
Abstract
Cultural mistrust is a critical factor underlying the racial/ethnic disparity in mental health care service utilization. It was hypothesized that there would be a difference in utilization attitudes and intentions before and after exposure to a culturally responsive intervention among individuals with moderate to high levels of cultural mistrust. Two Hundred Thirty-Six students from a predominately Black university participated in this study. This experiment employed a Solomon Four Groups design to assess the effectiveness of a culturally responsive cognitive intervention to neutralize the effects of cultural mistrust on health care attitudes and health care service utilization intentions. The results showed that the intervention was effective in neutralizing cultural mistrust and improving posttest utilization attitudes and intentions among individuals who had high levels of cultural mistrust. It was also found that health care utilization attitudes and intentions were enhanced for individuals with high levels of cultural mistrust.
Keywords
According to the National Survey on Drug Use and Health by the Substance Abuse and Mental Health Services Administration [SAMHSA] (2015), 18.1% of adults in the United States are diagnosed with a mental illness. However, only 14.8% of adults receive mental health treatment. The majority of adults with mental health disorders in the United States do not receive ongoing mental health services (Wang et al., 2005), and the low rates of treatment for mental health disorders are evident throughout all age groups (Schnittker, 2003; U.S. Department of Health and Human Services [U.S. DHHS], 1999). Since the Surgeon General’s 2001 report, racial disparity in mental health service utilization has been well documented (Alegria et al., 2008; Chen, Vargas-Bustamante, Mortensen, & Ortega, 2016; Garland et al., 2005; U.S. DHHS, 2001), although the implementation of the Affordable Care Act (ACA) may lead to a reduction of this disparity (Chen et al., 2016). Nevertheless, the Summary Health Statistics 2012 report indicates that racial and ethnic minorities are still less likely to have seen a doctor or other health professional within the previous 6 months, compared with their White counterparts (Centers for Disease Control and Prevention, Substance Abuse and Mental Health Services Administration, National Association of County Behavioral Health & Developmental Disability Directors, National Institute of Mental Health, The Carter Center Mental Health Program, 2012). Research also indicates that racial and ethnic minorities have less access to mental health services, are less likely to receive needed care, and are more likely to receive poorer quality care (U.S. DHHS, 2001). Theory and research suggest that the confluence of those factors and cultural mistrust undergird the burden in mental health among minorities (Aday, 1994; McGuire & Miranda, 2008; U.S. DHHS, 1999, 2001). This issue of cultural mistrust is critical to understanding the challenges African Americans face in seeking mental health services. Cultural mistrust is a concept that has largely been relegated to problematic behavior because researchers presume that such attitudes and predispositions are inappropriate responses for Blacks to have, despite evidence suggesting that such responses are natural outcomes of the historical relations between Blacks and Whites. Appreciation of the cultural relativity of responses between Blacks and Whites would greatly facilitate the development of effective interventions for minority populations in the area of health care utilization. This study attempted to assess the effects of cultural mistrust and exposure to a culturally sensitive informational campaign from health care professionals on attitudes toward seeking professional help and intentions to seek health care among African American college students.
The President’s New Freedom Commission on Mental Health (2003) reported that disparities in the mental health system are largely a result of the system not adequately recognizing and responding to the culturally diverse needs of patients. In order to meet that challenge, intervention and prevention efforts must become more culturally sensitive and responsive to the perceptions, values, and needs of diverse populations. One such cultural difference is the notion of cultural mistrust, which grows out of the idea of “cultural paranoia” by Grier and Cobbs (1968). Cultural mistrust posits that Blacks developed mistrust of Whites as a result of their historical and contemporary experiences (Terrell & Terrell, 1981; Whaley, 2001). The construct has been studied in a cross-section of service delivery areas. Individuals with high levels of cultural mistrust tend to report more negative experiences and more negative expectations of satisfactory service, particularly services provided by White healthcare service providers and counselors (Grant-Thompson & Atkinson, 1997; Nickerson, Helms, & Terrell, 1994; Watkins, Terrell, Miller, & Terrell, 1989; Whaley, 1998a, 2001). Studies also show that cultural mistrust influences health care attitudes, perceptions, beliefs, and intentions (Bruwer et al., 2011; Terrell & Terrell, 1981; Thompson, Bazile, & Akbar, 2004; Whaley, 1998a, 1998b, 2001), which, in turn, influences health care service utilization. Hence, this study was designed to explore the effects of a relatively brief, culturally sensitive informational campaign (persuasive communication) designed to neutralize the negative effects of cultural mistrust on the health-seeking attitudes and intentions with a sample of Black college students.
Cultural Mistrust, Service Utilization, and Intervention Programs
The historical evidence for cultural mistrust (Ashby, 1986; Baldwin, 1980; Bronstein, 1986; Terrell & Terrell, 1981; Whaley, 1998) suggest that Blacks in America, and throughout the world, have a valid reason to mistrust systems and constructs controlled and defined by White people, including the criminal justice system (Alexander, 2010; Johnson, 2008; Ramirez, 2014; Sauchelli & Rosenberg, 2015), the education system (Cohen, Steele, & Ross, 1999; Kozol, 1991; Okonofua & Eberhardt, 2015; Slavin, 1999), and the health care system (Arbisi, Rusch, Polusny, Thuras, & Erbes, 2013; Austin, Carter, & Vaux, 1990; Thompson, Bazile, & Akbar, 2004; Snowden, 1999; Whaley, 1998b, 2001). In the area of client-therapist relations, Nickerson et al. (1994) found a relationship between cultural mistrust and attitudes toward counseling for Blacks, especially when the counselor is White. In addition, studies show that Blacks with high levels of cultural mistrust also hold more negative views and expectations of White counselors and have more negative health-seeking attitudes (Grant-Thompson & Atkinson, 1997; Thompson, Worthington, & Atkinson, 1994; Watkins & Terrell, 1988; Watkins et al., 1989). The mistrust and cynicism among Blacks is largely explained by the history of race-based medical experimentations in America (Washington, 2006). Smedley, Stith, and Nelson (2003) posited that Blacks mistrust the U.S. health care system because of the health disparities experienced by people of color across various care settings. In addition, research on racial concordance between patients and providers further illustrate the significance of cultural mistrust (LaVeist & Nuru-Jeter, 2002; Thom, 2000). The mistrust of White people, White controlled institutions, and White counselors influence the help-seeking behaviors and attitudes of Blacks in most social domains. Consequently, the underutilization of mental health services and satisfaction with those services may be directly related to cultural mistrust (Austin et al., 1990; Townes, Chavez-Korell, & Cunningham, 2009; Watkins & Terrell, 1988).
Most intervention programs attempt to change behavior by either directly or indirectly altering perceptions and/or expectations of the health care system and its providers, which amounts in part to a neutralization of cultural mistrust. A few of those intervention programs may be interpreted as direct attempts to moderate or examine the effect of cultural mistrust (Gil, Wagner, & Tubman, 2004; Ng, Tsun, Su, & Young, 2013), while others obtained similar outcomes indirectly by employing cultural factors that neutralized cultural mistrust (Briggs, Banks, & Briggs, 2014; James & Moore, 1997; Ravitz et al., 2014). For example, in the Alcohol Treatment Targeting Adolescents in Need (ATTAIN) program with Hispanic and Black adolescents, Gil et al. (2004) found cultural and racial pride to be negatively associated with alcohol and other drugs (AOD) use after intervention, particularly for alcohol use among Blacks. They also found a negative relationship between cultural identity/ethnic pride and indiscriminant ethnic mistrust.
A persistent call among researchers is that effective treatment and intervention must become more responsive to the social barriers and cultural context of ethnic minorities and underserved populations (Griner & Smith, 2006; James & Moore, 1997; Ravitz et al., 2014). Two recent community intervention studies incorporating various social and cultural practices have demonstrated effective results (Briggs et al., 2014; Brody, Chen, Kogan, Yu, Molgaard, DiClemente, & Wingood, 2012). In those studies, knowledge and education about the mental health system provided by trusted experts increased utilization of mental health services by Blacks. Despite these findings, many intervention studies are plagued with limitations of cost, time, audience size, and reach. A major limiting factor is that many interventions are just too costly to test, both in terms of time and money. Some interventions require weeks, months, and even years before their effectiveness can be evaluated. The scope and reach of those interventions are generally limited to direct contact between the professionals and participants and as a result interventions are only able to reach a limited number of participants. Despite those limitations, the critical factor underlying the effectiveness of many intervention programs for minority populations may be that they increase the level of trust participants have for both the health care system and health care providers. Consistent with research on social cognition, many intervention programs are likely effective because they alter perceptions of the social environment or the information individuals use to evaluate the social world and the behavior of others in that world (e.g., health care providers). Intervention programs are largely effective because they build on the findings of cognitive and social neuroscience, memory, and social cognition (Amodio, 2008; Fiske, 2013; Gazzaniga, Ivry, & Mangun, 2009; Petty & Brinol, 2010) that reveal how individuals use recently acquired information to evaluate others and new contexts. The present study was a fundamental test of the ability of culturally responsive health care professionals to alter perceptions of trust, attitudes, and behavioral intentions. In other words, this study was designed to assess the effectiveness of a brief, culturally sensitive, cognitive, informational intervention to neutralize the effects of a primarily cognitive variable, cultural mistrust, on health-seeking attitudes and intentions. It was hypothesized that the intervention would produce differences in utilization attitudes and intentions before and after the intervention, as well as between those who received the intervention and those who did not, particularly among individuals with moderate to high levels of cultural mistrust. Those who received the intervention would show more favorable attitudes toward seeking health care and intentions to use it.
Method
Participants
Two hundred thirty-six students participated in the experiment. All of the participants were students at a Historically Black College or University (HBCU) in the Mid-Atlantic region of the United States of America. Fifty-one percent of the participants were freshman students, 17% were sophomores, 15% were juniors, 17% were seniors, and less than 1% were graduate students. Participants ranged in ages between 17 and 60 years, and 62% were female.
Materials
The Cultural Mistrust Inventory (CMI) developed by Terrell and Terrell (1981) was used to assess cultural mistrust. This is a 48-item measure used to measure Black peoples’ mistrust and suspiciousness of White people in four areas (law and politics, interpersonal relations, education and training, and business and work). This inventory has a test-retest reliability of .82, and an internal consistency of .89. For the current study, internal consistency was .88.
The Attitudes Toward Seeking Professional Psychological Help, Shortened Form (ATSPPH-S) developed by Fischer and Farina (1995) is a 10-item scale used to measure attitudes toward seeking professional psychological help. This scale has a test-retest reliability of .89 and an internal consistency of .86. This shortened form of the Attitudes Toward Seeking Professional Psychological Help has no subscales, unlike the original form. Consistent with the recommendations of the scale authors (Fischer & Farina, 1995) researchers are advised to use the total scale as a unidimensional instrument to assess help seeking orientation. The test-retest reliability for this instrument in this project was .83.
For this experiment, the term intention has been operationally defined as the participant’s plan to seek psychological services, physical health services, or visit a community-based clinic within the next 6 months, year, and 3 years. To assess intentions, participants were asked nine questions that focused on their plans to seek various types of services.
Participants were also given a demographics form and background questionnaires developed by the authors. The purpose of these forms were to obtain background information about the participants’ (a) past health care utilization practices, (b) past access to services on and off campus, and (c) future plans and intentions with regard to their health care service utilization practices.
Intervention Tasks
The Culturally Responsive Cognitive Intervention (treatment or experimental condition) consisted of two informational video presentations. The video presentations were used to provide background information and illustrate culturally responsive health care practices provided by primarily Black health care providers (doctors and nurses). One video exposed the participants to a medical facility that was primarily staffed by Black doctors describing their commitment and service philosophy to the community and clients they serve (primarily Black clients). The second video served to add authenticity to the intervention by connecting the medical facility/doctors video to an actual law that the students already knew about, the ACA. The informational video led students to believe that this study was designed to test the effect of the future community health care centers that would be a result of the implementation of the ACA. Students were led to believe that these centers were to be staffed by doctors and professionals from the community that they serve. Illustrating Black experts and clients in the video should have captured the attention of Black students and affected their perceptions of the race and dispositions of the doctors and staff likely to serve them in the future. The information in the medical facility video was designed to serve as a prime to activate conscious and unconscious cultural affinities and perceptions of trust between participants and hypothetical future health care providers, which should manifest differently for individuals governed by different levels of cultural mistrust (Gardner, Gabriel, & Lee, 1999).
The videos had two different formats. The experimenter narrated the first video and the second video consisted of a professionally developed presentation by health care providers from a well-known medical facility. The experimenter-narrated video outlined two critical factors: (a) the purpose of the experiment (described above) and (b) the connection between the experiment and the ACA (1 minute). After being introduced to the experiment, through the first video, participants were provided the medical facility video that outlined the philosophy, attitudes, and practices of medical professionals with regard to their desire and commitment to serve their community. The 4-minute, YouTube video featured multiple doctors (both male and female). Permission to use the video was provided by the medical facility (Morehouse School of Medicine). In the design of this study (described below), approximately half of the participants were randomly assigned to view the videos.
Design
This experiment consisted of two major phases. In one phase, participants completed a demographics/background questionnaire (BGQ) and the CMI. Half of the participants completed the BGQ and the CMI in the beginning of the experiment (before completing help-seeking attitudes and intention measures) and half completed those instruments at the end of the experimental phase but before completing the attitudes and intention measures. The second phase was the experimental phase, wherein the Solomon Four-Group Design (Dukes, Ullman, & Stein, 1995; Solomon, 1949) was used to maintain the rigors of experimental control and allow for multiple levels of comparisons to determine the effectiveness of the intervention. Participants were randomly assigned to one of four experimental conditions: Condition 1 (pretest, treatment [videos], posttest), Condition 2 (pretest, no video [brief downtime], posttest), Condition 3 (no pretest, treatment [videos], posttest); and Condition 4 (no pretest, no video, posttest-only). The pretest condition consisted of help-seeking attitudes and health care utilization intentions (half of whom completed the BGQ and CMI during the pretest and half completed them during the posttest). In this experiment, there was not a neutral task for the participants in Condition 2 who were not shown a video. There was only a brief downtime between completing the pretest and posttest measures. However, the pretest and posttest conditions were slightly different relative to the number of measures completed.
Procedure
Participants were recruited from various classes. They were given a link in their classes that directed them to a Qualtrics survey online. In the survey, the students completed an informed consent form. Half of the participants completed the BGQ and CMI before they were randomly assigned to one of the four experimental and control conditions described above, and half of the students completed the BGQ and CMI after they were randomly assigned and completed one of the experimental/control conditions. In the consent document, all participants were told that this study would be one that is investigating a pilot program, under the ACA, that could revolutionize health care delivery to urban communities.
An illustration of the procedures in this design is as follows: half of the participants in Condition 1 completed the BGQ and the CMI before they completed the pretest attitude and intention measures. After completing the pretest measures, they watched the videos, and then completed the posttest attitudes and intention measures only. Some participants in Condition 1 completed all measures in the pretest condition, watched the videos, and then completed the posttest attitude and intention measures, followed by completing the CMI and the BGQ. The unique aspect of this experiment was that everything was done online, so that individuals did not have any other human influence, other than the persons they saw on the videos. The software was able to precisely assign the students in the randomized conditions. After participating in the experiment, the students were electronically debriefed and thanked for their participation.
Results
To test the major hypotheses of this study, data were divided into two cultural mistrust groups: a pure high level and a pure low level.
The hypothesized difference in utilization attitudes before and after exposure to culturally responsive health care intervention was supported, Condition 1. To test this hypothesis, a paired samples t test was used to compare the participants’ attitudes toward seeking professional psychological help (ATSPPH) responses before and after the intervention. As expected, the analysis revealed that students who received the intervention had significantly higher posttest ATSPPH-S (M = 24.66; SD = 13.63) than pretest ATSPPH-S (M = 20.78; SD = 8.52), t(40) = 3.56 p = .001, Conditions 3 and 4. There was not a significant difference between the pretest attitudes across groups, nor was there a significant difference in the pretest and posttest attitudes in Condition 2 (the condition that did not receive the treatment). The postintervention attitude scores did not differ between the participants in Conditions 1 and 3 (those who received the intervention), nor did the post intervention attitude scores differ between the participants in Conditions 2 and 4 (those who did not receive the intervention). These findings indicate that the intervention produced differences in utilization attitudes and intentions.
A significant main effect was found for treatment on utilization attitudes, F(1, 99) = 15.76, p = .000, and intentions F(1, 118) = 23.26, p = .000, and an interaction effect for treatment by cultural mistrust, F(1, 99) = 4.28, p = .041, eta squared .041. Those who received the treatment had a higher posttest utilization attitude mean (M = 22.54, SD = 10.97) than those who did not receive treatment (M = 15.86, SD = 5.07). While participants who were low in cultural mistrust and received the treatment had higher posttest attitudes means (M = 20.00, SD = 8.35) than those who did not receive the treatment (M = 16.97, SD = 5.55); participants who were high in cultural mistrust and received the intervention had higher posttest attitudes (M = 24.69, SD = 12.72) and lower pretest attitudes (M = 15.07, SD = 4.60) than those with low cultural mistrust, suggesting that the treatment had a more powerful effect on those with high cultural mistrust. This interaction is illustrated in Figure 1 and Table 1.
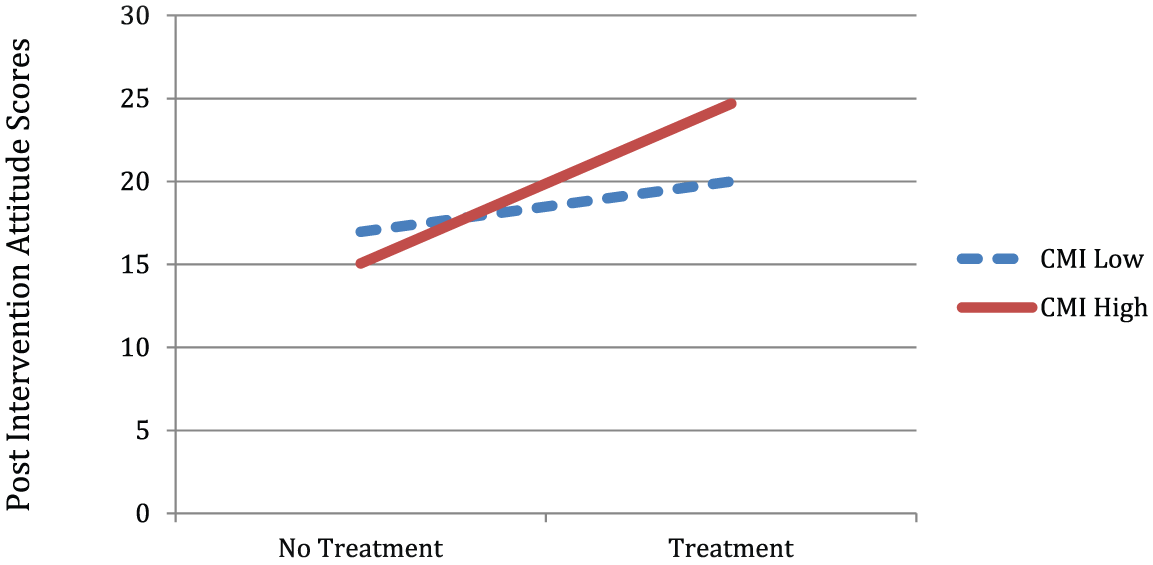
The treatment interaction between postintervention attitudes toward seeking professional psychological help and pure cultural mistrust.
Posttest Utilization Attitudes by Level of Cultural Mistrust and Treatment.
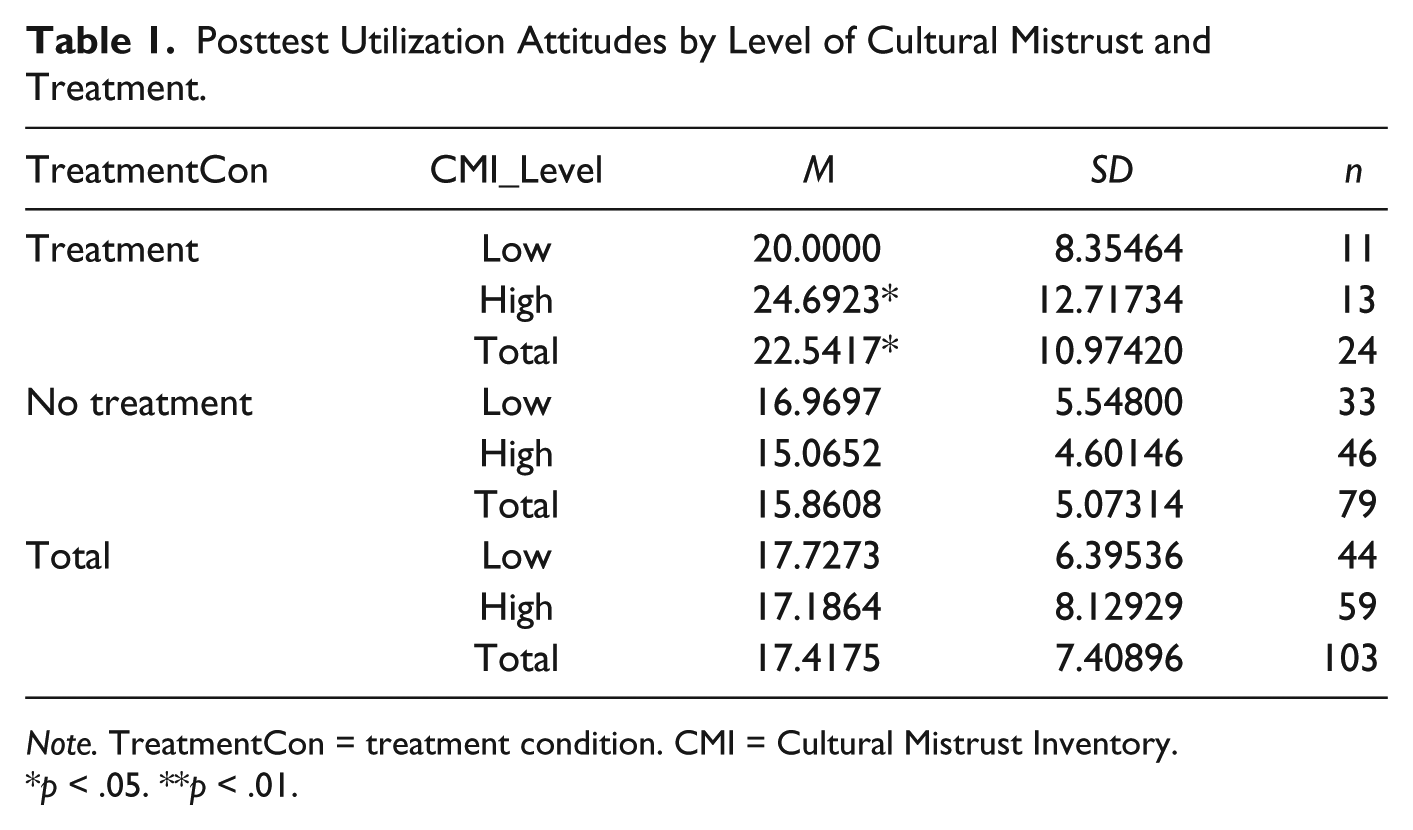
Note. TreatmentCon = treatment condition. CMI = Cultural Mistrust Inventory.
p < .05. **p < .01.
To further evaluate the second major hypothesis, that there would be a difference in utilization attitudes and intentions between individuals who did not receive the culturally responsive health care information and those who do receive the information among individuals with moderate to high levels of cultural mistrust, four independent-group factorial ANOVAs were conducted to evaluate the Cultural Mistrust × Treatment effects on posttest intentions in four areas of health care services utilization: (a) mental health, (b) medical, (c) community service facilities, and (d) overall utilization. The results revealed a main effect for each of the posttest intentions to utilize health care services over the next 3 years. Individuals who received the treatment intervention had (a) higher overall intentions (M = 41.71, SD = 32.62) versus (M = 24.38, SD = 6.51), F(1, 118) = 23.26, p = .000; (b) higher mental health intentions (M = 9.83, SD = 8.28) versus (M = 5.29, SD = 2.54), F(1, 118) = 21.06, p = .000); (c) higher medical intentions, (M = 12.71, SD = 10.74) versus (M = 7.63, SD = 2.93), F(1, 118) = 16.20, p = .000; and (d) higher community service facilities utilization intentions (M = 11.95, SD = 9.17) versus (M = 6.68, SD = 2.95), F(1, 118) = 22.50, p = .000. For more detail, please see Tables 1 and 2.
Posttest Utilization Intentions for All Health Care Services by Level of Cultural Mistrust and Treatment.
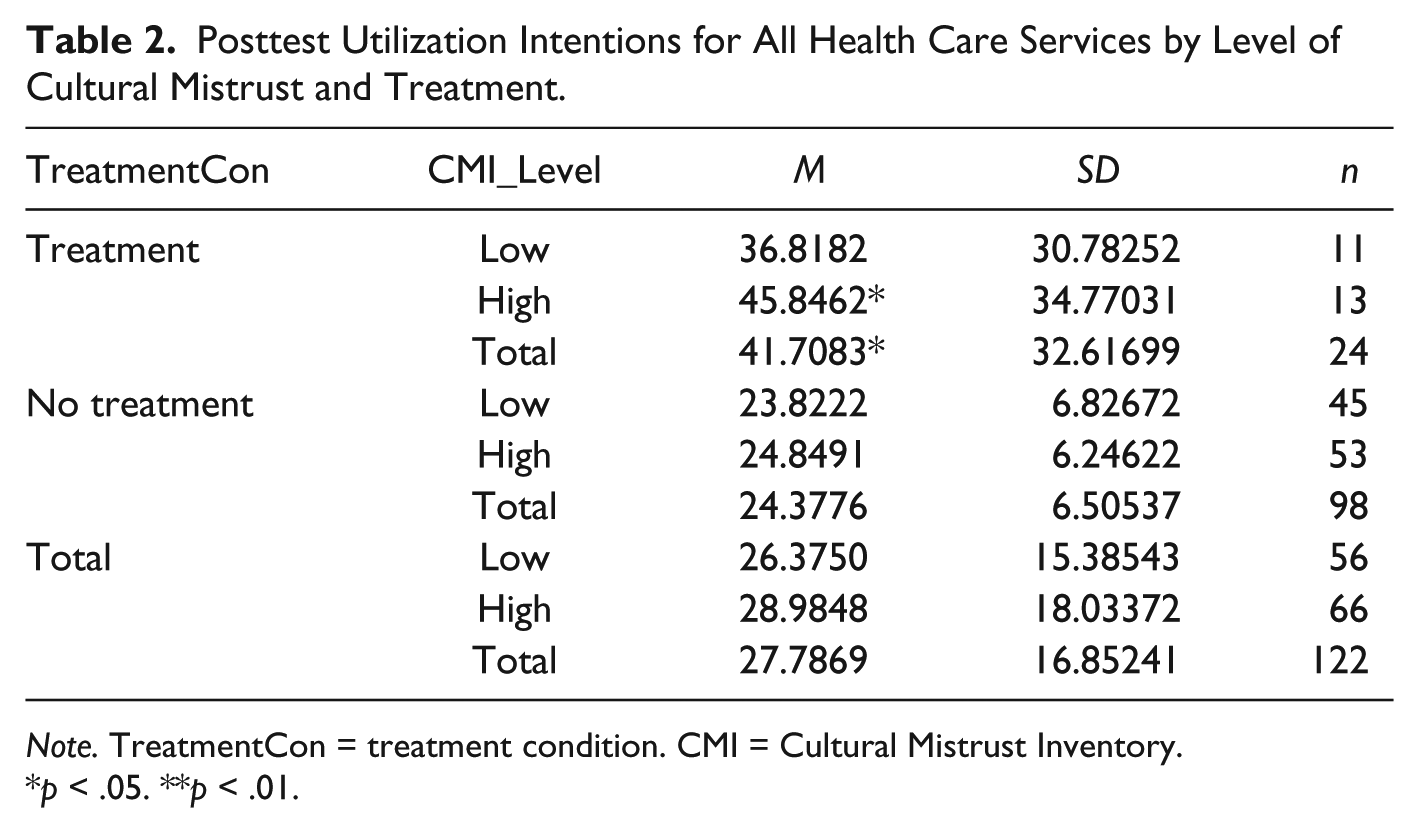
Note. TreatmentCon = treatment condition. CMI = Cultural Mistrust Inventory.
p < .05. **p < .01.
Discussion
The purpose of the current experiment was to examine the influence of cultural mistrust and exposure to a culturally responsive health care campaign on college students’ attitudes and intentions to seek mental health and physical health services. This experiment differs from previous work in this area by exploring the effects of a brief, informational intervention campaign designed to influence help-seeking attitudes and intentions of a sample of African American college students. At least two major conclusions can be drawn from this experiment: (a) Mental and physical health care utilization attitudes can be influenced by culturally responsive cognitive interventions, and (b) health care utilization attitudes and intentions of individuals high in cultural mistrust may be particularly enhanced by culturally responsive interventions.
Cultural Mistrust and Utilization
The goal of the experiment was to identify a way of neutralizing the negative effects of a common cultural predisposition and belief among Blacks that has been associated with their health care attitudes and utilization practices. The findings of the experiment revealed that mental health and medical health service utilization attitudes and intentions are influenced by cultural interventions designed toward building trust for the health care system and health care providers. Although prior research reveal the negative effects of cultural mistrust on help-seeking attitudes and intentions (Grant-Thompson & Atkinson, 1997; Thompson et al., 1994; Watkins & Terrell, 1988; Watkins et al., 1989), the implications of the differential effects of cultural mistrust on those attitudes and intentions in this experiment suggest that cultural mistrust is a missing link that should be factored into any intervention designed to improve attitudes and increase utilization practices among Blacks.
While prior research suggests that the neutralization of cultural mistrust is possible, those studies, however, were not specifically designed to neutralize cultural mistrust. For example, the findings of Briggs et al.’s (2014) culturally responsive intervention on improving mental health service utilization can be interpreted as a neutralization of cultural mistrust in Portland Oregon. Their research appeared to look at cultural mistrust as “a factor” as opposed to “a critical factor” that contributes to underutilization. Even though they were able to increase utilization through psychoeducation interventions, when interpreted in light of the theoretical underpinnings of the current study, their findings essentially had the effect of neutralizing cultural mistrust, albeit after months of psychoeducation intervention. After months interacting with professionals from their community, their intervention amounted to increased understanding and trust. Through months of interacting with Black professionals and experts as well as learning about health and the mental health system, participants were actually engaging in the same sort of culturally responsive intervention that was displayed in the intervention employed in the current experiment. The current experiment, as well as the research from Briggs et al. (2014) and others (Griner & Smith, 2006), indicates that increased diversity and cultural responsiveness in health care facilities and community settings may aid in the neutralization of cultural mistrust and increase help-seeking practices among Black populations.
Research on institutionalized racism in medicine, law, and education (Alexander, 2010; Perry, Steele, & Hilliard, 2004; Washington, 2006) illuminates its deleterious effects as well as the importance of trust in eliminating those effects (Steele, 2003). Without perceptions of increased equity in health care services and/or the experience of a culturally responsive health care intervention designed to foster trust in the health care system, disparities in health and health care utilization will largely persist. Without changed perceptions, many Blacks may continue to perpetuate the behavioral pattern that has led to the current disparities.
Cultural mistrust is about how one person’s acquired knowledge, perceptions, and/or interactions with Whites or with a system controlled by Whites influences their opinion, attitudes, and intentions with regard to the utilization of that system (Grefe, 2011). The apprehensions that some Blacks may experience when interacting with systems that are controlled by Whites are a result of centuries of institutionalized inequities, which may arguably undergird the development of cultural mistrust. The fears and suspicions of older generations about race relations are manifested in their mistrust of Whites and White-controlled institutions and practices, whether it is in a police encounter, a problem with the education system, or in the health care system. This study suggest that the encrustation of cultural mistrust that has taken centuries to harden may begin to be made pliable in less than 10 minutes (or a series of 60-second commercials) if the perceptions that sustain them are perceived to have changed. This is not to say that cultural mistrust can necessarily be eliminated (or even that it should be), but the findings of this study suggest that the process of building trust can begin by changing perceptions and expectations. That is, with sustained culturally responsive intervention by culturally responsive practitioners, cultural mistrust may be reduced long enough for individuals to give a system that they did not trust a chance.
The factor that must be developed in the process of neutralizing culture mistrust appears to be “trust.” What does it take to increase trust? Researchers have shown us that trust in a therapist or physician is not solely based on ethnicity, but, perhaps, equally as important is the physician’s behavior (Bonner, Ferrans, Moore-Burke, & Gorelick, 2005). Patients want to know that their doctor has their best interest in mind, and being able to communicate that to patients is, perhaps, the most critical factor. Having the ability to communicate the message to the patient that “you are cared for,” the doctor cares about you, the doctor wants you to get the best care possible, or we have your best interest in mind is a powerful tool that can quickly neutralize cultural mistrust, increase utilization, improve health, and reduce health disparities. The level of mistrust may have largely dictated responses to the intervention. The video was used to transmit the message to participants that their medical provider is someone who looks like them and is someone who cares about them and their community, which should have engendered feelings trust and allayed many fears and suspicions Blacks have of medical doctors. The feelings of trust or perceived future attitudes and practices of health care providers should elicit responses governed by the level of cultural mistrust of individuals exposed to the intervention. Even though this study suggests that it is possible to improve health-seeking attitudes and intentions, given that the overwhelming majority of medical doctors (like mental health providers) are White, one concern (discussed below) is what would be the effect of having White doctors communicate the same caring attitudes and practices? Nevertheless, this and other studies also suggest that culturally responsiveness must be incorporated in interventions to be effective.
Limitations of the Study
A failure to inquire about utilization practices prior to exposure to the treatment intervention was a limitation of this study. Ascertaining that information would have provided a more complete picture of the differences between intentions and attitudes that can be attributed to the intervention. It would have been useful to inquire about the students’ perceptions and opinions about the intervention (e.g., what were their likes and dislikes?). Another limitation was the downtime between the break in condition 2. The downtime may not have been long enough or a neutral video (or longer downtime) should have been used. Only the passage of time was employed in the control conditions of this study. The control conditions could have been filled with a neutral video, rather than filled with the free time and thoughts of participants. The free time could have allowed participants spend more time thinking about the measures completed and further strengthening their perceptions and attitudes. Although CMI was not designed to assess cultural mistrust in the health care domain, perhaps a measure of the mistrust of health care systems or professionals would provide insight into the nature of the trust that is being affected in interventions with minority populations (Benkert, Peters, Clark, & Keves-Foster, 2006).
Future Implications
More research exploring the long-term effects on attitudes, intentions, and actual utilization patterns would be beneficial for health care providers, policy makers, and citizens. If there is an actual increase in service utilization, we may begin to see a reduction in health care services costs, improved health, and a reduction in health disparities. This type of intervention should be tested with other ethnic groups that also experience cultural mistrust. One variation of this study could be to see if Blacks would have a similar response if this intervention were presented with White doctors expressing the same intent and desire to be responsive to the needs of the Black population. It is possible the opposite effects of the intervention may occur if all White doctors were featured in the video. In other words, less mistrustful individuals would likely be more encouraged and trusting of the information and, thereby, show more attitude change and intentions to seek health care than highly mistrustful individuals.
This intervention can inform outreach programs and campaigns for schools, law enforcement, mental health centers, and hospitals. Businesses, government agencies, advertisers, and so on, can use this research to serve as the foundation for employee and customer-service training to help increase customer satisfaction and compliance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.