
Abstract
The aim of the research is to examine the HIV risk factors affecting poor health in Ethiopia by epidemiological perspectives. The Demographic and Health Survey 2011 and other secondary data were used. Ethiopian population growth has slowed dramatically or stopped due to HIV and AIDS. A logistic regression and correlation between HIV positive towards AIDS, high risk factors leading to exposure to HIV infection was adopted with selected variables. The study confirmed that the high level of HIV positivity and poor health was highly affected by socio-economic and demographic factors.
Introduction
The HIV/AIDS epidemic is no longer merely a health problem but one of the greatest development challenges the world has ever faced (UNAIDS, 2010; UNICEF, 2002; WHO, 2014). Still, the disease continues to spread with no cure yet in sight. The epidemic is rightly said to be associated with poverty, but the reality is much more complex. In many sub-Saharan African countries, Ethiopia in particular, HIV/AIDS remains one of the key challenges for the country’s overall development. The national HIV prevalence in adults is at 1.9%; 14,695 people are HIV positive (Ethiopia Demographic and Health Survey, 2011). The country faces a mixed epidemic, where prevalence is low among the general population but high among sub-populations and certain geographic areas. The primary mode of HIV transmission in Ethiopia is heterosexual contact (Central Statistical Authority and ORC Macro, 2001). Young women are more vulnerable to infection than young men, and urban women are three times more likely to be infected than urban men are (Central Statistical Authority and ORC Macro, 2001; Ethiopia Demographic and Health Survey, 2005). From the evidence, the government of Ethiopia has proven committed in its response to the epidemic. Over the last three decades, the government has established numerous entities to coordinate efforts to deal with the epidemic (Ministry of Finance and Economic Development (MOFED) Ethiopia, 2010). These include a national HIV/AIDS Task Force within the Ministry of Health, an HIV/AIDS Prevention and Control Office (represented at federal, regional, district and kebele levels) responsible for the leadership and coordination of the country’s multi-sectoral response, and implementation of national strategic plans to enhance the country’s response (Ministry of Finance and Economic Development (MOFED) Ethiopia, 2010). By the end of 2012, the global estimate of people living with HIV/AIDS had reached 45 million, while more than 23 million people had died of AIDS since the emergence of the disease barely two decades ago (Bicego, 1997). While the pandemic is global, its prevalence and impact are overwhelming in the developing regions of the world, especially in Africa (Garenne et al., 1994; Ryder et al., 1991). Estimates suggest a 17.2% rise in global prevalence of the disease between 2000 and 2010, and a corresponding estimated 20% rise in sub-Saharan Africa during the same period. There is a growing body of literature on the demographic impact of HIV/AIDS on various populations, especially in Africa (Allen et al., 1993; Central Statistical Authority and ORC Macro, 2011). Obtainable studies have investigated the mortality implication of the pandemic, its impact on fertility, and its effect on population growth and age structure (Caldwel, 1997; Gregson et al., 1997; Ministry of Finance and Economic Development (MOFED) Ethiopia, 2010).
In Ethiopia, several studies have been conducted, focusing on the reproductive health issues of adolescents. Their findings show that in the country, sexual practice among unmarried young people starts at early ages, and the prevalence of sexually transmitted diseases (STDs) like HIV and AIDS is relatively high, most of them leading to death. For example, HIV and AIDS accounted for an estimated 34% of all deaths in people between the ages of 15 and 24 years who lived in the country, and 66% of all deaths of those age 15 to 49 years who resided in urban settings such as Addis Ababa (Central Statistical Authority and ORC Macro, 2011).
The studies also showed that adults aged 25 to 49 years and those aged 15 to 24 years are the centre of the HIV and AIDS pandemic (Ministry of Health, 2000). In addition, numerous studies have shown that early sexual activity has a profound influence on a young person’s current and future health, most directly through exposure to unprotected sexual practices resulting in unintended pregnancy and childbearing (Central Statistical Authority and ORC Macro, 2011 ). Deaths were also due to induced abortion in hazardous circumstances and to STDs, including HIV leading to AIDS. Factors believed to have contributed to the spread of HIV/AIDS include poverty, illiteracy, the low status of women, ignorance and denial, all of which foster risky sexual behaviour (Daly, 2000). This seems to apply to the Ethiopian situation, where despite the high level of awareness of HIV/AIDS (96% among men and 85% among women), only 42% of men and 35% of the women interviewed in the 2011 Ethiopia Demographic and Health Survey knew at least one way to avoid the disease (Central Statistical Authority and ORC Macro, 2011). Until awareness leads to attitudinal and behavioural changes, the prevalence rate might not stabilize (Dowell et al., 1994).
The Demographic and Health Survey (DHS) 2011 reported that, the overall adult HIV prevalence in Ethiopia has remained low. The HIV prevalence among adults aged 15 to 49 years in the 2011 Ethiopia DHS (EDHS) was 1.5%, while it was 1.4% in the 2005 EDHS (Ethiopia Demographic and Health Survey, 2005, 2011). Many findings show that the pandemic has varied impact that touches on the social, economic and demographic aspects of lives of the individuals and of society at large, as recognized by policy makers (Central Statistical Agency, 2007; Federal Democratic Republic of Ethiopia, 1998; Ministry of Finance and Economic Development (MOFED) Ethiopia, 2010; Statistical Abstract of Ethiopia, 2008). However, an understanding of the magnitude, nature and consequences of the demographic, social and economic impacts would help to generate greater commitment and adoption of more aggressive strategies for effective prevention of the spread of the virus and care for those living with the disease. The number of AIDS-related orphans was nearly 2.8 million by 2010 (Ethiopia Demographic and Health Survey, 2011). Obviously, this aggravates social problems. Most of the orphans in school would drop out without the help of relatives, due to the problems of fees, clothing, books and other related costs of education. In the absence of a social welfare system, many grandparents, who themselves need care, would of necessity care for both themselves and their orphaned grandchildren. The number of households headed by adolescents would also increase. The number of street children would tend to rise, while the problem of child labour would worsen as the orphans struggle for survival.
Besides these issues, large declines in expectation of life at birth would invariably result in a ‘young’ population in the long run, which has an inherent, adverse consequence on national development. Under a purely demographic process, a young population resulting from a high rate of natural increase constitutes an obstacle to a country’s socio-economic development (Ministry of Finance and Economic Development (MOFED) Ethiopia, 2010). A young population resulting from the demographic impact of HIV/AIDS would impede development not only due to the high rate of natural increase but also as a result of the loss of a substantial proportion of the productive members of the population, which would compound social and economic problems, especially at the household level (Argeseanu, 2004; Carpenter et al., 1997; Fontanet, 1998; Kidane, 1994; UNAIDS, 2003). By its nature, the demographic impact either generates or exacerbates the social and economic consequences of the disease. The fact that mostly people in their prime productive and reproductive ages (15–49) are affected by the pandemic has a demographic impact with both economic and social consequences. A serious HIV/AIDS pandemic can result in the loss of a substantial proportion of the skilled labour force. This suggests that unless the adult infection rate is reduced appreciably, AIDS deaths are likely to reduce the Ethiopian labour force substantially by the close of this decade. Yet, most of those who would die of AIDS would leave behind widows and orphans (who themselves may eventually die of the disease), thus adding to the social problems. As of 2001, about one million Ethiopian children had lost their parents to AIDS since the emergence of the pandemic (Carpenter et al., 1997; Fontanet, 1998; UNAIDS, 2003).
The latest report, DHS 2011, mentioned that for women aged 15–49 years, the HIV prevalence is 1.9%, and among men aged 15–49 and 15–59, HIV prevalence is 1.0%. For women, HIV prevalence increases with age, to a peak of 3.7% at age 30–34. For men, HIV prevalence increases from 0.0% at age 15–19, to 3.0% at age 35–39 and drops thereafter. Overall, HIV prevalence is higher for women than for men in most age groups (Ethiopia Demographic and Health Survey, 2011). Available evidence indicates that the HIV/AIDS epidemic has now spread to every region of the country and that the prevalence rate has been increasing rapidly, especially in Gambela, where it is 6.5%, and in Addis Ababa, where it is 5.2% (Ethiopia Demographic and Health Survey, 2011). For purposes of this paper, the researchers focused mainly on Addis Ababa, the capital city of Ethiopia. We wanted to understand why the HIV prevalence is so high in Addis Ababa and whether HIV prevalence does correlate with the wellbeing of those who are underprivileged in Addis Ababa, Ethiopia.
People in rural areas migrated to Addis Ababa for various reasons, but mainly for employment, education and treatment purposes. Interestingly, Addis Ababa achieved below replacement level fertility (1.2 children per woman) (Ethiopia Demographic and Health Survey, 2011). Because of this, the present study intends to contribute to facilitating appreciation of the magnitude, nature and possible consequences of the demographic and socio-economic impact of HIV/AIDS in Addis Ababa, in particular, and in Ethiopia in general. Such an understanding is necessary to generate an aggressive response that can effectively stabilize and possibly reverse the rising trend of the spread of the disease and consequently mitigate its devastating impact on the population. Therefore, the specific aim of the research is to examine the HIV risk factors affecting poor health in Addis Ababa by epidemiological perspectives.
Data
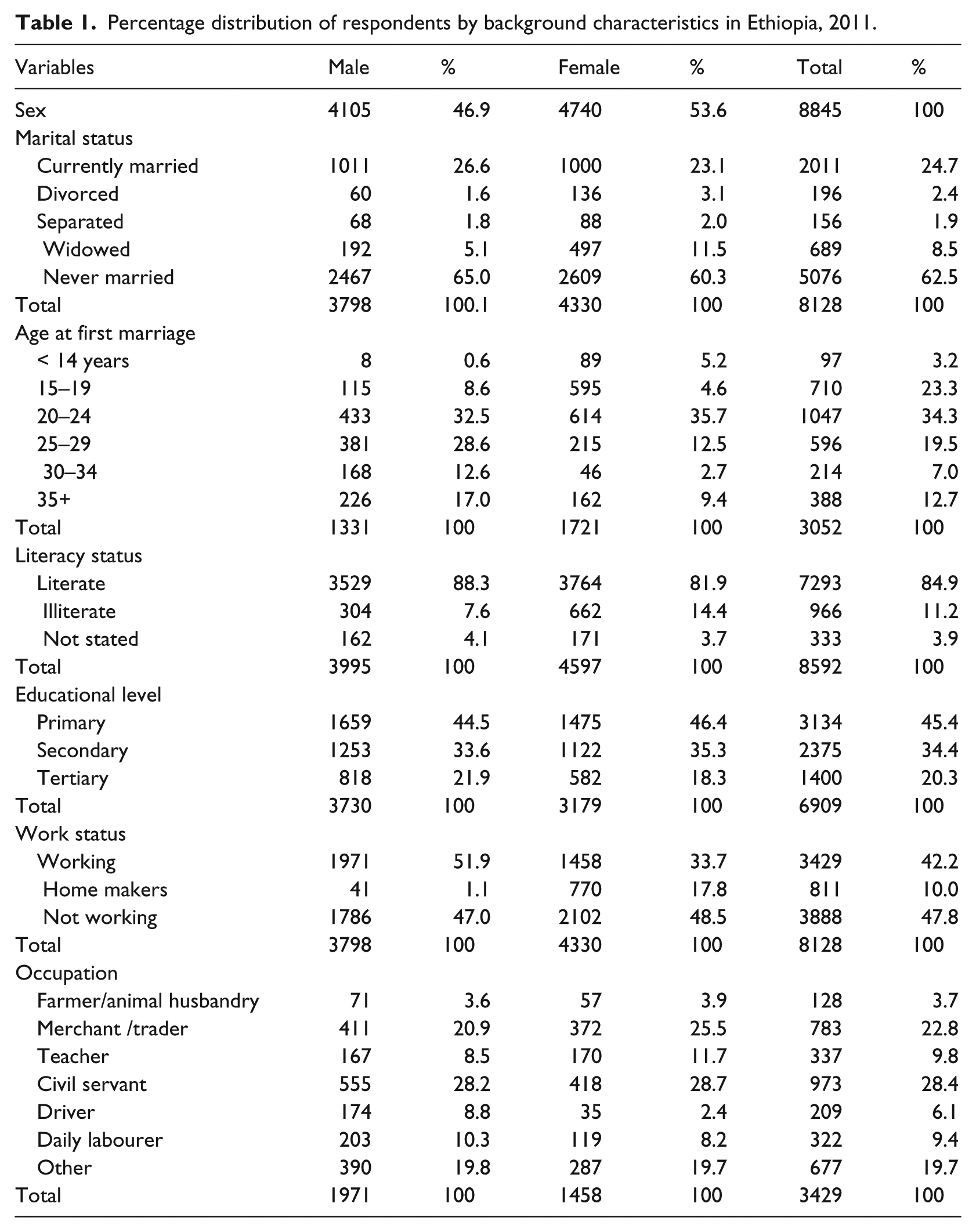
The DHS 2011 data sampled nearly 16,000 households in Ethiopia. There are different data files such as births, household, individuals, children, males, household members, and couples’ records. Of the total number of respondents used for the study, 46.9% (4105) were male and 53.6% (4740) were female in Ethiopia. Respondents were asked questions on background characteristics including age, education and media exposure, birth history, child mortality, knowledge and use of family planning methods, fertility preferences, antenatal care, delivery and postnatal care, breastfeeding and infant feeding practices, vaccinations, childhood illnesses, marriage and sexual activities, women’s occupations, husband’s background characteristics, awareness and behaviours regarding AIDS and other sexually transmitted infections, and adult mortality.
Methods
The fundamental needs for the study variables are identification of any household with a member(s) living with HIV/AIDS or whose member(s) had died of AIDS. Such information is not easy to obtain in a society where HIV/AIDS victims are stigmatized and systematic registration of death is lacking. At the household level, a background questionnaire was used to collect demographic, social and economic data as well as the main wealth index and expenditures of the household in the last 12 months before the survey. This information was collected from households with HIV/AIDS-related deaths (or morbidity) and those with non-HIV/AIDS-related deaths (or morbidity). Common symptoms included: coughing and shortness of breath, difficult or painful swallowing, mental symptoms such as confusion and forgetfulness, severe and persistent diarrhoea, fever, abdominal cramps, vomiting, weight loss, extreme fatigue, severe headaches, etc. The present study specifically focused on two dependent variables: (1) HIV positive and (2) symptoms of (a selected number of) diseases, such as severe fatigue, pneumonia, chronic coughing, high fever and night sweats, difficulty in breathing, and other symptoms of illness. In the latest HIV prevalence in women and men aged 15–49 years in Ethiopia, 2011 showed in the Figure 1.
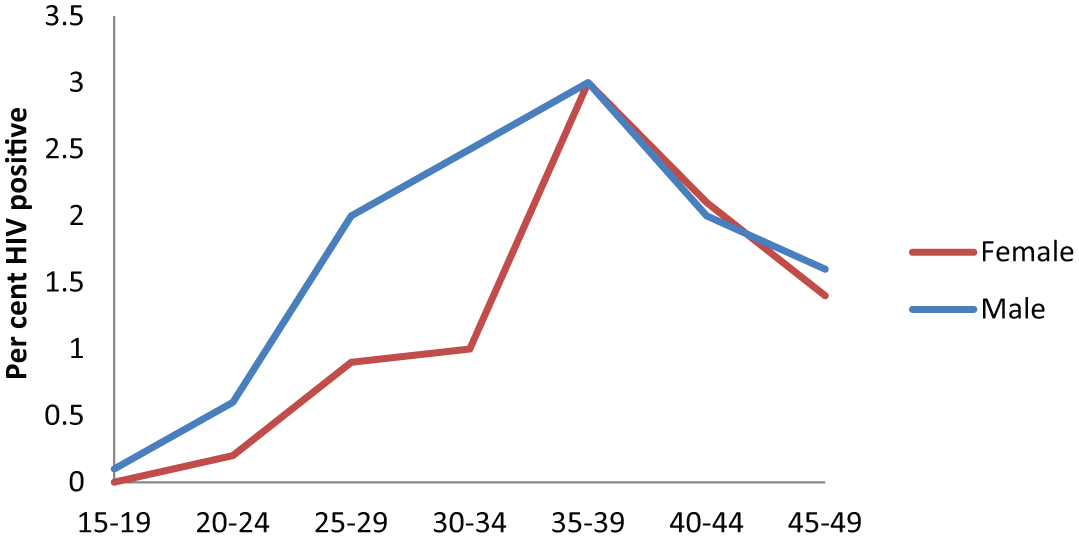
HIV prevalence in women and men aged 15–49 years in Ethiopia, 2011. Source: Ethiopia Demographic and Health Survey 2011.
Selected independent variables
The odds ratio for the logistics regression model of demographic and socio-economic implications of HIV/AIDS in the study area was adopted. There are nine variables included in the analysis: sex, literacy (for those aged five and older), education (for those aged five and older) work status, source of income, marital status, natural mother alive, natural father alive, and occurrence of illness (these variables are used as categorical variables). The correlates between HIV positive toward AIDS and high-risk factors leading to exposure to HIV infection with background variables were tested. This prompted further analysis of background variables and the analysis of variance was performed to isolate the effects of individual background variables on the HIV positive toward AIDS variable and high-risk factors leading to exposure to HIV infection by logistics regression analysis. The quantitative weighted data were analysed using SPSS 22.0 version for Windows. Quantitative data analysis is simple and clearer to give a more holistic view of the rate at which respondents suffered diseases and identification of the demographic and socio-economic correlates on HIV/AIDS in the study area.
Results
The findings of the study confirm the high level of HIV infection and that people of poor health were highly affected (when looking at the background characteristics). The sex composition of respondents showed that there were fewer young male respondents, at 46.9% (4105), than female respondents, at 53.6% (4740). The age composition demonstrated a higher number of respondents in the younger age groups (15–24 years), at about 26.5% for both sexes. Age at first marriage was 29.61 years, which was late compared with the national average at first marriage, which was 18 years. Regardless of the sex differences, 34.3% of the respondents married between the ages of 20 and 24 years and 23.3% married at the age of 15–19 years; half (57.6%) of the respondents married at the age of between 15 and 24 years.
A higher incidence of illiteracy was found in females (14.4%) than in males (7.6%), although the level of illiteracy was low for both sexes. In addition, more females were found to have primary (46.4%) and secondary education (35.3%) than their male counterparts, which was 44.5% for primary and 33.6% for secondary education. At the tertiary levels, the percentage of males (22%) exceeded that of females (18.3%). Regarding work status and occupation, more males indicated they were working (51.9%) than not working (47.0%) compared with females, of whom 33.7% were working and 48.5% were not working. There was only a slight difference in the primary economic activity (farmer/animal husbandry) between males (3.6%) and females (3.9%), with results for females higher than results for males. Nearly 30% of the respondents were identified as HIV positive, while the majority of the respondents were negative (66.5%). Most of the HIV positive respondents were distributed evenly across the different age groups (see Table 1). A high proportion of 20–24 years age group, 1047 out of 3052 cases, reported HIV positive. Symptoms of illness collected from the respondents for the last 12 months showed that 15.1% of male respondents experienced severe fatigue, 15.0% lacked appetite, 13.0% had high fevers and night sweats and 10.1% experienced rapid weight loss. Similarly, 16.0% of females endured severe fatigue, 15.3% lacked appetite, 13.3% had high fevers and night sweats and 10% observed rapid weight loss. For both males and females, the results showed a similar pattern for dominant symptoms of illness. The three least-reported symptoms of illness, exhibited by smaller proportions of respondents showing symptoms of illness, were irritating white patches in the mouth, gum and tongue (1.8% for males and 1.9% for females); skin rashes on the chest/abdomen/back (2.0% for males and 2.1% for females); and swollen lymph glands in the armpit, groin or neck (1.9% for males and 2.2% for females). Generally, the three most important symptoms of illness were severe fatigue, high fever plus night sweats, and rapid weight loss (Table 2).
Percentage distribution of respondents by background characteristics in Ethiopia, 2011.
Percentage distribution of respondents who have had illness at least for a month in the last 12 months by symptoms of illness, Addis Ababa, 2011.
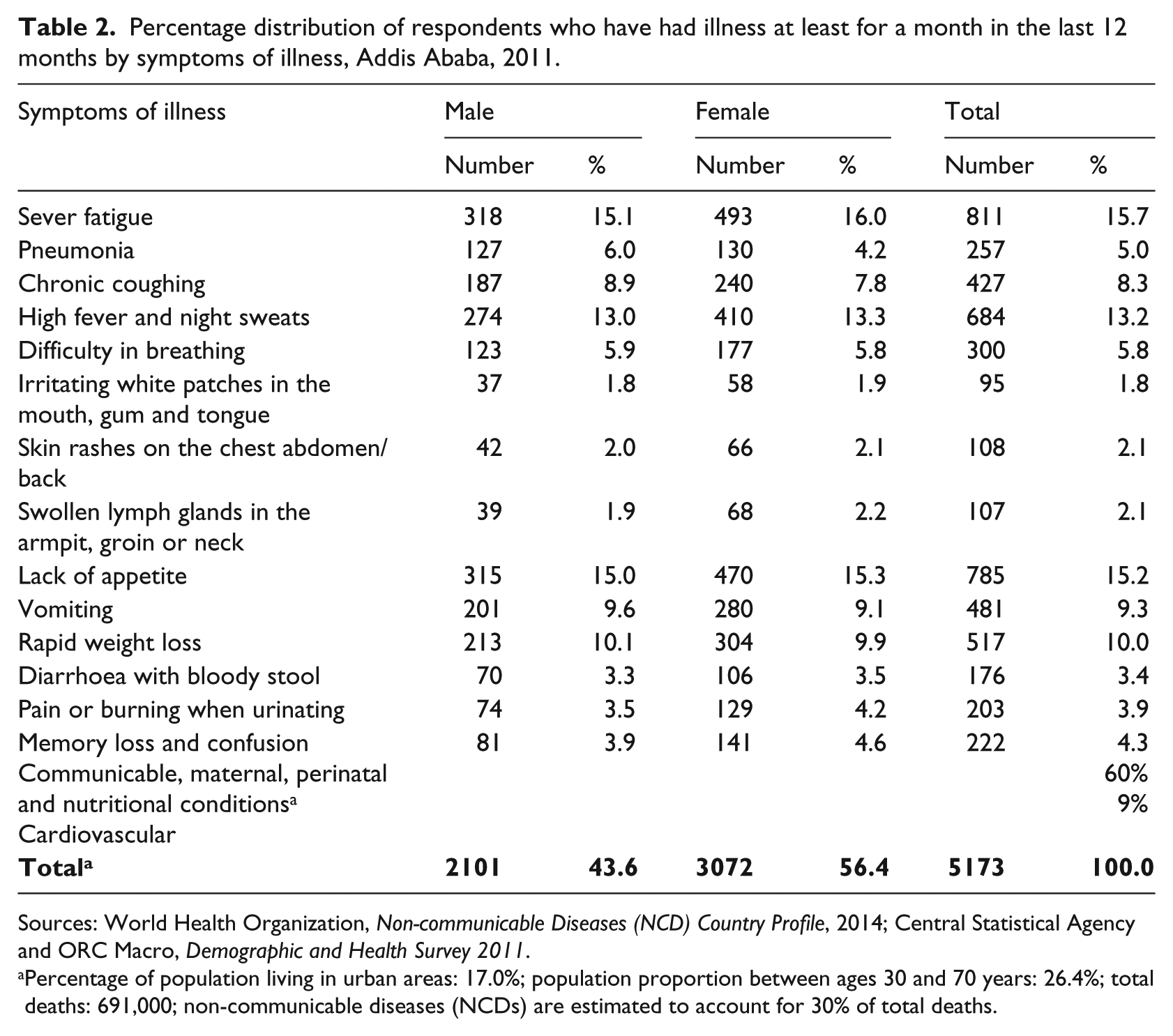
Sources: World Health Organization, Non-communicable Diseases (NCD) Country Profile, 2014; Central Statistical Agency and ORC Macro, Demographic and Health Survey 2011.
Percentage of population living in urban areas: 17.0%; population proportion between ages 30 and 70 years: 26.4%; total deaths: 691,000; non-communicable diseases (NCDs) are estimated to account for 30% of total deaths.
Regression analysis
Two odds ratio models were used to estimate the consequences of socio-economic and demographic factors related to HIV/AIDS and occurrence of diseases. These variables are provided as dichotomous variables. The outcome of the logistics regression scrutiny on the implications of HIV/AIDS variables regressed on socio-economic and demographic variables is specified in Table 3. Nine independent background variables were observed to be absolutely significant with HIV-positive respondents in model I. That left two independent variables, which are education (if the person was aged five or older) and natural father alive; these were shown not to be significantly related to being HIV positive. All these factors were used as explanatory variables in the equation to determine the comparative influence of each factor on the implications of HIV/AIDS in the two models. For marital status of respondents, those who were identified by the ‘other’ category showed vastly significant (p<0.001) results when compared with the currently married group. At the same time, occurrence of illness among those who were identified by the ‘other’ category showed noteworthy effects on HIV-positive categories.
Odds ratios for the logistic model of demographic and socio-economic implications of HIV/AIDS in Ethiopia, 2011.
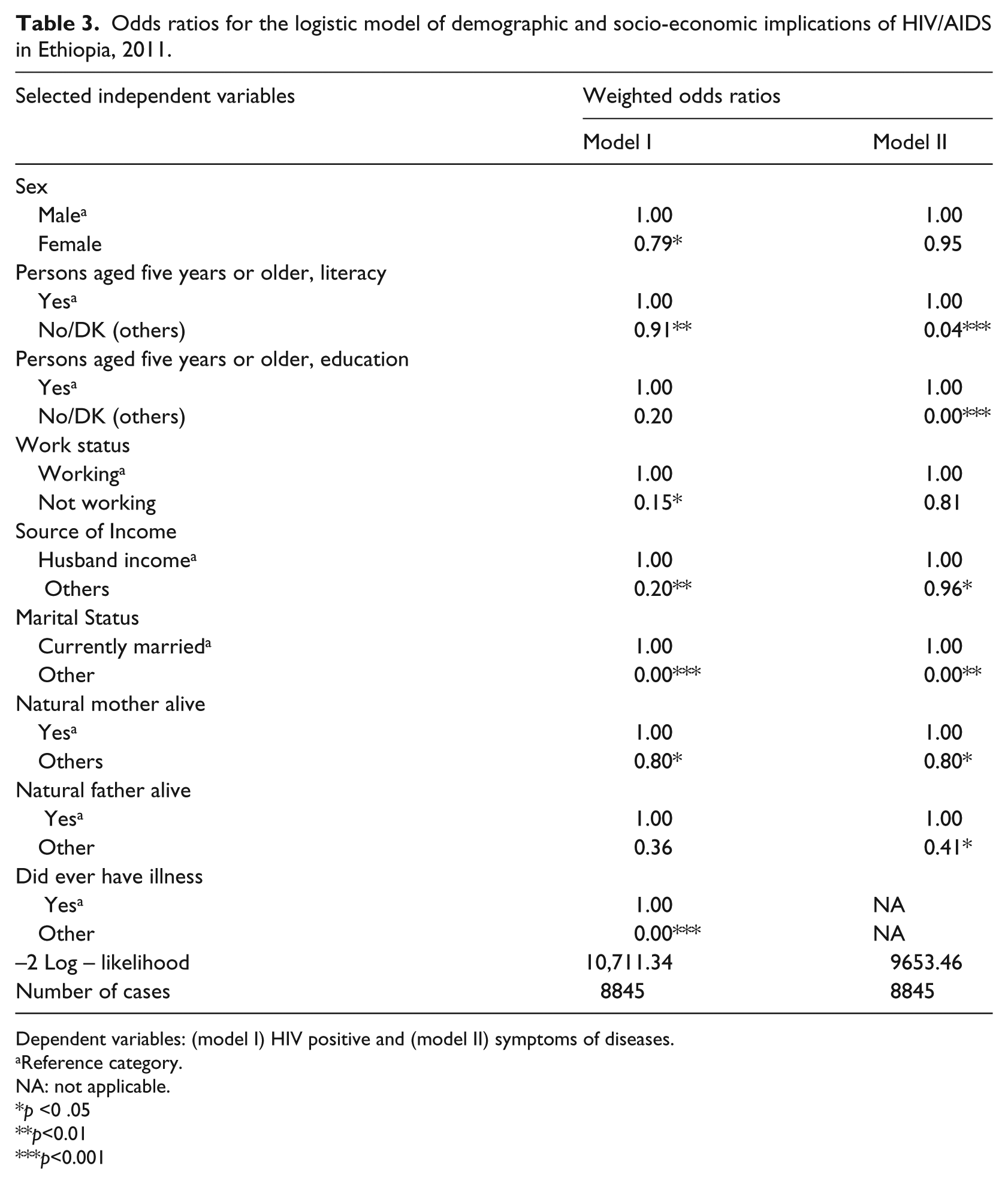
Dependent variables: (model I) HIV positive and (model II) symptoms of diseases.
Reference category.
NA: not applicable.
p <0 .05
p<0.01
p<0.001
Those who reported having their natural mother alive (within the ‘other’ category) were less likely (odds ratio 0.80; significant, p<0.05) to have HIV/AIDS and occurrence of diseases, compared with the reference category. The total number of 8845 cases at −2 log likelihood values showed 10,711.34 with the effect of all background explanatory variables affecting the HIV-positive variable. Overall, the HIV-positive effect plays a key role in the selected independent background variables. The effect of the odds ratio for the logistic model of demographic and socio-economic implications of HIV/AIDS in the study area is clearly noticeable.
In model II, two variables – persons aged five years or older exhibiting literacy, and education of persons aged five years or older – show highly significant effects on dependent variables. The odds ratios provided an exact picture of the present study; both of the models clearly show the effect and positive significant effect with the dependent variables. Also visible was the effect of the correlation between the variable of HIV positive toward AIDS high-risk factors leading to exposure to HIV infection, which demonstrates an additional proof of the study.
The correlation analysis perhaps suggested that the HIV positive toward AIDS and high-risk factors leading to HIV infection were more significantly correlated with the background variables than HIV positive towards AIDS and illness high-risk factors such as severe fatigue, pneumonia, chronic cough, high fever, difficulty breathing and other problems. The results of the multiple classification analysis of the dependent variables, namely, HIV positive and symptoms of diseases, are presented in Table 4. A more convenient way to interpret the main effect is to have a logistic regression model. Work status of the respondents has shown to be highly significant with HIV positive (at 0.30) and source of income is 0.33 times as likely to be a consequence of being HIV positive. At the same time, the marital status of the respondents showed a significant level, at 0.39 times the effect, and the probability value is p<0.01. Education of persons aged five years or older had a negative effect on HIV positive, which is −0.54 times, with the possibility value of p<0.001. High-risk factors leading to HIV infection during the course of some of the diseases include severe fatigue, pneumonia, chronic coughing, high fever, difficult breathing and other diseases. Severe fatigue disease is almost a significant outcome on several background variables, but education of those persons aged five years or older produced a negatively significant result with severe fatigue disease.
Correlation between HIV positive towards AIDS, high risk factors leading to exposure to HIV infection with background variables, Ethiopia 2011.
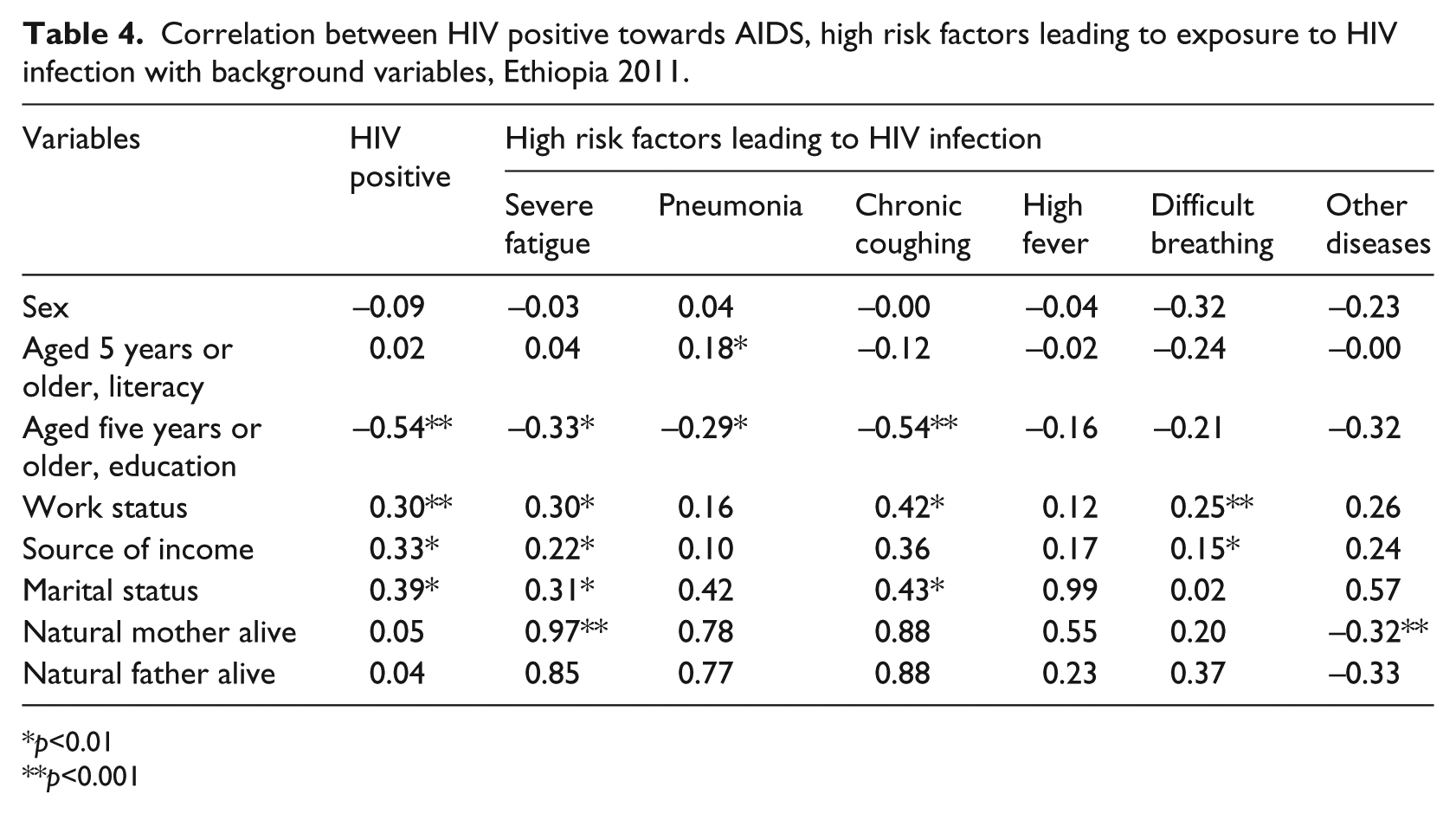
p<0.01
p<0.001
The circumstance of the mother being alive is decidedly significant with severe fatigue, but three variables – sex, literacy in persons aged five years or older, and circumstance of the father being alive – have not shown any significant effect on severe fatigue. Other diseases, such as pneumonia, showed significance on only two factors: literacy of persons aged five years or older had a significant effect (at 0.18) and education of persons aged five years had a negative significant effect (at −0.29) on pneumonia. While considering the effect of the predictor variable (literacy of persons aged five years) on the HIV-positive variable, it was observed that the unadjusted means for the categories ‘no’ and ‘other’ were 0.91 and 0.04, respectively. This study showed that those who were working exhibited more knowledge of AIDS compared with those in the non-working category.
Surprisingly, the non-working respondents exhibited more knowledge of AIDS than those respondents who worked in the primary sector. Although AIDS is considered one of the most serious public health challenges facing the country, the majority of women have never heard of the disease. Moreover, many of those who have heard of the disease do not know how to avoid AIDS. For more than a decade, HIV and AIDS prevalence levels have been on the rise in Addis Ababa. Prevention programmes need to continue to strengthen their educational outreach efforts, especially among less-educated women who have little or no exposure to the mass media.
Discussion
As per the study findings, younger age groups were more affected by HIV during sickness. Older people more often died of diseases due to being HIV positive. This study strongly recommends that the demographic and socio-economic implications of HIV/AIDS studies are considered at this juncture. Further research is required to establish how HIV and socio-economic status are related to poor health or illness in Addis Ababa. As HIV continues to spread – with no existing vaccine or cure – prevention remains the key strategy for curbing the epidemic. The most common mode of HIV transmission is sexual contact; thus, HIV prevention is closely linked to men’s and women’s sexual behaviour and reproductive health. Effective prevention programmes include interventions that promote abstaining from sex, delaying the onset of sexual activity, staying with one mutually faithful partner, limiting the number of sexual partners, consistently and correctly using condoms and counselling and testing for HIV. The most effective mix of these interventions depends on the characteristics of the groups infected with HIV. Effective programmes also consider the social, economic and cultural factors that influence people’s behaviour. Preventing HIV transmission from mothers to their infants is also key to saving lives (Gupta, 2000; Argeseanu, 2004; Kloos et al., 2007; Kidane, 1994; Statistical Abstract of Ethiopia. 2010). Women who are HIV positive need contraceptive choices and counselling to help them decide whether to have a pregnancy. Helping HIV-infected women avoid unintended pregnancies could prevent many HIV-positive births. Increasing contraceptive use to prevent such pregnancies appears to be at least as cost-effective as providing antiretroviral drug therapy during delivery and to new-borns of HIV-infected mothers. Key challenges for the future include controlling further spread of the epidemic in infants and young adults; treating and supporting the millions of people living with HIV; and mitigating the impacts of the epidemic in poor countries like Ethiopia. To meet these challenges, the international community, governments and civil society need to act. It is clear that much more needs to be done, especially in resource-poor countries.
Conclusions
Many children are dying, while many more are experiencing the scars that AIDS can leave on their lives – almost all of which is avoidable. The state of medical treatment is such that, in a developed country, a woman living with HIV can now be almost certain that her child will not be infected and yet there are still delays in making the appropriate tests and drugs available around the world. If infected with HIV, children can be effectively treated, and, given this treatment, can lead longer, healthier lives—yet they continue to die, because the treatment is not available in many countries. However, developing countries like Ethiopia need not only the drugs to treat children, but also special training for staff and funding to enable treatment and on-going care. This study will be immensely useful for the policy makers and health care service providers, who already possess the tools to save children from needless suffering, but the tools are not reaching most of those who need them. Therefore, to understand in greater detail how HIV prevalence correlates to poor health in terms of the epidemic, further in-depth analysis on existing data and other data sources is strongly recommended.