
Abstract
Initial therapies for HIV infection comprised nucleoside analogues, but as single or dual agents, they failed to prevent disease progression. When a new class of drug was introduced, the protease inhibitors, an effective triple therapy became possible—namely, highly active antiretroviral therapy, or HAART. HAART reduced viral replication almost completely and enabled immune system recovery. The probability of classical infections and tumors attributed to HIV were dramatically reduced, and life expectancy correspondingly increased. The initial disadvantages of HAART included the need for strict adherence to prevent drug resistance, the cost that initially precluded their widespread use in the developing world, and the short- and long-term side effects. One of the most disabling long-term complications was HIV lipodystrophy, which in extreme cases lead to severe peripheral fat wasting and central fat gain. In recent years, many of these disadvantages have been addressed: Once-daily drug combinations improve adherence; global access to HAART has been markedly improved; and new drugs enable patients to avoid many of the initial side effects. Future research will determine at what CD4 count HAART should be initiated, and new approaches such as immunotherapeutic HIV vaccines are being tested with the aim to delay or obviate the need for antiretroviral drugs.
AIDS was first recognized in 1981, but for several years, there were no effective therapies to moderate the course of the disease. The median survival from the diagnosis of AIDS was just over 12 months (Peters et al., 1991a). The typical natural history of the patient with AIDS in this era was one of progressive disease attributed to debilitating opportunistic infections or tumors. For example, approximately one-third of patients with HIV got cytomegalovirus disease and, in 70% of these, retinitis, which threatened the patient with blindness (Peters et al., 1991b). Patients with advanced-stage HIV disease had a poor prognosis; they were entering or soon entered a stage of palliative care.
The first drug found to have an effect on HIV viral replication was AZT (zidovudine), and it was widely introduced into clinical practice from 1988. In the first trial of AZT, mortality was reduced in those who were randomized to receive the drug (Fischl et al., 1987). However, patients were observed for only 8 to 24 weeks, although some other studies also found benefit. AZT is a nucleoside reverse transcriptase inhibitor that blocks the conversion of viral RNA to DNA, which is otherwise integrated into the host genome. The news that there was a treatment for HIV engendered hope and activism for its immediate and widespread use in equal measure. Although AZT appeared to convey some initial clinical benefit, the effects were short-lived. A large international multicenter study, the Concorde trial, demonstrated that zidovudine monotherapy made no effect to long-term outcome from HIV (Concorde Coordinating Committee, 1994) because the HIV virus rapidly develops resistance to one drug, owing to its extremely high rate of mutagenesis. A similar principle governs the need for 3 drugs for tuberculosis therapy.
Without a specific anti-HIV therapy, the only approaches that had any effect were prophylaxis to prevent infectious conditions—particularly, PCP or toxoplasmosis—or treatments for the opportunistic infections and tumors (Peters et al., 1991b). Prophylactic antibiotics such as cotrimoxazole were given to prevent PCP and toxoplasmosis when the CD4 count fell (< 200 cells/mm3), and they helped reduce mortality in the short term. All management strategies during this era were, however, just a holding approach. Once someone presented with advanced-stage HIV disease or AIDS, the prognosis for survival was measured in months. In an attempt to develop effective chemotherapy against HIV, new drugs were developed from the reverse transcriptase inhibitor class. Trials began using combinations of 2 nucleoside reverse transcriptase inhibitors. There was little extra benefit when 2 drugs were used in combination (Delta Co-ordinating Committee, 1996).
The Era of Effective Therapy for HIV
It was only when 3 drugs were used that real benefit on outcomes were observed. In the mid-1990s, triple-combination therapy was found to be truly effective against HIV infection. The initial combinations comprised one protease inhibitor and two nucleoside reverse transcriptase inhibitors. The benefits of this therapy were profound. Most patients responded clinically, even many of those who had entered “terminal decline.” Moreover, provided that the patients adhered to their treatment, the clinical benefits frequently persisted for many years, even decades. The advantages of triple combination therapy for HIV—or HAART (highly active antiretroviral therapy), as it became known—led to a period of unalloyed optimism. The benefits were real and often sustained, but the honeymoon period soon gave way to a realization that HAART was associated with problems. The disadvantages of HAART included the need to adhere to complicated regimens of pills, the problem of drug resistance, side effects of the medication, drug interactions with one another as well as non-HAART drugs, and the cost of treatment.
Hence, realization soon dawned that the marriage of anti-HIV drugs and patients who relied on them for their survival was far from perfect. The initial HAART combinations required that the pills be taken several times a day. Depending on the regimen, patients might have to take up to 20 pills each 24-hour period, some with food, some on an empty stomach, and many of them large and, hence, a challenge to swallow. Furthermore, it was essential that patients took their medications with near-perfect adherence (Fig. 1). Even missing as little as 1 dose a week drastically increased the chance of failing that regimen.
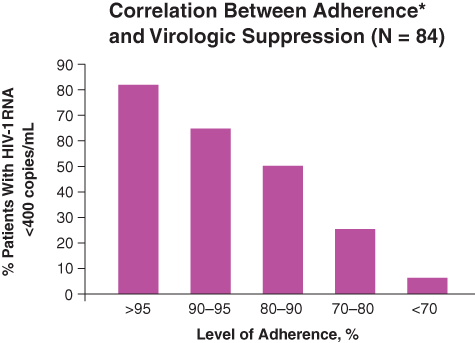
The importance of adherence to HAART.
As we have seen, because HIV mutates so rapidly, it usually requires at least 3 drugs taken according to protocol to avoid drug resistance. If the level of 1 or more anti-HIV drugs fall—because of poor adherence, poor absorption, or drug interactions that reduce the serum level—then the development of drug resistance is likely. The only option, if viable regimens remain, is to change the treatment.
The side effects of HAART were protean, and each class and each drug had commonly associated toxicities. Immediate side effects that might occur included nausea and diarrhea, neuropsychiatric side effects, and malaise. (A detailed account of the many types of delayed and chronic toxicities are beyond the scope of this article.) Most antiretroviral drugs have interactions with human metabolic pathways—often, the same ones involved with the metabolism of other drugs. Great caution needs to be exercised when HAART regimens are prescribed, to avoid interactions among the components within the regimen but also with these drugs and other commonly prescribed medications.
Finally, one of the greatest barriers to the use of HAART worldwide has been the cost of therapy and the monitoring of its effects. These are substantial but affordable within developed countries. It has been a prohibitive factor in the use of HAART in the developing world.
These problems associated with HAART have been addressed with varying degrees of success. Advances in therapies have delivered once-daily combinations, and one, Atripla, even combines the 3 component drugs in one pill. The development of new drugs and improvements in formulation have improved the tolerability of many combinations and reduced long-term side effects (Figs. 2, 3). A huge amount of research has been undertaken to delineate the main drug-drug interactions and the means to avoid them (Dickinson et al., 2010). This has been made easier by websites that enable the interactions of antiretroviral drugs to be checked at the time of prescription (http://www.hiv-druginteractions.org/).
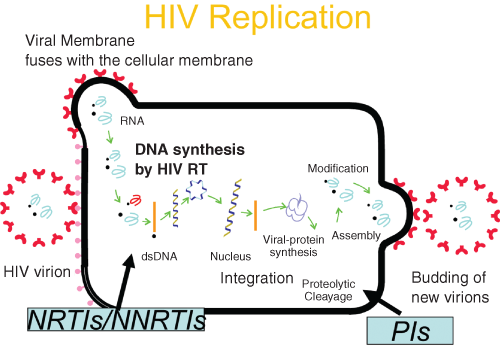
Targets for HIV therapy.
Drugs licensed to treat HIV.
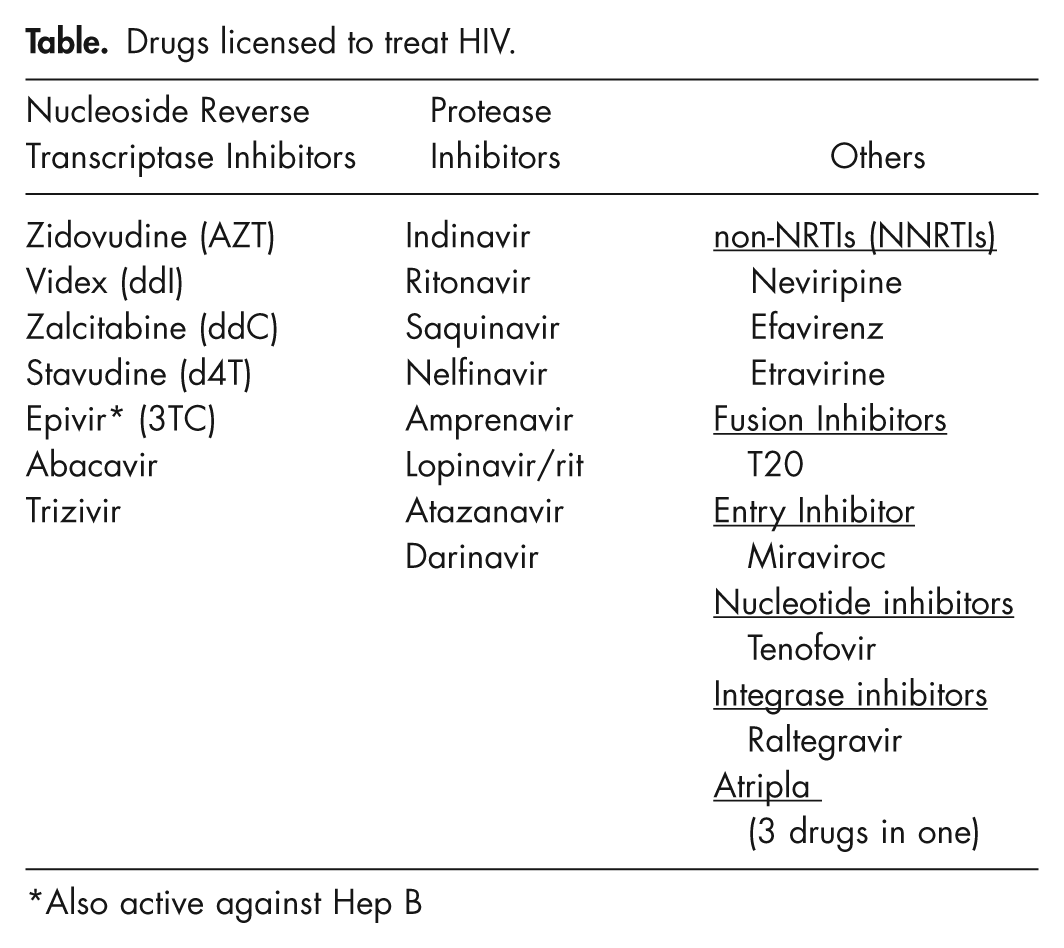
Also active against Hep B
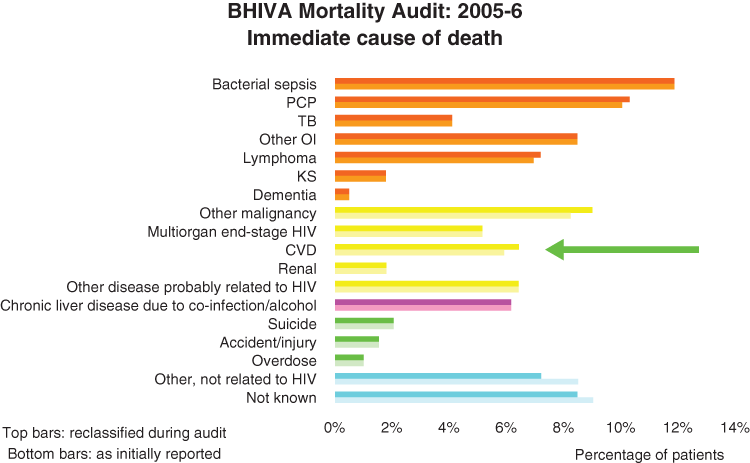
Changing patterns of mortality in HIV.
The cost of HAART has been a massive barrier to its use in the third world. Great progress has been made in recent years with rollout programs for these drugs in the poorest countries and by differential pricing strategies (Waning et al., 2009). The best of these initiatives have demonstrated the ability to transform health care services in these settings (El-Sadr and Abrams, 2007). Several million people in the poorest countries are now on treatment, but the disheartening news is that many tens of millions still do not have access to treatment that they need (Ramirez-Amador et al., 2011).
Problems with the Newer Treatments Emerge
Despite the inherent problems of HAART, by the late 1990s many HIV-infected individuals had access to a treatment that offered them a long-term future free of disease. Most patients on HAART tolerated it well, with no major side effects, showing an excellent virologic and immunologic response. It seemed as though these individuals had a prognosis for morbidity and survival that was similar to that of their HIV-uninfected peers. This did not turn out to be the case for many patients. The era of HAART heralded the chance for HIV patients to avoid suffering from further major opportunistic infections or tumors associated with HIV. However, diseases not characteristically associated with HIV were becoming increasingly common, such as cardiovascular disease; bone disease, especially osteoporosis (Cazanave et al., 2008); hepatic disease (Vogel and Rockstroh, 2009); and various metabolic abnormalities, including insulin intolerance (Aboud et al., 2007) and lipodystrophy.
Lipodystrophy is illustrative of the unexpected consequences of HIV therapy. In 1998, just 2 years after successful combination therapy was widely introduced, patients began to present with body shape changes—typically, loss of fat from the face and the limbs and central accumulation of fat, especially in the abdomen. HIV lipodystrophy (as this collection of features became known) was subsequently found to be common in patients taking certain antiretroviral drugs (Wierzbicki et al., 2008). One “well” HIV-infected patient presented to me with a gaunt face due to HIV lipodystrophy, and he summarized the feelings of many of my other patients with this condition: “Doctor, I should be grateful that you gave me these drugs which have saved my life, but in many ways I am not. For the first time in my life I feel well, but for the first time in my life I look ill and I am terrified of going anywhere lest people identify me as having HIV.”
I instituted an HIV metabolic clinic in late 1998 to manage patients with these HIV-associated metabolic issues. The number of patients being referred has mushroomed as a consequence of an increased awareness of these complications in HIV and the need to manage them. My observations have been reflected in the general experience of HIV physicians worldwide. Cardiovascular disease has emerged as a major cause of morbidity and mortality in HIV, probably resulting from a combination of the proinflammatory effects of HIV infection, an increased prevalence of traditional risk factors, and the effects of HAART (Friis-Møller et al., 2003; DAD Study Group et al., 2007; Currier et al., 2008; Kuller et al., 2008).
Hence, many manifestations of HIV disease currently relate to new patterns of morbidity (Fig. 3). Because our patients live much longer, problems become unearthed as they relate to the underlying effects of HIV on the body and to HAART therapy.
A 2006 trial reported important clues regarding why these problems arose (Strategies for Management of Antiretroviral Therapy [SMART] Study Group et al., 2006). The trial hypothesized that once patients’ CD4 counts stabilized at a high-enough level, they could stop their therapy for a period. It was postulated that intermittent treatment with HAART avoided the side effects associated with anti-HIV drugs, without any disadvantages. In this study, patients were randomized to a group that stopped HAART once their CD4 count was above 350 cells/mm3 and only restarted if their CD4 count fell below 250 cells/mm3 or there were HIV-related problems. The other group continued on HAART. To the surprise of the investigators, there was a much greater rate of HIV-related and non-HIV-related morbidity and mortality in the group who stopped treatment. This even occurred in patients with a relatively high CD4 count. The hazard ratio for death among the patients who discontinued their treatment compared to those who continued was 2.6 (95% confidence interval, 1.9-3.7). So it became clear that there were factors that could be improved by treatment, were independent of CD4 counts, and could lead to end organ disease in HIV-infected patients. What was causing the morbidity or mortality in patients off HAART treatment?
A substudy of that 2006 trial (Strategies for Management of Antiretroviral Therapy [SMART] Study Group et al., 2006) helped provide the answer (Kuller et al., 2008). When patients stopped HAART, there were significant increases in inflammatory and coagulation markers such as IL-6, D-Dimer, and hsCRP. These markers are associated with greater risk of a number of diseases—particularly, cardiovascular diseases—in addition other end organ damage.
Evidence has therefore emerged that HIV is a inflammatory condition that HAART treatment may modulate. Even those individuals who naturally have a low viral load and are slow progressors or nonprogressors have this basic proinflammatory background. Although HAART treatment will improve these markers (i.e., reduce them), they will not bring them down to normal levels compared to those of a control population. Hence, it appears that HIV infection, just like diabetes or rheumatoid arthritis, carries morbidity and mortality for cardiovascular disease and other conditions at a rate relatively higher than that of the general population.
How should we respond to our newfound knowledge that HIV patients are more likely to get a range of diseases associated with an increase in background inflammation? A key response is to select HAART in terms of safety as well as efficacy and to avoid or cautiously use any drugs that might increase the risk of myocardial infarction, particularly in those with raised cardiovascular risk. Hence, patients with HIV should be frequently screened for increased risk of cardiovascular or coronary heart disease, and they should be screened for morbidity common in HIV, such as reduced bone density. To emphasize the importance of this, a recent study indicated that HIV is an independent risk factor for cardiovascular disease and that, when all other traditional risk factors are adjusted for, HIV increases the risk of developing cardiovascular disease by 50% (Grunfeld et al., 2009). This is roughly equivalent to the risk posed by smoking, diabetes, or an increase in age of 6 to 9 years. Hence, it is important to avoid drugs that exacerbate cardiovascular disease or worsen the metabolic syndrome or increase the body shape changes.
The Future of HIV Therapy
So what of the future? Over the next few years, studies will improve our understanding of the significance of increased cardiovascular risk and increased risk of bone and other organ disease in HIV. This will require large well-controlled studies, and a number of these are underway. These studies should help us understand the extent and manner in which immune activation contributes to HIV disease in humans, although some of this evidence may come from nonhuman primate models. We will continue using HAART as the cornerstone of our therapy for HIV for many years to come, and new compounds are being developed (Stellbrink, 2009). However, rather than use it early to reduce the inflammation of HIV, we will probably develop treatments that target immune activation or information itself. In that way, we can avoid the use of HAART at an early stage—and, thus, the toxicities of HAART—as well as the cost and likelihood of viral resistance while treating the underlying proinflammatory problems associated with HIV infection. The more-distant future (10-20 years) is much more speculative. Therapies such as immunotherapeutic HIV vaccines (Pett, 2009) and gene therapy (Berkhout, 2009) or novel approaches such as radioimmunotherapy (Dadachova and Casadevall, 2009) may allow us to change the treatment paradigm of HIV.
Conclusions
Huge progress has been made in the treatment that is available for HIV, and this has extended the horizon of patients such that most can expect good health for many decades. Much more needs to be done in making these drugs available to all those affected throughout the world. The problems associated with each treatment regimen means that “tailor-made” therapy is the minimum standard of care for each patient with HIV, thereby necessitating estimation of basic risk factors for patients with HIV (e.g., heart and bone disease) and selection of the appropriate HAART. Despite the challenges of the HIV epidemic, therapy has significantly improved, and we can look forward to further advances in treatment for one of the greatest threats to global health of the past and present millennium.
Footnotes
Acknowledgements
B.S. Peters has received honoraria for attending advisory boards, or contributions to conference expenses, from Gilead, Abbott and ViiV pharmaceuticals.