
Abstract
Bifidobacteria are aciduric bacteria that might play a role in the caries process. To test the hypothesis that Bifidobacteria behave as caries-associated organisms, as predicted by the ecological plaque hypothesis, we determined salivary levels of Bifidobacteria and caries-associated organisms for 156 older adults. Salivary levels of Bifidobacteria, mutans streptococci, lactobacilli, and yeasts were correlated with each other (p < 0.001), negatively correlated with salivary flow rate (p < 0.001), and positively correlated with plaque index (p < 0.05). Salivary Bifidobacteria levels were positively associated with the number of filled (p < 0.001) and decayed (p = 0.036) tooth surfaces and negatively associated with number of teeth (p < 0.001) and salivary flow rate (p = 0.049). In regression analyses, caries experience was significantly associated with only salivary Bifidobacteria (p < 0.001) and yeast (p < 0.001) levels and the individual’s age (p = 0.021). Bifidobacteria should be regarded as caries-associated organisms whose role in the caries process and as markers of caries risk requires further investigation.
Keywords
Introduction
The ecological plaque hypothesis (Marsh, 1994) is the most widely accepted model to explain the role of the oral microbiota in the caries process. This model proposes that microbiota, able to take advantage of an oral environment conducive to caries initiation, will proliferate. The advantaged organisms, caries-associated organisms, include lactobacilli, yeasts, and mutans streptococci, while certain other species, Streptococcus gordonii and Streptococcus sanguinius, are disadvantaged. Bifidobacteria are sometimes hypothesized to play a role in caries pathogenesis (Becker et al., 2002; Beighton, 2005). However, while there are abundant data to support the hypothesis that lactobacilli, yeasts, and mutans streptococci behave as predicted by the ecological plaque hypothesis (Beighton et al., 1991; van Houte, 1993; Fure, 1998; Närhi et al., 1998), there are no equivalent data for Bifidobacteria. Further, there are no data in which the salivary levels of Bifidobacteria are associated with the salivary levels of the accepted caries-associated organisms or caries experience.
The major human habitat for Bifidobacteria is the gut, with around 30 species (Ventura et al., 2004), but the number of recognized oral Bifidobacteria is much smaller and includes Bifidobacterium dentium, Scardovia inopicata, Parascardovia denticolens, and Alloscardovia omnicolens (Scardovi and Crociani, 1974; Crociani et al., 1996; Jian and Dong, 2002; Huys et al., 2007), while “Scardovia sp. T01-04” and “Scardovia genomospecies C1” have also been reported (Munson et al., 2004; Hooper et al., 2006). Bifidobacteria have been sporadically isolated from saliva, supragingival plaque, endodontic infections, and infected dentin (Edwardsson, 1974; Sanyal and Russell, 1978; Maeda, 1980; Moore et al., 1984; Hoshino, 1985; van Houte et al., 1996; Becker et al., 2002; Chavez de Paz et al., 2004; Aas et al., 2005; Chhour et al., 2005; Modesto et al., 2006; Hojo et al., 2007). Bifidobacteria have been detected in high numbers from caries lesions in children (Becker et al., 2002), but, with a 16S rRNA cloning strategy, Bifidobacteria were undetected in the mouths of healthy individuals (Aas et al., 2005) and in active root caries lesions (Preza et al., 2008). There is clearly a discrepancy in the reported association of Bifidobacteria with caries, and this may be due to the primer sequences designed to amplify all 16S rRNA genes from DNA extracted from mixed microbial populations having reduced homology for Bifidobacteria (Frank et al., 2008).
The development of novel selective media containing mupirocin (Rada and Petr, 2000) enabled Bifidobacteria in root caries lesions in adults and occlusal lesions in adults and children to be enumerated and identified (Mantzourani et al., 2009a,b). In this report, we used conventional culture techniques to investigate the hypothesis that Bifidobacteria exhibit characteristics similar to those shown by the accepted caries-associated microbiota.
Materials & Methods
Participants
Fully or partially dentate patients (n = 156; 99 female and 57 male) with a minimum age of 60 yrs (mean = 70.4 ± 7.2 yrs; maximum 90 yrs) were enrolled into the study. None had been taking prescribed antibiotics in the previous 4 wks, and all had > 6 teeth. The study was approved by the local ethics committee, and all participants gave informed consent to their inclusion in the study.
Clinical Examination
The clinical caries status of all coronal (DMFs) and root (root-DMFs) decayed, missing, and filled tooth surfaces was recorded based on nationally agreed criteria (Kelly et al., 2000). Gingival (GI) and plaque (PI) indices, denture-wearing status, and denture plaque scores were recorded as previously described (Simons et al., 2001, 2002). The total of all caries experience was calculated by the summation of DMFs and rootDMFs as AllDMFs. All examinations were by the same investigator (M.Al-H), who had been trained and calibrated by other experienced clinicians, and kappa scores for inter-examiner reliability were 0.86 for coronal caries and 0.78 for root caries. A stimulated saliva sample was collected from each participant, who chewed a sterile paraffin wax tablet for 5 min and expectorated all saliva into a sterile container, enabling salivary flow rate to be determined. The saliva samples were delivered on ice to the laboratory within 3-4 hrs.
Microbiological Investigations
The salivary levels of mutans streptococci, lactobacilli, and yeasts were determined (Beighton et al., 1991). The Bifidobacteria levels in saliva were determined with the use of a selective medium (MMTPY; Mantzourani et al., 2009a) consisting of Proteose Peptone (Oxoid, Basingstoke, UK) 7 g, Soya Peptone (Oxoid) 5 g, Yeast extract (Oxoid) 5 g, glucose 15 g, raffinose 5 g, cysteine.HCl 0.5 g, K2HPO 2 g, MgCl2.6H2O 0.5 g, ZnSO4.7H2O 0.25 g, CaCl2 0.15 g, FeCl3 0.001 g, agar 15 g, and Tween 80 1 mL per L of de-ionized water. The medium was autoclaved at 15 psi for 15 min, cooled, and 1 mL of glacial acetic acid and 1 mL of a 5 mg/mL mupirocin 50% ethanolic solution were added. The MMTPY medium was incubated anaerobically for 4 days, and typical Bifidobacteria colonies were counted. To confirm the reliability of the bifid enumeration process, we identified a number of each colony type presumptively identified as Bifidobacteria from 124 samples using 16S rRNA sequencing (Mantzourani et al., 2009a).
To assess the acidogenicity of the predominant Bifidobacte-rium, B. dentium, we grew 25 independent isolates on two separate occasions in Brain Heart Infusion supplemented with 1% (w/v) glucose at 37°C for 7 days, and the medium pH was determined with the use of a glass electrode.
Statistical Analysis
Salivary concentrations of micro-organisms were calculated as log10(colony-forming-units [cfu] + 1) per mL. Means and standard errors were calculated, and data were compared by the appropriate non-parametric test; Spearman correlation coefficients were calculated. Regression analyses were performed with the individual salivary microbiota levels as the dependent variable, and sex, GI and PI scores, participant age, salivary flow rate, number of teeth, decayed coronal surfaces, filled coronal surfaces, filled root surfaces, and decayed root surfaces as the independent variables, in a stepwise model. Caries experience (DMFs and AllDMFs) was also used as a dependent variable in regression analyses, with sex, GI and PI scores, participant age, salivary flow rate and salivary levels of mutans streptococci, lactobacilli, Bifidobacteria, and yeasts as independent variables, with both a stepwise model and a model with all dependent variables entered simultaneously. Collinearity and multilinearity of variables can significantly impair the interpretation of regression analyses; therefore, the variance inflation factors, tolerance values, and condition indices were calculated for all variables in each of the regression analyses. All analyses were performed with SPSSPC.
Results
The selective medium performed well such that, of presumptive Bifidobacteria colonies (n = 404) subcultured from the MMTPY medium, 367 (93%) were Bifidobacteria, 6 were Gram-positive cocci, 8 were Actinomyces spp., 12 were lactobacilli, and 2 were yeasts. Of the Bifidobacteria, 305 (83%) were B. dentium, 39 (12.8%) were Bifidobacterium longum, 12 (3.9%) were P. denticolens, 14 (4.6%) were S. inopinata, 4 (1.3%) were Bifidobacterium scardovii, and 2 (0.7%) were A. omnicolens. The salivary levels of the caries-associated microbiota and Bifidobacteria are shown in Table 1. Bifidobacteria were isolated from 96.8% of participants, and mutans streptococci, lactobacilli, and yeasts from 91.7, 90.4, and 60.3% of participants, respectively. The salivary levels of Bifidobacteria was significantly (p < 0.001) greater than those of lactobacilli and yeasts, but not significantly different (p > 0.05) from that of the mutans streptococci, and each of these 4 taxa was significantly (p < 0.001) inter-correlated, and each was also significantly (p < 0.001) negatively correlated with the stimulated salivary flow. The mean final pH values of the duplicate pH determinations of the B. dentium cultures were significantly correlated (r = 0.971; p < 0.001), and the mean [± SD] pH was 4.37 [± 0.14] (range, 4.20-4.68).
Mean (± SE) Levels of Caries-associated Microbiota as log10(colony-forming units +1) per mL of Saliva, Salivary Flow Rate [mL min-1], and Gingival and Periodontal Indices and Correlation Coefficients between Variables (***p ≤ 0.001; **p < 0.01; *p < 0.05)
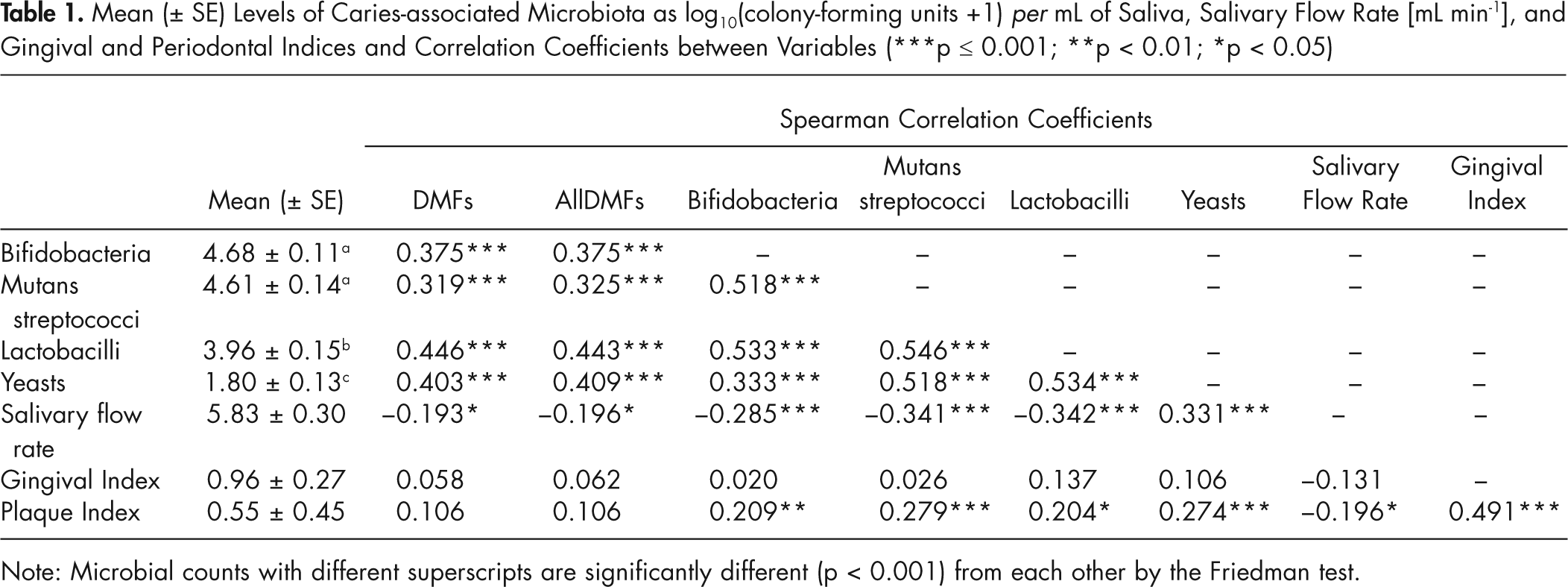
Note: Microbial counts with different superscripts are significantly different (p < 0.001) from each other by the Friedman test.
Participant gender did not significantly affect microbial counts, the salivary flow rate, or the clinical indices (Appendix), except for the decayed surface score, which was significantly (p = 0.048) greater in males (2.02 ± 0.59 and 0.73 ± 0.19, respectively). The mean PI and GI scores were 0.55 (± 0.04) and 0.96 (± 0.02), respectively, and were significantly correlated (r = 0.491). Salivary flow rate was negatively correlated with PI (r = −0.196; p = 0.014), but not GI, and the PI, but not GI, was significantly (p ≤ 0.01) correlated with each of the 4 microbial variables. Denture wearing was associated with significantly (p = 0.048) lower salivary flow rate (4.85 ± 0.40) for non-denture-wearers and 6.17 ± 0.38 for denture-wearers. Significantly (p ≤ 0.001) greater salivary levels of lactobacilli (3.51 ± 0.20 and 4.67 ± 0.20) and yeasts (1.39 ± 0.15 and 2.66 ± 0.24), but not Bifidobacteria or mutans streptococci, were found in denture-wearers. The presence of denture plaque was associated with significantly (p = 0.032) greater salivary levels of yeasts (2.37 ± 0.258 and 3.60 ± 0.44), but not lactobacilli, mutans streptococci, or Bifidobacteria.
The salivary levels of the 3 caries-associated taxa and the salivary Bifidobacteria levels were each tested as the dependent variable in the regression analyses (Table 2). The salivary levels of Bifidobacteria were significantly related to salivary flow rate and number of teeth (negative) and filled and decayed tooth surfaces (positive), and these variables were found to be associated with the salivary levels of lactobacilli and yeasts. For the mutans streptococci, the significant independent explanatory variables were salivary flow rate and GI (negative) and filled surfaces and PI (positive).
Significant Independent Variables Identified in Step-down Regression Analyses with Salivary Concentrations of Caries-associated Microbiota [as log10(colony-forming units +1) per mL of saliva], DMFs, and AllDMFs (DMFs plus rootDMFs) as Dependent Variables
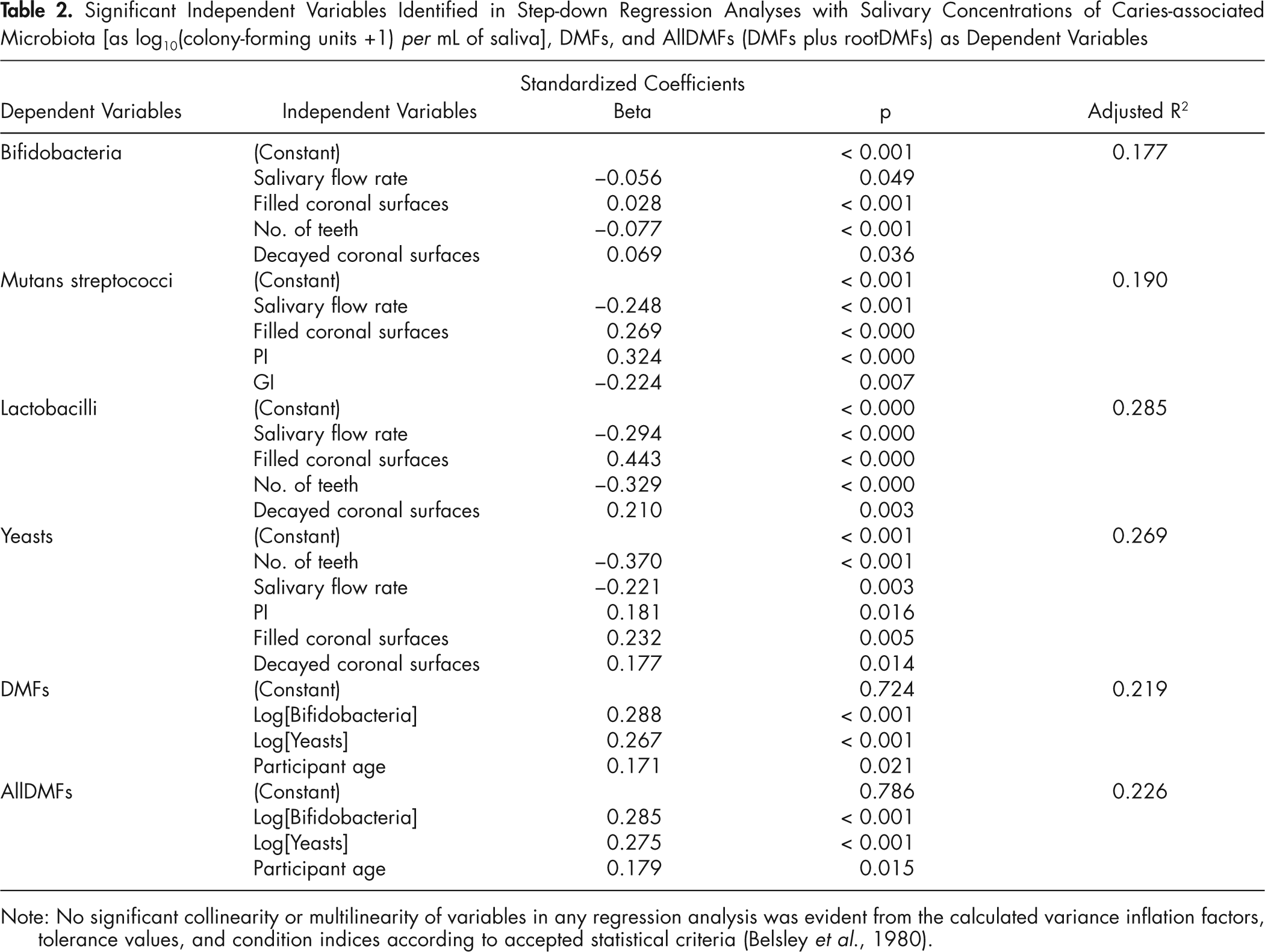
Note: No significant collinearity or multilinearity of variables in any regression analysis was evident from the calculated variance inflation factors, tolerance values, and condition indices according to accepted statistical criteria (Belsley et al., 1980).
The stepwise regression analyses indicated that salivary levels of Bifidobacteria, yeasts, and participant age were the independent variables significantly associated with the DMFs and AllDMFs scores (Table 2). When all variables were entered into the regression analysis simultaneously, a similar outcome was observed. For DMFs, the adjusted R2 value was 0.200 (p < 0.001), and only salivary levels of Bifidobacteria (p = 0.003), yeast (p = 0.011), and participant age (p = 0.031) were identified as significant dependent variables, while for AllDMFs, the adjusted R2 value was 0.205 (p < 0.001), and only salivary levels of Bifidobacteria (p = 0.003), yeast (p = 0.007), and participant age (p = 0.021) were identified as significant dependent variables.
Discussion
The oral microbiota is very diverse, with many hundreds of different species or phylotypes being identified by 16S rRNA sequencing, other species being identified by sequence comparison of other ‘housekeeping’ genes, and all species so far investigated showing evidence of multiple genotypes isolated from the majority of individuals. It is therefore impossible, with our present level of knowledge, to identify taxa causing dental caries, but, on the basis of the ecological plaque hypothesis, it should be possible to identify phenotypic characteristics required by organisms to proliferate in an oral environment conducive to caries initiation. They should be acidogenic and aciduric, characteristics of mutans streptococci, lactobacilli, and yeasts, associated with dental caries. Bifidobacteria are also aciduric and acidogenic (van Houte et al., 1996), but their ability to respond in the manner of these established caries-associated taxa has not been demonstrated. They have been only sporadically isolated from conventional non-selective culture media, but when isolated, they are often associated with carious dentin. Bifidobacteria have also been identified, by cloning methodologies, usually at low levels from infected dentin, but not in all studies.
Bifidobacteria have been isolated, in a novel selective medium (Rada and Petr, 2000), from the majority of elderly individuals, but with a cloning approach no Bifidobacteria were detected in the oral cavities of healthy individuals or among the microbiota of root caries lesions (Preza et al., 2008), which may be related to primer design (Frank et al., 2008), the resistance of Bifidobacteria to cell lysis, primer bias, or the problems involved in amplifying DNA with a high content of G+C (Marchesi et al., 1998). It is instructive that Becker et al. (2002), using a DNA-DNA hybridization checkerboard approach, which did not require DNA amplification, found that Bifidobacteria were significantly associated with dentinal caries in children and were present in lower numbers on sound enamel surfaces.
We have previously undertaken an analysis of the predominant cultivable microbiota of root caries lesions and found that Bifidobacteriaceae formed around 8% of the cultivable microbiota in root caries lesions in adults and occlusal lesions in children and adults (Mantzourani et al., 2009a,b), but were seldom recovered from sound tooth surfaces. This suggested to us that Bifidobacteria might, like mutans streptococci and lactobacilli, be caries-associated micro-organisms, and that evidence that they behave as other caries-associated micro-organisms in the ecological plaque hypothesis could be demonstrated. Here, we have found that the salivary levels of Bifidobacteria were significantly correlated with the salivary levels of the caries-associated taxa, were negatively associated with salivary flow rate, and were positively associated with the plaque score, as has been previously reported for these other taxa (Beighton et al., 1991; van Houte, 1993; Fure, 1998; Närhi et al., 1998). These relationships alone indicate that Bifidobacteria behave as the established caries-associated organisms. However, we have also demonstrated that, in this sample, the Bifidobacteria had a relationship with caries experience similar to those exhibited by mutans streptococci, lactobacilli, and yeasts in other subject groups, including the elderly (Beighton et al., 1991; van Houte, 1993; Fure, 1998; Närhi et al., 1998).
We also found that the salivary levels of Bifidobacteria, like lactobacilli and yeasts, were positively related to the filled and decayed surfaces of the participants and negatively associated with salivary flow rate and the number of teeth present, as was also found for the same 2 taxa. Bifidobacteria and mutans streptococci were each associated with salivary flow rate and filled surfaces, but, additionally, mutans streptococci were associated with the PI and GI scores.
We had expected that, with DMF and AllDMF used as dependent variables and the 4 taxa plus other explanatory variables used as predictors, all microbial taxa would have emerged as significant explanatory variables for caries experience. However, only salivary levels of Bifidobacteria and yeasts significantly explained variations in caries experience, while mutans streptococci and lactobacilli did not. A possible explanation for these unexpected results could be that the mutans streptococcus and lactobacillus coefficient estimates were artificially inflated by collinearity, although no significant collinearity or multilinearity of variables in any regression analysis was found. Alternatively, it may be that mutans streptococci and lactobacilli are not included in either model of DMFs or AllDMFs, since they do not add significantly to the model with the other microbial variables included.
The proliferation of Bifidobacteria in these participants would appear to be due to their ability to proliferate in oral environments conducive to the initiation and progression of dental caries, as would be predicted from the ecological plaque hypothesis. Since they are found primarily in active caries lesions (Becker et al., 2002; Mantzourani et al., 2009a,b), they may be involved in disease progression and not initiation.
In conclusion, analysis of these data indicates that, in adults 60 yrs old, salivary levels of Bifidobacteria were not significantly different from those of mutans streptococci, and they were isolated from almost all individuals. Further investigations are required to ascertain their role in the caries process, especially in persons in younger age groups, and to identify characteristics that enable them to proliferate in the oral cavity. It also remains to be determined if the salivary levels of Bifidobacteria can act as markers of caries risk at the individual level.
Footnotes
Acknowledgements
The authors acknowledge support from the Dunhill Medical Foundation, Dental Institute, King’s College London, and from the Department of Health via the National Institute for Health Research (NIHR) Comprehensive Biomedical Research Centre award to Guy’s & St Thomas’ NHS Foundation Trust in partnership with King’s College London and King’s College Hospital NHS Foundation Trust. We also thank one reviewer for bringing important aspects of the study to our attention, and Dr. Girvan Burnside for his expert statistical advice.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.