
Abstract
This study examined the trends and factors associated with early pregnancies and motherhood among young women in three sub-Saharan African countries: Malawi, Mali, and Niger. Descriptive and multivariate analyses showed that the prevalence of early childbearing declined significantly in all three countries between 2006 and 2016. Moreover, the determinants of age at first childbearing varied across these nations. It is crucial to implement programmes that encourage delaying the age of the first sexual debut. In addition, providing adolescent women with comprehensive knowledge about responsible and safer sex practices and motherhood is paramount in addressing this challenge.
Introduction
Adolescence is a vulnerable phase in human development, as it represents a transition from childhood to physical and psychological maturity (United Nations Children’s Fund (UNICEF), 2019). Pregnancy before a girl is physically, developmentally, and socially ready jeopardises her right to a safe, successful transition into adulthood (United Nations Population Fund (UNFPA), 2015). Adolescent pregnancies, known also as early pregnancies, defined as pregnancies below the age of 20 (World Health Organization (WHO), 2011), effectively derail girls’ childhood. Research emphasises that adolescent pregnancy and child birth is a serious medical and public health problem for both developed and developing countries, as it may affect the health and social and economic well-being of society at large (Chemuru and Srinivas, 2015; Franjić, 2018). Therefore, age at first childbearing is an important factor related to public health.
Adolescent pregnancy remains a major challenge occurring across the world. Statistics indicate that approximately 21 million girls below the ages of 15–19 give birth each year (Darroch et al., 2016), and at least 777,000 births occur to adolescent girls younger than 15 years in developing countries (Woog and Kågesten, 2017). Between 2015 and 2020, an estimated 62 million babies were born to mothers between the ages of 15 and 19 worldwide, 46% of them in sub-Saharan Africa (United Nations Department of Economic and Social Affairs, Population Division, 2019). There have been substantial improvements in adolescent pregnancy and early motherhood in the world over the past 20 years, but rates remain high in sub-Saharan Africa. Between 2015 and 2020, the adolescent birth rate was highest in sub-Saharan Africa, at 103 per 1000 women aged 15–19, down from 126 births between 2000 and 2005 (UNICEF, 2019). Unsurprisingly, the countries with the highest rates of adolescent fertility are found in this region (UNICEF, 2019).
Numerous scholars revealed that early childbearing was associated with a number of negative health, educational, social, and economic outcomes (Casterline and Lazarus, 2010; Kara and Maharaj, 2015; Loaiza and Liang, 2013). For that reason, there has always been particular interest to investigate different factors affecting young women at first childbearing. Findings from developing countries exposed that early childbearing is associated with a higher risk of maternal and neonate deaths as well as a higher overall fertility rate (Casterline and Lazarus, 2010; Kara and Maharaj, 2015; WHO, 2012). Globally, complications from pregnancy and childbirth are the leading causes of death among adolescent girls aged 15–19 (UNICEF, 2019).
Several studies have examined factors associated with early pregnancy and motherhood in developing countries. In the context of sub-Saharan Africa, a wide range of factors contribute to the high rates of pregnancies and childbirths among adolescents: poverty, educational status, religion, early marriage, early sexual debut, unequal gender power relations, lack of comprehensive sexuality education, poor knowledge of sexual and reproductive health services, and legal barriers to accessing services (Kassa et al., 2018; Wado et al., 2019; Yakubu and Salisu, 2018). The education of women has been considered as a major protective factor for early pregnancy: the more years of schooling, the fewer early pregnancies (Kassa et al., 2018; Wado et al., 2019; WHO, 2011). Likewise, it has been found that material living conditions affect girls’ reproductive behaviour. Scholars have emphasised that adolescents and young people’s attitudes towards sexuality, marriage and early motherhood are shaped largely by the parent or husband’s financial capability to meet their basic needs (Kamal et al., 2015; Kara and Maharaj, 2015; Wado et al., 2019; Yakubu and Salisu, 2018). Indeed, early childbearing is dangerous, and girls from poor households are most likely to become pregnant during adolescence (Kara and Maharaj, 2015; Wado et al., 2019; Yakubu and Salisu, 2018). Researchers have identified that the place of residence is associated with reproductive behaviour, given that it is an important element of social identification and affects economic opportunities. Findings from sub-Saharan Africa underline that a rural environment is favourable for early sexual debut, early marriage, and early motherhood (Kara and Maharaj, 2015; Kassa et al., 2018). The broader cultural milieu and social institutions always affect young women’s reproductive behaviour. Researchers found that in sub-Saharan Africa and South Asia, motherhood is often simply seen as what girls are ‘for’; their social value is firmly rooted in their capacity for reproduction (Hindin and Fatusi, 2009; Rossier, 2007). Scholars have shown that early sexual activity is most often unprotected and induces a high prevalence of early and unwanted pregnancies or early motherhood (Iklaki et al., 2012; Yakubu and Salisu, 2018). Therefore, early sexual activity is an exposure factor in the risk of early motherhood, and the sooner this initiation, the longer the exposure time would be. However, child marriage is identified as one of the key drivers of teenage pregnancies, especially in South Asia and sub-Saharan Africa (Raj et al., 2009; UNFPA, 2012; WHO, 2011). Girls who get married early habitually have their experience of pregnancy and childbirth at a young age due to their higher frequency of sexual activity. The UNFPA (2015) emphasises that 9 out of 10 births between the ages of 15 and 19 in developing countries occur within early marriage where there is often an imbalance of power, no access to contraception, and pressure on girls to prove their fertility.
There is a need for a context-specific understanding of the factors that affect early childbearing of adolescent women, since sub-Saharan Africa is not homogeneous, and determining factors of teenage pregnancy and motherhood might differ sizeably across countries. Therefore, this paper focuses on the socioeconomic, demographic and behavioural determinants of young women’s age at first childbearing with special reference to the situation in Niger, Mali and Malawi.
Methods
Data sources
Data used for the analyses come from the Malawi Standard Demographic and Health Survey (2010, 2015–2016, 2017), the Mali Standard Demographic and Health Survey (2006, 2012–2013, 2014) and the Niger Standard Demographic and Health Survey (2006, 2012). Sub-samples of young women aged 15–24 who were pregnant at the time or who had already given birth were used.
Conceptual framework
The conceptual framework for this study was grounded on an updated Adamchak et al.’s (2000) Model for Factors that Influence Youth Reproductive Health. This model focuses on explaining the important social, cultural, and cognitive variables and their interrelationships underlying the behaviours used in predicting reproductive health. Consistent with this model, individual demographic, socioeconomic and cultural characteristics, family planning and behavioural characteristics may be conceptualised as factors that mould fertility among young women in sub-Saharan Africa (Figure 1). Demographic factors involve the woman’s age, marital status and age of her husband/partner. Socioeconomic and cultural factors include variables such as woman’s educational level and literacy, household wealth quintile index, woman’s employment status, exposure to media, husband/partner’s education, region, place of residence, religion and ethnicity. With reference to family planning factors, variables including knowledge of ovulatory cycles, knowledge of contraceptive methods and ever-used method or tried to delay pregnancy were considered. Behavioural characteristics are the most immediate cause of reproductive health outcomes such as age at first marriage and age at first intercourse.
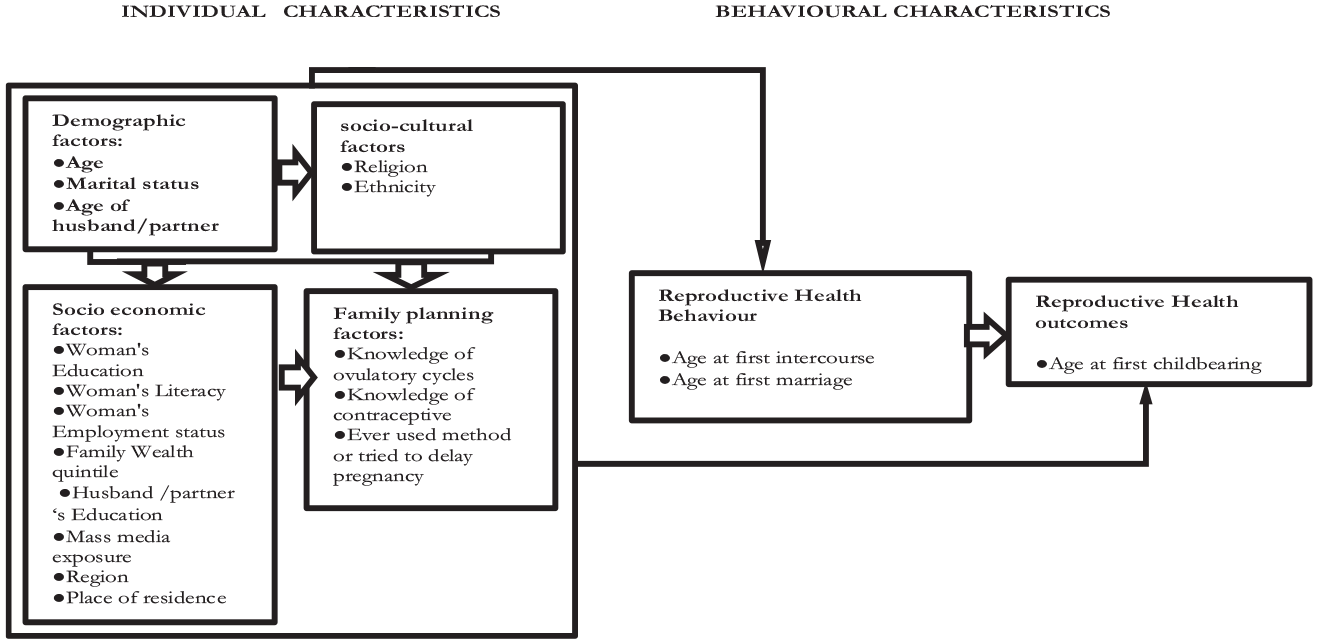
Conceptual framework of the study (Apdated from (Adamchak et al.’s, 2000)).
Study setting
This study was carried out in three sub-Saharan African (SSA) countries namely Malawi, Mali and Niger.
Malawi is a landlocked country in Southern Africa, has an estimated population of 19.1 million, with about 83% living in rural areas in 2020 and 44% aged below 15 years (Population Reference Bureau (PRB), 2020). The country had a Human Development Index (HDI) of 0.485 in 2018 (Conceição, 2019). The total fertility rate (TFR) was 4.2 per woman in 2018 (PRB, 2020), an adolescent birth rate (ABR) of 137.6 per 1000 (WHO, 2020), and a child marriage prevalence rate of 42% (UNICEF, 2018). Under the Constitution, the minimum legal age of marriage is 18 years, with no exceptions (African Child Policy Forum (ACPF), 2018). Malawi’s National Youth Policy of 2013 (Ministry of Youth and Sports, 2013) is protective against teenage pregnancies. Furthermore, the National Sexual and Reproductive Health and Rights (SRHR) Policy (2017–2022) commits to positioning adolescent sexual and reproductive health as a strategy for empowerment, development and social well-being (Ministry of Health, Malawi, 2016).
Mali is a landlocked country in the Western Africa region with an estimated population of 20.3 million in 2020 (PRB, 2020). In total, 43% of the population live in urban areas, and 48% are younger than 15 (PRB, 2020). Mali is predominantly (94%) Muslim (Central Intelligence Agency (CIA), 2020); the HDI for 2018 was 0.427 (Conceição, 2019). The country had the worst ABR at 164 per 1000 during the period 2010–2018 (WHO, 2020), one of the worst TFRs at 6.3 births per woman in 2018 (PRB, 2020), and the child marriage prevalence of about 52% (UNICEF, 2018). The Code of Persons and the Family 2011(Assemblée Nationale République du Mali, 2011) provides 18 years as the minimum legal age for civil marriage. The ‘Plan d’Action National Budgétisé de Planification Familiale du Mali 2019–2023’ (Ministère de la Santé et des Affaires Sociales du Mali, Direction Générale de la Santé et de l’Hygiène Publique, 2019) and ‘Plan d’action multisectoriel de la santé des adolescents et des jeunes (2017–2021)’ aim to increase the use of family planning services and reduce the incidence of early and/or unwanted pregnancies among adolescent girls and young people in Mali.
Likewise, Niger is a landlocked country located in Western Africa and home to 24.2 million inhabitants, youthful with 51% below the age of 15 and predominantly rural (84%; PRB, 2020). The population is mostly Muslim (99%; CIA, 2020). The country had the world’s lowest HDI (0.377) in 2018 (Conceição, 2019). With an ABR of 154.0 per 1000 (WHO, 2020), a TFR of 7.1 per woman (PRB, 2020), and a child marriage prevalence of 76% in 2018 (UNICEF, 2018), Niger still exhibits the highest fertility rate and child marriage prevalence in the world. The legal minimum age of marriage for women is observed at 15. The Niger Government has implemented several initiatives and projects to promote adolescent’s reproductive health and reduce adolescent pregnancy and motherhood. In 2015, the Niger Government has developed and adopted the National Strategic Plan for the Prevention of Adolescent Pregnancy (United Nations Population Fund West and Central Africa Regional Office, 2017).
Statistical analyses
Descriptive and multivariate analyses were used. At the descriptive level of analysis, the characteristics of the sample as well as the prevalence and trends of early childbearing were analysed. The Pearson chi-square test was used to examine the association between independent and outcome variables. Moreover, the Pearson product moment correlation between independent variables was calculated to check for high intercorrelations among independent variables. A generalised linear model specifying binomial distribution and negative log–log link further established the determinants of age at first childbearing. The Statistical Package for Social Sciences, Version 25.0, was used for estimations. All analyses were weighted to account for survey design. For the consideration of the country aspect of analysis, descriptive and multivariate analyses were performed independently for each country.
Selected study variables
Dependent variable
Young women’s age at first childbearing was employed as the dependent variable of the study.
Age at first childbearing determines the age of the mother at the time of the first pregnancy or first birth. Age at first childbearing is dichotomised by assigning the value of 0 for age 20 and above, and the value of 1 for age at first childbearing birth below 20; based on 20 years as the advocated age at first pregnancy.
Independent variables
Eighteen independent variables grouped into socioeconomic and cultural, demographic, planning family and behavioural characteristics were used in the analyses, explicitly education, literacy, wealth index, employment status, mass media exposure, religion, ethnicity, current age, marital status, knowledge of ovulatory cycles, knowledge of contraceptive methods, ever used method or tried to delay pregnancy, husband’s/partner’s education, age of husband/partners, region, place of residence, age at first sexual intercourse and age at first marriage/cohabitation.
Results
Trends and distribution of age group, behavioural, and family planning characteristics
Table 1 reveals significant increases in age at first intercourse in Niger and Mali during the period of study. The percentage of young women who faced early sexual intercourse (by 16 years) in Niger significantly decreased from 67.9% to 62.2% between 2006 and 2012. Similarly, early sexual activity in Mali declined from 63.7% in 2006 to 59.2% in 2013. In reverse, no significant variations were detected in age at first sexual activity Malawi. Regarding the age at first marriage, findings show 87.9%, 78.8% and 59.4% of adolescents (in Niger, Mali and Malawi, respectively) had experienced early marriage (by 18 years), according to the latest DHS surveys. However, significant declines in the proportion of early marriage were observed in all target countries between 2006 and 2016 (1.7%, 6% and 5% in Niger, Mali and Malawi, respectively). Overall, the three countries experienced an increase in adolescents’ knowledge of ovulatory cycle and contraceptive methods.
Trends and distribution of age group, behavioural and family planning characteristics in Niger, Mali and Malawi.
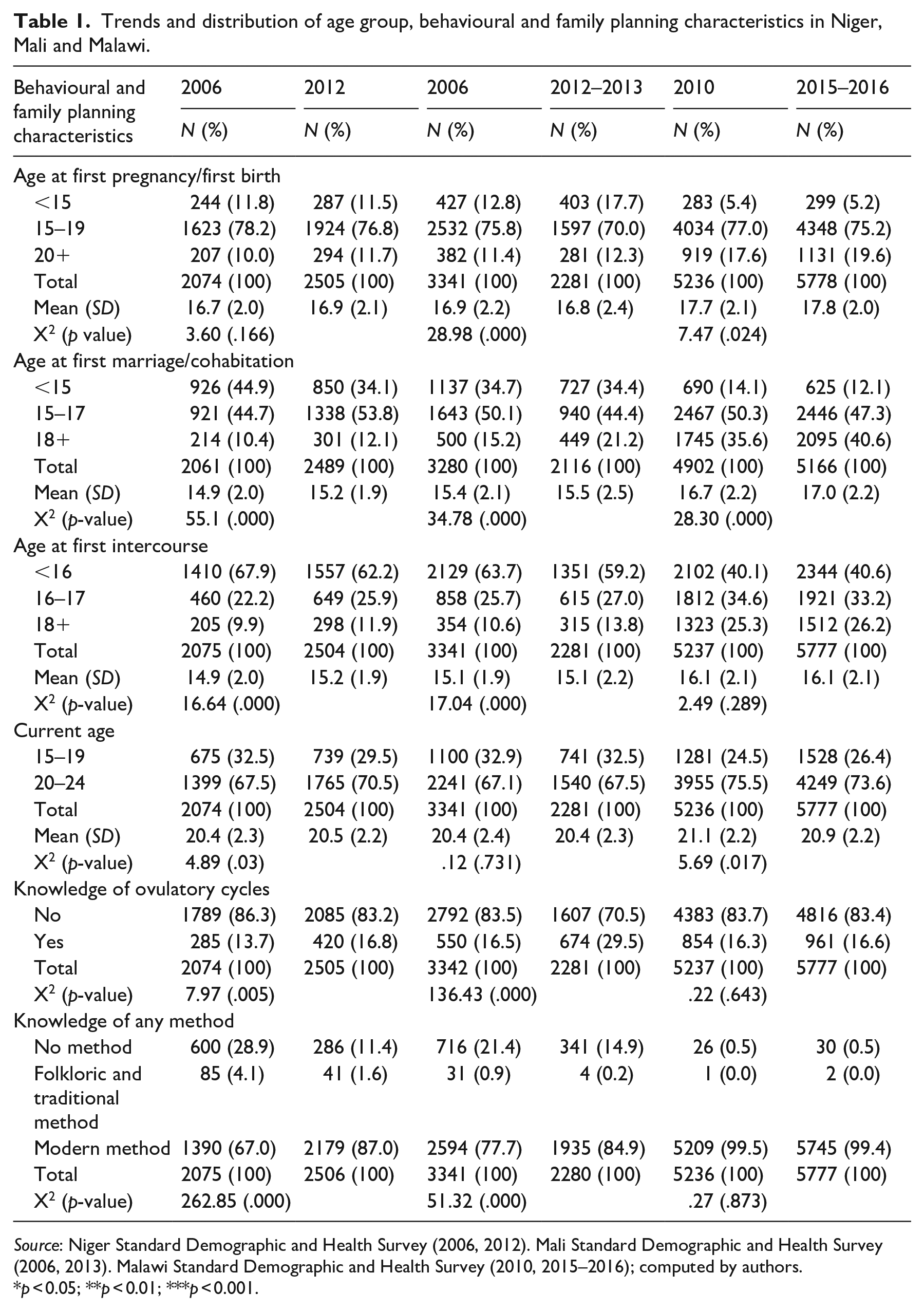
Source: Niger Standard Demographic and Health Survey (2006, 2012). Mali Standard Demographic and Health Survey (2006, 2013). Malawi Standard Demographic and Health Survey (2010, 2015–2016); computed by authors.
p < 0.05; **p < 0.01; ***p < 0.001.
Trends in early childbearing
Table 1 shows that most of the young women experienced early childbearing (by 20 years) in all the three countries (88.3%, 87.7% and 80.4% in Niger, Mali and Malawi, respectively), and few (11.5%, 17.7%, 7.4% and 5.2%, in that order) experienced it in their early adolescence (by 15 years), according to the latest DHS surveys. It transpires that early childbearing remained a crucial issue in the three countries. Over time, the prevalence of early childbearing in Malawi significantly dropped to 80.4% in 2016, down from 82.4% in 2010. Likewise, early childbearing in Mali declined from 88.6% to 87.7% between 2006 and 2013. In Niger, however, no significant change in the prevalence of early childbearing was noticed between 2006 and 2012.
Age at first childbearing by background characteristics
Women’s education and literacy were significantly related to the age at first childbearing in Niger, Mali and Malawi. As shown in Appendix Table 2, the prevalence of early childbearing was higher among women with no education (89.9%, 89.0% and 86.1% in Niger, Mali and Malawi, respectively), compared to those with secondary and tertiary education (70.4%, 81.6% and 63.3%, in the same order). This suggests that women’s age at first childbearing varied with mothers’ level of education. Appendix Table 2 highlights that the age at first childbearing significantly varied according to women living either in rural or urban areas in the three countries studied. On average, young women who resided in a rural area were more likely to enter into motherhood early than those who resided in an urban area. Likewise, other socioeconomic variables, particularly the family wealth index, husband’s/partner’s education and region were associated with age at first childbearing in all three of the target countries. Besides, mass media exposure was found to be associated with age at first childbearing in Niger and Malawi. In turn, women’s religious belief and ethnicity were found to be associated significantly with the age at entry into motherhood in Malawi. In the light of this, the proportion of early motherhood increases from Christian mothers (79.6%) to Muslim mothers (85.6%).
The results from Appendix Table 2 indicate that women’s age and husband’s/partner’s age were associated with the age at first childbearing in all the three countries, while marital status was associated with the age at first childbearing in Mali and Malawi.
With regard to the mothers’ family planning characteristics, Appendix Table 2 shows significant associations with the knowledge of ovulatory cycles and contraceptive methods. It shows a higher prevalence of early childbearing (88.7%, 89.1% and 80.7% in Niger, Mali and Malawi, respectively) among women who had no knowledge of ovulatory cycles, in comparison with those who had knowledge of ovulatory cycles (86.1%, 84.3% and 79.0% in that order).
Behavioural characteristics, namely age at first marriage/cohabitation and age at first intercourse, were significantly associated with age at first childbearing in all three countries. With reference to age at first cohabitation, Appendix Table 2 reveals that young women who married in early adolescence (by 15 years) were more likely to face early motherhood (97.4%, 99.1% and 98.7% in Niger, Mali and Malawi, respectively), in comparison with 42.2%, 57.0% and 53.7% (in the same order) of those who married in emerging adulthood (18–24 years of age). This implies that the age at first marriage positively induced early motherhood differential behaviour. Also, the proportion of respondents who faced early motherhood was larger among women who experienced sexual intercourse by 16 (96.3%, 96.6% and 94% in Niger, Mali and Malawi, respectively), which decreased among those who experienced it at the age 18–24 (40.7%, 45.1% and 44.6%, in that order). It appears that the age of entry into motherhood largely changed with initiation of sexual activity.
Multivariate
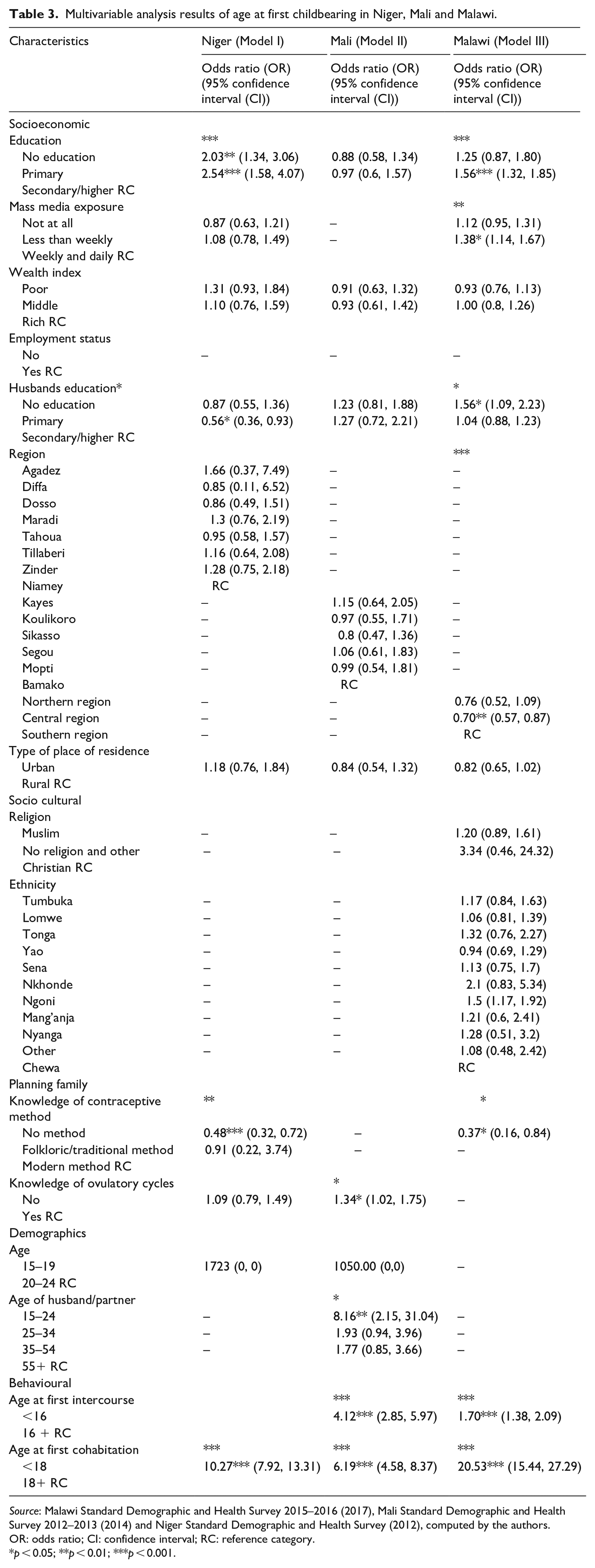
Negative log–log regression analyses were performed to determine the risk factors of early childbearing. In these models, age at first childbearing was used as a dependent variable. Moreover, age at first childbearing was dichotomised by assessing the value of 0 for age at first marriage being 20 years and above, and the value of 1 for age being below 20 years. Appendix Table 3 presents the results based on the negative log–log regression analyses for early childbearing. The results of the study have highlighted nine factors that significantly predict young women’s risk of early childbearing at 95% in at least one of the three countries, namely age at first marriage/cohabitation, age at first intercourse, women’s education, husband’s/partner’s education and age, mass media exposure, region of residence, knowledge of contraceptive methods and knowledge of ovulatory cycles. Findings show that age at first marriage/cohabitation was the strongest positive factor related to the postponement of childbearing in all three countries studied.
Young women who got married in their early and middle adolescence (by 18 years) were 20.53, 10.27 and 6.19 times (95% CI = [15.44, 27.29], 95% CI = [15.03, 27.02] and 95% CI = [4.58, 8.37] in Malawi, Niger and Mali, respectively) more prone to experience early motherhood than were those who got married at 18 and above. Furthermore, the risk of facing early childbearing decreased with age at first intercourse in Mali and Malawi. Participants who engaged in sexual activity by 16 years (OR = 4.12 in Mali) and (OR = 1.70 in Malawi), had a higher risk of early childbearing compared to those who initiated it at age 16 and above.
Indeed, women’s and husband’s/partner’s educational level significantly affected the likelihood of early childbearing in Niger and Malawi. Women with primary education in Niger and Malawi were 2.54 and 1.56 times (95% CI = [1.34, 3.06] and 95% CI = [1.32, 1.86], respectively) more likely to undergo early childbearing than their secondary and higher educated counterparts were. With regard to husbands’/partner’s education, findings reveal that young women whose husbands had a primary education in Niger (OR = 0.56) were less likely to challenge early motherhood than those whose husbands had a secondary and tertiary education. In turn, women whose husbands had no education in Malawi (OR = 1.56) were more likely to challenge early motherhood than those whose husbands had secondary and tertiary education were. Region of residence was also a determinant of variation for age at first birth in Malawi. Respondents from the Central region in Malawi were 30% (95% CI = [0.57, 0.87]) less likely to give birth by 20 years than those from the Southern region were. Researchers’ findings revealed the likelihood of confronting early childbearing increased with the knowledge of contraceptive methods. Participants who had no knowledge of contraceptive methods in Niger and Malawi were 52% and 63% (respectively) less likely to confront early childbearing than those who knew about contraceptive methods. Furthermore, results indicate that the probability of facing early childbearing decreased with the knowledge of ovulatory cycles in Mali. Young women who had no knowledge of ovulatory cycles (OR = 1.34; 95% CI = [1.02, 1.7]) were more at risk of early childbearing when compared to those who had knowledge of ovulatory cycles. Other predictors of age at first childbearing were women’s exposure to media and husband’s/partner’s age. Respondents in Malawi who were exposed to media less than weekly (OR = 1.38) had a greater risk of early childbearing than those who were exposed weekly and daily. Furthermore, respondents whose husbands were aged 15–24 were 8.16 times (95% CI = [2.15, 31.04]) more likely to undergo early motherhood than their counterparts whose husbands were aged 55 and above in Mali were.
Discussion
Key findings
Trend in early childbearing
One of the main aims of this study was to examine the trends of early childbearing among young women aged 15–24 in three sub-Saharan African countries using data from the DHS between 2006 and 2016. The findings show that early childbearing remains common in these countries, ranging from 80.4% in Malawi to 88.3% in Niger. However, recent trends show a significant decline in Malawi and Mali, while no significant change was observed in Niger. There was a significant reduction in the percentage of early marriage in Niger, Mali and Malawi from 2006 to 2016. However, significant increases in age at sexual debut, knowledge of ovulatory cycle and contraceptive methods were observed in Niger and Mali.
Factors associated with early childbearing
The aim of this study was to examine the socioeconomic and demographic determinants of early childbearing among young mothers in sub-Saharan African countries using data from the Malawi Standard Demographic and Health Survey 2015–2016 (2017), the Mali Standard Demographic and Health Survey 2012–2013 (2014) and the Niger Standard Demographic and Health Survey (2012).
Our findings reveal that the risk of early childbearing was strongly associated with age at first marriage/cohabitation in all three countries studied. Young women who confronted early marriage (by 18 years) were more at risk of early childbearing than those who married at the age 18 and above. This implies that the earlier the marriage, the higher the probability of facing early motherhood. Similarly, the likelihood of confronting early childbearing was associated strongly with age at first sexual intercourse. Participants who challenged early sexual activity (by 16 years) in Mali and Malawi were more at risk of early childbearing than were those who initiated it at the age 16 and above. This suggests that the sooner the sexual intercourse initiation, the higher the odds of early childbearing. Moreover, it was found that the risk of early childbearing decreased with women’s education educational level in two of the countries studied, namely Niger and Malawi. The findings indicate that women without formal education and those with primary education had a higher risk of early childbearing than their secondary or higher educated counterparts had. This implies that the lower the level of education, the higher the chance of confronting early childbearing. Our study uncovered that women’s knowledge of ovulatory cycles and contraceptive methods were determinants of early childbearing. Young women who had no knowledge of ovulatory cycles were more likely to go through early birth when compared to those who had knowledge of ovulatory cycles in Mali. Furthermore, the likelihood of facing early birth increased when women had knowledge of contraceptive methods in Niger and Malawi. Concerning women’s media exposure, the results underline that participants who had been exposed to media in Malawi less than weekly were more likely to confront early childbearing than those who had been exposed weekly and daily. Other factors associated with age at first childbearing in this study were region of residence, husband’s/partner’s education and age.
Study findings in relation to other studies
The findings of our research indicate that women’s reproductive health behaviour such as age at first marriage/cohabitation and age at first intercourse are critical factors associated with age at first childbearing and motherhood. The multivariate analysis reveals that, in all three countries studied, respondents who married in their early and middle adolescence were more at risk of early childbearing than those who married in their emerging adulthood (18–24 years) were. These results bring to light that early marriage leads to early pregnancy and childbearing; several previous studies suggest the same (Kassa et al., 2018; UNFPA, 2012; Yakubu and Salisu, 2018). A possible reason might be cultural. Indeed, in most sub-Saharan African countries, girls’ social value is firmly rooted in their capacity to reproduce (Hindin and Fatusi, 2009; Presler-Marshall and Jones, 2012; Rossier, 2007), and women’s main role is to provide children for their husband’s family (Rossier, 2007). Therefore, child marriage and rapid conception are encouraged. In this context, marriage and pregnancy are ‘socially accepted, found identity, are sources of status, and reaffirm entry into adulthood’ (Goicolea, 2009). There is an urgent need to change societal attitudes towards early marriage and motherhood.
Also, young mothers who challenged early sexual activity (by 16 years) in Mali and Malawi were more at risk of early childbearing in comparison with those who faced first sexual activity at the age of 16 and above. This corroborates the results from prior research and systematic reviews (Iyanda et al., 2020; Wado et al., 2019; Yakubu and Salisu, 2018). A possible explanation could be the fact that in many African societies, many adolescent girls initiate sexual activity with older partners, which might lead to many births among adolescent girls occurring outside of, or shortly after, marriage. Moreover, our study indicates that socioeconomic factors, namely woman’s education, mass media exposure and region of residence are important determinants of age at first childbearing. Findings show that in Niger and Malawi, young mothers with no education and primary education were more likely to undergo early childbearing compared to their counterparts with secondary or tertiary education. However, no significant influence of mothers’ educational level on the age at first childbearing was found in Mali. This suggests that higher education is protective against early motherhood. Several previous studies have revealed maternal education as a strong and negative predictor of early childbearing (Iyanda et al., 2020; Kassa et al., 2018; Wado et al., 2019; Yakubu and Salisu, 2018). This could potentially be because educated women are considered to have a greater awareness of the existence of family planning services and may benefit from using such services. Other scholars found that incorrect knowledge of ovulation and contraceptive methods were significant predictors of unintentional child and pregnancy among young women in sub-Saharan Africa (Iyanda et al., 2020). Our analyses show that the probability of facing early birth decreased when women had knowledge of ovulatory cycles in Mali only. This may result from the fact that many adolescents frequently do not discover how their bodies work, how pregnancy occurs and how to prevent pregnancy. In fact, mastering the cycle can help an adolescent to negotiate the most suitable time for her to have sex and to abstain during the ovulation period. This study also found an increased likelihood of confronting early childbearing with increased knowledge of contraceptive methods in Niger and Malawi. Various researchers have shown the effect of knowledge of contraceptive methods on fertility behaviour (Ayuba and Gani, 2012; Bankole and Malarcher, 2010; Malarcher, 2010; Wado et al., 2019). While most adolescents are aware of modern methods of family planning, they are often misinformed about how they work.
Limitations of the study
This study has some important limitations. Given the cross-sectional nature of our data, the direction of causal associations cannot always be ascertained. Moreover, nearly all information collected in DHS is subject to reporting and recall biases. Certain information such as initiation to sexuality, age at marriage and age at childbearing refers to events in the past. This inevitably causes biases. In spite of all these limitations, this study contributes to the wealth of knowledge on the determining factors of early childbearing in sub-Saharan Africa countries, more particularly Malawi Mali and Niger, by investigating the effects of several socioeconomic, demographic and behavioural characteristics.
Conclusion
This study has reinforced the state of knowledge of the factors determining early entry of the youth into motherhood in three sub-Saharan African countries, namely Niger, Mali, and Malawi. Results indicate that early childbearing remains common among young women in the three target countries, despite the fact that it is likely to decrease over time. Also, the highest likelihood of early childbearing was found among participants who married in early adolescence (by 15 years). Findings of this study show that age at first childbearing among sub-Saharan African young women was determined by a range of individual and behavioural characteristics. It was found that age at first marriage/cohabitation, age at first intercourse, women’s education, husband’s/partner’s education, mass media exposure, age of husband/partner, region of residence, knowledge of contraceptive methods and knowledge of ovulatory cycles were factors that significantly determined young women’s risk of early childbearing in at least one of the three target countries. In addition, this study brought to light the similarity and variability in risk and protective factors that affect early entry into motherhood in the countries studied. This emphasises the need for a context-specific understanding of the factors that influence reproductive behaviour of adolescents and young adult women.
Recommendations
This study yielded worthy results that add necessity to calls for empowering and protecting adolescent girls in sub-Saharan Africa countries. There is an urgent need to introduce programmes that promote delaying the age at first sexual debut and equip adolescent women with knowledge about responsible and safer sex and/or motherhood. Besides, government authorities (policymakers) have to promote prolonged enrolment in school for adolescents and enforce a law that criminalises child marriages.
Footnotes
Appendix
Multivariable analysis results of age at first childbearing in Niger, Mali and Malawi.
| Characteristics | Niger (Model I) | Mali (Model II) | Malawi (Model III) |
|---|---|---|---|
| Odds ratio (OR) |
Odds ratio (OR) (95% confidence interval (CI)) | Odds ratio (OR) |
|
| Socioeconomic | |||
| Education | *** | *** | |
| No education | 2.03** (1.34, 3.06) | 0.88 (0.58, 1.34) | 1.25 (0.87, 1.80) |
| Primary | 2.54*** (1.58, 4.07) | 0.97 (0.6, 1.57) | 1.56*** (1.32, 1.85) |
| Secondary/higher RC | |||
| Mass media exposure | ** | ||
| Not at all | 0.87 (0.63, 1.21) | – | 1.12 (0.95, 1.31) |
| Less than weekly | 1.08 (0.78, 1.49) | – | 1.38* (1.14, 1.67) |
| Weekly and daily RC | |||
| Wealth index | |||
| Poor | 1.31 (0.93, 1.84) | 0.91 (0.63, 1.32) | 0.93 (0.76, 1.13) |
| Middle | 1.10 (0.76, 1.59) | 0.93 (0.61, 1.42) | 1.00 (0.8, 1.26) |
| Rich RC | |||
| Employment status | |||
| No | – | – | – |
| Yes RC | |||
| Husbands education* | * | ||
| No education | 0.87 (0.55, 1.36) | 1.23 (0.81, 1.88) | 1.56* (1.09, 2.23) |
| Primary | 0.56* (0.36, 0.93) | 1.27 (0.72, 2.21) | 1.04 (0.88, 1.23) |
| Secondary/higher RC | |||
| Region | *** | ||
| Agadez | 1.66 (0.37, 7.49) | – | – |
| Diffa | 0.85 (0.11, 6.52) | – | – |
| Dosso | 0.86 (0.49, 1.51) | – | – |
| Maradi | 1.3 (0.76, 2.19) | – | – |
| Tahoua | 0.95 (0.58, 1.57) | – | – |
| Tillaberi | 1.16 (0.64, 2.08) | – | – |
| Zinder | 1.28 (0.75, 2.18) | – | – |
| Niamey | RC | ||
| Kayes | – | 1.15 (0.64, 2.05) | – |
| Koulikoro | – | 0.97 (0.55, 1.71) | – |
| Sikasso | – | 0.8 (0.47, 1.36) | – |
| Segou | – | 1.06 (0.61, 1.83) | – |
| Mopti | – | 0.99 (0.54, 1.81) | – |
| Bamako | RC | ||
| Northern region | – | – | 0.76 (0.52, 1.09) |
| Central region | – | – | 0.70** (0.57, 0.87) |
| Southern region | – | – | RC |
| Type of place of residence | |||
| Urban | 1.18 (0.76, 1.84) | 0.84 (0.54, 1.32) | 0.82 (0.65, 1.02) |
| Rural RC | |||
| Socio cultural | |||
| Religion | |||
| Muslim | – | – | 1.20 (0.89, 1.61) |
| No religion and other | – | – | 3.34 (0.46, 24.32) |
| Christian RC | |||
| Ethnicity | |||
| Tumbuka | – | – | 1.17 (0.84, 1.63) |
| Lomwe | – | – | 1.06 (0.81, 1.39) |
| Tonga | – | – | 1.32 (0.76, 2.27) |
| Yao | – | – | 0.94 (0.69, 1.29) |
| Sena | – | – | 1.13 (0.75, 1.7) |
| Nkhonde | – | – | 2.1 (0.83, 5.34) |
| Ngoni | – | – | 1.5 (1.17, 1.92) |
| Mang’anja | – | – | 1.21 (0.6, 2.41) |
| Nyanga | – | – | 1.28 (0.51, 3.2) |
| Other | – | – | 1.08 (0.48, 2.42) |
| Chewa | RC | ||
| Planning family | |||
| Knowledge of contraceptive method | ** | * | |
| No method | 0.48*** (0.32, 0.72) | – | 0.37* (0.16, 0.84) |
| Folkloric/traditional method | 0.91 (0.22, 3.74) | – | – |
| Modern method RC | |||
| Knowledge of ovulatory cycles | * | ||
| No | 1.09 (0.79, 1.49) | 1.34* (1.02, 1.75) | – |
| Yes RC | |||
| Demographics | |||
| Age | |||
| 15–19 | 1723 (0, 0) | 1050.00 (0,0) | – |
| 20–24 RC | |||
| Age of husband/partner | * | ||
| 15–24 | – | 8.16** (2.15, 31.04) | – |
| 25–34 | – | 1.93 (0.94, 3.96) | – |
| 35–54 | – | 1.77 (0.85, 3.66) | – |
| 55+ RC | |||
| Behavioural | |||
| Age at first intercourse | *** | *** | |
| <16 | 4.12*** (2.85, 5.97) | 1.70*** (1.38, 2.09) | |
| 16 + RC | |||
| Age at first cohabitation | *** | *** | *** |
| <18 | 10.27*** (7.92, 13.31) | 6.19*** (4.58, 8.37) | 20.53*** (15.44, 27.29) |
| 18+ RC | |||
Source: Malawi Standard Demographic and Health Survey 2015–2016 (2017), Mali Standard Demographic and Health Survey 2012–2013 (2014) and Niger Standard Demographic and Health Survey (2012), computed by the authors.
OR: odds ratio; CI: confidence interval; RC: reference category.
p < 0.05; **p < 0.01; ***p < 0.001.
Acknowledgements
The researchers would like to thank the USAID for the free Demographic and Health Survey Data Set on the Internet.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.