
Abstract
Minimally invasive caries-removal procedures remove only caries-infected dentin and preserve caries-affected dentin that becomes remineralized. Dental cements containing calcium phosphate promote remineralization. This study evaluated the in vivo remineralization capacity of resin-based calcium-phosphate cement (Ca-P) used for indirect pulp-capping. Carious and sound teeth indicated for extraction were randomly restored with the Ca-P base or without base (control), followed by adhesive restoration. Study teeth were extracted after three months, followed by elemental analysis of the cavity floor. Mineral content of affected or sound dentin at the cavity floor was quantified by electron probe micro-analysis to 100-μm depth. After three months, caries-affected dentin underneath the Ca-P base showed significantly increased calcium and phosphorus content to a depth of 30 μm. Mineral content of treated caries-affected dentin was in the range of healthy dentin, revealing the capacity of Ca-P base to promote remineralization of caries-affected dentin.
Introduction
Minimally invasive treatment concepts use adhesive materials to stabilize lesions by halting the bacterial caries process and providing caries-affected tissue an opportunity to heal (Peters and McLean, 2001a,b). Contemporary tissue-saving treatments, such as ultraconservative caries removal (Mertz-Fairhurst et al., 1998; Ribeiro et al., 1999; Maltz et al., 2002), atraumatic restorative techniques (Frencken et al., 1994), and indirect pulp-capping procedures (Bjørndal et al., 1997; Bjørndal and Larsen, 2000), assume that caries can be halted and affected tissue can be remineralized. Healing of remaining affected dentin may be encouraged by the use of bioactive, ion-releasing base materials, e.g., glass-ionomer or Ca-P cements (Mukai et al., 1998; Dickens et al., 2003, 2004; Exterkate et al., 2005). Recent in vitro studies in an artificial caries model showed that calcium phosphate from a resin-based calcium-phosphate cement (RCPC) was able to remineralize diseased tooth tissue, showing the potential of promoting dentin repair (Dickens et al., 2003, 2004; Dickens and Flaim, 2008). During remineralization experiments, hydroxyapatite and/or other calcium phosphates precipitated in the lesions, resulting in significantly increased mineral content (Dickens et al., 2003; Dickens and Flaim, 2008). These in vitro experiments suggest that where complete removal of carious tissue is contra-indicated, these cements may induce remineralization of mineral-deficient dentin. The mineral phase in RCPC is based on the resin-free calcium-phosphate cement, developed as a bone-regenerating material (Chow et al., 2000). The incorporation of calcium phosphates into dual-curing resins enhanced clinical handling and performance, yielding command cure and increased strength and dentin adhesion (Dickens et al., 2004).
This proof-of-principle study investigated the potential clinical benefit of RCPC. Following standardized caries removal procedures, the bioactivity of RCPC-base material on caries-affected and sound dentin was evaluated in adhesively restored teeth after 3 mos of in vivo service. We tested the hypothesis that placement of RCPC on caries-affected dentin would increase calcium and phosphorus content of mineral-depleted dentin over time. In vitro elemental analysis of the cavity floor by electron probe micro-analysis (EPMA) techniques complemented evaluation of clinical hardness at re-entry.
MATERIALS & METHODS
A prospective randomized controlled clinical trial investigated clinical efficacy of RCPC in permanent human teeth. The study protocol was approved by governing Institutional Review Boards (UM #H03-00001883, FOBUSP #126/2003, and CONEP-Brasil #9846). The clinical phase (August- December, 2005) included 44 adult patients of the Bauru School of Dentistry, who signed informed consent, presenting 87 periodontally involved carious and healthy teeth, indicated for extraction. Teeth were prepared and randomly restored with/ without RCPC-base. Prior to application of RCPC-base, the cavity floor was etched or left unetched (Fig. 1), followed by an adhesive composite resin restoration according to common clinical protocol (etch-bond-restore). Randomization according to random number table was concealed in numbered envelopes. Patients were blinded to treatment delivered, while clinicians were not. Clinical, physical, radiographic, and microbial characteristics of cavity walls were evaluated at baseline and 3 mos later at re-entry after extraction. All patients presented after 3 mos for extraction. Extracted teeth were prepared for extensive in vitro physical and microbiological testing of dentinal walls. This report focuses on the mineral content of caries-affected, demineralized dentin at the cavity floor of 27 randomly selected carious and sound teeth.
Standardization of Caries-affected Dentin
After the cavity was opened and circumferential caries removed, leaving a clean hard dentino-enamel junction, central carious dentin was removed with a polymer bur (SmartPrep-System®, SSWhite Burs, Inc., Lakewood, NJ, USA). This self-limiting instrument produced a standardized affected dentin surface of about 25 KHN Knoop hardness (Peters, unpublished observations). Cavity walls in sound teeth were instrumented with the polymer bur according to the same protocol. After standardized caries removal, hardness of the cavity floor was clinically assessed by means of an explorer (Kidd et al., 1993).
Clinical Treatment Protocol
Teeth were divided into 2 main groups: C = carious (N = 14) and S = sound (N = 13) (Fig. 1). Seven non-restored teeth, serving as control [caries-affected CN (N = 4) and sound SN (N = 3)], were extracted immediately after cavity preparation and standardized caries removal. Components of RCPC, a two-paste system, and their function are shown in Table 1. Prior to the application of RCPC-base, both C and S teeth (N = 10) were randomized into 2 equal subgroups (N = 5): CE, SE with pre-treatment of dentin (Total Etch®, Ivoclar Vivadent AG, Schaan, Liechtenstein) and CU, SU without pre-treatment. Application and light-curing of RCPC were followed by the application of a thin film of vaseline to facilitate restoration removal at re-entry. Subsequently, remaining cavity walls were etched and bonded (Excite®, Ivoclar Vivadent AG, Schaan, Liechtenstein), and a microfilled composite resin (Epic®-TMPT Restorative, Parkell Inc., Edgewood, NY, USA) restoration was placed. Restoration margins were re-etched and re-bonded (same agents) to achieve optimal seal.
Specimen Preparation
Three mos later, restored teeth were extracted and restorations removed, followed by careful partial removal of base material, exposing half of the cavity floor. Dentin at the cavity floor was clinically assessed for its hardness. All 27 teeth were fixed, embedded, and longitudinally sectioned through the cavity (~ 3 sections/tooth, 200 μm thick) in preparation for elemental analysis. Two teeth (1 per subgroup, CU and SU) provided only 1 section and were excluded from further analysis.
Quantitative Elemental Analysis (EPMA-WDS)
Using electron probe micro-analysis (EPMA) based on wavelengthdispersive spectroscopy (WDS), we determined elemental composition of the cavity floor (Ngo et al., 1997). Quantitative elemental analysis was carried out by EPMA spot analysis (Cameca SX-100 Microprobe Analyzer, Cameca Science & Metrology Solutions, Gennevilliers, France) to measure weight-% of calcium (Ca) and phosphorus (P) in each pre-determined point. Ca and P levels in each tooth section (N = 75) were measured along 3 lines, starting at the cavity floor toward the pulp (0–100 μm depth, 11 datapoints, 10 μm apart). As internal control, a fourth line was measured distant from the lesion in sound dentin. In total, 2409 datapoints were obtained, 1287 in caries-affected and 1122 in sound dentin, respectively.
Statistical Analysis
Data were analyzed by ‘random coefficient models’, accounting for the inherent variability of dentin (inter- and intra-tooth biologic variation, lesion depth). We used a linear mixed model to fit the amount of both calcium and phosphorus at each depth for each section within a tooth. The slope was measured (i.e., change in phosphorus or calcium content with depth). A sample size of 12 sections for CN and 36 sections for SE_SU_SN allowed for detection of a 0.006 slope difference with 90% power, at an alpha level of 0.05 (Diggle et al., 2002). This assumes that residual variance around the regression line is 0.616 (based on actual results for phosphorus), and 10 measurements were made for each section (at depths of 0, 10, 20, . . ., and 100 μm). Correlation between values was very high for calcium, resulting in even more power for calcium.
Effects of treatment on EPMA data (means) were estimated separately for sound and carious teeth by Random Coefficient Models (Verbeke and Molenberghs, 2000). Models included fixed effects of treatment, depth, and treatment-by-depth interactions. Effect of depth was modeled by both a linear and a quadratic trend to allow for a curved relationship as depth increased. Linear and quadratic effects of depth were allowed to differ by treatment. The model for EPMA data included random intercepts and slopes for each tooth, allowing characteristic Ca-and P-levels and fitted curves to vary randomly between teeth. Although this proof-of-principle study was essentially exploratory, we used Bonferroni correction for multiple comparisons within each depth. All statistical analyses were carried out with the Proc Mixed procedure in SAS (SAS Institute, 2004).
RESULTS
Clinical Evaluation (Baseline and 3-month Recall)
No adverse events related to RCPC material were reported. Clinical characterization of affected (C) dentin at the cavity floor pre- and post-caries removal (CR) showed the distribution of ‘soft/medium/ hard’ tissue to be 69/31/0 % (Pre-CR), 8/92/0 % (Post-CR), and 0/0/100 %, respectively, at re-entry after 3 mos (re-entry data only for treated caries groups CE and CU). Sound dentin was ‘hard’ at both timepoints: baseline and re-entry.
Quantification of Calcium Levels
Predicted Ca levels (wt%) are shown at intercept (interface, 0 μm depth) and different depths for affected (CN), affected treated/based (CE_CU, pooled), and sound (SE_SU_SN, pooled) dentin (Fig. 2A). The regression line for CN showed a pronounced quadratic effect (p = −0.001), demonstrating increasing Ca levels from the mineral-depleted cavity floor into deeper, less demineralized, dentin. Regression lines for CE_CU (carious teeth that received RCPC-base) were much flatter, indicating a more similar mineral level at the cavity floor and in deeper, sound dentin. For sound teeth, Ca levels appeared to be similar across all depths and all treatments, and regression lines were flat.
Since no difference in Ca levels (Table 2) was observed among sound subgroups (SE, SU, and SN) and between CE and CU (base after etch or no-etch), data from these groups were pooled, allowing for comparison among sound, and base and no-base, caries-affected groups (Fig. 2A).
Quantification of Phosphorus Levels
Predicted P levels (wt%) are presented for affected (CN), affected RCPC-treated (CE_CU, pooled), and sound (SE_SU_ SN, pooled) dentin at various depths (Fig. 2B). Linear and quadratic effects were highly significant for CN. Linear effects were significant for both CE and CU, while quadratic effects were not (data not shown). For sound teeth, only SE showed a statistically significant linear and quadratic effects in phosphorus levels (data not shown). The p-values (Table 2) for phosphoruslevel comparisons showed patterns similar to those of calcium levels, resulting in similar pooling of data.
DISCUSSION
A base material that promotes remineralization of affected dentin and enhances tissue repair would be clinically beneficial and a useful clinical treatment strategy. In vivo strontium and fluorine ion penetration from GIC into dentin showed a penetration pattern consistent with a remineralization process (Ngo et al., 2006). In vivo remineralization data concerning Ca and P are lacking. Studies supporting stepwise excavation have reported the repair potential of carious dentin: Clinical assessment of affected dentin at re-entry showed hard, dry, and dark dentin, characteristic of arrested caries (Bjørndal et al., 1997; Bjørndal and Larsen, 2000). From a caries-preventive point of view, a more mineralized (‘harder’) dentin will not only be more resistant to mechanical forces, but will also delay bacterial accumulation and penetration, halting a potentially recurring caries-active process (ten Cate, 2001).
This study focused on the remineralization-enhancing ability of resin-based Ca-P cement (RCPC). Clinical efficacy of this ionreleasing base material to encourage tissue repair was explored after 3 mos of intra-oral service. At re-entry, qualitative clinical assessment of residual affected dentin suggested lesion reversal, since the dentin floor was hard, apparently remineralized after 3 mos.
The amount of caries to be removed is a point of continual discussion among clinicians. We obtained a standardized endpoint by using a self-limiting polymer bur, leaving remaining affected dentin of 25 KHN Knoop hardness (Peters, unpublished observations; Boston, 2003). Since hardness is the only validated clinical measure (Kidd et al., 1993), this approach provided optimal standardization of the caries-removing process.
Remineralization was quantified by elemental analysis with EPMA. Resulting weight-% (wt%) data for Ca- and P-content in sound dentin were in the same range as those reported previously (Ngo et al., 1997; Hossain et al., 2003a,b), with Ca-levels ranging from 27–32 wt% and P-content from 13–15 wt%. Reports on artificially demineralized dental tissues showed a decrease in mineral content for Ca- and P-levels, with the Ca:P ratio close to 2.2 (Ngo et al., 1997). These data were corroborated by outcomes of this in vivo study, where similar levels and ratios were detected in carious teeth.
In non-treated carious teeth, low Ca- and P-content at the cavity floor indicated the amount of demineralization in the outer lesion area. Mineralization levels gradually increased toward the inner lesion area. This pattern followed the characteristic hardness curve throughout a caries lesion, as described previously (Ogawa et al., 1983). Mineral content peaked at 60–70 μm. The slight decrease of mineral toward the pulp (at depths of 90–100 μm; not significantly different) might be explained by closer proximity to the pulp, where sound deep dentin was less mineralized (Ogawa et al., 1983). Although randomly chosen, this group may have included deeper lesions compared with other groups not showing this phenomenon.
Sound subgroups presented no difference between treated and non-treated teeth. Once mineral content was within normal limits, equilibrium was maintained, and no additional mineral was deposited. When compared with carious teeth, sound teeth showed higher Ca- and P-levels over the entire depth measured, possibly caused by differences in cavity depth. Cavity preparations in sound, vital teeth were, for ethical reasons (post-operative sensitivity), limited to outer dentin, resulting in a higher grade of mineralization than inner dentin (Ogawa et al., 1983).
Acid-etching opens dentin tubules and facilitates adhesive procedures (Brännström and Johnson, 1974). Etching of cavity floor prior to base placement did not result in increased mineral levels in treated carious teeth after 3 mos compared with unetched teeth. Despite patent tubules in etched dentin, remineralization occurred to the same degree as in unetched dentin. This agrees with the concept that lesion repair occurs only by precipitation onto residual crystals and not by new nucleation of mineral on organic matrix (Levine and Rowles, 1973; Daculsi et al., 1979; Tveit and Selvig, 1981; Klont and ten Cate, 1991). A definitive statement, however, cannot be made, since the study was not powered to address the acid-etch stratification. This question needs further study. Even without enhanced remineralization after 3 mos, etching of dentin may still be indicated to achieve optimal adhesion of base material (Dickens et al., 2004).
After 5 mos of in vitro remineralization, artificial root caries lesions (500 μm deep) showed lesion repair corresponding to 50–85% mineral gain and 40% reduction in lesion depth (Mukai and ten Cate, 2002). Depth of mineral deposition in this in vivo study was 30 μm. This is in accordance with data from in vitro studies (range, 20–30 μm depth) (Mukai et al., 1998; Massara et al., 2002; Kitasako et al., 2003; Exterkate et al., 2005). In our in vivo study, after a period of 3 mos, mineral levels were similar at interface and 100 μm into dentin. This supports the clinical use of the Ca- and P-releasing base as a remineralization tool to increase Ca- and P-levels in affected dentin.
The actual depth of demineralization and re-entry time may have influenced the maximum depth at which remineralization occurred. Further investigations focusing on mineral uptake from RCPC base over deeper areas of mineral-depleted dentin (remineralization distance) and at different timepoints (initial remineralization mechanism, longer-term remineralization extent) are warranted to reveal a complete picture of the in vivo potential of RCPC to replenish Ca- and P-ions in caries-affected dentin.
Composition of the Resin-Based Calcium-phosphate Cement (RCPC)
Mineral Content: p-values* for Comparisons of Groups
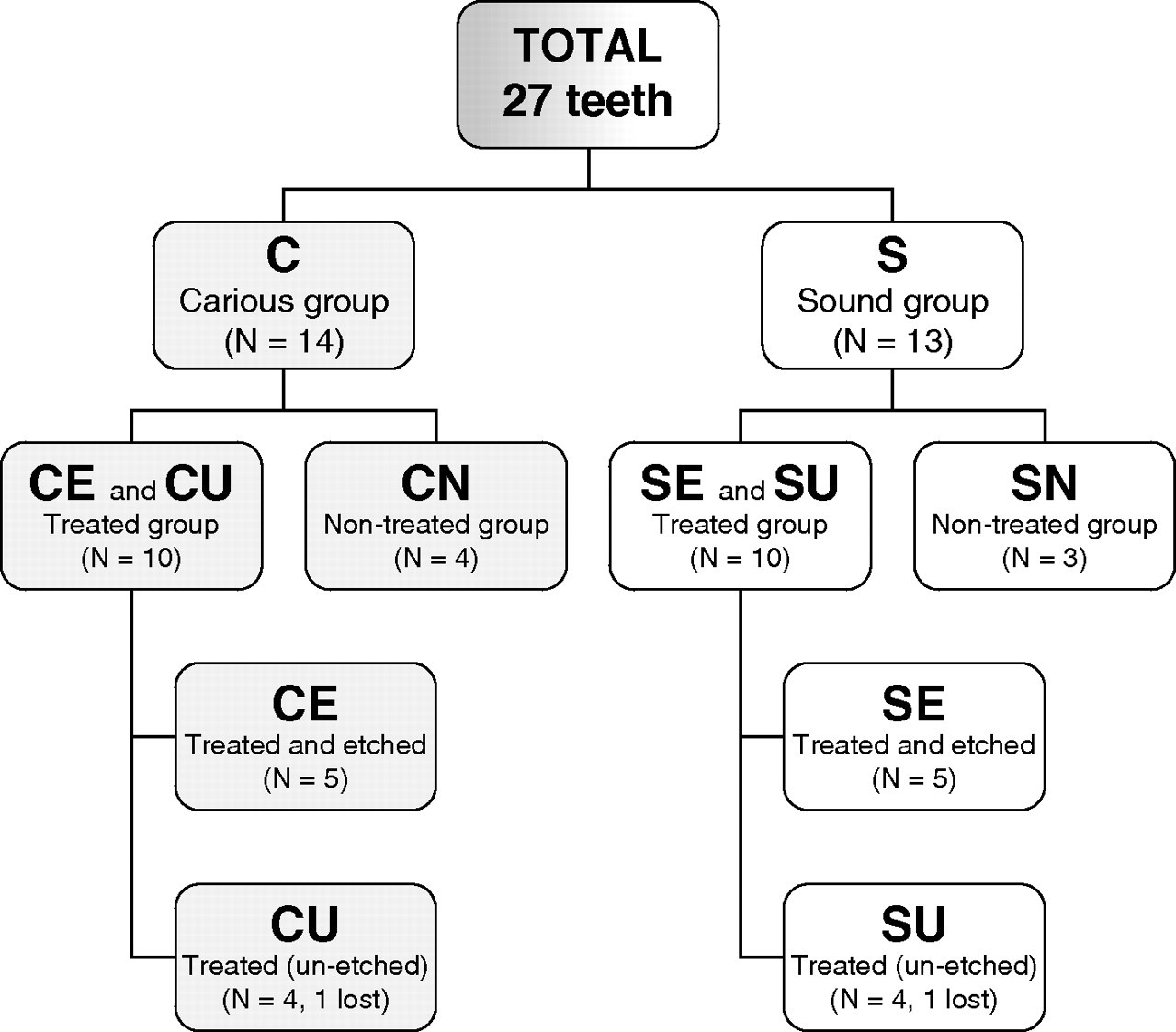
Sample distribution.
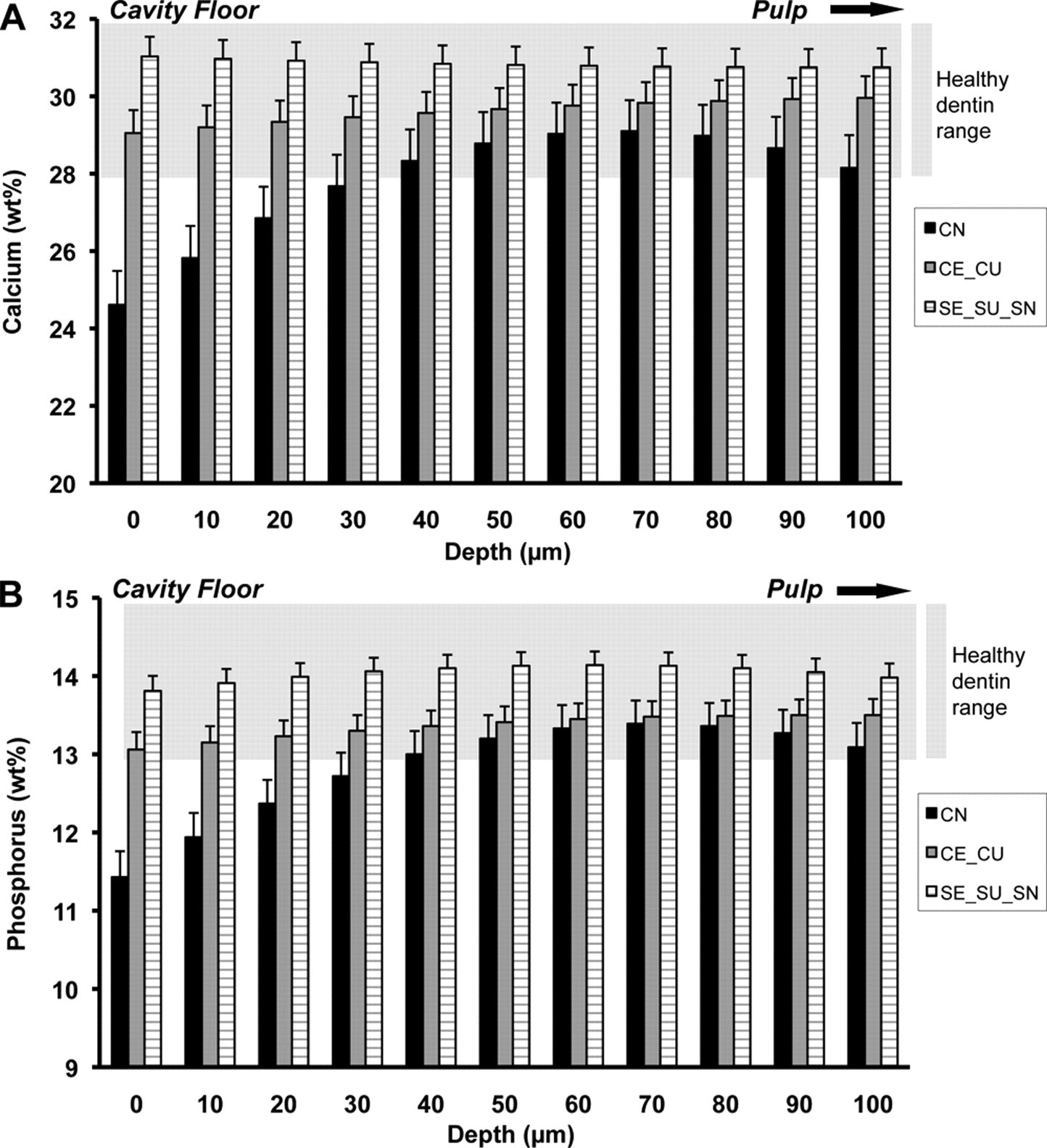
Mineral content of the cavity floor (p-values in Table 2). Connection of datapoints per group by a line provides the regression lines for each group from cavity floor up to 100 μm into dentin towards the pulp. (
Footnotes
Acknowledgements
The authors thank Dr. R.B. Rutherford (University of Washington, Seattle) for contributing to the study design and the manuscript, Carl Henderson (UM-EMAL) for EPMA assistance, Kathy Welch (UM-CSCAR) for invaluable statistical assistance, and S.S. White Burs for providing SmartPrep-Systems®. This study was supported by Dentigenix/Ivoclar-Vivadent AG (Schaan, Liechtenstein), by the University of Michigan, and by CAPES #BEX3404-8 (Brazil). Co-author SHD developed the cement at the Paffenbarger Research Center, American Dental Association Foundation. She was not involved in sample collection or the analysis of data, but contributed to manuscript writing. Preliminary data were presented at the 2006 Annual Meetings of the Academy of Operative Dentistry (Chicago), the American Association for Dental Research (Abstr# 481, Orlando), and the Academy of Dental Materials (São Paulo, Brazil).