
Abstract
The effects of pulpal inflammation on the sensitivity of dentin to cold (5°C) and negative hydrostatic pressure (−300 mm Hg) stimuli in man were compared, since recent evidence suggests that these stimuli excite different classes of sensory receptors. Dentin was exposed in premolars in 14 participants aged 15-25 years. Stimuli were applied to etched dentin immediately after cavity preparation and after the cavity had been filled with gutta percha for 7 days. This treatment increased significantly the intensity of pain produced by cold, and at the same time decreased that evoked by negative pressure stimuli. Pulpal blood flow was increased in the treated teeth, indicating that their pulps were inflamed. It is concluded that the sensory receptors responsible for the response to cold were probably sensitive to some change other than an outward flow of fluid in dentinal tubules, which would be caused by both forms of stimulus.
Introduction
Much of the available evidence indicates that all of the different forms of stimulus that produce pain when they are applied to enamel or dentin generate impulses in intradental nerves via a common sensory transduction mechanism (the hydrodynamic mechanism) that detects movement of the contents of the dentinal tubules through hydrodynamic receptors (Brännström, 1963; Pashley, 1990; Andrew and Matthews, 2000; Orchardson and Cadden, 2001; Vongsavan and Matthews, 2007). However, recent experiments (Chidchuangchai et al., 2007) indicate that pain caused by cold stimulation of dentin in man may not always involve hydrodynamic receptors. It was found that etching freshly exposed dentin increased its sensitivity to cold, but decreased the fluid flow through the dentin that was caused by a cold stimulus. Furthermore, oxalate treatment, which re-occluded the tubules of the etched dentin, decreased the sensitivity of the dentin to cold but increased the dentinal fluid flow that was produced by a cold stimulus.
We carried out the present experiments to determine the effects of pulpal inflammation on the sensitivity of dentin to cold and to sub-atmospheric (negative) hydrostatic pressure stimulation of exposed, etched dentin in man. Cold stimuli cause outward flow of fluid through dentin (Andrew and Matthews, 2000), as does the application of negative hydrostatic pressure stimuli. The latter have been used previously to activate hydrodynamic receptors in teeth (Andrew and Matthews, 2000; Vongsavan and Matthews, 2007; Charoenlarp et al., 2007).
We induced pulpal inflammation by filling the teeth with gutta percha for 1 wk (Anderson et al., 1958). Clinical experience indicates that carious teeth with inflamed pulps may be very sensitive to cold.
Materials & Methods
The experiments were carried out on 14 pairs of healthy premolars in 14 human participants (mean age, 20.5 yrs; range, 15-25 yrs). All teeth were scheduled to be extracted for orthodontic purposes. Radiographic and clinical examinations confirmed that all teeth were fully erupted, vital, free of caries, and without restorations.
The experiments were carried out in the Advanced Clinic, Faculty of Dentistry, Mahidol University. The study was approved by the Ethics Committee on the Use of Human Rights Related to Human Experimentation of the Mahidol University and complied with the principles of the Declaration of Helsinki. An informed consent was obtained from each participant or, for those under 18 yrs of age, from a parent or guardian.
Experimental Design
In each participant, 2 upper or 2 lower premolars were used, 1 on each side. Both hydrostatic pressure and cold stimuli were applied to 1 of the 2 teeth (Pressure and Cold Group), which was selected at random; only cold stimuli were applied to the other (Cold Only Group).
On Day 0, a cavity was prepared in each of the pair of teeth, both cavities were etched, and the test stimuli were applied. Gutta percha temporary fillings were then placed in the teeth for 1 wk. On Day 7, the temporary fillings were removed, and the teeth were again tested as before. At the end of the experiment, the teeth were extracted under local anesthesia (2% lidocaine HCl with 1:100,000 epinephrine).
Tooth Preparation
The preparation was the same as used in previous experiments (Ajcharanukul et al., 2007). Without local anesthesia, dentin was exposed at the tip of the buccal cusp by the cutting of a small cylindrical cavity (approximately 3 mm in diameter and 3 mm in depth) with diamond burs (No. 201, round and No. 204, cylindrical; Intensive®, Viganello-Lugano, Switzerland) in an air-rotor handpiece under a constant stream of water. The smear layer was removed from the exposed dentin by 30 sec of etching with 35% phosphoric acid, after which the dentin was rinsed with water for 1 min. A stainless steel tube (needle gauge 14: o.d. 2.11 mm, i.d. 1.56 mm; length 5 mm), which was used to apply stimuli, was sealed into the cavity with composite resin. Between stimuli, the tube was filled with normal saline at room temperature. The tube was removed by being rotated in the cavity before the gutta percha temporary filling was inserted on Day 0, and replaced after the filling was removed on Day 7. The dentin was not re-etched on Day 7.
Test Stimuli
We applied the hydrostatic pressure stimulus by connecting a manometer preset at 300 mm Hg below atmospheric to the stainless steel tube attached to the tooth for 5 sec. This negative pressure stimulus was selected because, in a previous study, it evoked pain reliably (Charoenlarp et al., 2007).
We applied the cold stimulus by injecting normal saline at 5°C from a syringe into the stainless steel tube for 5 sec, while removing the overflow by suction. A 5°C stimulus was chosen rather than the 0°C used previously (Chidchuangchai et al., 2007), because in the earlier experiments the 0°C stimulus evoked a near-maximum response in some teeth when it was applied to freshly exposed, etched dentin, and we wished to be in a position to record an increase in the response to cold stimuli after the induction of pulpal inflammation. The cavity was dried with a cotton pellet before the cold stimulus was applied.
After each stimulus, the participant indicated the intensity of any pain produced by placing a mark on a simple visual analogue scale calibrated from 0 (no sensation) to 100 mm (the most severe pain one can imagine) (Holland et al., 1997).
Pulpal Blood Flow
Pulpal blood flow was recorded with a Moor Type MBF3D/42 blood flow monitor (Moor Instruments, Axminster, England). During recording, an opaque black rubber dam (Four D Rubber Co. Ltd., Heanor, England) was applied to the tooth to reduce to a minimum the contribution of blood flow in tissues outside the tooth (Soo-Ampon et al., 2003). The probe of the instrument (o.d. 1.5 mm) contains two 0.2-mm-diameter optical fibers with their centers separated by 0.5 mm. The probe was fixed to the tooth with a clip-on splint. The splint was constructed from self-curing acrylic resin on a plaster model of the tooth. The probe tip was supported on the tooth surface by a short length of stainless steel tube (i.d. 1.5 mm) that was incorporated into the splint. The tube was positioned so that it was perpendicular to the enamel surface, with its center 2 mm from gingival margin and over the central long axis of the crown of the tooth. We kept the rotation of the probe around its long axis within the tube constant between trials by aligning marks on the probe and tube. This precaution was necessary to ensure that reproducible results were obtained under each of the experimental conditions.
The flux signal from the blood flow monitor was transferred to a computer and analyzed with the Moorsoft program (Moor Instruments, Axminster, England). The sensitivity of blood flow signal was standardized as described previously, and recordings were made with an upper bandwidth setting of 14.9 kHz and a time constant of 0.1 sec. Blood flow was measured in arbitrary perfusion units (Vongsavan and Matthews, 1993).
Control recordings of pulpal blood flow were made from both teeth on Day 0 approximately 5 min after cavity preparation but before the stainless steel tube was inserted for stimulation. The recording was repeated after stimulation, approximately 5 min after the tube was removed, and at the corresponding stages before and after stimulation on Day 7. During the recordings on each occasion, the cavity was filled with saline, and the mean pulpal blood flow signal was determined over a period of 1 min.
Statistical Analysis
The pain and blood flow data are summarized as box-plots in Figs. 1 and 3. Each box represents the median (a line through its center) and the 25th and 75th percentiles. Whiskers above and below the box indicate the 90th and 10th percentiles. The significance of changes in the pain scores following gutta percha treatment was determined by comparison of corresponding median pain scores with the non-parametric Wilcoxon Signed Rank Test for paired data. This test was used in preference to a parametric test, because the pain data, although satisfying tests of normality, were not drawn from a continuous distribution. The pulpal blood flow data were not normally distributed, and the effects of the different stimuli and of gutta percha treatment on blood flow were also analyzed by the Wilcoxon Signed Rank Test. P values of less than 0.05 were considered significant.
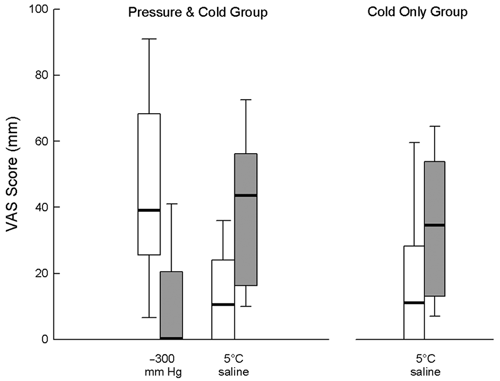
Pain scores recorded after the application of cold (5°C normal saline) and sub-atmospheric hydrostatic pressure (−300 mm Hg) stimuli to both groups of teeth in 14 participants on Day 0 (open boxes) and on Day 7, after gutta percha treatment (shaded boxes). The line through the center of each box indicates the median and the lower and upper limits of the box, the 25th and 75th percentiles, respectively. The bars below and above each box indicate the 10th and 90th percentiles.
Results
The VAS pain scores obtained from stimulation of both groups of teeth, before and after gutta percha treatment, are summarized in Fig. 1. In the Pressure and Cold Group, the median pain score recorded in response to the −300 mm Hg hydrostatic pressure stimulus decreased significantly from 39 mm (range, 0-98) to 0 mm (range 0-50) between Days 0 and 7 (p = 0.001, Signed Rank Test, n = 14). Over the same period and in the same teeth, the median pain score in response to the 5°C stimulus increased significantly from 10.5 mm (range, 0-42) to 43.5 mm (range, 8-82), (p < 0.001, n = 14). In the Cold Only Group, the median pain score evoked by the 5°C stimulus increased significantly from 11 mm (range, 0-67) on Day 0 to 34.5 mm (range, 4-66) on Day 7 (p = 0.017, n = 14).
Examples of the blood flow records obtained from both teeth in one participant before and after stimulation, both before and after gutta percha treatment, are shown in Fig. 2.
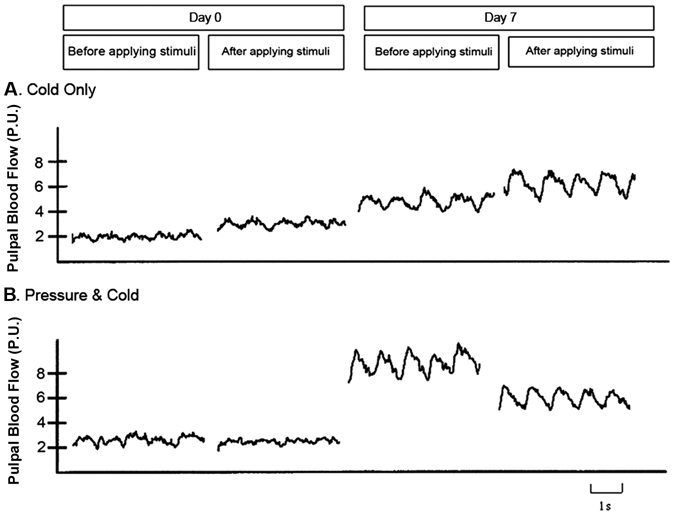
Records of pulpal blood flow from teeth tested with pressure and cold stimuli
The pulpal blood flow values recorded from both groups of teeth, before and after gutta percha treatment, are summarized in Fig. 3. In this Fig., we normalized the data by expressing the values recorded after stimulation on Day 0, and those recorded both before and after stimulation on Day 7, as percentages of the corresponding control value obtained before stimulation on Day 0. Considering the raw data, pulpal blood flow increased significantly between Days 0 and 7, but stimulation produced no significant change on Day 0 or on Day 7 in either group. In the pooled data from both groups, the median value on Day 0 was 1.6 (range, 0.1-68) perfusion units, and this increased to 2.7 (range, 0.5-111) perfusion units on Day 7 (p < 0.001, Wilcoxon Signed Rank Test, n = 56).
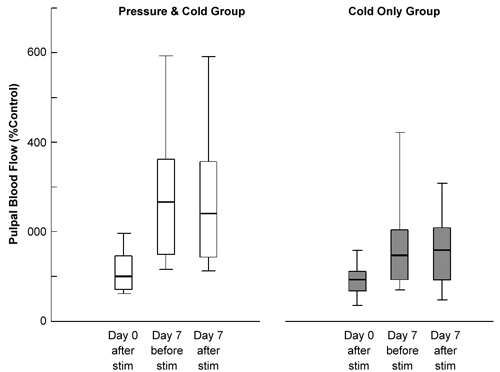
Values of the pulpal blood flow signal recorded from both groups of teeth in 14 participants on Day 0, and on Day 7 after gutta percha treatment. We normalized the data by expressing the values recorded after stimulation on Day 0, and those recorded both before and after stimulation on Day 7, as percentages of the corresponding control value obtained before stimulation on Day 0. Each box shows the median and the 10th, 25th, 75th, and 90th percentiles, as in Fig.1.
Discussion
This study has shown that gutta percha treatment increases the sensitivity of human dentin to cold stimuli at the same time as it decreases its sensitivity to negative hydrostatic pressure stimuli. The increase in the response to cold in the Pressure and Cold Group was not due to an effect of the preceding hydrostatic pressure stimulus, since the same effect was seen in the Cold Only Group.
Since both the cold and negative pressure stimuli would have caused outward flow through the dentin, these observations provide further evidence that the pain produced by cold stimuli in man is not due to hydrodynamic receptors, but to some other type, such as specific cold receptors (Chidchuangchai et al., 2007). Naylor (1963) showed that the reaction times to cold stimulation of dentin in man were too short to be due to activation of cold-sensitive receptors at the pulp-dentin junction. The involvement of hydrodynamic receptors at the pulp-dentin junction could account for this short latency, but the proposed specific cold receptors would have to be located more peripherally, in the dentinal tubules. Since nerve terminals are confined to the inner 100 µm of the dentin (Lilja, 1979; Holland et al., 1987), this raises the possibility that the odontoblasts, with cold-sensitive membrane ion channels, may be involved in the sensory transduction mechanism (Magloire et al., 2009). However, Son et al. (2009) found no evidence that the specific cold receptors TRPM8 and TRPA1 were expressed in odontoblasts in neonatal mouse incisors.
The gutta percha treatment also produced a significant increase in pulpal blood flow. This can be attributed to inflammation of the pulp, which is known to occur under this type of filling (James et al., 1954; Massler, 1956). An increase in pulpal blood flow, with histological evidence of inflammation, has been observed previously with preparations similar to that used in the present experiments (Veerayutthwilai, 2001).
Although the test stimuli evoked pain, they did not produce any significant increase in pulpal blood flow. This lack of evidence for neurogenic inflammation may be because only the large-diameter pulpal afferents were stimulated (Andrew and Matthews, 2002), or, in the gutta-percha-treated teeth, because the blood flow had already increased maximally. Also, a transient increase in blood flow may have been missed due to the delay of ca. 5 min while the laser Doppler recording system was set up after the stimulation was completed.
There are several possible explanations for the changes in dentin sensitivity observed following gutta percha treatment. For example, the increase in response to cold may have been due either to an increase in the sensitivity of the sensory receptors in the teeth (peripheral sensitization) or to changes in the pain pathways in the brain that are activated by the discharge evoked in the primary afferent nerve fibers (central sensitization). An increased sensitivity of pulpal afferents to cold following exposure of the dentin for 1 wk has been reported in the dog (Hirvonen et al., 1992), although, in other studies in experimental animals, little evidence was found of peripheral sensitization in inflamed teeth (Andrew, Sirimaharaj, and Matthews, unpublished observations). The decrease in response to a negative pressure stimulus we observed could have been due to a decrease in hydraulic conductance of the dentin, resulting in less flow through dentinal tubules and a reduced response from hydrodynamic receptors. Such a change might result from the polymerization of fibrinogen that leaked into the tubular fluid from the pulp (Pashley et al., 1984). If there was a decrease in conductance that was confined to the peripheral ends of the tubules, the outward flow produced at the pulpal ends of the tubules by the application of a cold stimulus to the cavity may have been increased compared with that in freshly exposed dentin (see Chidchuangchai et al., 2007). This is a possible alternative explanation for the observed difference in the effects of gutta percha treatment on responses to negative pressure and cold stimuli.
Evidence for central sensitization in trigeminal nociceptive pathways has been obtained in experimental animals (Sessle, 2000). Also, Veerayutthwilai et al. (2002) showed that the sensory thresholds to electrical stimulation of tooth pulp in human participants were decreased following gutta percha treatment, an effect that is likely to have been due to central sensitization.
Our finding that gutta percha treatment reduced the sensitivity of dentin to negative pressure stimuli appears to contradict the results of Anderson and Matthews (1967), who showed that the same treatment increased the sensitivity of dentin to osmotic stimuli. However, in those experiments no allowance was made for a smear layer. A smear layer would have been present on the exposed dentin surface immediately after cavity preparation, and this may have been etched away during the ensuing week by acids that accumulated under the leaky gutta percha filling. Removal of the smear layer in this way could account for the observed increase in sensitivity of the dentin. No data are available on the effects of smear layer removal on the sensitivity of dentin to osmotic stimuli.
Footnotes
Acknowledgements
This study was supported by The Thailand Research Fund and The Faculty of Dentistry, Mahidol University.