
Abstract
Temporomandibular disorders (TMDs) are a common group of chronic illnesses. There is evidence that health professionals find them difficult to diagnose and manage. A consequence of this difficulty in diagnosis might be that sufferers of TMDs have an experience of illness comparable with other chronic illnesses. To explore the sufferers’ experience of TMDs, we conducted a qualitative study with a purposive maximum variation sample of secondary care TMD patients. Semi-structured interviews were conducted with the sample and were recorded and transcribed verbatim. Data collection and analysis continued until data saturation (n = 19). For analysis, we broadly followed the constant comparative method and used frameworks to organize the data. The key finding was that a lack of diagnosis caused uncertainty over the nature of the cause of the sufferer’s complaint. This uncertainty reportedly caused negative impacts on sufferers’ daily lives. Clearly, diagnosis of TMDs needs to be encouraged at the first point of contact.
Introduction
Chronic illnesses are prevalent in Western societies (Wilson et al., 2005), and their management presents challenges to health service policy and provision (DoH, 2005). At an individual level, being diagnosed with a chronic condition is likely to have a significant effect in terms of both how individuals perceive themselves and how their condition affects their everyday life (Bury, 1982; Charmaz, 1983). Some chronic conditions, however, can be difficult to diagnose (Zavestoski et al., 2004; Jerlock et al., 2005; Nettleton, 2006). Individuals who experience symptoms of a chronic illness and do not receive a diagnosis can encounter particular difficulties, because obtaining a diagnosis is one means of legitimizing symptoms and illness experience (Shaul, 1995; Glenton, 2003; Lillrank, 2003).
There is evidence that temporomandibular disorders (TMDs) constitute a group of chronic illnesses which health professionals find difficult to diagnose, manage, and understand with any degree of certainty (Just et al., 1991; Le Resche et al., 1993; Garro, 1994; Durham et al., 2007). This article aims to describe the difficulties that sufferers of TMDs encounter in obtaining a definitive diagnosis of their condition and to examine critically the impact this has upon them.
Materials & Methods
This qualitative study sought to explore TMD sufferers’ experiences of their illness and care. NHS Research Ethics Committee approval was obtained prior to the commencement of data collection. We used a purposive maximum variation sample to obtain a broad range of patient experiences (Table). The sample was recruited from a hospital in the North East of England. A secondary specialist care center was chosen, since patients here were likely to have the longest experience of care and be able to provide more detailed accounts of their experiences. The sample used for this study is detailed in the Table.
Purposive Sample Details
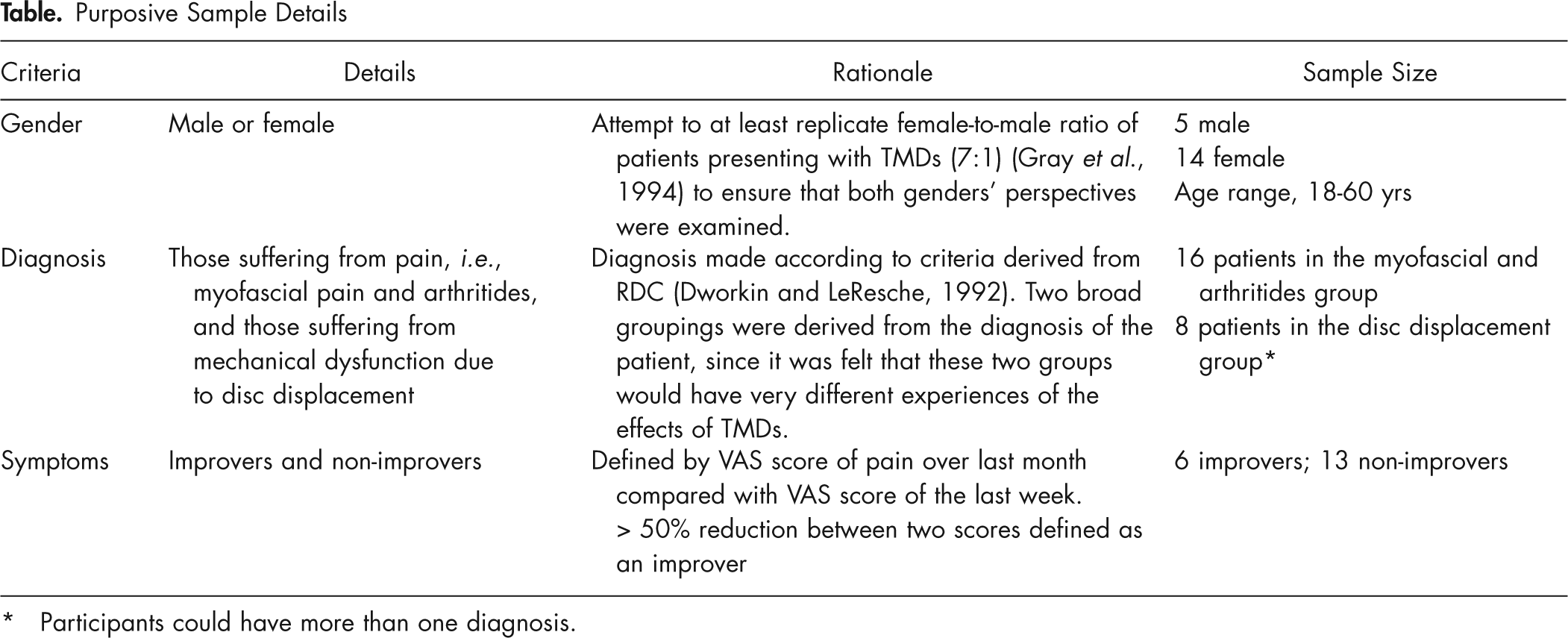
Participants could have more than one diagnosis.
Recruitment took place through specialist oral and maxillofacial surgery and restorative dentistry clinics. Consultants identified potential interviewees to nurses, who then gave a standardized information sheet to each individual to read. If they were willing to participate, an interview time was arranged. Only two individuals declined to participate, due to difficulties in arranging a time to come back for an interview. All patients interviewed had experienced more than 3 months’ treatment in secondary care. This time in treatment was selected since we felt that interviewees fitting this criterion would be able to discuss in depth the perceived effects of TMDs, the initial consultation, and subsequent management.
Semi-structured interviews were used to examine sufferers’ experiences. Semi-structured interviews cover a pre-determined set of questions or topics with each respondent, but are designed to enable people to respond in an unrestricted way and are flexible enough to allow new topics to be introduced by respondents or the interviewer if appropriate. Topics covered within the interview included: experiences and perceptions of first symptoms, experience of obtaining a diagnosis, current management, and the impact of TMDs on everyday lives. Written informed consent was obtained prior to interview. All interviews were conducted in a comfortable office away from the clinic at a time convenient to the interviewee.
Interviews were conducted by JD and recorded on digital media, transcribed verbatim, and their anonymity was maintained. Data collection and analysis broadly followed the principles of the constant comparative method, whereby data collection and analysis occur concurrently, allowing earlier propositions to be explored in subsequent interviews (Glaser, 1965). With this method, data collection continues until no new themes emerge from the data; in this study, this occurred after 19 interviews. Both JD and CE coded the data, and a line-by-line approach was used for data analysis (Strauss and Corbin, 1990). An inductive and iterative process was used to develop theory from the data. To help organize and facilitate the process of data analysis, we placed data in frameworks. Two different types of framework helped organize the data: (1) a case-by-case framework, whereby each individual respondent could be examined against all emergent recurrent themes; and (2) thematic frameworks, whereby each theme could be examined across all respondents (Ritchie and Lewis, 2003).
Results
In this section, each emergent theme appears in bold type and is represented by illustrative quotes to support the discussion presented. Further illustrative quotes from the emergent themes can be found in the Appendix.
After patients experienced their first symptoms, they commonly reported consulting with their primary care general dentist (PCGDP). Often respondents referred to this early time in their care as being a time of ‘uncertainty’, caused by inadequate or partial explanations of their symptoms by the clinician.
“He [the PCGDP] just said that he wasn’t sure why it was doing that [the jaw locking] so it might have been because I had a lot of work done before on my teeth and stuff and it could have been from that.” (Sufferer 2)
In addition to receiving inadequate explanations for their symptoms, patients also experienced ‘uncertainty’ when they failed to receive a diagnosis. There was recurring
“Well, he [the PCGDP] x-rayed my tooth to see if it was something… a problem there. And he said whilst he couldn’t see anything really wrong… And he said he would refer us up to the dental [hospital] to have it checked out…He said the kind of facial pain I had he said I think I’ll refer you to the experts.” (Sufferer 7)
For most people, the initial primary care consultation compounded the uncertainty and
“Well, I felt terrible, especially when my GP [general medical practitioner] refused to refer me anywhere and told me I was a timewaster who was just imagining it. And, you know, not to bother him anymore.” (Sufferer 8)
With no clear diagnosis from primary care, while awaiting a secondary care appointment, most respondents began to develop their own explanations for their symptoms. Unfortunately, this often led to
“It preyed on my mind…because I did have a big pain, you know…the girl I worked with she’s got a brain tumour … she’s had it about five years now. She had headaches for a long time… You know, it sounds really hard, but you think.” (Sufferer 9)
“I think it [the pain and problems] got worse in a sense. And I was probably becoming more distressed because I thought that once the tooth was taken out, and that was a big step to have something like that removed, that it would be okay [the pain and problems would be resolved].” (Sufferer 3)
Waiting to be seen in secondary care and the ongoing symptoms (headache, facial pain, decreased mouth opening) had considerable negative effects on sufferers’ everyday lives. The constant pain experienced by some was regarded as having negative effects on close personal relationships, social activities, and job performance.
“It [TMDs] sort of made us…when it was really, really bad, a little bit irritable. People seemed to like get on my nerves… I felt as if sometimes I used to take it out on my husband.” (Sufferer 7)
The lack of or uncertainty about their diagnosis caused some people to question the ‘legitimacy’ of their symptoms. In particular, the lack of a diagnosis seemed to make sufferers feel that others might perceive that there was “nothing wrong” with them, or that they may be malingering. Such
“I got to the point where because I’d complained about it so much I just stopped complaining because…no-one seems to know what’s wrong. So you think oh maybe it’s just me, you know, psychosomatic.” (Sufferer 3)
“I think parents and parents-in-law were just fed-up of this woman that was always in pain. Always in the corner, you know, at a party taking painkillers and drinking water rather than having fun.” (Sufferer 8)
Finally receiving a diagnosis in secondary care was always reported positively; having a ‘label’ for their condition was very important.
“I mean you had a name for it and you knew you weren’t alone with it so it eased your mind totally really knowing that it wasn’t anything too serious.” (Sufferer 7)
Analysis of these data suggests that receiving a diagnosis – that is, the acknowledgment and naming of their illness – was integral to respondents beginning to manage the illness successfully (
“You want a magic wand waved over and then it’s [the pain’s] gone…Then reality kicks in and you think no that’s in never never land, that’s not the way it works.” (Sufferer 13)
Discussion
The sufferers interviewed gave clear accounts of the difficulties, concerns, and uncertainty they experienced during their illness. This uncertainty, largely due to the lack of a diagnostic label, meant that respondents often felt that friends and family might find their story difficult to listen to or to believe; this is similar to other work on the narratives of ill individuals (Frank, 1995).
The disruption in sufferers’ day-to-day lives caused by TMDs also meant that their story, or narrative, continued to evolve. They felt that they lacked legitimacy in their complaint, due to the lack of a diagnosis, and their narrative only ended once a diagnostic label was applied.
The difficulties experienced by TMD sufferers in obtaining a diagnosis meant that they often searched for explanations of their signs and symptoms. The literature shows that this search can be a double-edged sword: Sufferers may receive a diagnosis, or, by repeatedly questioning the authority of different clinicians, they may find themselves labeled/typified as troublesome or difficult (Friedson, 1970; Jeffery, 1979; Garro, 1994).
The difficulties in, and the importance of, obtaining a diagnosis demonstrated in this study are supported by findings from other studies about chronic illness and medically unexplained symptoms (Shaul, 1995; Glenton, 2003; Lillrank, 2003; Grytten and Maseide, 2005). The major difference between TMD sufferers and studies examining other chronic illnesses, such as rheumatoid arthritis and back pain (Shaul, 1995; Glenton, 2003; Lillrank, 2003), is that our respondents reported their symptoms worsening due to the anxiety over the source of their complaint.
Once a diagnostic label was obtained, sufferers interviewed in this study reported that they were more able to manage their illness and had the potential to be “successfully ill”. Some of this sample of sufferers could be defined as being part of ‘a remission society’ (Frank, 1995); that is, they have reconstructed their narrative, and their selves, and now live successfully with an illness.
This study is a qualitative study of sufferers’ experiences within a specialist secondary care setting within the UK. Further research is therefore required to explore sufferers’ experiences in other health care contexts, and this would be helpful to understand the generalizability of our findings. The sufferers’ accounts of the difficulties they experience in receiving a diagnosis are, however, reflected in professional accounts of TMDs, where negative stereotypes of patients were implicitly evident (Durham et al., 2007). Analysis of our data suggests that those suffering from TMDs experience many of the same problems of uncertainty and concern faced by those with other non-oral chronic conditions. Analysis of data from this study, and from other work on chronic illness, suggests that achieving a diagnostic label is important for patients to learn to adjust to their conditions.
Uncertainty in dental chronic illness – specifically, a reluctance to provide a diagnostic label – is likely to have a negative impact on patients and cause unnecessary worry. A better understanding of the psychosocial effects of TMDs may allow clinicians to address these effects with their patients and attempt to reduce them. Analysis of our data suggests that the introduction of simple diagnostic indices (Hasanain et al., 2009) – even if provisional - might help consultations and reduce the anxiety of sufferers.
Footnotes
Acknowledgements
The authors acknowledge the financial support received from Newcastle Healthcare Charity, which funded this research, and thank all the patients whose individual stories made this article possible. We are grateful to the anonymous reviewers for their positive critique and for drawing our attention to the work of Garro.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.