
Abstract
Few studies have examined, comprehensively and prospectively, determinants of oral-health-related quality of life. The aim of this study was to examine the relationships between psychosocial factors and oral health status, health perceptions, and quality of life. Measures of symptom and functional status, health perceptions, quality of life, oral health beliefs, and psychological (sense of coherence, self-esteem, health locus of control) and social factors (parents’ income and education) were collected from 439 12- and 13-year-olds at baseline and six-month follow-up, together with a clinical examination at baseline. Structural equation modeling indicated that increased levels of caries and more symptoms predicted more functional limitations, and, cross-sectionally, greater functional impact was associated with worse health perceptions, which were linked to lower quality of life. Sense of coherence was the most important psychosocial predictor. These factors are important in understanding how oral health affects young people’s daily lives.
Keywords
Introduction
Oral health quality of life (OHQoL) refers to the extent to which oral disorders disrupt an individual’s normal functioning. OHQoL is an important focus for assessment of the impact of oral conditions from the patient’s perspective in adults (e.g., Bekes et al., 2009) and children (e.g., Agou et al., 2008).
Nevertheless, understanding of the relationships between OHQoL and its determinants and consequences is incomplete. The Wilson and Cleary (1995) model conceptualizes the relationship between clinical factors and health-related quality of life (HRQoL) (see Appendix 1) in five main levels: biological variables, symptom status, functioning, general health perceptions, and overall quality of life (QoL). Relationships are hypothesized between adjacent levels (Appendix 1; Paths 1-4) along with complex, direct, and indirect (mediated) relationships between non-adjacent levels (e.g., Path 5). Moreover, individual and environmental factors may mediate these relationships (Paths 6-13).
Most examinations of this model have been broadly supportive, but have been cross-sectional and have not examined the model in its entirety (Baker et al., 2007, 2008). None has incorporated relevant individual and/or environmental factors identified in the health and psychology literature. Three individual factors that may protect health are sense of coherence, self-esteem, and health locus of control.
Sense of coherence is a generalized orientation that facilitates successful coping with stressors in daily living (Antonovsky, 1979). Strong sense of coherence is related to fewer symptoms and better self-rated health and QoL in adults and children (Eriksson and Lindstrom, 2007), and with regular dental attendance, fewer caries, more regular toothbrushing, and better OHQoL in adults (e.g., Ayo-Yusef et al., 2008).
Health locus of control refers to an individual’s belief in his/her ability to control his/her health (Wallston et al., 1987). A person with an internal health locus of control interprets health as dependent on his/her own abilities, whereas a person with an external health locus of control sees health as dependent on outside forces (e.g., a dentist). Health locus of control has been associated with several health behaviors and indicators (Steptoe and Wardle, 2001), including regular dental visits and less caries (Kneckt et al., 1999).
Self-esteem refers to one’s overall evaluation or appraisal of one’s own worth. Higher self-esteem is associated with life satisfaction, fewer health problems, more frequent toothbrushing and dental visits, and fewer oral health impacts in adolescents (e.g., Agou et al., 2008). In addition to these three generalized resources, oral health beliefs (e.g., avoiding sweet foods, visiting the dentist) are related to clinical status (e.g., caries), oral hygiene, and self-rated oral health across the lifespan (Broadbent et al., 2006).
Socio-economic status is an environmental contributor to HRQoL (income, occupation, education). A large body of evidence details its relationship with health (Marmot and Wilkinson, 2006), including clinical and patient-reported oral health outcomes in adults and adolescents (e.g., Donaldson et al., 2008).
The aim of this research was to examine comprehensively the role of psychosocial factors in adolescents’ oral health status, health perceptions, and quality-of-life outcomes according to the theoretical model of Wilson and Cleary (1995).
Materials & Methods
Participants
Participants were 439 12- and 13-year-olds (180 boys, 259 girls) from five schools in Banting district, Selangor, Malaysia.
Measures
The clinical and self-report measures chosen a priori to operationalize the model are described below and in Table 1. A more detailed description and operationalization of all measures can be found in Appendix 2. The questionnaires were translated into Malay by forward-backward translation techniques. Only minor discrepancies between the original and back-translated versions were found (Guillemin et al., 1993). These were discussed by two bilingual teachers and four bilingual students aged 12 to 14 yrs, and minor modifications were made before the questionnaire was tested in a pilot study.
Mean (SDs) and Sample Ranges for the Clinical and Self-report Measures at Baseline (T1) and Six-month Follow-up (T2)
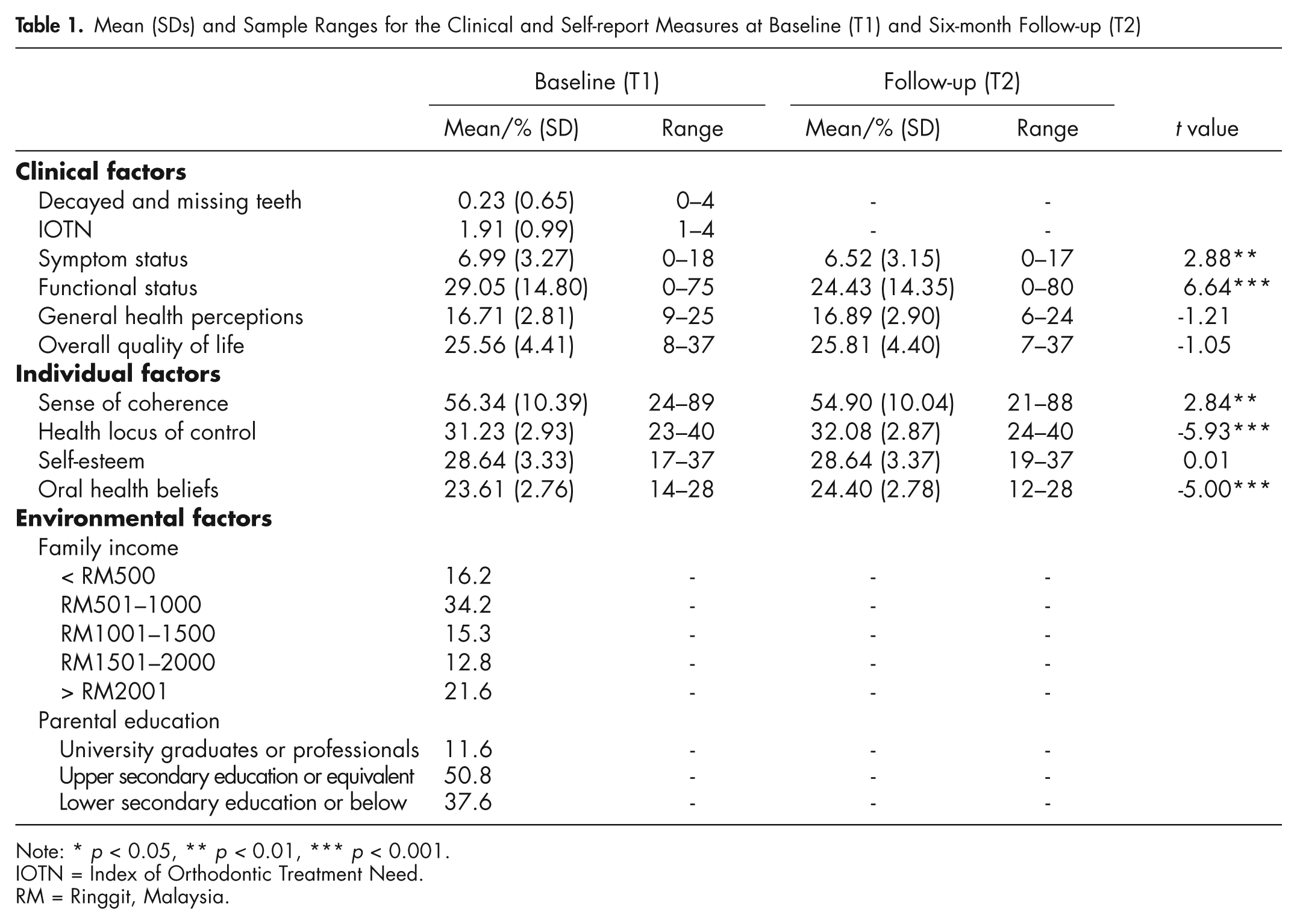
Note: * p < 0.05, ** p < 0.01, *** p < 0.001.
IOTN = Index of Orthodontic Treatment Need.
RM = Ringgit, Malaysia.
Clinical Factors
Clinical data [caries (number of decayed and missing teeth)] were collected at baseline according to WHO diagnostic criteria (1997) and the Index of Orthodontic Treatment Need (IOTN) (Brook and Shaw, 1989).
Symptoms and Functional Status
Symptoms and functional status data were collected by means of the child perceptions questionnaire (CPQ11–14) (Jokovic et al., 2002). The CPQ has 37 items about the frequency of events in relation to the child’s teeth, lips, jaw, or mouth. In the present analysis, the symptoms variable was comprised of the symptoms sub-scale from the CPQ11–14, while the functional status variable was comprised of the functioning, emotional, and social well-being sub-scales from the CPQ11–14. In both cases, higher scores indicate greater impacts.
General Health Perception
Perceived general health status was measured by 5 questions from the general health perceptions sub-scale of the SF36v2 (Ware et al., 2000). Participants rated, on a scale from 1 (definitely true) to 5 (definitely false), how much statements about their health are true for them. Higher scores indicate better health perceptions.
Overall Quality of Life
The Student Life Satisfaction Scale (SLSS) measured overall QoL (Huebner, 1991). Participants indicate their degree of agreement with 7 statements on a scale from 1 (strongly disagree) to 6 (strongly agree), with a higher score indicating greater satisfaction.
Environmental Factors
Environmental characteristics were defined as household income and education level.
Individual Factors
Sense of coherence was measured by the 13-item orientation-to-life questionnaire (Antonovsky, 1987) and self-esteem by Rosenberg’s (1965) 10-item scale, with higher scores indicating a greater sense of coherence and self-esteem. Health locus of control was measured by the children’s 20-item scale (Parcel and Meyer, 1978) to which the child answers ‘Yes’ (1) or ‘No’ (0). Higher scores indicate a greater external locus of control. Oral health beliefs were measured by Broadbent et al.’s (2006) battery of 6 items, with 1 additional item added to assess children’s beliefs about participating in the school dental program. All 7 items were scored on a scale from 1 (extremely important) to 4 (not at all important), with higher scores indicating more positive beliefs.
Procedure
Multistage probability sampling first sampled 5 of the 16 secondary schools in Banting district. Based on a power calculation of 20 participants per variable to detect a difference with 95% power at p < 0.05, a sample of 300 was required. Assuming a 25% loss to follow-up, and a 75% recruitment rate, 453 12- and 13-year-olds were randomly selected, and their parents/guardians were approached with information leaflets. Only children who returned the consent form and the parental questionnaire were recruited (96.9%). Ethical approval was obtained from the University of Sheffield and the Economic Planning Unit, Government of Malaysia.
Participants completed all questionnaires at baseline (T1) and at six-month follow-up (T2). At baseline, children were also clinically examined, and their parents/guardians provided demographic data.
Analysis
Structural equation modeling is a powerful technique that allows for simultaneous testing of complex interrelationships between variables specified within a priori models (Kline, 2005). It was used to assess whether the Wilson and Cleary model was an acceptable fit to the data, specifically testing the relationships hypothesized within the model in lagged analyses; that is, baseline (T1) variables were used to predict follow-up (T2) scores.
We used AMOS 7.0 and maximum likelihood estimation. We assessed mediation by testing the significance of the indirect effect using the bias-corrected bootstrap confidence intervals (MacKinnon et al., 2002). Model fit was evaluated according to indices from the 3 fit classes: absolute fit [χ2/df ratio; standardized root mean squared residual (SRMR)], parsimony adjusted [root-mean-squared error of approximation (RMSEA) with 90% confidence intervals (90% CI)], and comparative [Tucker-Lewis index (TLI); comparative fit index (CFI)] (Hu and Bentler, 1999). A χ2/df ratio < 3.0, RMSEA values < .08, CFI and TLI of 0.90 or above, and an SRMR < 0.08 were taken to indicate an acceptable model fit (Hu and Bentler, 1999).
Results
Participant demographics are presented in Table 1, which indicates that they were healthy; disease and treatment-need levels (mean decayed and missing teeth = 0.23; IOTN = 1.91) and self-reported symptom and functional impacts were low.
In relation to the hypothesized structural equation model, the basic model (Model 1) did not immediately fit any of the indices [χ2/df = 9.784, SRMR = 0.0908, CFI = 0.714, RMSEA = 0.142 (90% CIs 0.128-0.155)]. The modification indices indicated that allowing (i) sense of coherence and self-esteem and (ii) income and education to correlate would help model fit. Since sense of coherence and self-esteem are similar constructs and family income is related to parental education, the model was re-run with these covariances. Model 2 was a good fit [χ2/df = 2.762, SRMR = 0.0515, CFI = 0.946, RMSEA = 0.063 (90% CIs 0.048-0.079)]. The difference between Models 1 and 2 was significant [Δχ2 (2) = 7.02, p < 0.05]. To create a statistically parsimonious model, all non-significant paths were deleted [Model 3; χ2/df = 2.041, SRMR = 0.0585, CFI = 0.949, RMSEA = 0.049 (90% CIs 0.036-0.062)]. Models 2 and 3 were not significantly different from one another [Δχ2 (20) = 0.72, ns]. Thus, Model 3 was a better fit (see Fig.), accounting for 6%, 38%, 8%, and 11% of the variance in symptoms, functional status, general health perceptions, and quality of life at follow-up. [The model was also run with IOTN as the clinical variable. There was no significant difference in model fit between IOTN and decayed and missing teeth.]
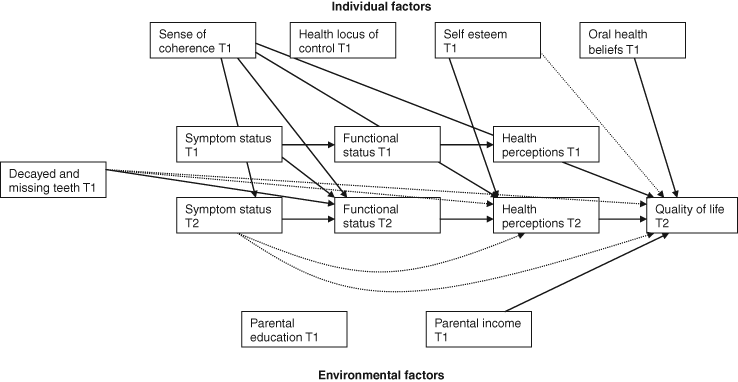
Significant direct and indirect effects for the final statistically parsimonious Wilson and Cleary model. Solid lines = direct effect; dashed line = indirect effect. For bootstrapped standardized estimates, see Tables 2 and 3. Error terms and covariances omitted for ease of interpretation. T1 = baseline; T2 = six-month follow-up.
Direct Effects
Only two of the main paths within the model were prospectively significant (Table 2); more decayed and missing teeth and more symptoms predicted greater functional impact, but not symptom status. The remaining two paths—functioning to general health perceptions and general health perceptions to quality of life—were significant only when tested cross-sectionally. Among the psychosocial factors, stronger sense of coherence predicted fewer symptoms, better functioning, greater health perceptions, and a better QoL. Higher self-esteem predicted better general health perceptions. Higher family income and more positive oral health beliefs predicted better QoL.
Significant Direct Effects for the Wilson and Cleary Model
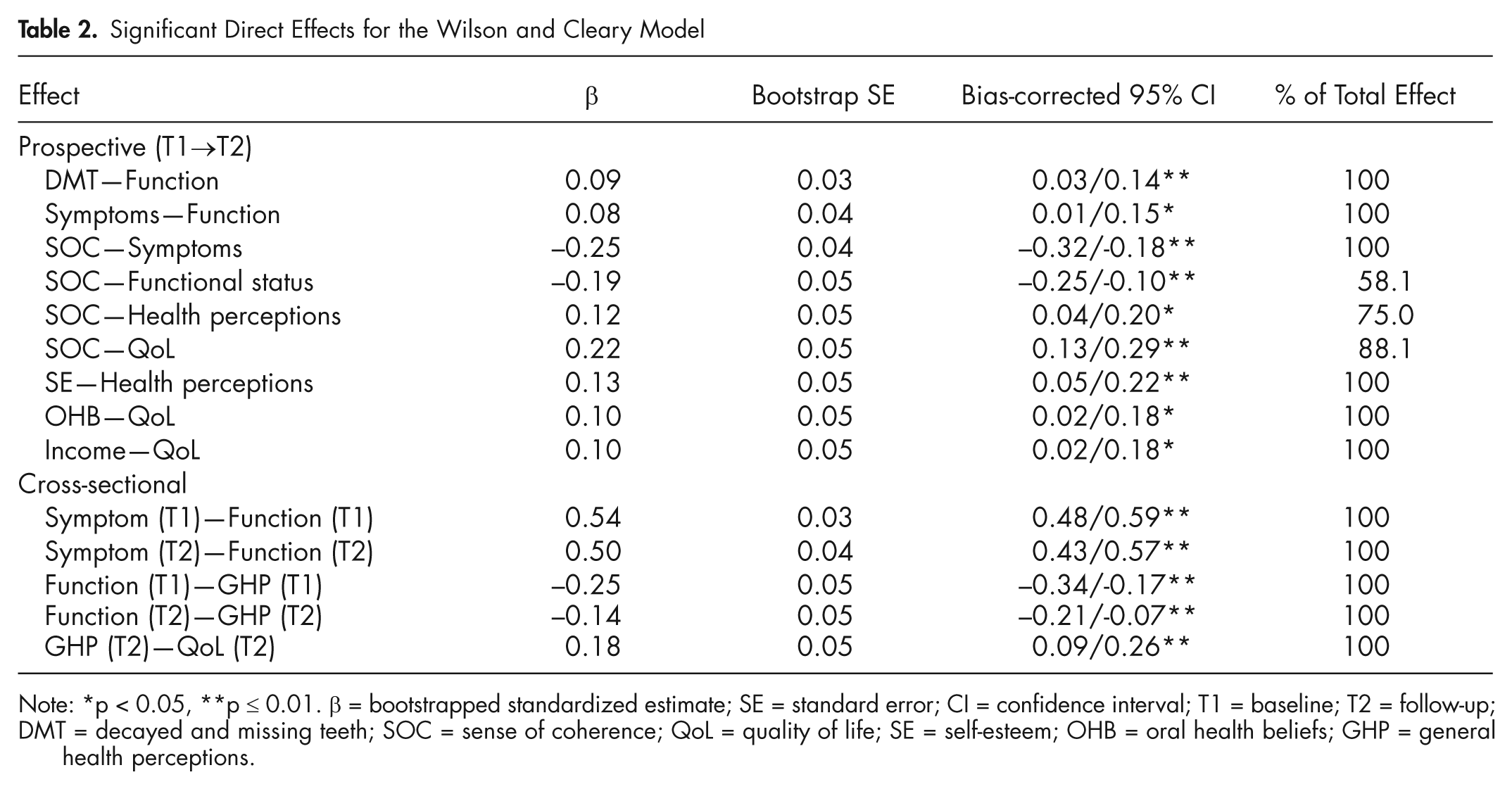
Note: *p < 0.05, **p ≤ 0.01. β = bootstrapped standardized estimate; SE = standard error; CI = confidence interval; T1 = baseline; T2 = follow-up;
DMT = decayed and missing teeth; SOC = sense of coherence; QoL = quality of life; SE = self-esteem; OHB = oral health beliefs; GHP = general health perceptions.
Indirect Effects
Significant prospective indirect effects (Table 3) included a link from more decayed and missing teeth via functioning to worse general health perceptions and lower QoL. Worse symptom status was linked via functioning to poorer health perceptions and lower QoL. Greater sense of coherence predicted better functioning, positive health perceptions, and higher QoL via better symptom status. Finally, higher self-esteem was linked to better QoL via better health perceptions.
Significant Total Indirect Effects for the Wilson and Cleary Model
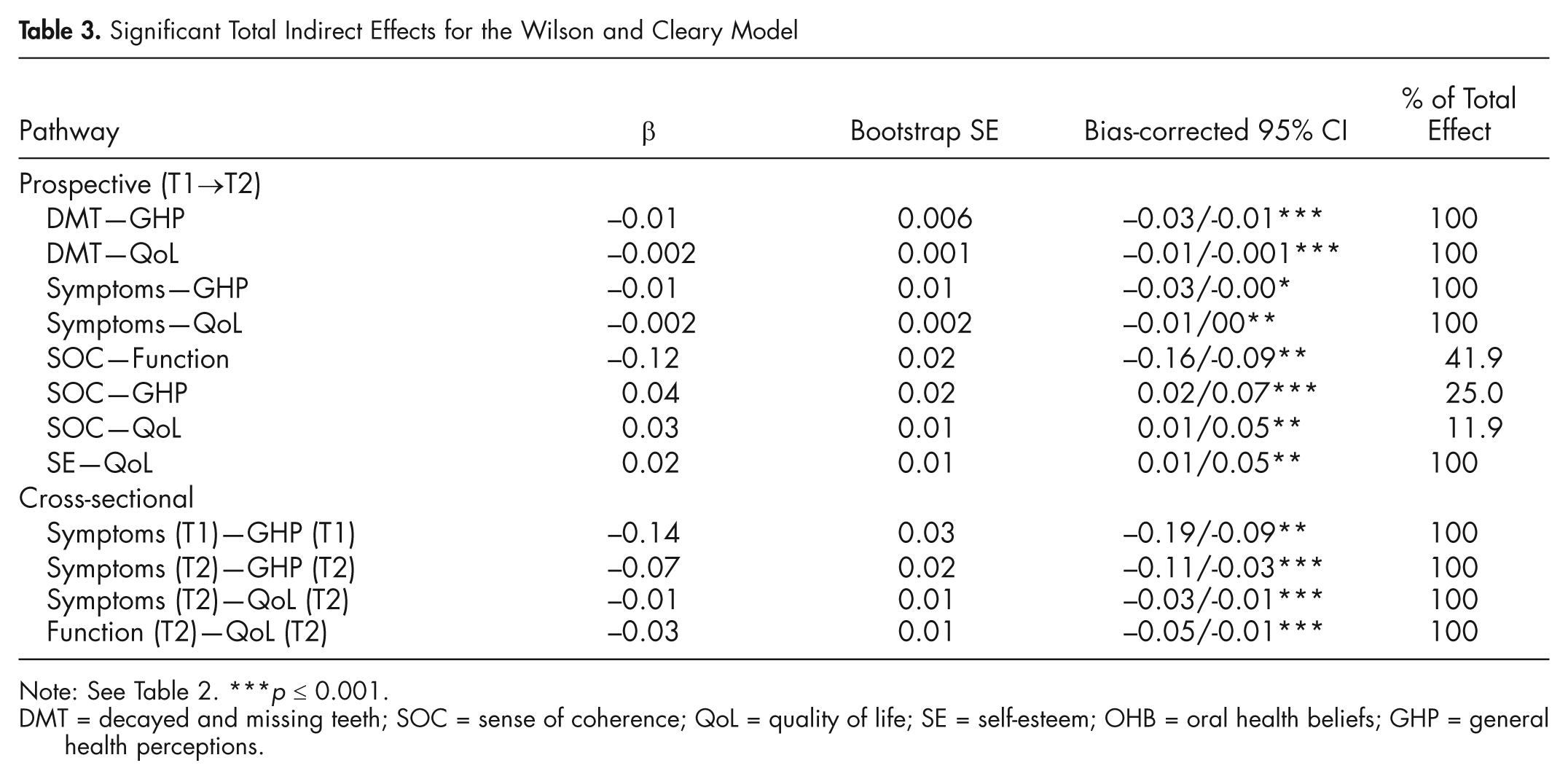
Note: See Table 2. ***p ≤ 0.001.
DMT = decayed and missing teeth; SOC = sense of coherence; QoL = quality of life; SE = self-esteem; OHB = oral health beliefs; GHP = general health perceptions.
Discussion
Analysis of these data lends broad support to Wilson and Cleary’s (1995) model and further implicates psychosocial factors in oral health impacts on young people’s daily living, health perceptions, and overall quality of life. As such, they support previous studies in adults (e.g., Baker et al., 2007, 2008).
The pathways among clinical status, health perceptions, and quality of life were indirect; for example, adolescents with more caries reported worse quality of life, but this was dependent on functional status (e.g., being called names) and health perceptions (e.g., expectation of poor health). These findings highlight the complex relationships between clinical and patient-reported outcomes and have several implications. First, modeling indirect effects may help reconcile why observations between clinical and subjective assessments have generally been weak (e.g., Marshman et al., 2005). Second, they re-emphasize the importance of patient-reported outcomes being routinely assessed in research and clinical practice (Valderas and Alonso, 2008). Moreover, interventions that are solely clinical, which do not take into account patient experiences, may not be fully effective.
Psychosocial factors helped explain the impact of oral health on well-being. Sense of coherence consistently predicted subjective assessments. Having a greater sense of coherence—that is, perceiving the world as comprehensible, meaningful, and manageable—predicted fewer symptoms, functional impacts, and better health perceptions and quality of life. Such findings support Antonovsky’s (1979) salutogenic theory and previous studies with both adults and children (Eriksson and Lindstrom, 2007). It may be that sense of coherence influences wider health via changes in oral health behaviors, as suggested recently (e.g., Ayo-Yusuf et al., 2008; Bernabe et al., 2009).
Parental income predicted adolescents’ quality of life, but was not linked to symptoms, functional limitations, or general health perceptions. The effect of income on, for example, health perceptions may be indirect via adolescents’ psychological resources (e.g., sense of coherence or self-esteem) (see Taylor et al., 1997). Previous research supports this explanation; for example, higher socio-economic profile has been linked to greater sense of coherence (e.g., Lundberg and Nyström Peck, 1994), and sense of coherence mediated a relationship between childhood socio-economic profile and adult oral health behaviors (Bernabe et al., 2009).
This is the first a priori and longitudinal investigation of adolescents’ oral health outcomes using a theoretical model. The findings support the Wilson and Cleary model as a conceptual framework for classifying patient-reported outcomes and delineating key pathways underpinning adolescents’ everyday experiences of oral health (Valderas and Alonso, 2008). However, we tested only one possible model with only one sample. Although the model was an acceptable fit to the data, the low percentage of variance explained, particularly in symptoms (6%) and health perceptions (8%), suggests that important variables were omitted (Tomarken and Waller, 2003). Additionally, alternative models may fit the data equally well or better (Bollen, 1989). The present model and possible alternatives should be cross-validated in other settings with differing dental service provisions and health states, especially given the low disease level [mean DMFT = 0.499 (SD = 0.955)] in this sample.
Nevertheless, theoretically driven research facilitates understanding of the processes underlying experiences of oral health and well-being and highlights potential points for intervention. Here, caries had only an indirect impact on individuals’ quality of life. Strategies to promote young people’s oral health might better target psychological/social well-being (e.g., embarrassment, teasing), alongside sense of coherence, as has been advocated in recent health promotion initiatives (Eriksson and Lindstrom, 2008).
From another perspective, Swann et al. (2007) suggested that, in longitudinal studies of health outcomes with multiple predictors, a correlation of 0.30 approaches the limit of detection between a predictor and the outcome variable. An association of 0.03 between aspirin and reductions in heart attacks led to recommendations for at-risk patients to take aspirin daily. The magnitude of the relationships between sense of coherence and the outcomes in the present study (betas = 0.12-0.25) indicate that enhancing sense of coherence may be an important “psychological flu shot” for longer-term inoculation against oral ill health.
Footnotes
This study was funded by the Oral Health Division, Ministry of Health in Malaysia via a doctoral studentship to Amdah Mat.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.