
Abstract
Human immunodeficiency viruses (HIV) counselling and testing (HCT) plays a major role in the continuum of HIV programmes in Nigeria. However, HIV-related stigma (STGM) poses a serious threat to its success. Consequently, a cross-sectional study was carried out to examine whether STGM mediates the relationships between the explanatory variables (HIV-related knowledge, HIV transmission misconception (MSHIV), and perceived seriousness of HIV/acquired immune deficiency syndrome (AIDS)), and the outcome variable (HCT service utilization). The mediation analysis was undertaken using data from 768 individuals collected through convenience sampling in the Local Government Areas of Alimosho, Ikorodu, and Surulere of Lagos state, and deploying partial least squares–structural equation modelling. The results show that STGM played a mediating role in the relationship between MSHIV, perceived seriousness of HIV/AIDS, and HCT utilization. These findings offer wide ramifications for the intensification and enforcement of Nigeria’s HIV/AIDS Anti-Discrimination Act 2014 to eradicate stigma, which is important to enhance uptake of HCT to achieve the United Nations’ 90-90-90 HIV targets by 2020.
Keywords
Introduction
With a population of about 182 million (National Population Commission, 2017), Nigeria ranked third among countries burdened with human immunodeficiency viruses (HIV)/acquired immune deficiency syndrome (AIDS) in the world (United Nations Programme on HIV and AIDS, 2018). According to the National Agency for the Control of AIDS, (2019), the latest national HIV prevalence rate was 1.4% for the age group 15–49 years old, while 1.9 million people are living with HIV. HIV counselling and testing (HCT) is among the several programmes established to reduce the spread of HIV in Nigeria. HCT plays a critical role in the continuum of HIV programmes, which range from prevention to care (Bwambale et al., 2008; Ostermann et al., 2015; United Nations Programme on HIV and AIDS, 2015).
Studies have shown that HCT contributes to reducing risky sexual behaviour which may ultimately lead to a reduction in the probability of HIV transmission (Denison et al., 2008; Fonner et al., 2012). HCT affords individuals the opportunity to know their serostatus and spur their motivation for self-care (Okawa et al., 2017). Also, it plays a significant role in attaining the much touted United Nations’ 90-90-90 HIV targets by 2020 and Sustainable Development Goals (SDGs) by 2030 (United Nations Programme on HIV and AIDS, 2014). However, the utilization of this essential HIV service in Nigeria, like other sub-Saharan Africa (SSA) countries, is still low, which is a major policy concern. According to Staveteig et al. (2013) about 50% of people living with HIV/AIDS (PLWHA) in SSA do not know their HIV status. According to the Nigeria Demographic and Health Survey report, only 21.5% adult men and 29.5% adult women were tested for HIV in Nigeria in 2013 ( Nigeria Demographic and Health Survey, 2014).
One of the major problems confronting HCT utilization is the stigma associated with HIV infection (National Agency for the Control of AIDS, 2015). HIV-related stigma (STGM) is among the non-financial factors that pose significant barriers to the successful implementation of HCT in high HIV burdened SSA countries. Stigma is regarded as a negative judgement cast by the society which is often generated by fear, ignorance and false belief (Word Health Organization, 2015). Fear of knowing one’s HIV status owing to the stigmatization of HIV-positive individuals has been documented in the literature as the primary barrier to HCT utilization among youths and students (Buldeo and Gilbert, 2015; Ndabarora and Mchunu, 2014; Nothling and Kagee, 2013); pregnant women attending antenatal health care facilities (Sarker et al., 2007; Workagegn et al., 2015); PLWHA (Earnshaw et al., 2014, 2016), and the population in general (Bova et al., 2016; Bwambale et al., 2008; De Jesus et al., 2015; Ma et al., 2007). Although Studies that demonstrate a bivariate relationship between HIV serostatus with knowledge about HIV and stigma have been reported (e.g. Yang et al., 2006), little is known about the mediation effects of STGM on the relationship between HIV-related knowledge (KNHA), HIV transmission misconception (MSHIV), perceived seriousness of HIV/AIDS (PHSEV) and HCT service utilization (HCTU). Therefore, the purpose of this study is to examine the mediating role of STGM on HCT utilization.
In his contribution to stigma theory, Goffman (1963) defined stigma as “an attribute that is deeply discrediting”. STGM is specifically defined, according to Steward et al. (2008), as “socially shared knowledge about the devalued status of people living with HIV”. Also, Nyblade and MacQuarrie (2006) describe HIV stigma as the “beliefs and attitudes that deeply discredit a person or group because of an association with HIV”. STGM often attracts discrimination, prejudice, and discrediting toward PLWHA and individuals (such as friends, family members, and caregivers), groups, associations, and communities that are associated with them (Bos et al., 2013; Steward et al., 2008). STGM also manifests in different settings, such as educational bodies, workplaces, health care centres, and religious institutions (Feyissa et al., 2012; Parker and Aggleton, 2003; Sekoni et al., 2012; Ulasi et al., 2009).
This STGM has been recognized as an essential driver of epidemics, which poses a serious threat to the effectiveness of HIV/AIDS prevention, treatment, and care programmes (Herek, 1999; Niang et al., 2003; Parker and Aggleton, 2003; Piot, 2006). For example, Yang et al. (2004) reported that STGM was associated with a decrease in individual’s willingness to participate in HIV and sexually transmitted disease prevention intervention activities. Derlega et al. (2002) found that stigma prevented people living with HIV from disclosing their serostatus, and discouraged them from assessing available HCT and treatment services. The low level of HIV/AIDS awareness is associated with discriminating and stigmatizing attitudes towards PLWHA (Babalola, 2007; Vorasane et al., 2017). Therefore, we hypothesized stigma as a mediator in the relationship between KNHA, HIV/AIDS transmission misconception, PHSEV, and HCTU. The analytical framework and hypotheses for the mediating effect of STGM is presented in Figure 1.
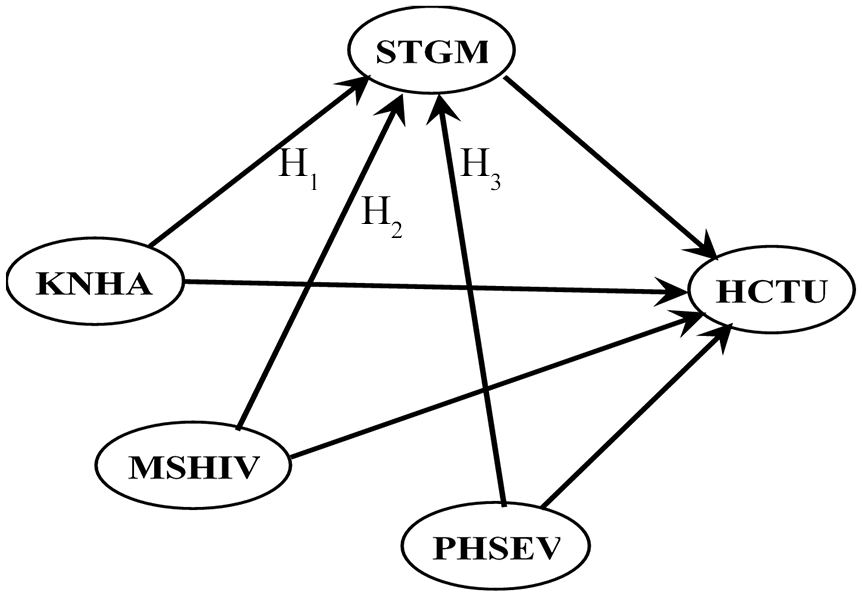
Conceptual/analytical framework of human immunodeficiency viruses (HIV)-related stigma mediator.
The following three hypotheses were tested in the mediation model:
Hypothesis 1: STGM significantly mediates the relationship between KNHA and HCTU.
Hypothesis 2: STGM significantly mediates the relationship between MSHIV and HCTU.
Hypothesis 3: STGM significantly mediates the relationship between PHSEV and HCTU.
Materials and methods
Study location and participants
The study was conducted in Lagos state, Nigeria. The three Local Government Areas (LGAs)—Alimosho, Ikorodu, and Surulere covered in this study had an estimated 2.3 million people according to Nigeria’s 2006 population census. Lagos state has a metropolitan population of about 17 million. It is among the states with the highest HIV/AIDS prevalence rate (1.4%) in Nigeria (National Agency for the Control of AIDS, 2015). Lagos state is in the southwestern part of Nigeria and has 20 LGAs and 38 Local Council Development Areas. The state is politically divided into three districts: North, Central and South Senatorial Districts. The participants were adult men and women aged 20 years and above chosen from the households in the selected areas.
Research design, sampling procedure, and sample size
The study deployed a cross-sectional survey using a nonprobability sampling method from the target population. A nonprobability sampling method was adopted because of the sensitivity of the topic involved, as well as a lack of data on both users and non-users of HCT in the study area. To improve the representativeness of the respondents for a reasonable interpretation and generalization of the results, this study combined both quota and convenience sampling methods in which one LGA was selected from each of the senatorial districts of Lagos state (Lagos East senatorial district – Ikorodu LGA, Lagos West senatorial district – Alimosho LGA, and Lagos Central senatorial district – Surulere LGA) based on their HIV prevalence rate. Trained research enumerators went to the selected locations to recruit eligible individuals from the households for the survey. The enumerators obtained informed consent from each participant before pilot testing and revising self-administered questionnaires. The completion time for the questionnaire was approximately 40–60 minutes. A sample of 768 adults were recruited from the three LGAs: Alimosho; Ikorodu; and Surulere.
Data collection, instrument and measurements
Data for this study were collected using the pre-tested structured questionnaire administered face to face by twelve enumerators from the three LGAs of Lagos state lasting from May 2015 to July 2015. The questionnaires were administered to the individuals who were available in the households at the point of data collection. The questionnaires were presented in English with close-ended questions. The survey instrument was structured into sections: sociodemographic information; knowledge about HIV/AIDS and HCT; STGM questions; and MSHIV. The questions mainly covered the three latent predictor constructs: KNHA; MSHIV; and PHSEV; and the mediator variable, STGM. The latent constructs were measured by multi-items, which were sourced from previous studies with some modifications to suit this study.
STGM
According to Baron and Kenny (1986), a “variable may be said to function as a mediator to the extent that it accounts for the relation between the predictor and the criterion”. The mediator, STGM latent construct was measured using 9-items, which were adapted from past studies (Berger et al., 2001; Genberg et al., 2008; Nigeria Demographic and Health Survey, 2014; Nyblade and MacQuarrie, 2006; Nyblade et al., 2005; Van Brakel, 2006). The items include: “Can you play with a person who has HIV?”; “Can you eat/share food with a person who has HIV”; and “Can you buy things from a person who has HIV?”. These measurement items or indicators were measured on a 3-point categorical nominal scale in which 1 stands for “Agree”, 2 stands for “Disagree”, and 3 stands for “Don’t Know/Not Sure/Depends”.
KNHA
Three items were used to measure this construct: “Have you heard about HIV and AIDS”; “Do you know someone infected with HIV virus”; and “Do you know someone who died as a result of AIDS”. These indicators were measured on a 2-point nominal scale: yes and no (Nigeria Demographic and Health Survey, 2014; Yang et al., 2007).
MSHIV
This latent predictor was operationalized using seven items, such as, “Can HIV can be transmitted through mosquito bites?”; “Can HIV be transmitted by sharing foods or drinks with an HIV infected person?”; and “Can HIV be transmitted by shaking hands or hugging an HIV infected person?” These items were measured on a 2-point nominal scale: yes and no.
PHSEV
A 9-item questionnaire assessed the perceived severity of HIV/AIDS. The measurement items include, “AIDS is a hopeless disease”, “AIDS would be a serious problem for me”, “I believe contracting HIV/AIDS would interfere with my role in the family” (Janz and Champion, 2002; Rosenstock, 2005). Responses were measured on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree).
HCTU
The criterion variable, HCTU, was operationalized by knowledge about HCT and HCT testing history. Two main items were used to measure the latent construct, HCTU: “Do you know where to get an HIV test?”; and “Have you been tested for HIV?”
Analytic techniques
We deployed two statistical software packages – SPSS v22.0 and WarpPLS 5.0 – to analyse the primary data collected. SPSS v22 was used to examine the descriptive statistics, while WarpPLS version 5.0 was deployed in the structural equation modelling (SEM) analysis of mediating effects of STGM. SEM is preferred over regression analysis when two conditions are clear. First, SEM tends to produce less biased results when using cross-sectional datasets. Secondly, it is preferred when there is more than one measurement item for each of the constructs (Frazier et al., 2004; Gunzler et al., 2013; Holmbeck, 2002; Jaccard and Wan, 1996; Peyrot, 1996). In light of the above, we deployed partial least squares–structural equation modelling (PLS-SEM) to analyse the mediating effect of STGM. WarpPLS is a robust PLS-based SEM software developed by Ned Kock. PLS is a non-parametric variance-based SEM approach suitable for SEM analysis where the sample is not too large and data are not normally distributed (Kock, 2015).
Mediation analysis
In the analysis of the mediation effects of STGM, we deployed the alternative approach to the analysis of mediating effect as suggested by Preacher and Hayes (2008) and (Kock, 2014). We first examined the significance of the direct effect of the exogeneous variables on the criterion variable and subsequently assessed the significance of the indirect effect from exogenous variables via the mediator to criterion variable. Both the simple models – which show the bivariate relationship between the constructs and the complex model that includes the mediator – were simultaneously estimated using WarpPLS (Kock, 2015). The PLS-SEM mediation analysis followed the Anderson and Gerbing (1988) recommendation of a two-step approach, which takes care of both measurement and structural model analyses. We used the Stable-3 resampling method in WarpPLS for the analysis (Kock, 2017).
Stage 1: Assessment of measurement model
The measurement models were first analysed to establish the validity and reliability of the measured items of the three predictors and mediator constructs in the model.
Reliability and validity of measurement items
We first established the reliability of the measurement items of each construct by examining their individual loadings to confirm whether they satisfied the recommended minimum loading of 0.5 (Bagozzi and Yi, 1988). In addition, we assessed the reliability of each construct in the model by using the widely used construct reliability measure in survey research, the Cronbach’s alpha (recommended minimum loadings = 0.70) and composite reliability (recommended minimum loadings = 0.60) (Chin, 1998; Fornell and Larcker, 1981; Wetzels et al., 2009). The two validity tests recommended in PLS-SEM analysis are convergent and discriminant tests (Chin, 2010; Hair et al., 2012). The criteria we considered for the establishment of convergent validity were item factor loadings on parent factor (which must be above 0.50 and significant at p < 0.05) and average variance extracted (AVE) (above 0.50). The discriminant validity was examined by comparing the correlations among the latent constructs in the model with the square roots of AVE for each construct (Chin, 2010). According to Fornell and Larcker (1981), to establish discriminant validity all values in the diagonal must be higher than other elements that are off-diagonal. Items that failed to meet the minimum criteria were removed from the model.
Multicollinearity test
We checked for the presence of multicollinearity in our measurement models by assessing the variance inflation factor (VIF). To establish absence of multicollinearity in the SEM model, Kock (2015) recommended a VIF of 3.3.
Stage 2: Assessing structural model of STGM mediator
Having satisfied the reliability and validity of the measurement model in stage 1 of the analysis, we estimated the structural model of the mediating relationship of STGM on HCT utilization. Before we examined the mediating effect in the path analysis, we first considered the coefficient of determination (R2) and effect sizes. To establish the mediation effect of a mediating variable in the model, the extant literature suggests three outcomes of mediating effect: full or complete; partial; and no mediation effect (Baron and Kenny, 1986; Hayes and Preacher, 2014; James and Brett, 1984; Kock, 2014). We deployed the mediation analytical approach of Kock (2014), which requires testing for the significance of both the direct and indirect effects to establish the presence of mediation in the model. Full mediation is achieved when the path running from independent variables to the dependent variable (direct effect) is not significant while the path through the mediator variable (indirect effect) is significant. If both the direct and indirect effects are significant then there is partial mediation. Lastly, if the path running from the mediator to dependent variable is not significant, there is no mediation effect.
Ethical considerations
This study protocol was approved by the Health Research and Ethics Committee of Lagos State University Teaching Hospital, (LASUTH) Ikeja, Lagos State, Nigeria (Approval No: LREC/10/06/497).
Results
Respondents’ sociodemographic characteristics
Table 1 presents the summary of participants’ sociodemographic characteristics. Of the 768 participants, 54% (413) were males, 57% were married, 88% were below 50 years of age, 98% have heard about HIV/AIDS, and only 18% know someone living with HIV/AIDS.
Sociodemographic characteristics of the participants.
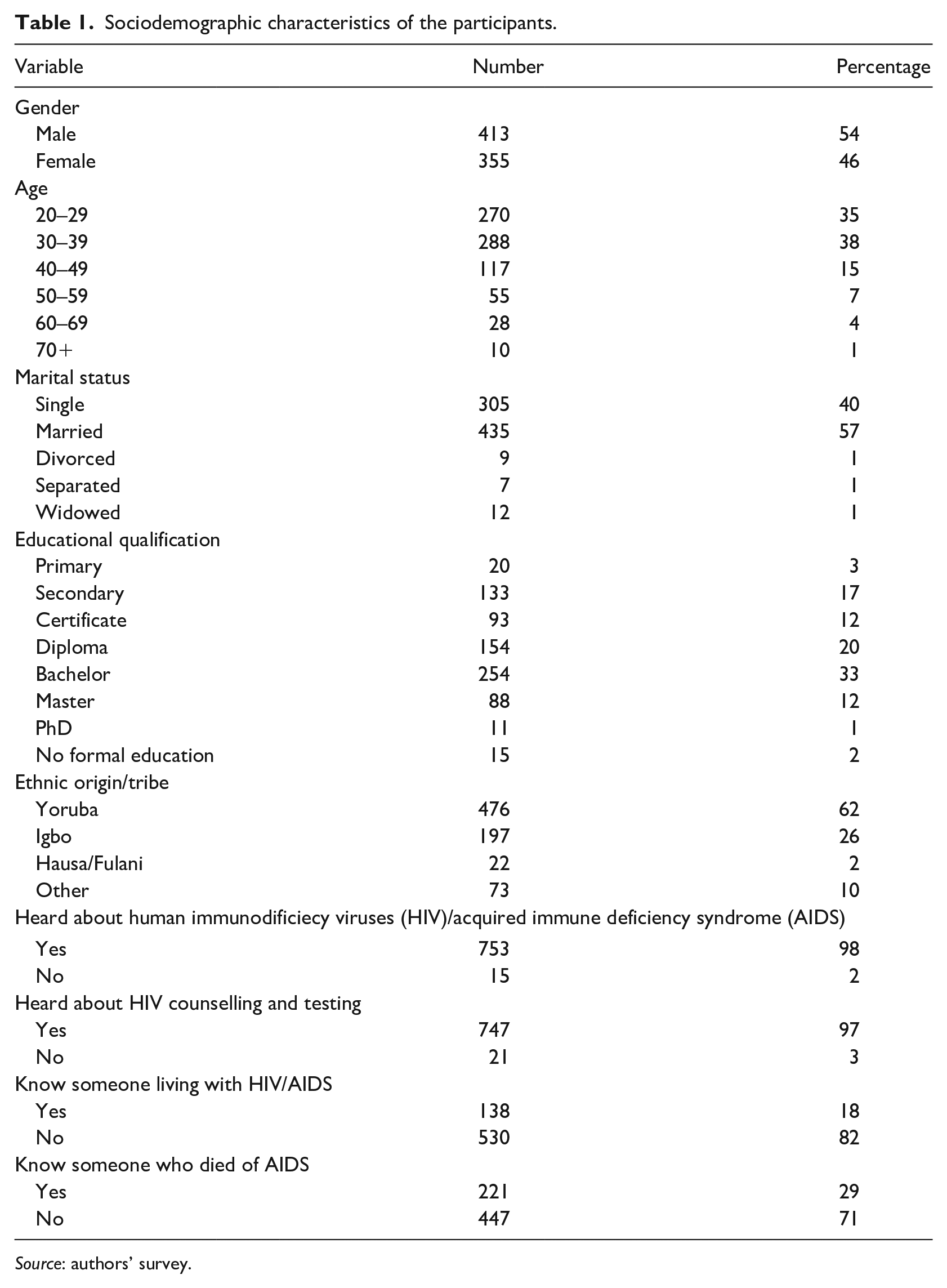
Source: authors’ survey.
Mediation analysis (PLS-SEM)
Assessment of the measurement model
The PLS-SEM analysis results show that the measurement indicators passed the items reliability test with loadings more than the recommended value (Table 2). Therefore, all the constructs measurement items show a satisfactory level of reliability. Composite reliability for all predictor constructs and mediator were higher than the recommended 0.70 (Hair et al., 2011; Urbach and Ahlemann, 2010). Also, the Cronbach’s alpha statistics for the constructs were satisfied (>0.60) (Lyberg et al., 1997), which indicates good construct reliability.
Reliability and convergent validity of the measurement model.
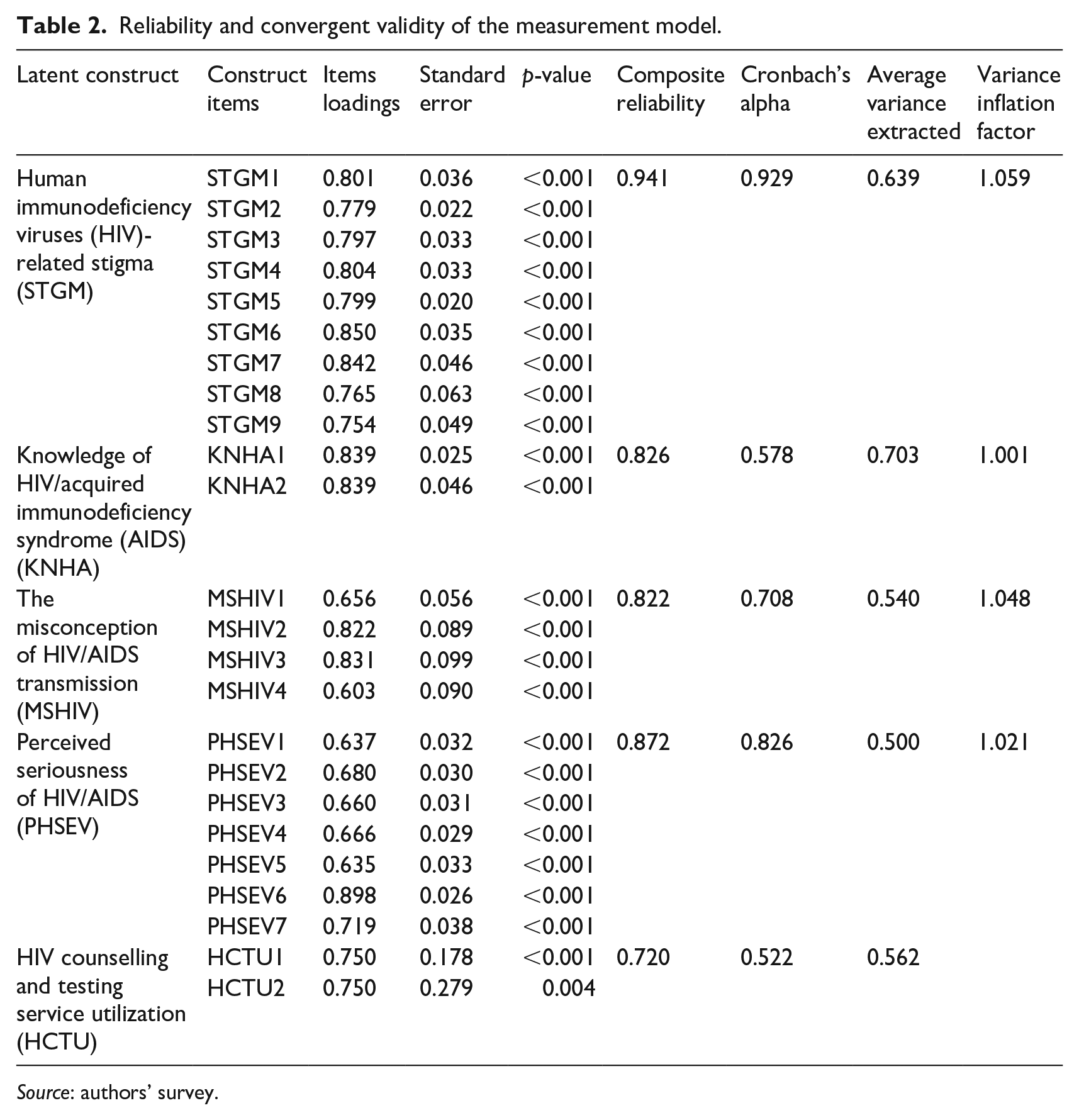
Source: authors’ survey.
The results of the measurement model as presented in Table 2 reveal that all the measurement item loadings were more than the recommended minimum value of 0.50 and significantly loaded on the parent factor p < 0.05 (Gefen et al., 2000; Kock, 2015). AVE of all the constructs were well above the accepted threshold of 0.50 (Hair et al., 2013). Thus, all the latent predictor and mediator constructs satisfied the recommended minimum value and were considered valid. The discriminant validity results as shown in Table 3 reveal that all the values in the diagonal are larger than correlation values in both column and row. Therefore, the discriminant validity criterion was satisfied. In addition, as revealed in Table 2, the VIFs were lower than the Kock (2015) recommendation of 3.3. Thus, there was no multicollinearity among the predictor variables in the model.
Discriminant validity of the measurement model.
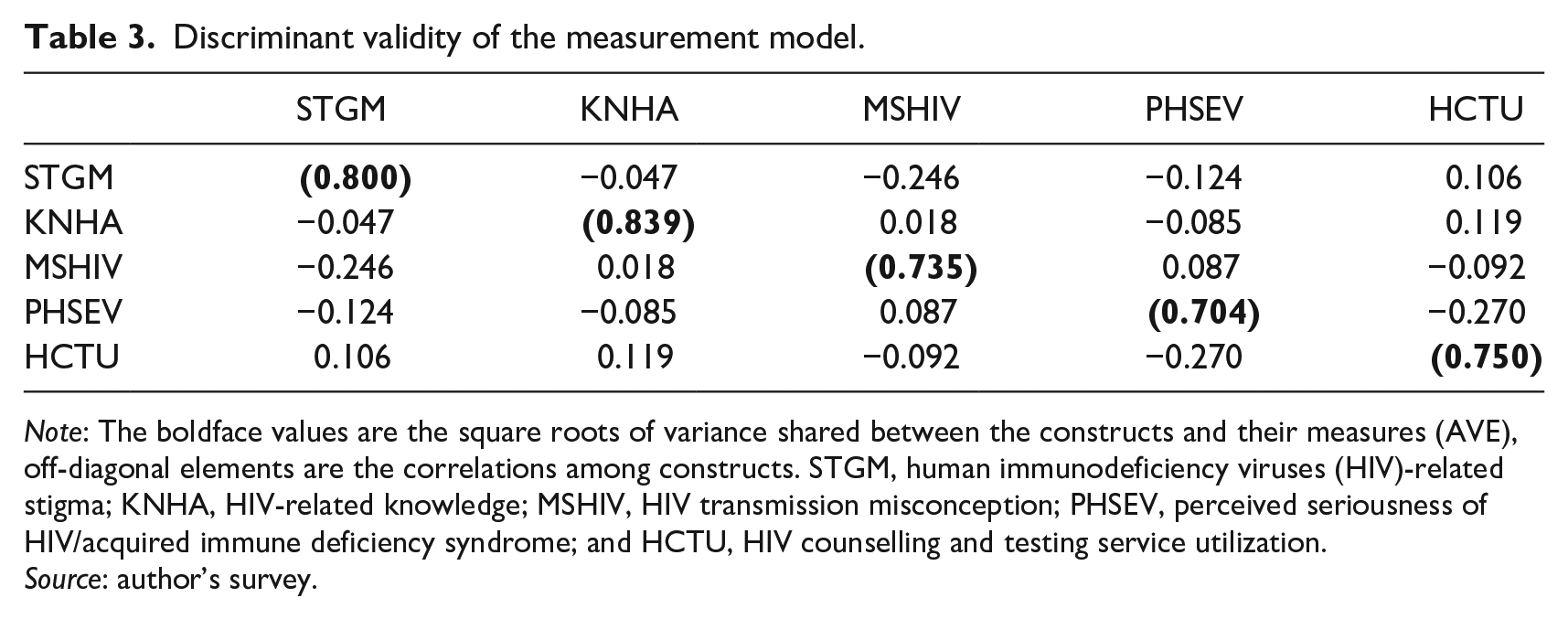
Note: The boldface values are the square roots of variance shared between the constructs and their measures (AVE), off-diagonal elements are the correlations among constructs. STGM, human immunodeficiency viruses (HIV)-related stigma; KNHA, HIV-related knowledge; MSHIV, HIV transmission misconception; PHSEV, perceived seriousness of HIV/acquired immune deficiency syndrome; and HCTU, HIV counselling and testing service utilization.
Source: author’s survey.
Assessment of structural model
The results of the structural model reveal that the R2 was 0.13 as shown in Figure 2, which signifies that all the four exogenous variables accounted for 13% variation in HCT. The R2 is low. The effect sizes range from 0.001 to 0.062 as shown in Table 3, which shows small effect sizes (Wong, 2016).
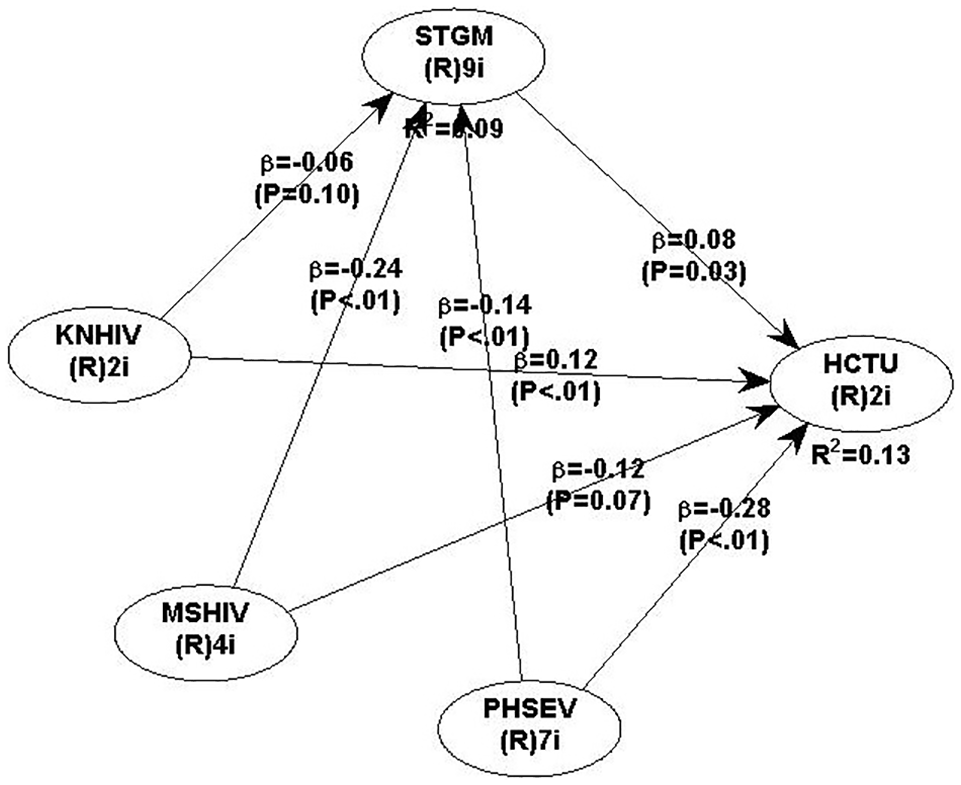
The estimated mediating model of human immunodeficiency viruses (HIV)-related stigma.
The mediation analysis and results
In this subsection, we present the mediation effect of STGM on the relationship between KNHA, MSHIV, PHSEV and HCTU as specified in the three hypotheses from the model.
Hypothesis 1: The results as revealed in Table 4, show that the direct path from KNHA to HCTU is significant (β = 0.119; standard error (SE) = 0.039; p = 0.001), while the indirect path from KNHA to HCTU through STGM was not significant (β = −0.005; SE = 0.005; p = 0.181). Thus, we can conclude that STGM did not mediate the relationship between KNHA and HCTU.
Hypothesis 2: The direct path from MSHIV to HCTU was not significant, (β = −0.121; SE = 0.084; p = 0.074). However, the indirect path was significant (β = −0.018; SE = 0.011; p = 0.054). Thus, there is evidence of full mediation effect. In other words, STGM served as a mediator in the relationship between the misconception of HIV transmission and HCTU.
Hypothesis 3: The direct path from PHSEV to HCTU was significant (β = −0.285; SE = 0.109; p = 0.005), while the indirect effect was also significant (β = −0.011; SE = 0.007; p = 0.059). The results indicate that stigma partially mediates the relationship between PHSEV and HCTU. The effect sizes of the mediation relationship fell within a small category (Chin, 1998).
Summary of direct, indirect, and total effect of the structural mediating model.
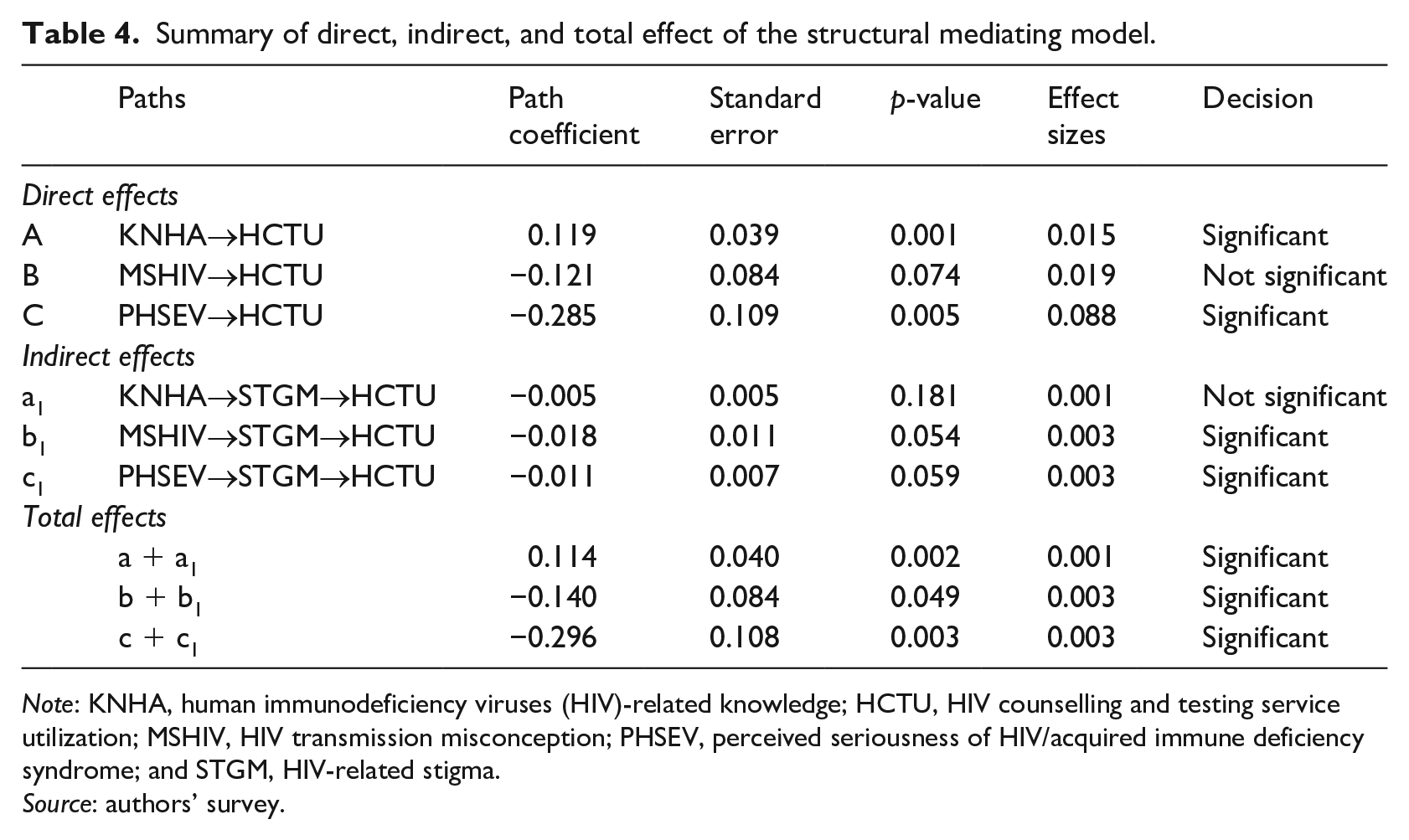
Note: KNHA, human immunodeficiency viruses (HIV)-related knowledge; HCTU, HIV counselling and testing service utilization; MSHIV, HIV transmission misconception; PHSEV, perceived seriousness of HIV/acquired immune deficiency syndrome; and STGM, HIV-related stigma.
Source: authors’ survey.
Discussion
This research examined the mediating effect of STGM on the relationship between individuals’ misconception about HIV transmission, KNHA, PHSEV, and HCT. The stigma associated with being HIV-positive served as a barrier to HCTU in Nigeria (Nyblade and MacQuarrie, 2006). Findings from this study reveal that two of the three hypotheses formulated were satisfied.
However, the results did not confirm our first hypothesis that STGM would significantly mediate the relationship between KNHA and HCTU, which contrasts with the findings of Yang et al. (2006). Moreover, the results show that KNHA has significant direct effects on HCTU and the relationship between them is positive, which suggests that an increase in awareness about HIV will increase the uptake of HCT. This finding concurs with AIDS-risk reduction behaviour with three components (Fisher and Fisher, 1992): information; motivation; and behavioural skills. Information about HIV can guide individuals to participate in activities that will reduce his or her risk of contracting HIV. Also, it supports Fisher et al. (1996), who found that information about HIV/AIDS was germane to AIDS risk reduction behaviour among college students in the United States.
Subsequently, we hypothesized that STGM would significantly mediate the relationship between MSHIV and HCTU. Our hypothesis was confirmed as the relationship between individuals’ misconception of HIV transmission and HCTU was mediated by STGM. Stigma associated with HIV/AIDS is significant in determining how individuals willing to do HIV tests will respond to HCTU. Information about HIV/AIDS transmission and specific methods of prevention are necessary requirements of action aimed at reducing HIV infections (Fisher and Fisher, 2000). According to Adeokun et al. (2006) and Qian et al. (2007), misconception about the HIV transmission mechanisms could impact on STGM and attract discriminating attitudes. An increase in stigmatization and discriminating attitudes towards individuals infected with HIV or living with AIDS could hinder HCTU. These findings agree with a qualitative study by Meiberg et al. (2008), in which AIDS stigma was found to be a solid barrier towards HIV voluntary counselling and testing among university students in South Africa. Low willingness to participate in the intervention programmes designed to protect against HIV infection and sexually transmitted diseases among rural–urban migrants in China was reported by Yang et al. (2004), which suggests that STGM plays a negative role in HCTU.
Finally, we hypothesized that STGM mediates the relationship between PHSEV and HCTU. Our hypothesis was confirmed as stigma associated with HIV/AIDS mediated the relationship between perception of individuals concerning the potential threats of HIV and HCTU, which shows that individuals may perceive HIV/AIDS to be a serious problem but the presence of stigma may hinder participation in HIV testing. In other words, people may be aware of the threat HIV/AIDS poses, and yet may not participate in HIV testing because of the fear of being stigmatized by society. Individuals’ perceptions about the seriousness of HIV and AIDS could lead to stigmatization of PLWHA, which in turn could adversely affect HCTU. The results concur with the findings of Meiberg et al. (2008) and Odimegwu et al. (2013) where fear and stigma associated with HIV were found to be strong barriers to HIV voluntary counselling and testing in Nigeria.
Also, Bova et al. (2016) found that the low testing rates and poor attitudes toward HIV testing were due to stigma attached to AIDS among African born men in the United States. Denial, fear of disclosure, fear of knowing one’s HIV status, social exclusion and isolation, negative reactions from partners and other people, were all tied up with HIV stigma, which invariably dissuade people from participating in HCT activities (De Jesus et al., 2015; Lindkvist et al., 2015; Ma et al., 2007; Sarker et al., 2007). Our result also partially concur with the findings of Yang et al. (2006), which showed that STGM mediated the relationship between the HIV knowledge and willingness to disclose HIV serostatus among rural–urban migrants in China. If stigmatization and negative attitudes rampantly manifest in ostracization, abuses, rejection, mistreatment, and denials, people will be deterred from seeking HIV testing. Therefore, the focus should not only be on promoting the benefits of having HIV tests, but also on eliminating HIV stigma in all its forms from society, which should enhance HCT uptake in Nigeria. Furthermore, consistent with the findings of Chin et al. (2003), the small size effect in the mediation models does not signify that the impact of stigma is inconsequential.
Conclusion
This study examined the effect of STGM on HCT. The findings show that stigma impacted negatively on the relationship between PHSEV, MSHIV, and HCT. The significant findings offer implications for HCT uptake in Nigeria specifically and the world generally. For HCT to contribute effectively towards the achievement of the first 90 of the United Nations’ HIV 90-90-90 targets by 2020 and SDGs by 2030 in Nigeria, the problem of stigmatization of PLWHA must be addressed. The Nigerian government must strive to achieve zero stigmatization and discrimination towards PLWHA in society. We recommend that the government and all stakeholders collaborate towards ensuring that STGM is eradicated or substantially reduced to improve HCTU, which inter alia, can be achieved by continuously educating people to have an attitudinal change towards PLWHA. Vigorous publicity and enforcement of the Nigeria HIV/AIDS Anti-Discrimination Act 2014 should be carried out to discourage people from stigmatizing individuals with HIV.
Is spite of its significance, the study has some limitations. Firstly, the study was conducted in an urban setting in Lagos state, which invariably has characteristics different from rural areas, and as such, the results obtained might not perfectly fit into other contexts. Secondly, the study deployed a cross-sectional survey, which does not allow the establishment of causality. Lastly, the HIV-stigma data obtained were based on the perception of the general population rather than the individual living with HIV and facing stigmatization and discrimination in society. Therefore, there is a possibility of biases, which might have led to overestimating or underestimating of the level of STGM.
Footnotes
Author’s note
Felix Oluyemi Adekunjo is also affiliated with the Department of Economics, Faculty of Social Sciences, Lagos State University, Lagos, Nigeria.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.