015). In contrast, older adults might face barriers such as limited health literacy, restricted access to relevant information, or discomfort discussing EOL issues (Ke et al., 2017; Shen et al., 2020; Simon et al., 2015; Wang et al., 2024).
Previous studies had also identified several reasons why individuals with low income were less likely to participate in ACP, due to challenges such as a lack of family support, low self-esteem, reduced motivation, and limited access to resources (Kimpel et al., 2022). Our findings indicated that, with regard to health status, individuals who perceived themselves as healthier appear more willing to engage in ACP. Since ACP involved sensitive topics, individuals who felt anxious or unprepared might avoid discussing such issues with their families (Brighton and Bristowe, 2016). These findings suggest that ACP interventions may be more effective when initiated earlier, rather than being limited to hospital settings. Specifically, ACP discussions may be better introduced when individuals are relatively healthy, confident, and psychologically prepared to engage in future care planning. This also aligns closely with current national policies in Taiwan, particularly the “Healthy Taiwan” initiative and Long-Term Care 3.0, both of which emphasize healthy aging and the extension of healthy life expectancy as core visions (Ministry of Health and Welfare R.O.C., 2024). From an implementation perspective, ACP services should be conceptualized and delivered as an integrated continuum, encompassing community outreach, pre-ACP preparation, and formal ACP consultations. To enhance accessibility and implementation efficiency, community-based infrastructures—such as community care stations and LTC facilities—may serve as key delivery platforms and appropriate units for program implementation and subsidy allocation. In this way, ACP promotion can be integrated into existing community care systems and function synergistically with national health and LTC policies.
Motivations for ACP participation
In all variables of motivations, to die with dignity was a central motivation not only reflecting societal values but also aligned with previous research findings (Detering et al., 2010) that the promotion of ACP was primarily aimed at making arrangements for a dignified EOL. Another significant motivation for ACP participation was the wish to alleviate the decision-making burden on family members. This concern was rooted in Taiwanese and broader Asian cultural norms, where familial roles and responsibilities were highly valued. In many Asian societies, it was common for EOL decisions to be made by family members rather than the individuals themselves (Cheng et al., 2020). The findings of this study not only demonstrated the necessity of including second-degree relatives in ACP consultations of the PRAA but also reflected the cultural and social importance of familial participation in EOL care in Asia culture.
Effectiveness of group-based consultations interventions
This study indicated that the AD completion in the group-based consultation setting was significantly higher than in the individual format. Our findings were consistent with previous research, which has suggested that the group dynamics, shared disease experiences and a supportive environment are key factors encouraging patients to express their thoughts (Ahluwalia et al., 2021; Bandini et al., 2021). From a cultural perspective, discussing death with family members has traditionally been avoided in many Asian societies; however, ACP serves not only as an opportunity for transformation but also as an effective medium for family discussions (Fan and Kao, 2024; Hsu et al., 2020; Yang et al., 2020). Despite the traditional emphasis on patient self-determination in western medical decision-making, approaches that underscore the family as the fundamental social unit may facilitate decisions that better serve the client’s best interests (Ho, 2008). While there is no right or wrong answer, group-based consultations, which are often family-centered seeking collective answers in nature, may allow the Confucian or Buddhist in nature to depict death as a cyclic process in life (Lin and Lwin, 2026). As a result, the findings demonstrated group-based consultations attracted participants with diverse demographic characteristics and engaged individuals who were previously less interested in ACP-related discussions. In addition, previous studies have highlighted the need for consultation formats tailored to different demographic groups (Tsai and Yang, 2019; Yang et al., 2020). Therefore, the present findings highlight the potential of group-based ACP as a culturally adaptable model that bridges individual autonomy, social support and family-centered decision-making in diverse healthcare settings.
Factors influencing the completion of advance direction after engaging in ACP
Religious belief has been identified as a significant predisposing factor in both previous studies and the present research. Our study specifically found that Buddhists were more likely to complete an advance directive than individuals from other religious backgrounds. In Buddhism, contemplating the nature of death and what happens afterward is a central doctrinal theme, suggesting that life involves reincarnation, or the rebirth of a soul into another body (Bülow et al., 2008; McCormick, 2013). In western countries, previous studies have indicated that the Mainline Protestants show higher rates of advance directive completion than other Christian groups, such as Evangelicals and Catholics (Huang et al., 2016). Similarly, research conducted in Kenya indicated that knowledge regarding AD varied across religious groups (Oshow et al., 2024). Religious beliefs can help individuals express their care preferences and facilitate the completion of advance directives (Bülow et al., 2008; Dronamraju et al., 2022; Lum et al., 2017; Stewart et al., 2013). Religion may also help individuals clarify their values and expectations regarding life and death, thereby facilitating discussions about ACP and increasing the likelihood of completing advance directives (Miyashita et al., 2021). Future research could compare Buddhists and Mainline Protestants, which represent major religious traditions in eastern and western contexts, to further explore the core beliefs and meanings underlying religious adherence and their influence on end-of-life decision-making.
This study also found that individuals without welfare status were more likely to complete an AD than those with welfare status in the individual consultation format. This finding was consistent with previous research, indicating that individuals residing in neighborhoods with lower socioeconomic status were less likely to complete an advance directive (Nouri et al., 2020). However, prior studies had demonstrated that individuals with chronic or terminal illnesses were more likely to articulate their care preferences (Ko et al., 2016). Our study provided a more nuanced perspective. Specifically, we observed that participants with better self-perceived health were more likely to engage in ACP consultations. However, it was those with poorer self-perceived health who were more likely to complete an AD. This finding highlights the complex relationship between perceived health status and the actual decision to formalize EOL care preferences. A review of studies conducted in the United States on ACP and palliative care awareness indicated that while most individuals understood the concept of ACP, only a small proportion actually formalized their preferences through written directives. One key motivator for completing advance directives was negative past medical experiences, which served as catalysts prompting individuals to document their care preferences (Grant et al., 2021). In summary, when introducing ACP, it is essential to take into account patients’ current health and welfare status, as this approach can facilitate smoother implementation and greater public acceptance. These findings further supported the importance of introducing ACP earlier in the life course, rather than only at crisis points (Detering et al., 2010). From a social work perspective, practitioners may incorporate the 4R framework (Resources, Risks, Roles, and Relationships) in pre-ACP and ACP processes, as a structured assessment approach to promote preference-concordant decision-making. By systematically assessing the individual needs, available resources, and relational dynamics, social workers can better support clients and families in navigating complex end-of-life decisions while ensuring that care planning remains person-centered and context-sensitive.
Strengths and limitations
A notable strength of this study lay in its focus on a rarely implemented intervention model in Taiwan, as group-based ACP consultations have been reported in only two institutions nationwide according to the literature. This unique context offered valuable insights into the feasibility and cultural adaptation of such models within local healthcare settings. A primary limitation was that the study was conducted in a single public hospital within a specific district, which may limit the generalizability of the findings to other regions. This limitation was anticipated, as variations in the organization and delivery of group-based consultations exist across institutions, making it challenging to standardize and expand the sample nationwide within the study period. Nevertheless, approximately 32% of all ADs in Taiwan were completed in Taipei City hospitals (Ministry of Health and Welfare, 2025), suggesting that the findings retain reasonable credibility and relevance despite the geographic limitation. Future research employing prospective randomized controlled trials with primary data is warranted to further examine the magnitude of these differences and clarify the mechanisms influencing individuals’ engagement in ACP. In addition, future studies could explore additional demographic and needs-based factors, including education level, socioeconomic status, and illness characteristics. Moreover, adopting qualitative approaches, such as simulated or in-depth interviews, could help uncover the underlying motivations for participating in group-based consultations and reveal how personal values and care preferences are expressed in signed ADs.
Conclusion
This article highlights an innovative social worker-led, group-based consultation model that effectively engages participants from diverse demographic backgrounds. Internationally, ACP approaches are often disease-oriented or population-specific; however, this study suggests that a family-centered approach could provide a valuable alternative, particularly in collectivist cultural contexts. While certain variables, such as religion, self-rated health status, and welfare status, were found to be significant, these factors should be considered in both ACP and pre-ACP processes, as well as in policy development, in order to effectively promote the expression of advance care preferences and the completion of advance directives.
Footnotes
Acknowledgements
We sincerely thank the Department of Social Work at Taipei City Hospital for their support in organizing and implementing the ACP consultations.
Special thanks are extended to Deputy Director Ching-Nu Liu for her assistance in reviewing and verifying the accuracy of the data used in this study.
We are also grateful to Dr Da-cheng Qu, former Superintendent of Taipei City Hospital, for his administrative support and for promoting this research initiative.
We further acknowledge Professor Pesus Chou of National Yang Ming Chiao Tung University and Professor Ming-Chin Yang of National Taiwan University for their insightful suggestions during the initial stages of this research.
Ethical considerations
This study was approved by the Taipei City Hospital Institutional Review Board (IRB No. TCHIRB-11305017-E).
Consent to participate
All participants provided informed consent before participating in the ACP consultations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data underlying this study were obtained from Taipei City Hospital and are part of patients’ medical records. Due to privacy and ethical considerations, these data cannot be shared publicly. Data access may be granted upon reasonable request to the corresponding author and with permission from Taipei City Hospital.
Statement on AI
This manuscript was prepared with the assistance of Chat GPT as a language tool for grammar checking and language polishing and some of the reference translate and finding some references. All AI-assisted outputs were reviewed and validated by the authors for accuracy.
Statement on written informed consent
This study used secondary data from Taipei City Hospital, which were fully anonymized before the authors accessed them. According to the approval from the Institutional Review Board of Taipei City Hospital, individual informed consent for participation and publication of personal data was not required.
Statement on interview questions
This study involved secondary data analysis and did not include any interviews. Therefore, no interview questions were developed or used.