
Abstract
The evidence concerning the management of shortened dental arch (SDA) cases is sparse. This multi-center study was aimed at generating data on outcomes and survival rates for two common treatments, removable dental prostheses (RDP) for molar replacement or no replacement (SDA). The hypothesis was that the treatments lead to different incidences of tooth loss. We included 215 patients with complete molar loss in one jaw. Molars were either replaced by RDP or not replaced, according to the SDA concept. First tooth loss after treatment was the primary outcome measure. This event occurred in 13 patients in the RDP group and nine patients in the SDA group. The respective Kaplan-Meier survival rates at 38 months were 0.83 (95% CI: 0.74-0.91) in the RDP group and 0.86 (95% CI: 0.78-0.95) in the SDA group, the difference being non-significant.
Keywords
Introduction
There are essentially three viable treatment options for patients with complete molar loss in one jaw: preserving or restoring a premolar occlusion, molar replacement with a removable dental prosthesis (RDP), and fixed restoration with dental implants. A premolar occlusion is a limited treatment goal following the principles of the shortened dental arch (SDA) concept. Only RDPs and implant restorations allow for the replacement of all missing molars.
The SDA concept was originally introduced by Käyser and has been further documented by the Nijmegen group (Käyser, 1981; Witter et al., 1999). The approach is accepted in the professional community (Allen et al., 1998; Korduner et al., 2006). It may provide acceptable oral function while being a cost-effective option (Allen, 2008). In a review on the shortened dental arch concept, most included papers were either based on questionnaires measuring different outcomes or they were retrospective clinical trials (Kanno and Carlsson, 2006). The authors concluded that the concept deserves serious consideration in treatment planning, while continued clinical research within properly designed experimental studies is required.
Only very few data are available from comparative studies on the outcomes of different treatment approaches (Jepson et al., 2003; Thomason et al., 2007). Thus, the need for randomized clinical trials is apparent. This study aimed at generating reliable outcome data with regard to treatment following the SDA concept compared with molar replacement with RDPs. The hypothesis was that different treatments lead to differences in the incidence of tooth loss, due to substantial differences between the clinical approaches.
Materials & Methods
Study Design
The study was designed as a multi-center, randomized, controlled clinical trial with 14 participating dental schools (Walter et al., 2001). The trial and the clinical protocol were approved by the Institutional Review Board (TU Dresden, EK 260399). The study has been registered at ClinicalTrials.gov under ISRCTN68590603 (pilot study) and ISRCTN97265367 (main study). In this paper, the three-year results are reported.
Participants
Any patient over 35 years old who requested prosthetic treatment and exhibited dental status matching the following inclusion criteria was considered for participation. All molars had to be missing in one jaw (study jaw), with at least the canine and one premolar present on each side. Further inclusion criteria were good health according to ASA classification group one or two (ASA, 1963) and the rejection of implant treatment. Exclusion criteria were psychological disorders, craniomandibular disorders, malocclusion (Angle Class II or III), and drug abuse.
Once a patient had given informed consent, randomization was conducted by tables with randomly permuted blocks of 6, stratified for center and age (over/under 50 yrs). The allocation concealment was warranted because randomization was conducted centrally (Department of Medical Informatics and Biomathematics, University of Münster). The obvious discrepancies between the two treatments allowed for no blinding.
Interventions
Patients were allocated either to:
RDP Treatment: Molar replacement
Molars and, if needed, second premolars were replaced by an RDP. This RDP was retained by precision attachments (Mini SG No. 055 675, CMSA, Biel, Switzerland). Attachments were connected to either splinted crowns or a fixed dental prosthesis (FDP) abutment on the posterior-most tooth on each side.
or
SDA Treatment: No molar replacement
If the posterior-most tooth was the second premolar, no extension of the dental arch for molar replacement was conducted. If it was the first premolar, a cantilever FDP for the replacement of the missing second premolar was incorporated. If all premolars and anterior teeth were present, no prosthetic treatment was provided.
In both treatment groups, missing anterior teeth in the study jaw were replaced by FDPs. Any endodontically treated abutment tooth was restored with a cast post and core. The opposing jaw had to be sufficiently restored up to the first molar (for RDP treatment) or the second premolar (for SDA treatment).
In most cases, an appropriate pre-treatment had to precede prosthetic treatment. Periodontal conditions were considered acceptable in case of pocket depths ≤ 4 mm and bleeding on probing rates ≤ 25%. All restorations were made according to a standardized protocol.
Outcomes
The first tooth loss after prosthetic treatment, regardless of the jaw, was the primary outcome. Tooth loss is a viable indicator of oral health and can be measured with high reliability. Several secondary outcome measures were recorded (Walter et al., 2001; Wolfart et al., 2005). They will be the subject of further publications.
The required sample size was calculated in advance, presuming an expected tooth loss rate of 20% for RDP and 5% for SDA after five years’ follow-up. Applying a two-sided primary significance test (alpha = 5%), we required 70 patients per group to provide 75% power of detecting treatment differences of the above magnitude. The basic design of the study constituted a group sequential plan, according to the O’Brien-Fleming approach (O’Brien and Fleming, 1979). Two interim analyses were scheduled after 1.5 and 3 years’ follow-up, respectively, and a final analysis after 5 yrs. To control for an overall type I error of alpha = 5% (two-sided), we performed interim analyses for significance levels alpha = 0.05% and 1.4%, respectively, and the final analysis for alpha = 4.5%. This report presents the results of the second interim analysis.
Follow-up visits were scheduled at 4 to 8 wks (baseline), at 6 mos, and at 1, 2, 3, 4, and 5 yrs after treatment.
All statistical analyses were based on the intention-to-treat principle. Kaplan-Meier survival analyses were performed. The survival distributions were compared with the Mantel-Cox logrank test (SPSS, Version 15.0.1, SPSS Inc., Chicago, IL, USA). The incidences of tooth losses and the survival analyses refer to 38 mos.
Results
Flow of Participants
The enrollment period was 01/2001 to 02/2004. Of 215 enrolled patients, 109 were allocated to RDP treatment and 106 to SDA treatment.
Eighty-one patients received RDP treatment, and 69 patients received SDA treatment between 01/2002 and 03/2005 (Fig. 1). For details on patients who dropped out and about patients’ dental and prosthetic status, see the Appendix.
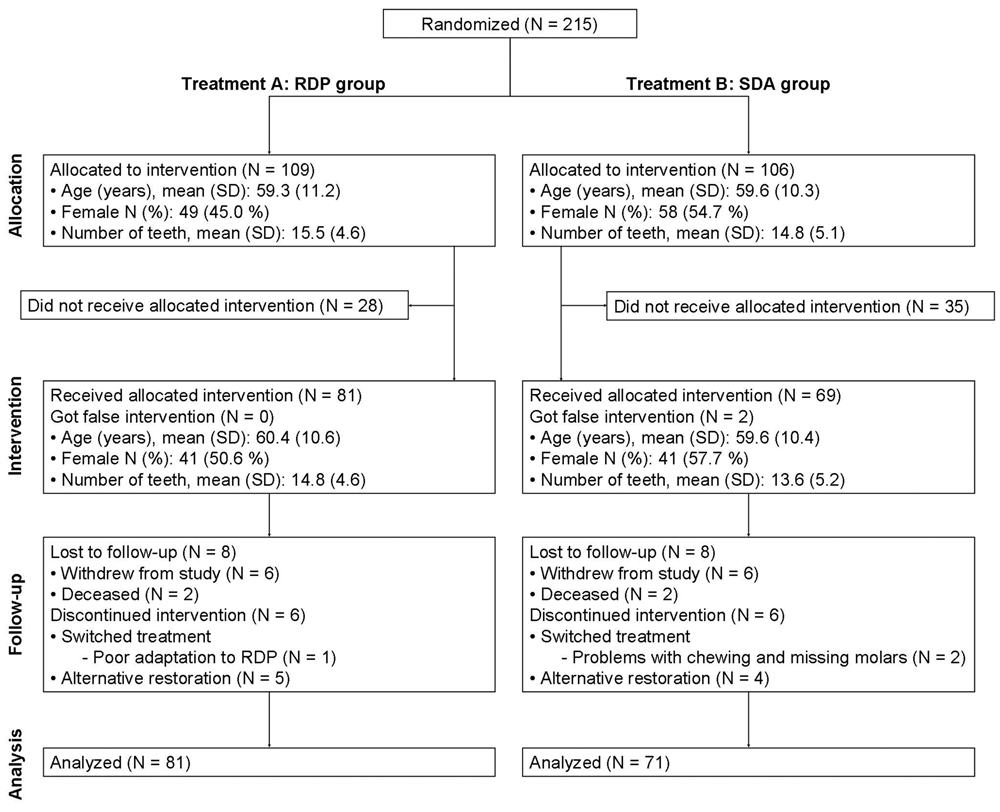
Flow of participants.
The number of drop-outs prior to treatment did not differ significantly between the treatments. For both treatments, no significant differences were found between treated patients and patients who dropped out prior to treatment with regard to age, number of teeth, as well as presence and types of restorations. The number of males was significantly higher in the drop-out patients than in those actually treated in the RDP group.
Tooth loss (primary outcome) occurred in 13 patients in the RDP group and nine patients in the SDA group (Table). In the RDP group, 5 extractions occurred in the study jaw, 8 in the opposing jaw. Reasons for extraction were endodontic complications (N = 9), caries (N = 3), or fracture (N = 1). In the SDA group, 5 extractions occurred in the study jaw, 4 in the opposing jaw. Reasons for extraction were endodontic complications (N = 4) or fracture (N = 5). Additionally, analyses for a modified primary outcome considering exclusively the extractions in the study jaw were conducted (modified primary outcome). Tooth loss (modified primary outcome) occurred in six patients each in the RDP group and the SDA group. In five cases each, abutment teeth were affected. In one case each, this modified primary outcome occurred after an initial extraction had been performed in the opposing jaw (and had been counted as primary outcome). Kaplan-Meier survival analyses were conducted for the primary outcome and the modified primary outcome. No significant differences between the survival distributions of both treatments could be found. This applied to both the primary outcome and the modified primary outcome (primary outcome, p = 0.57; modified primary outcome, p = 0.83). The graphs of the survival functions for both treatments were very similar. For the modified primary outcome, survival probability decreased slightly earlier in the SDA group, but at 38 mos was equal to the value in the RDP group (Figs. 2, 3). None of the three patients who switched treatment was affected by the primary outcome event or modified primary outcome event.
Primary Outcome Data at 38 mos (95% confidence interval in parentheses)

Removable Dental Prosthesis. ** Shortened Dental Arch.
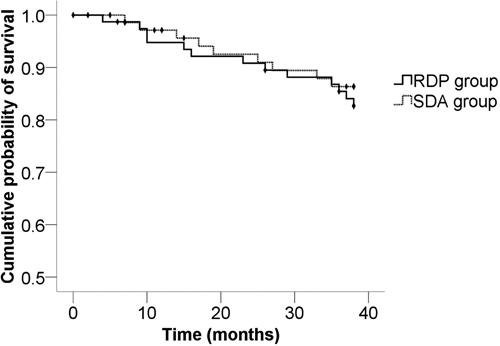
Kaplan-Meier survival function for the primary outcome measure. RDP (removable partial denture) group: N = 81. SDA (shortened dental arch) group: N = 71.
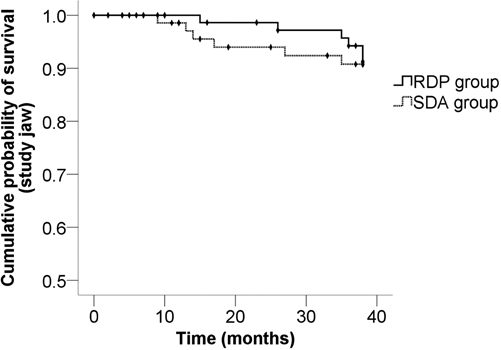
Kaplan-Meier survival function for the modified primary outcome measure. RDP (removable partial denture) group: N = 81. SDA (shortened dental arch) group: N = 71.
Discussion
The use of data from existing trials for the comparison of fixed and removable treatment options for shortened dental arches is not an option, because treatments often are allocated based on clinical indication (Wöstmann et al., 2005). This introduces a bias and makes the randomized trial design the only feasible option. Excluding implant treatment indeed limited the conclusions. However, including a third treatment option was not considered a viable approach. In that case, most probably a much higher proportion of the patients would have refused further participation after randomization, because many of them might have had a predetermined positive or negative attitude toward implants.
The most important confounders in prosthetic treatment studies are the dentist him/herself, the applied treatment principles, and the treatment environment (Graham et al., 2006). The multi-center approach, involving almost half of all German dental schools, and extensive training of investigators, dentists delivering the treatment, and study nurses were considered appropriate to reduce this bias.
While the trial was powered to detect differences in the primary outcome at 5 yrs, a report on the second scheduled interim analysis at 3 yrs was considered important. The incidence and progression of tooth loss in both groups represent meaningful results allowing for preliminary clinical implications. The same applies to the lack of significant differences between the treatments, along with low p-values.
The relatively high number of patients who did not receive the allocated treatment is intrinsic to a complex prosthetic trial and inevitable. The main reason for their high proportion was that patients with apparently predetermined preferences simply tested whether they would be offered that option. Further reasons were financial limitations or ineligibility after pre-treatment. For the outcome tooth loss, however, the resulting bias might be negligible. The RDPs were attachments retained on splinted crowns and FDPs. Because of critical differences in design and denture dynamics, no conclusion can be drawn with regard to clasp-retained dentures.
The study hypothesis could not be confirmed. The primary outcome, tooth loss, could be considered too unspecific to deliver usable results within a reasonable observation time. Surrogate parameters such as caries and periodontal attachment loss are therefore more widely used and probably more suitable to deliver early results and differences. The respective data collected within this trial will be the subject of further publications. However, because of its high impact and reliability, tooth loss is a very robust indicator of oral health. The rationale behind defining tooth loss as the primary outcome measure regardless of the jaw was the known impact of a prosthetic treatment on the opposing arch. For instance, a shortened dental arch might lead to a higher loading of the opposing teeth. In contrast, the analysis of tooth loss in the study jaw only (modified primary outcome) was also conducted to improve comparability with other studies.
Because of the multi-center design, the results can be extrapolated to patient groups comparable with those of this study. In the setting up of an appropriate trial design, standardized criteria and procedures are mandatory. For this reason, the results cannot be simply applied in a general practice environment.
The survival rates relative to the primary outcome were relatively low considering the standardized study conditions. More than half of the first tooth losses occurred in the opposing jaw. Although the required condition of the opposing jaw was clearly defined, pre-existing restorations with a satisfactory, but less predictable, prognosis had to be accepted. This explains the survival data relative to the primary outcome. Also, it had not been expected that not even a tendency to a difference between the treatments could be found. Although the five-year results are forthcoming, a substantial change of the results is unlikely. Tooth loss is increasingly considered a complex outcome influenced by an array of clinical, behavioral, socio-economic, and cultural factors (Holm-Pedersen et al., 2007; Müller et al., 2007). A further explanation for the absent differences could be that the extent to which the incidence of tooth loss can be influenced by restorative measures is minor (Müller et al., 2007).
In all analyses, the overall approach applied to tooth loss in our study has to be taken into account. In patients with a considerable number of remaining teeth at risk, this may lead to much higher incidences than when only the loss of abutment teeth is reported. Several papers are available on the clinical outcome of certain prosthetic appliances relevant to this study, such as FDPs, cantilever FDPs, and RDPs. Comparisons of the respective survival data are difficult if not impossible (Goodacre et al., 2003). Data on tooth loss rates are extremely rare. Less than 5% of FDP abutments were found to be removed at 10 yrs (Scurria et al., 1998; Tan et al., 2004). The incidence of the loss of abutment teeth of different types of RDPs has been reported to be from 3.4 to 11.4% after a 5.3- to 8.1-year function period (Saito et al., 2002). In telescopic crown-retained removable dental prostheses, abutment teeth were found to be lost in 3.8% of the cases after a mean observation period of 5.3 yrs (Wöstmann et al., 2007). In a retrospective study on telescopic dentures, 8.8% of abutment teeth were lost within a mean period of function of 6.26 yrs (Dittmann and Rammelsberg, 2008). In a highly heterogeneous sample, a retrospective evaluation of RDPs gave a tooth loss rate of 9.8% after 4 to 17 yrs (Vanzeveren et al., 2003).
There are no published studies available that allow for a comparison with our results. In a randomized clinical trial, treatments of shortened dental arches with cantilever resin-bonded bridges and RDPs were studied. The latter group showed a significantly higher rate of new or recurrent caries over 2 yrs. Of a total of 312 teeth in 60 patients, 4 (1%) fractured (Jepson et al., 2001). After 5 yrs, no significant differences in failure rates between the two treatment groups could be found in the same cohort. Tooth loss rates were not reported, although the authors assumed a higher risk of tooth loss through caries in the RDP group (Thomason et al., 2007).
In conclusion, tooth loss was more frequent than expected, at least in the SDA group. Moreover, the anticipated differences between the treatments could not be shown. The observation period of 3 yrs might have been too short for these differences to be detected, especially with regard to the statistical power calculation that aimed at a five-year observation period. If the five-year results, however, confirm the current observation—that tooth loss and other clinical parameters are not or are only weakly associated with the type of prosthetic treatment in shortened dental arch cases—this strengthens the importance of considering patient preferences in clinical decision-making.
Footnotes
Acknowledgements
This study was supported by the Deutsche Forschungs gemeinschaft (German Research Association), grant DFG WA 831/2-1 to 2-6, grant DFG WO 677/2-1.1 to 2-2.1.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.