
Abstract
Online mental health peer support is a developing approach which appeals to young people and also contributes to central challenges and possible opportunities for social work practice. This quantitative study explored the use of online peer support and youth mental well-being in Northern Ireland and China and examined potential factors associated with the selection of online peer support. The findings revealed a country-specific disparity in the use of online peer support. Social work practitioners should be aware of the potential of online peer support for youth mental health as an accessible supplement to traditional services.
Keywords
Introduction
Mental health is a significant health concern for young people. Globally, one in seven 10–19-year-olds experiences a mental disorder, increasing the global burden of disease in this age group (World Health Organization, 2024). The Lancet Psychiatry Commission on youth mental health (McGorry et al., 2024) also reported that mental illnesses tend to have a peak age of onset at around 15 years, with 63% to 75% of cases emerging by the age of 25, and prevalence rates appear to have been increasing across many countries over the past 20 years. These high rates of mental health problems have been identified in Northern Ireland (NI) and China. In NI, the Young Persons’ Behaviour and Attitude Survey (Northern Ireland Statistics and Research Agency, 2023) indicated that 21% of young people experienced depression or anxiety in the past 12 months. Meanwhile, UNICEF China (2021) demonstrated that almost 25% of young people in China felt mild or severe depression and estimated that at least 30 million young people under 17 years old were struggling with emotional or behavioural problems. However, a significant proportion of young people do not seek professional help (Birrell et al., 2023; Horgan et al., 2013). Some barriers to help-seeking have been identified, including services being too formal, inaccessible and inadequate (Tatlow-Golden and McElvaney, 2015); wider societal issues about stigma and mental health (HSC Public Health Agency, 2025) may contribute to these services not being sufficiently resourced. It has also been reported that young people are frequent users of the Internet, with an increasing number of young individuals turning to alternative online support for mental health issues (Ali et al., 2015; Lau et al., 2024). Ashcroft et al. (2018) highlighted the pivotal role of mental health social workers within primary health care settings, emphasising their contribution to addressing patients’ psychosocial needs. However, a marked increase in mental health issues among young people and a shift of services from in-person to online have created more complicated challenges for mental health social workers, such as workload, ethical problems and adaptive skills (Gilson et al., 2024). Meanwhile, defining the role of mental health social workers in developing online services is an urgent matter.
Peer support is a promising aspect of digital mental health interventions, offering a valuable addition to traditional mental healthcare services (Coote et al., 2024). In recent years, eight specific types of online peer support have emerged, such as forums, message boards (asynchronous, moderated and general or specific) and mental health apps (asynchronous and synchronous, moderated and specific) (Yuan et al., 2026). Consequently, young people are presented with opportunities and space to receive and provide support for others with shared experiences (including mental health issues and experiences of seeking help from services). There are five main potential mechanisms for how online peer support may help. It provides opportunities for unidirectional and reciprocal interaction, information about mental health, understanding and shared experiences, social support, and an online community environment (Kotera et al., 2025; Pavarini et al., 2023; Yuan et al., 2025). Pavarini et al. (2024) found online peer support could improve mental well-being (MWB), social connectedness and self-esteem in both quantitative and qualitative results. The outcomes in self-reported well-being, connectedness with online peers and self-esteem were each significantly higher among the intervention group compared to the control group, according to different scales in the posttest. In qualitative analysis, participants reported that they learnt helpful skills and developed new connections, as well as improved existing friendships through courses, and were empowered to help themselves and provide support to others, which directly promotes general MWB. The effectiveness of online peer support has also been identified by a further quantitative study, which has the potential to reduce depression, anxiety and nonsuicidal self-injury (Van Meter and Agrawal, 2024). Early studies demonstrated the overall benefits and potential of online peer support, promoting clinical and personal recovery and offering a positive experience for young participants worldwide (Ludwig et al., 2020; Van Meter and Agrawal, 2024), although it is also acknowledged that this form of support may not work well for everyone and in all contexts (Marshall et al., 2024). It has been observed that the effectiveness of online peer support might be influenced by country-specific factors, particularly in the context of Western and Eastern countries (Yeo et al., 2025). In terms of early digital mental health interventions, culturally influenced mental health literacy and stigma have been validated as significant barriers to engagement (Jardine et al., 2023). Furthermore, a comparative qualitative analysis indicated a notable distinction in the discourse observed among UK and US open mental health-related Facebook groups. Users from the United Kingdom prefer choosing self-disclosure as a means of addressing mental health challenges, while US users might engage in discussions about contemporary articles and news narratives to eliminate stigma shrouding mental health issues (Prescott et al., 2020). However, previous research into online peer support, including cross-country comparisons, has targeted the general population rather than young people. Our research team is based in NI and China, and so data collection was focused on these settings to provide a comparison between these Western and Eastern cultural contexts. To date, no article has demonstrated the online peer support usage and addressed the mental health issues among young people to promote MWB in NI and China to better understand global mental health challenges and the cultural adaptability of online peer support at a global level. Therefore, the aim of this study was to explore the use of online peer support as well as MWB, especially in NI and China, and to identify key factors associated with online peer support use, and the research questions were as follows:
To what extent do young people use online peer support for mental health issues?
Is there any difference in online peer support use in NI and China?
How does MWB based on 12-item General Health Questionnaire (GHQ-12) scores vary across genders and the experience of online peer support use in NI and China?
Does time spent on peer support influence GHQ-12 scores?
What factors predict the choice of online peer support among young people?
Methods
Research design
A comparative cross-sectional design was employed in this quantitative study. Data were collected using survey methodology on the MWB and online peer support use of young people in NI and China. A survey was selected to gather data from a potentially representative sample and also to facilitate anonymity to enhance the authenticity of responses on this potentially sensitive subject.
Sample and data collection
Eligible participants for this study were young people aged 18–25 years living or studying in NI and China. Although the term ‘young people’ typically refers to those aged 12–25 years (Thorn et al., 2023), some individuals under the age of 18 do not have full access to digital tools and are still under parental supervision for various reasons, leaving them with limited time to connect with others online. Furthermore, turning 18 marks a significant transition into adulthood for most young people. Individuals leave their familiar homes and parents to attend universities, which provide a completely new environment where they must live independently. This transition can be challenging, as they face academic demands, social activities and personal responsibilities that may increase the likelihood of developing mental health issues. Meanwhile, they also have the freedom to make their own choices, including the use of electronic devices. Therefore, young individuals are more willing to explore and select their preferred online platform.
The sample population were recruited from 11 August 2024 to 12 February 2025 via two pathways: (1) a general recruitment strategy involved the utilisation of social media platforms (e.g. Instagram, Facebook, X, TikTok, Reddit, Rednote and Weibo) and email to enhance awareness and identify potential participants. In addition to this, offline strategies were also employed, including posters with QR codes linking to online surveys that were distributed on campus at Queen’s University Belfast and Qingdao University of Science and Technology, using convenience sampling to identify young individuals who had experience of online mental health peer support; (2) specific recruitment involved contacting relevant mental health organisations and charities, requesting their assistance in contacting participants through young people they had already served, their online accounts, websites and online peer support groups they held. The minimum sample size was determined, using Raosoft’s sample size calculator, based on a margin of error of 5% and confidence level of 95%, as 377 young people in each country.
Measures
Mental well-being
The GHQ is a tool designed to assess current mental health and has been widely utilised in diverse settings and different cultural contexts (Montazeri et al., 2003). A shortened version, the GHQ-12, was employed in this study to identify potential mental health problems for young people. Each item has four answers (not at all, less than usual, no more than usual and much more than usual) and can either be scored based on a 0–12 scoring system (0-0-1-1) and 0–36 scoring system (0-1-2-3). The two scoring systems mean the data can be used in different ways. Both scoring systems were employed in this study. The mean scores from the 0 to 36 scoring system can be compared across different groups (e.g. female vs male). At the same time, based on a 0–12 scoring system, a score of 4 or more indicates a possible mental health problem or ‘caseness’.
Ethical considerations
Participation in the survey was voluntary. Participants would be accessible to the survey after choosing ‘I agree’ in the consent form on the first page of the survey. The surveys were administered through Microsoft Forms. It is important to stress that the confidentiality of respondents was protected, as no personally identifiable information was provided by them. Meanwhile, to ensure the psychological safety of participants, they were informed at the beginning of the online survey that they could stop at any point in the process. Furthermore, information was provided about where participants can access relevant support in case any discomfort is experienced during the online survey. The study received ethics approval from the School of Social Sciences, Education and Social Work Ethics Committee of Queen’s University Belfast.
Analysis
The SPSS v26.0 was used for statistical analysis (Pallant, 2020). The following tests reported in this article included the Mann–Whitney test, Pearson correlation test and Spearman’s rho correlation test for correlational analyses and binary logistic regression, which was conducted for predicting the use of online peer support in the future.
Results
There were 872 completed and valid survey questionnaires. The design of the survey included that you were only able to submit your responses at the end of the survey, which may have helped prevent incomplete survey responses and missing data. On the other hand, this means that it is not possible to identify how many additional people may have started the survey and not completed it.
Demographics and participant characteristics
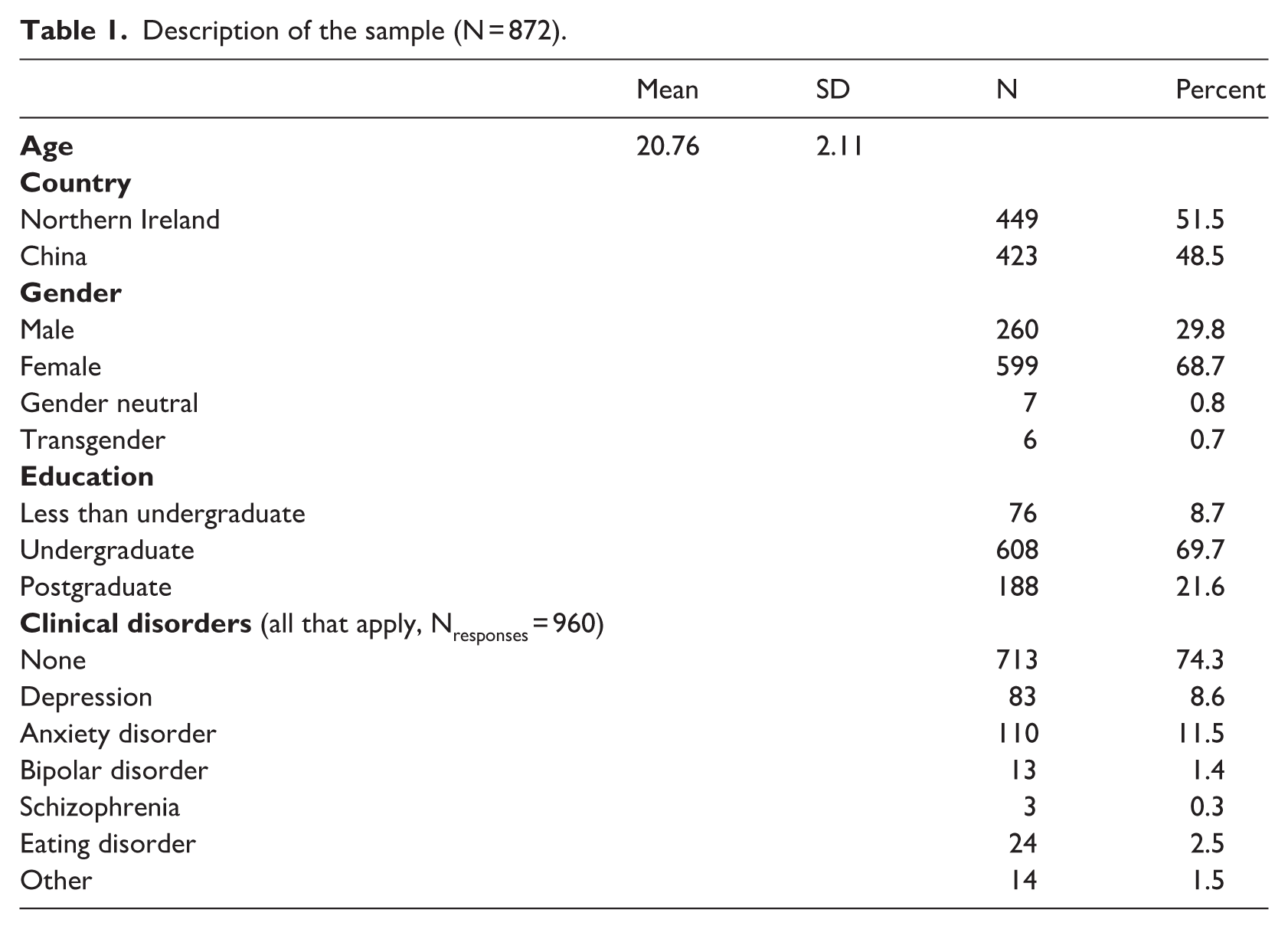
During the 2-month survey period, 872 young individuals, with 449 participants from NI and 423 participants from China, responded to the online survey either using a web link or scanning the QR code. The mean age of the participants was 20.76 (SD = 2.11), and 68.7% (n = 599) were female. The majority of young individuals (n = 608, 69.7%) studied at the undergraduate level (Table 1). Due to low numbers in other gender identity categories, they were considered only at the descriptive analysis stage. Inferential analysis was limited to male and female participants.
Description of the sample (N = 872).
To what extent do young people use online peer support for mental health issues?
The respondents’ online peer support use is summarised in Table 2, with 318 of 872 participants (36.5%) reporting they had some experience of online peer support use for mental health issues. The mean age of first use of online peer support among participants was 16.77 (SD = 3.05). Of those struggling with mental health issues 61.6% (n = 196) used online peer support less than once or once a week, with 30.2% (n = 96) using it two to five times a week. In terms of duration of use, young participants mostly use less than 30 minutes (n = 142, 44.7%) or 30–60 minutes (n = 131, 41.2%). Moreover, social media (n = 272, 59.8%) was the first choice of peer support platforms, followed by online forums (n = 66, 14.5%) and online peer support groups (n = 51, 11.2%).
Usage of online peer support by young participants (N = 318).
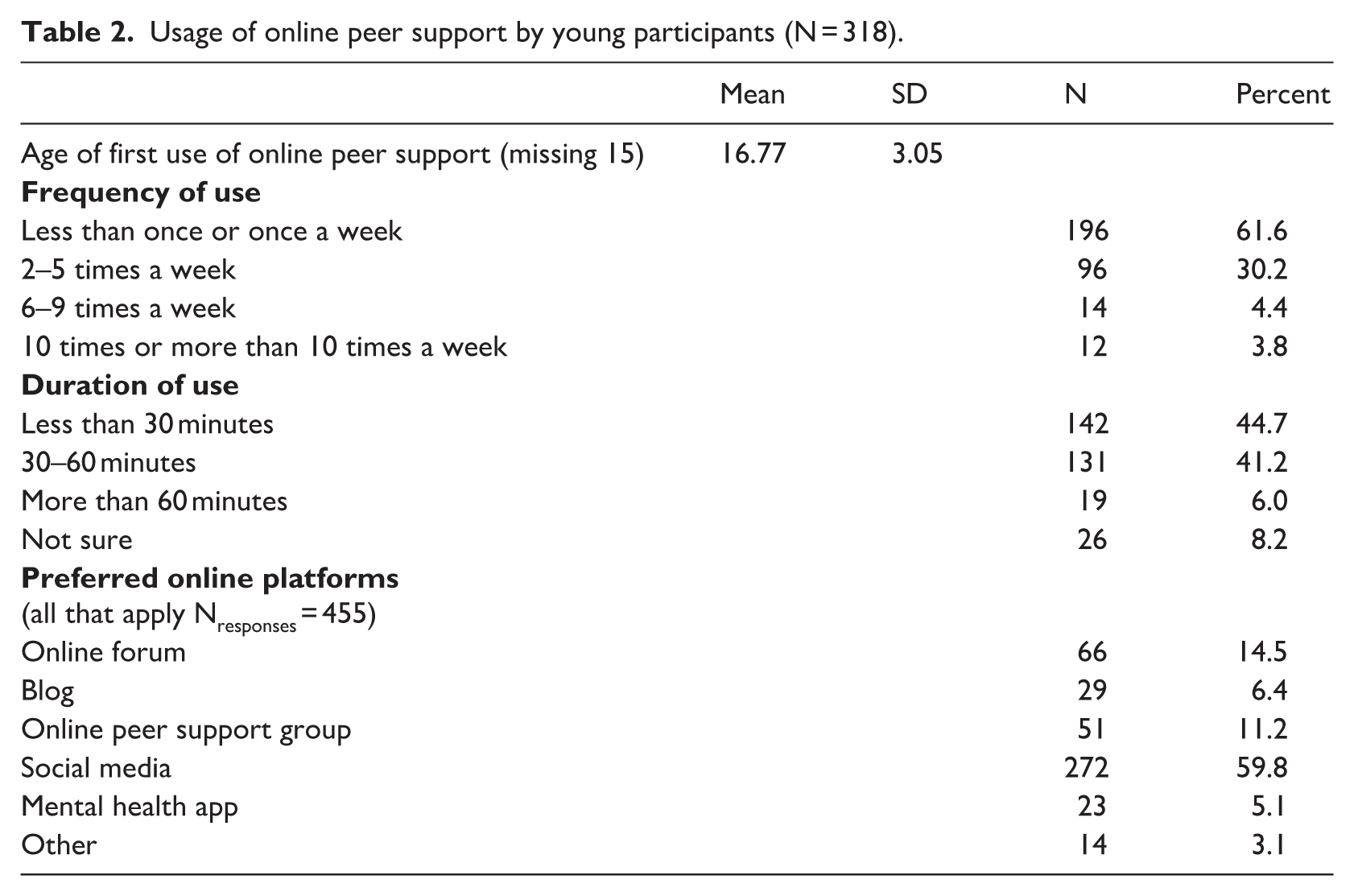
Of the total number of respondents, 318/872 (36.5%) reported that they had some experience of online mental health peer support. Table 2 provides more information about their experience and use of online peer support.
Of a sample of 872, 554 participants had no experience of online mental health peer support. They were asked to identify reasons for not accessing online peer support and possible barriers; multiple answers were allowed. The identified barriers are presented in Figure 1. No mental health issues were the primary reason (n = 306, 36.1%), followed by a lack of trust in the cyber environment (n = 138, 16.3%) and a lack of specific knowledge of online peer support (n = 107, 12.6%).
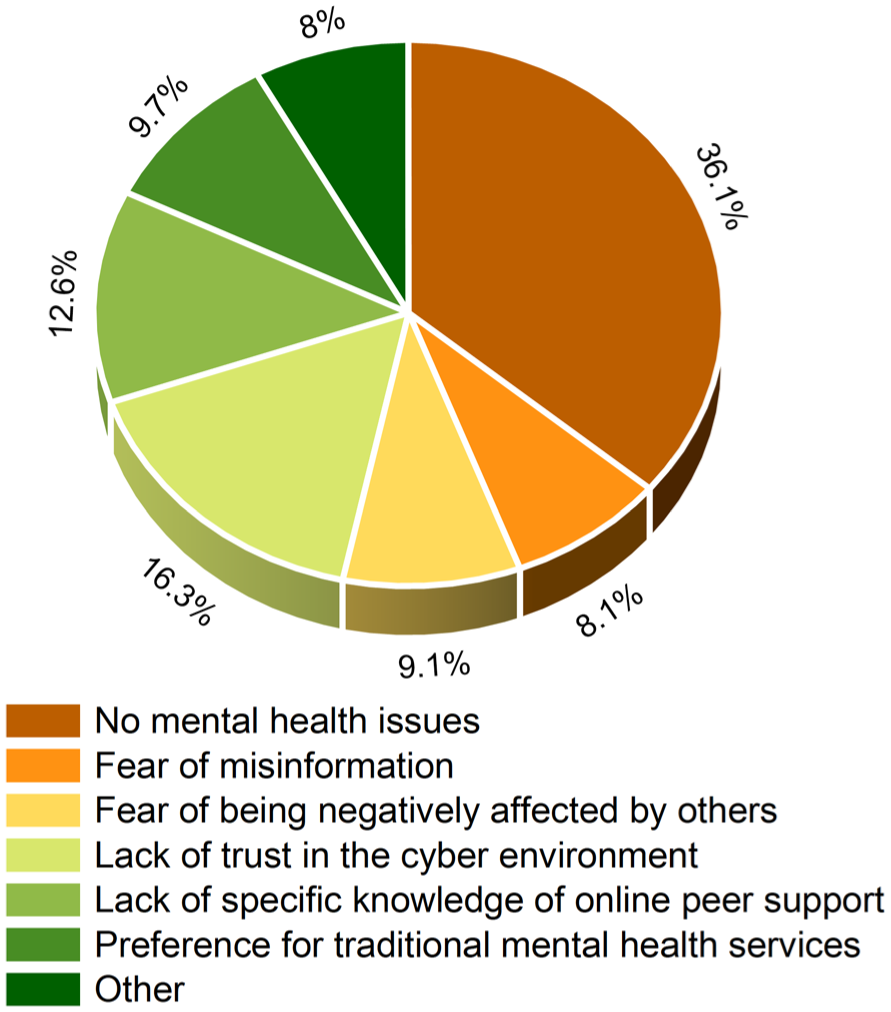
Possible barriers prevent young participants from choosing online peer support for mental health problems.
Is there any difference in online peer support use in NI and China?
The mean age of first use of online peer support in China was 2 years older than that in NI. More than half of participants used online peer support less than once or once a week, with 69/105 (65.7%) and 127/213 participants (59.6%), respectively, in NI and China; 23.8% (n = 25) of young individuals struggling with mental health problems in NI and 33.3% (n = 71) in China sought support 2–5 times a week. Afterwards, participants were asked about the duration of use; less than 30 minutes (n = 55, 52.4%) was the preferred choice for most respondents in NI, followed by 30–60 minutes (n = 37, 35.2%), while patterns in China showed the reverse trend.
The question about frequently used online platforms allowed multiple selections. Social media remained the most popular platform of online peer support, with 64.9% (n = 96) and 57.3% (n = 176), respectively, in NI and China. Twenty (13.5%) and 46 (15%) young participants, respectively, chose the online forum to access support from others. Mental health apps (e.g. Calm Harm and SHaRON) attracted more young respondents (n = 15, 10.1%) in NI, while in China, the online peer support group (n = 39, 12.7%) was the third choice of respondents with mental health problems.
How does MWB based on GHQ-12 scores vary across genders and the experience of online peer support use in NI and China?
Based on the 0–12 scoring system, scoring 4 or more accounted for 69.38%, which indicates probable mental health problems in more than half of the respondents. The overall mean score from the 0 to 36 scoring system was 15.72, and the mean score for females was slightly higher than that for males (15.84 and 15.21, respectively); based on the 0–12 scoring, the proportion of females with probable mental health problems was lower than that for males (69.11 and 69.23, respectively).
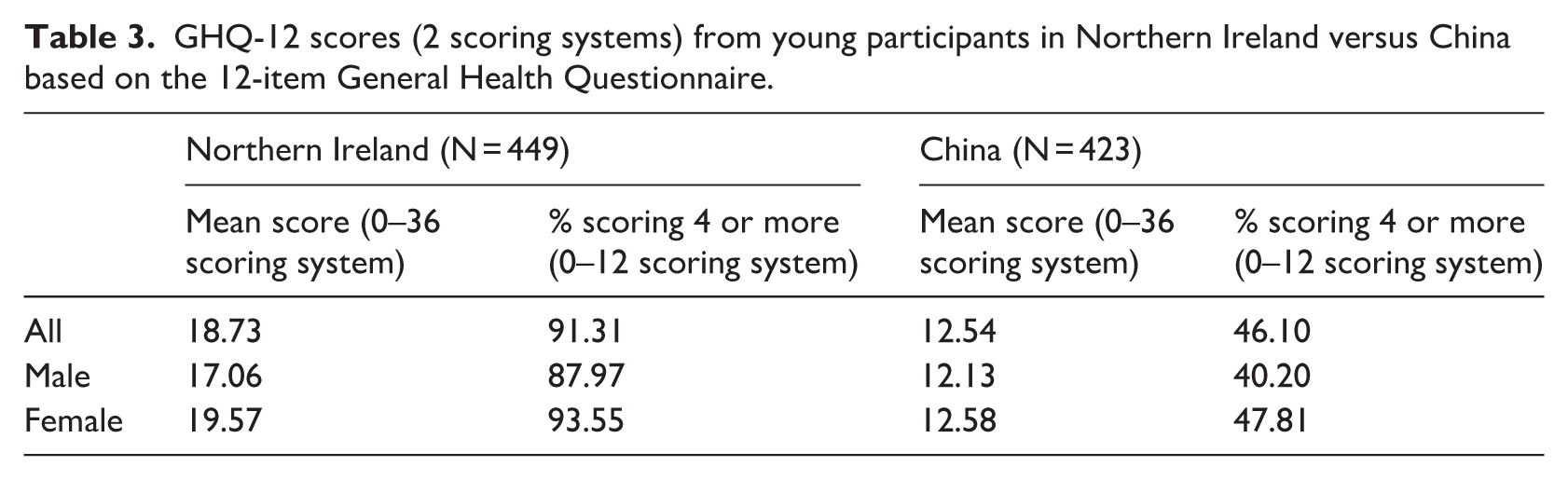
A Mann–Whitney U test was performed to compare the difference in GHQ-12 scores for males and females. There was no significant difference in scores between groups (U = 74,066.500, p = 0.254, r = 0.039). Therefore, gender was not associated with GHQ-12 scores among young people. Similarly, a Mann–Whitney U test was also employed to compare the difference in GHQ-12 scores for those who had some experience of online peer support use and those who did not. No significant difference was found in scores between groups (U = 83684.500, p = 0.711, r = 0.013). Consequently, using online peer support for mental health issues was not associated with differences in GHQ-12 scores among respondents in this article. Further, the Mann–Whitney U testing demonstrated a significant difference in GHQ-12 scores for young participants in NI and China (U = 45265.500, p < 0.001, r = 0.441). Table 3 shows the detailed difference in GHQ-12 scores between countries. The mean score of all samples, females and males, in NI was higher than that in China. It is noted that the mean score for females was the highest, even exceeding that for the total sample in both countries. In terms of possible mental health problems or ‘caseness’, the figure in NI was almost twice that in China.
GHQ-12 scores (2 scoring systems) from young participants in Northern Ireland versus China based on the 12-item General Health Questionnaire.
Out of 449 respondents in NI and 423 respondents in China, 39 and 16, respectively, provided multiple responses to a multiple-choice question related to clinical disorders. Results showed for both NI and China that the majority of respondents didn’t have clinical disorders (n = 334, 66.7% and n = 379, 84.4%, respectively). Anxiety disorder (n = 89, 17.8%) was the main clinical disorder in NI, while in China, it was depression (n = 54, 6.5%).
For young participants, especially those who were studying at university, academic challenges were the primary cause of mental health issues for both countries, with 34.3% (n = 341) in NI and 27.3% (n = 287) in China. Relationship struggles came in second place; 16.6% (n = 165) of NI participants were troubled by relationship issues, with 19.1% (n = 201) in China. Life obstacles and career setbacks ranked as the third most significant source of mental health issues among respondents in NI and China, respectively (n = 144, 14.5% and n = 169, 16.1%). This question regarding the possible causes of mental health problems was a multiple-response item, allowing respondents to select more than one answer, and no missing data were observed.
Does time spent on peer support influence GHQ-12 scores?
The data regarding the frequency of online peer support use on GHQ-12 scores were normally distributed, while the data relating to the duration of use were not. Therefore, both Pearson’s correlation test and Spearman’s rho correlation test were utilised. Pearson’s correlation test indicated no significant relationship between GHQ-12 scores and frequency of online peer support use (r = 0.063, n = 309, p = 0.266). Meanwhile, no significant positive correlation between duration of use and GHQ-12 scores was observed in Spearman’s rho correlation test (ρ = −0.002, n = 309, p = 0.965). Although results from the two tests above were not significant, 303 of 318 respondents (95.3%) who had experience with online peer support held an optimistic view of its effectiveness in addressing mental health challenges.
What factors predict the choice of online peer support among young people?
A binary logistic regression analysis was conducted to predict the likelihood of using online peer support as a dependent variable related to sociodemographic characteristics (age, gender, country and education) and MWB factors (GHQ scores and clinical disorders). The overall model was statistically significant, χ2(7) = 180.253, p < 0.001, indicating that the set of predictors reliably distinguished between outcome groups. The model explained approximately 26% of the variance in the outcome (Nagelkerke R2 = 0.260) and correctly classified 70.2% of cases. Model fit was adequate according to the nonsignificant Hosmer–Lemeshow test, χ2(8) = 5.759, p = 0.674. Among the predictors, gender was a significant factor, with females being more than twice as likely as males to choose online peer support (B = 0.741, SE = 0.188, p < 0.001, OR = 2.098, 95% CI [1.452, 3.033]). Country also had a strong effect: participants from China were significantly six times more likely than those from NI to use online peer support (B = 1.876, SE = 0.204, p < 0.001, OR = 6.529, 95% CI [4.381, 9.730]). The GHQ-12 score was also a significant positive predictor (B = 0.040, SE = 0.013, p = 0.002, OR = 1.041, 95% CI [1.015, 1.068]), indicating that higher GHQ-12 scores (higher psychological distress) increased the likelihood of the use of online peer support. For every point increase in distress, the odds of using peer support went up by about 4%. Regarding clinical disorders, participants with clinical disorders were almost five times more likely to report the utilisation of online peer support compared to the reference group (young people without clinical disorders) (B = 1.518, SE = 0.221, p < 0.001, OR = 4.565, 95% CI [2.963, 7.035]). Age and education were not significant predictors (p > 0.05). Furthermore, no issues of multicollinearity were detected Variance Inflation Factor (VIF < 2). These findings suggested that gender, country, GHQ-12 scores and clinical disorders were significant predictors of the outcome, while age and education did not contribute meaningfully to the model. The results of the binary logistic analysis are shown in Table 4.
Possible predictors affecting whether young people engage with online peer support use.
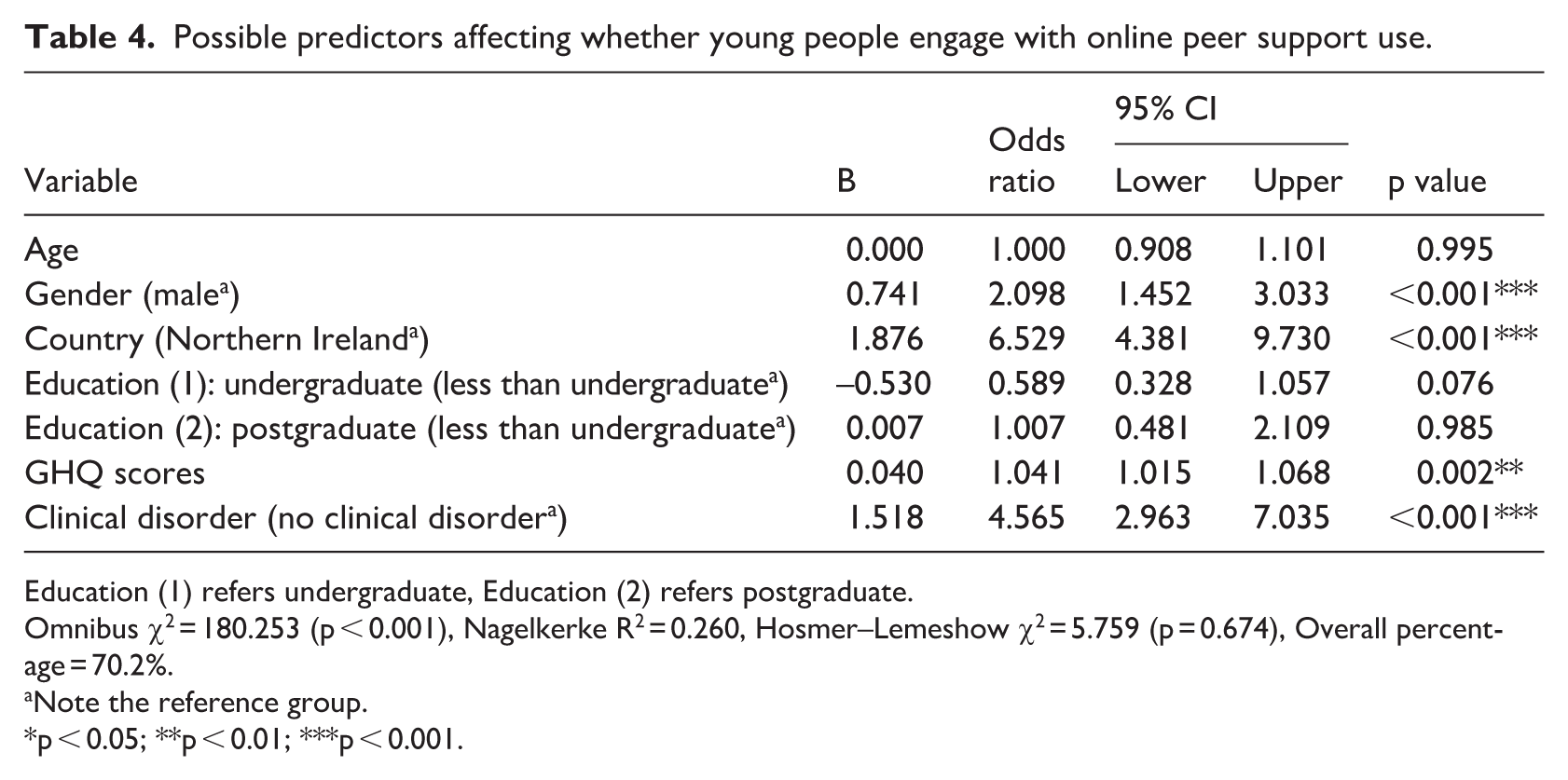
Education (1) refers undergraduate, Education (2) refers postgraduate.
Omnibus χ2 = 180.253 (p < 0.001), Nagelkerke R2 = 0.260, Hosmer–Lemeshow χ2 = 5.759 (p = 0.674), Overall percentage = 70.2%.
Note the reference group.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
To the best of our knowledge, this is the first study investigating online peer support use and youth MWB based on the different cultural backgrounds between Western and Eastern countries (NI and China). According to the responses, we demonstrated the basic usage of online peer support, the MWB of young people, and identified key factors associated with online peer support use in the future.
The prevalence of poor MWB
Mental health issues among young people are a global concern, irrespective of cultural background, especially for those who are still studying in university, facing multiple challenges such as academic pressure and relationship difficulties. The study revealed that almost 70% of respondents had poor MWB, with mental health problems in NI being more severe than those in China. In NI, the proportion of young people likely to have mental health issues was almost double that of China. It is difficult to identify all of the possible explanations, but these may include the legacy of political conflict in NI; associated issues of intergenerational trauma; and areas of relatively high deprivation (McLafferty et al., 2019). The study found a relatively high proportion of young people to be at risk of mental health issues, largely due to the fact that the study’s participants exhibited more severe mental health issues and were struggling with mental health problems. Even so, regardless of geographical location, it is essential for mental health social workers to take measures aimed at alleviating young people’s psychological distress. It is noteworthy that a greater proportion of young people in China did not report any clinical disorders. On the one hand, there were lower GHQ-12 scores in China than NI. On the other hand, the majority of young people reporting no clinical mental health conditions have never received a professional diagnosis for mental health issues, which is largely attributable to the absence of systematic mental health education and stigma associated with culture (Li et al., 2023). The lack of adequate mental health education among young people may result in the disregarding of mental health issues, which probably in turn leads to delays in diagnosis and treatment. Furthermore, within the context of the culture, there is a perception of mental health and related issues as a source of shame. Young people may also be concerned that a mental health disorder diagnosis could have a negative impact on their academic performance and future career development.
The usage of online peer support
In accordance with the findings of previous research, online peer support is growing in popularity among young people (Bennett et al., 2022). More than a quarter of young people selected it to seek assistance with their mental health concerns and focused on more opportunities to interact with peers experiencing similar problems, which represented the great potential of online peer support to address mental health problems. However, it is evident that online peer support functions as a complementary service to professional services (Pretorius et al., 2019). Some young people have expressed concerns about the reliability of online peer support. Given the absence of professional mental health training among many peers, their experiential knowledge is largely drawn from personal narratives and viewpoints (Watson, 2017; Yuan et al., 2025), which is highly likely to result in the dissemination of misinformation and the spread of negative sentiment to exacerbate mental health issues among young people.
Moreover, a significant proportion of young people with experience of online peer support reported that social media was the most frequently used platform, providing dynamic and interactive experiences that appeal to youth (Van Meter and Agrawal, 2024). Young users would be immediately inundated with content, so concerns about exposure to stigmatising influences would be reduced. Therefore, the potential of social media to provide a confidential and accessible pathway for those who would prefer not to seek professional help should not be underestimated. However, social media tends not to specifically focus on mental health issues, and young people may be more likely to engage with a wider range of users and receive more complex information, further exacerbating the risks associated with online peer support. Meanwhile, more than a quarter of participants have expressed concerns about the current online environment. Consequently, improving the moderation of social media (perhaps with social workers as moderators to promote safety and sustainability) or incorporating online peer support within traditional mental health and social work services would be the most promising pathways for young individuals who are struggling with mental health issues or have been diagnosed with mental disorders.
The evidence indicated that the primary reason for the lack of experience of online peer support among young people was the absence of mental health difficulties. However, the GHQ-12 scores revealed a significant potential for mental health challenges among this demographic. This group of young people have the potential to utilise online peer support, particularly during the early stages, when social workers can provide valuable assistance. At this stage, promotion or education is able to equip young people with emotional management skills and problem-solving strategies through mental health courses to enhance the ability to respond to challenges and improve social support, even in the absence of current mental health symptoms (Yuan et al., 2026). In the meantime, prevention may help them recognise stress, anxiety and other issues more easily, thereby preventing these problems from escalating into more serious mental disorders (Carlisle et al., 2024).
The perceived effectiveness of online peer support
The results showed no significant association between time spent on online peer support and GHQ-12 scores. However, most of the young participants reported that online peer support was helpful to acquire emotional or informational support and improve their MWB (Prescott et al., 2017), which suggested that, in line with previous research, the effectiveness of online peer support would probably be affected by the dosage (Kohl et al., 2013; Yeo et al., 2025). Online peer support interventions typically last from 1 to 144 weeks, with optimal results achieved when implemented at the outset. However, the effectiveness of the intervention tends to diminish over time (Yeo et al., 2025). Conversely, greater doses or longer durations of intervention are more likely to lead to adverse effects from online peer support, such as contagion and cyberbullying. Consequently, how to design and assign the dosage of digital interventions to achieve the benefits of online peer support remains an area requiring further investigation. During the data collection phase, we did not have access to detailed information regarding the utilisation of online peer support by respondents (e.g. when did they recently use it?). In addition, our study design did not adopt a rigorous pre–posttest design. This may, therefore, be one of the reasons for the lack of significant results.
Factors associated with online peer support use
The binary logistic regression confirmed a set of variables as potential predictors of the choice of online peer support, such as gender, country, GHQ-12 scores and clinical disorders. In terms of gender, a large number of studies have identified that females are more likely than males to experience mental health symptoms and to seek support through the Internet (Roberts and Parry, 2023; Smail-Crevier et al., 2019). Meanwhile, it is believed that females provide more social support on social network sites and show higher acceptability of using digital interventions (Smail-Crevier et al., 2019; Tifferet, 2020). Conversely, young males are highly likely to be reluctant to seek help due to social norms and traditional masculinity, preferring professional mental health services (Best et al., 2014; Sheikh et al., 2025). The existence of gender differences and preferences determines that more young females than males will use online peer support for mental health struggles.
The country is another key factor affecting the option of online peer support. In line with prior research, China, as a typical Eastern country, values collectivism more strongly. Chinese individuals tend to prioritise emotional self-adjustment and self-management of mental health issues over self-disclosure (Lee et al., 2014). Mental health issues are accompanied by a greater likelihood of encountering stigmatisation compared to Western countries (Misra et al., 2021). Therefore, online peer support can be a valuable alternative for young people, offering an anonymous platform to share their experiences and reduce the risk of stigmatisation. While in NI, it was found that young people were encountering a number of barriers to accessing mental health services. These included long waiting times, unaffordable expenses and a limited type of services (National Children’s Bureau, 2024). Online peer support can be developed with particular emphasis on meeting the needs of specific cultural groups and providing access to mental health resources. In China or other similar Eastern countries, the primary focus should be on education and prevention to increase mental health literacy. This will assist young people in the elimination of incorrect beliefs and stigma surrounding mental health issues and encourage them to seek help bravely, thereby effectively linking to traditional services. While in NI or other similar Western countries, it should mainly focus on prevention and early intervention to address the existing relative gaps in the treatment of subclinical symptoms and distress (Bernecker et al., 2020) and prevent problems from escalating when young people are unable to access professional services temporarily.
With regard to GHQ-12 scores and clinical disorders, young people who are currently struggling with mental health difficulties or have been diagnosed with mental disorders are likely to turn to online peer support. This is because they clearly feel troubled and urgently seek resonance, understanding and support from those who have had similar experiences (Yuan et al., 2025). Compared to traditional mental health and social work services, online peer support is free of charge and 24/7 accessible without a waiting list, which makes it a particularly convenient option for young people who have limited offline resources. Furthermore, young people who have been diagnosed with mental disorders may have been advised to try online peer support run by related mental health organisations or charities during treatment or may have independently recognised the importance of peer support while seeking available resources. It is possible that young individuals with lower GHQ-12 scores or who do not have a mental disorder may lack appropriate guidance and, therefore, be unaware of the forms or benefits of online peer support, which was also found in our sample. Lacking specific knowledge of online peer support was identified as an important component hindering participants from opting for online peer support to deal with mental health issues. Therefore, social workers from related mental health and young people’s organisations and the MWB support services of universities should disseminate and develop appropriate services to improve the awareness of positive online peer support and reduce the risks posed by unprofessional peers.
While the results did not indicate that age was an associated factor in the selection of online peer support, it was observed that the initial users of online peer support in NI were younger than those in China, which needs further investigation through future comparative research to understand the underlying reasons.
Limitations
There are several limitations of this study. First, although the overall model of binary logistic regression was significant, the lower sensitivity of 46.6% when focusing on users suggests the model was more accurate at predicting nonuse than use of online peer support. Another potential limitation is the possibility of bias in the sources used. A large number of young people responded to the online survey. However, the convenience sample employed in this study might not be a precise representation of the nonparticipating individuals and the broader population, because most of the participants in China were from Northern China, which might cause a challenge to fully demonstrate the situation in China. Meanwhile, the study included a standardised scale and conducted a pilot study to reduce result bias, although care should still be taken if generalising to the broader population in both countries and internationally. Finally, it also should be noted that the higher proportion of female participants may have an impact on the generalisability of the findings. Future research should intentionally focus more on the engagement of online mental health peer support among young males in order to validate the robustness of the results.
Conclusion
The current study demonstrated that poor mental health among young people in NI and China was common. It is vital that we maintain a constant focus on the MWB of young people and explore as many potential and effective strategies as possible to help young individuals with mental health issues all over the world appropriately deal with them. Meanwhile, social work practitioners and other mental health professionals would come to recognise the importance of online peer support in light of the changing preferences regarding help-seeking, which results in an increased use of digital mental health interventions. The study did not find a significant association between time spent on online peer support use and MWB. However, the majority of respondents reported the effectiveness of online peer support, which suggests that online peer support might have greater potential to supplement traditional mental health and social work services at different stages (e.g. during waiting periods, ongoing therapy and posttreatment care) and reduce the inherent risks (Alvarez-Jimenez et al., 2025). Furthermore, doses of online peer support are another element that needs to be taken into account. This research highlights the potential appeal of online peer support to the younger generation and its potential effectiveness in addressing mental health problems, with possible application in countries with different cultural backgrounds. Future research should further explore the accessibility, content and quality assurance of online peer support with particular emphasis on different cultural and country contexts.
Footnotes
Ethical considerations
This study was approved by Queen’s University Belfast, the School of Social Sciences, Education and Social Work Ethics Committee (REF 165_2324) on 22 July 2024. The participants were recruited from 11 August 2024 to 12 February 2025.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Due to confidentiality obligations, the data are not publicly available. Data supporting the findings of this study are available from the author upon reasonable request.
Statement on artificial intelligence (AI)
AI was not used in this research or to draft this article.