
Abstract
Biodegradable fixation systems could reduce or delete the problems associated with metallic systems, since removal is not necessary. The aim of this study was to establish the effectiveness and safety of biodegradable plates and screws as potential alternatives to metallic ones. This multi-center randomized controlled trial was conducted from December 2006 to July 2009. Included were patients who underwent mandibular and/or Le Fort I osteotomies and those with fractures of the mandible, maxilla, and zygoma. The patients were assigned to a titanium control group (KLS Martin) or to a biodegradable test group (Inion CPS). The primary outcome measure was ‘bone healing 8 weeks post-operatively’. The Intention-To-Treat (ITT) analysis of 113 patients in the titanium group and 117 patients in the biodegradable group yielded a significant difference (p < 0.001), primarily because in 25 patients (21%) who were randomized to the biodegradable group, the surgeon made the decision to switch to titanium intra-operatively. Despite this ‘inferior’ primary outcome result, biodegradable plates and screws could be safely used when it was possible to apply them. The benefits of using biodegradable systems (fewer plate removal operations) should be confirmed during a follow-up of minimally 5 years (Controlled-trials.com ISRCTN number 44212338).
Introduction
Essential prerequisites for the bone healing of fractures and osteotomies include sufficient vascularization, anatomical reduction, and immobilization of bone segments. At present, immobilization of bone fragments is obtained with metallic plates and screws without MaxilloMandibular Fixation (MMF; Stoelinga, 2003). This allows patients to load their masticatory system functionally immediately following surgery. The currently available metal plating systems have the advantage of combining excellent mechanical and handling properties. A disadvantage of metallic plates and screws is their long life remaining in situ, resulting in several potentially adverse effects, such as: (1) sensitivity to hot and cold stimuli (Suuronen et al., 1994), (2) palpability of the plates, (3) possible growth disturbance or mutagenic effects (Penman and Ring, 1984; Yaremchuk and Posnick, 1995), and (4) interference with imaging or radio-therapeutic irradiation techniques (Rozema et al., 1990; Peltoniemi et al., 1997). As a consequence, the implants are removed following bone healing in a second operation in 5-40% of the cases (Matthew and Frame, 1999; Bhatt et al., 2005). Biodegradable plates and screws degrade in the human body, reducing or eliminating the problems associated with metallic systems. This is desirable from the viewpoint of cost-effectiveness, patient comfort, healthcare quality, and risk of complications due to plate removal. However, adverse tissue reactions to degradation products have been reported (Bergsma et al., 1993; Bergsma et al., 1995; Böstman et al., 1990; Böstman and Pihlajamaki, 2000). Moreover, biodegradable systems are mechanically less favorable than metallic systems, which can result in insufficient bone healing. A few controlled trials have been published on this subject (Ferretti and Reyneke, 2002; Cheung et al., 2004; Norholt et al., 2004; Ueki et al., 2005), which have previously been summarized and analyzed in a systematic review (Buijs et al., 2006). Since the results were inconclusive, mainly because of the lack of sufficiently powered and appropriately designed trials and heterogeneity among the included studies, there is a need for well-designed randomized controlled trials of sufficient size.
The aim of this study was to establish the effectiveness and safety of biodegradable plates and screws as an alternative to metallic ones. Therefore, we tested the null hypothesis that the performance of the Inion CPS biodegradable system is inferior to that of a titanium system in terms of bone healing following treatments of mandibular, maxillary (Le Fort I), zygomatic fractures, and bilateral-sagittal split (BSO) and/or Le Fort I osteotomies.
Materials & Methods
Study Population
This prospective randomized controlled trial was conducted from December 2006 to July 2009. The source population consisted of patients who were treated at the Departments of Oral and Maxillofacial Surgery (OMFS) of the: (1) University Medical Centre Groningen (UMCG), (2) Rijnstate Hospital Arnhem (RHA), (3) Amphia Hospital Breda (AHB), and (4) Medical Centre Leeuwarden (MCL).
Patients meeting the inclusion criteria were eligible for this study (Fig. 1). All patients were informed regarding the treatment options prior to surgery and were required to provide informed consent to participate in the study. The surgeons recruited the participants and assigned them randomly to two treatment groups a day before (osteotomies) or immediately prior to (fractures) the operation. A statistician generated the randomization sequences using a computerized randomization program. The randomization sequences were linked to a central telephone, which was available 24 hrs a day, to conceal the sequence until the interventions were assigned. Stratification to hospital was executed to detect hospital effects. The study was approved by the Medical Ethical Committees of the participating hospitals.
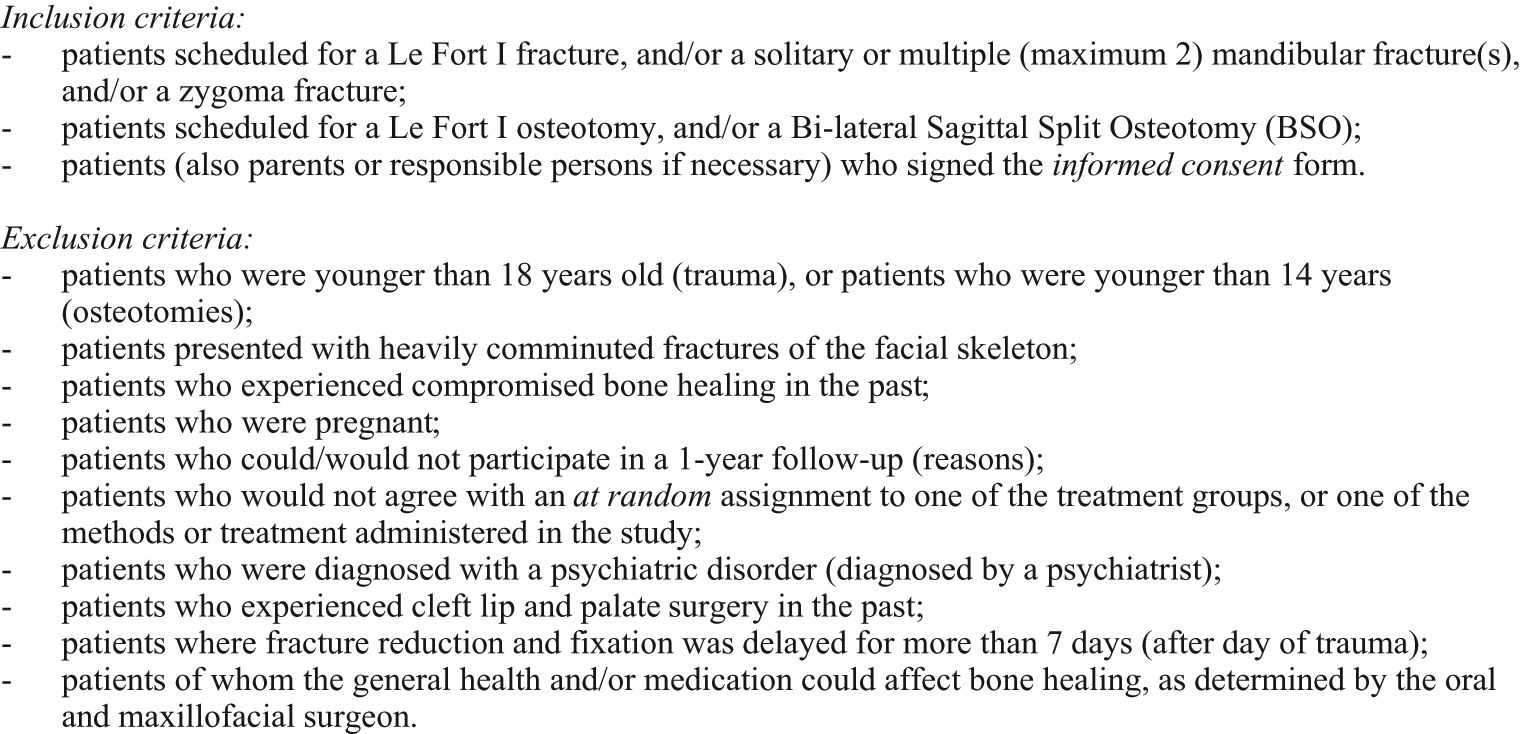
Inclusion and exclusion criteria.
Interventions
The patients were assigned to a titanium control group (KLS Martin, Gebrüder Martin GmbH & Co., Tuttlingen, Germany) or to a biodegradable test group (Inion CPS, Inion Ltd. Tampere, Finland). Neither prior to nor after surgery were the patients aware of the system that had been used.
All plates and screws were applied according to the instructions of the manufacturers. The screw holes were pre-drilled for both titanium and biodegradable screws, and pre-tapped for biodegradable screws. For fixation of mandibular osteotomies and fractures, 2.5-mm biodegradable or 2.0-mm titanium plates and screws were used, whereas 2.0-mm biodegradable or 1.5-mm titanium plates and screws were used for fixation of zygoma fractures, Le Fort I fractures, and Le Fort I osteotomies. Each participating OMF surgeon performed 2 ‘test surgeries’ using the biodegradable system to acquire the different application skills, i.e., pre-tapping the screws and pre-heating the plates, and to get used to the different dimensions. These ‘test surgeries’ were not included in the study. The patients received guiding elastics, rather than MMF, post-operatively, and they were instructed to eat a soft diet.
Outcome Measures
The primary outcome measure was ‘bone healing 8 wks after surgery’, which was defined as follows:
absence of clinical mobility of the bone segments assessed by bi-manual traction on the distal and proximal bone segments, and;
absence of radiographic signs of disturbed bone healing assessed on an orthopantomogram (OPT; all indications), a lateral cephalogram (osteotomies), an occipito-mental radiograph (zygoma fractures), and a fronto-suboccipital radiograph (mandible fracture).
The following secondary outcome measures were assessed:
clinical: correct occlusion (yes;no), palpability of plate/screw (yes;no), wound dehiscence (yes;no), and signs of inflammation (rubor, calor, dolor, tumor, or functio leasa: yes;no);
radiographic: correct position of the bone segments (yes;no; position of teeth, path of mandibular canal, and contour of cortical structures);
patient-related (self-evaluation): pain reported on a Visual Analogue Scale (VAS; range, 1-100) and mandibular function evaluated by the mandibular function impairment questionnaire [MFIQ (Stegenga et al., 1993); range, 17-85]; and
handling characteristics (plate adaptation, drilling/tapping, screw insertion, and wound closure; scale, 1-10).
Post-operative interventions, such as wound irrigation with saline, use of antibiotics, abscess incision and drainage, or removal of plate/screws within 8 wks, were reported separately. The primary and the secondary outcome measures were evaluated 8 wks following surgery by a colleague of the OMF surgeon who performed the surgery.
Statistical Analysis
Hypothesis testing was conducted following the principles of non-inferiority analysis (one-tailed test). Based on an expected percentage of bone healing of 95% with a titanium system and a maximum acceptable difference of 5% between the two groups in terms of the primary outcome measure, two groups of 109 patients were necessary to demonstrate non-inferiority with a power of 80% at a significance level of 5%. When patients violating the study protocol were taken into account, 115 patients were included in each group.
The Statistical Package for the Social Sciences (SPSS, version 18.0) was used for data analysis. The means and standard deviations of normally distributed variables were calculated and analyzed by the independent-samples t test. Dichotomized variables were analyzed by the Chi-square or the Fisher’s exact test. No interim analyses were performed during the study period.
Results
Fig. 2 represents the flow of 230 randomized patients during the phases of the study regarding the Intention-To-Treat (ITT) analysis and Treatment-Received (TR) analysis. The inclusion of the different UMCG, RHA, AHB, and MCL centers resulted in 103, 78, 44, and 5 patients, respectively. The randomization procedure resulted in an ITT population of 113 patients in the titanium group and 117 patients in the biodegradable group (Table 1). Inclusion errors were made for seven patients; four patients did not complete the follow-up. The outcome data for these patients were ‘imputed’, i.e., adequate bone healing, according to the strategies of the Cochrane Collaboration (http://www.cochrane-net.org). In 25 patients (‘switchers’) who were randomized to the biodegradable group, the OMF surgeon made the decision to switch to the titanium system intra-operatively. The main reasons for switching were material failures, including non-grip screws (n = 6), inadequate stability after the first fixation (n = 3) and after re-positioning (n = 4), inadequate plate adaptation (n = 2), dimension of plate too big (n = 1), and plate fracture during fixation (n = 1). Other reasons were logistical problems (n = 3), ‘bad split’ (n = 1), and ‘unknown’ (n = 4). In the ITT analysis, the switches were assessed as failures for the primary outcome measure. Regarding the TR analysis, the seven ‘inclusion error’ patients and the four ‘lost to follow-up’ patients were excluded. Additionally, the 25 ‘switchers’ were added to the titanium control group. This resulted in TR analyses of 133 patients and 84 patients in the titanium group and the biodegradable group, respectively.
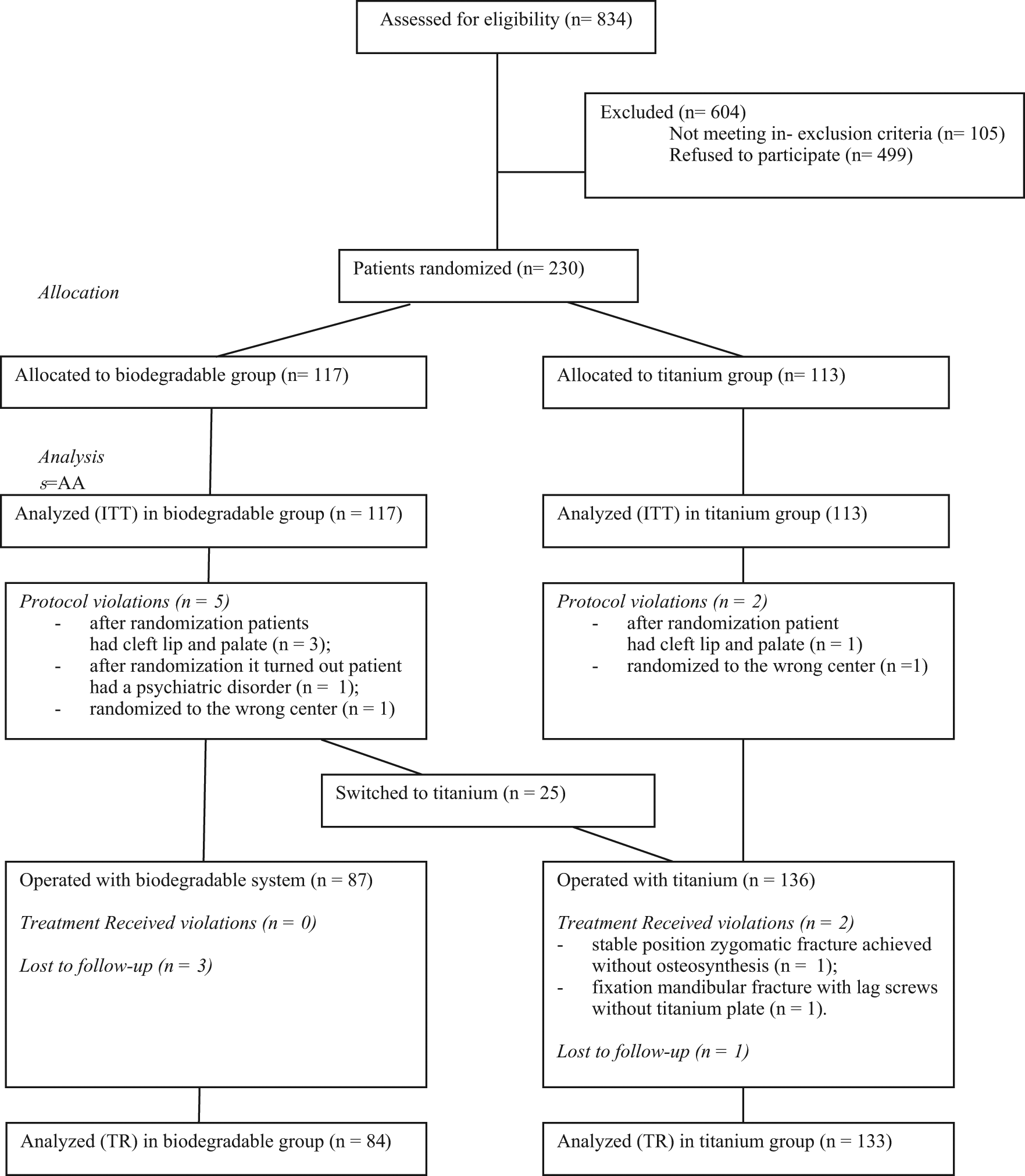
Flow diagram of patients’ progress though the phases of the RCT.
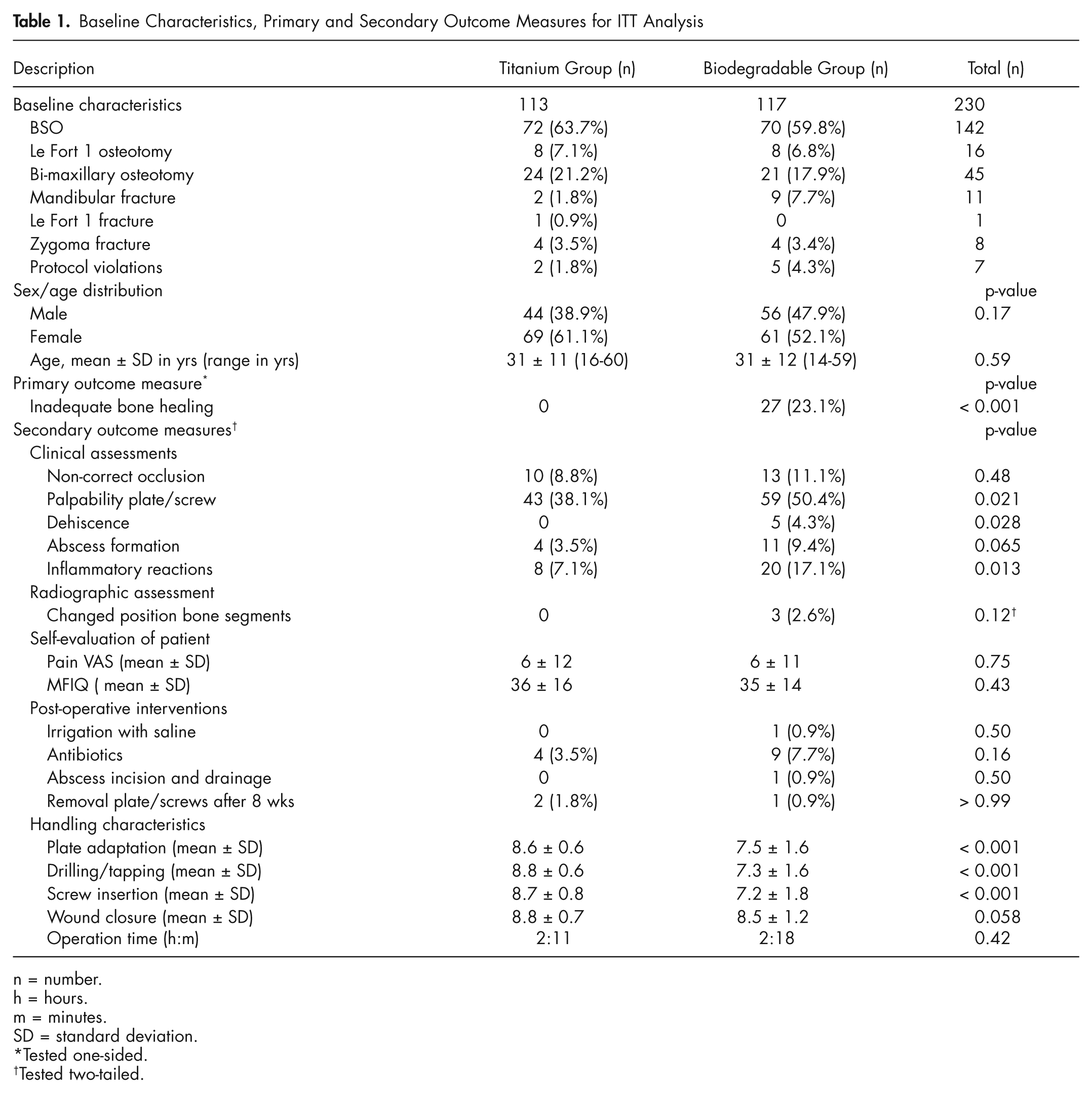
Baseline Characteristics, Primary and Secondary Outcome Measures for ITT Analysis
n = number.
h = hours.
m = minutes.
SD = standard deviation.
Tested one-sided.
Tested two-tailed.
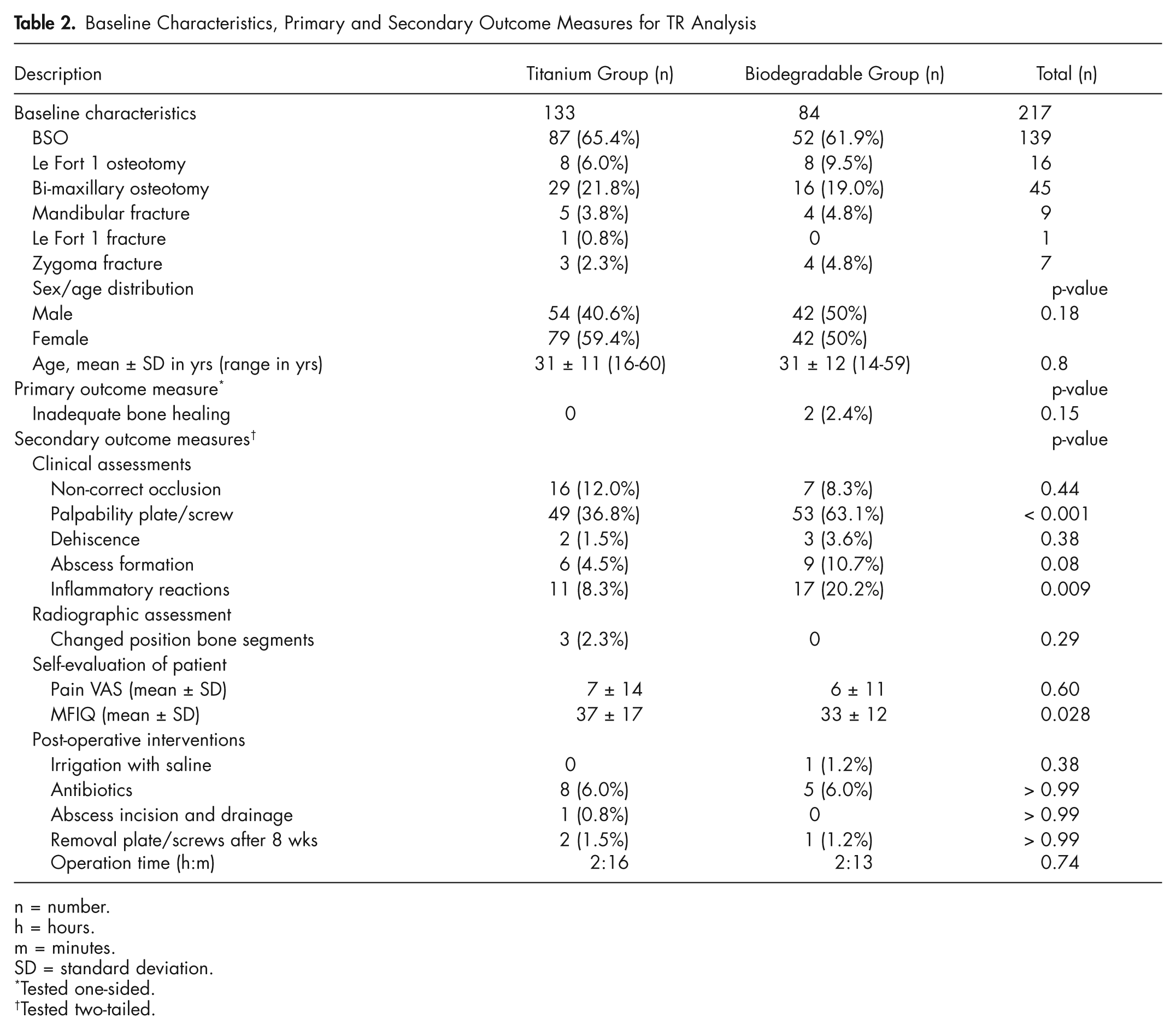
Inadequate bone healing of two patients in the biodegradable group was reported. One patient had a mobile maxilla one day after surgery and was re-operated with the titanium system. The second patient had a mobile maxilla after 8 wks that healed without intervention. Following the ITT analysis, 27 patients in the biodegradable group (25 ‘switchers’ and the two above-mentioned patients) and no patients in the titanium group showed inadequate bone healing, resulting in a significant difference (p < 0.001). Regarding the TR analysis, the two above-mentioned patients in the biodegradable group and no patients in the titanium group showed inadequate bone healing, resulting in a non-significant difference. The ITT analysis showed significant differences regarding dehiscence of the plate/screws, palpability of the plate/screws, and inflammatory reactions. There were no significant differences regarding incorrect occlusion and position of the bone fragments 8 wks after surgery. Self-evaluation of pain revealed VAS scores lower than 10 for both groups, whereas the MFIQ showed nearly equal scores for mandibular function. The post-operative interventions, wound irrigation with saline, use of antibiotics, abscess incision and drainage, and removal of plate/screws after 8 wks, did not significantly differ between both groups. The handling characteristics revealed significantly lower scores for the biodegradable system for plate adaptation, drilling/tapping, and screw insertion. Wound closure and mean operation time did not reveal a significant difference, despite the variation in handling characteristics. The results of the ITT and TR analyses for the primary and secondary outcome measures are summarized in Tables 1 and 2.
Baseline Characteristics, Primary and Secondary Outcome Measures for TR Analysis
n = number.
h = hours.
m = minutes.
SD = standard deviation.
Tested one-sided.
Tested two-tailed.
An ancillary analysis revealed that there was no ‘center effect’ with regard to bone healing. Analysis of the various surgeries did not differ significantly between the groups [p = 0.31 (ITT); p = 0.74 (TR)].
Discussion
The ITT analysis revealed that biodegradable plates and screws performed inferiorly to titanium plates and screws, whereas the TR analysis revealed that biodegradable plates and screws did not perform inferiorly regarding bone healing after 8 wks. The relatively many intra-operative ‘switches’ (21%) were primarily responsible for the inferior outcome result. These results imply that the biodegradable system is inferior to titanium plates and screws, but that the system could be successfully used without MMF when it is possible to apply them. Concerning the secondary outcome measures, the biodegradable system did not perform significantly differently from the titanium system, except for palpability of the system and inflammatory reactions. These differences could be expected at the 8-week follow-up and did not result in more plate removal operations. Up to 8 wks, the biodegradable plates and screws are safe to apply. The handling characteristics showed a remarkable difference between both systems, whereby biodegradable plates and screws were more difficult to use as compared with titanium plates and screws.
Other studies (Ferretti and Reyneke, 2002; Cheung et al., 2004; Norholt et al., 2004; Ueki et al., 2005), as discussed in a systematic review (Buijs et al., 2006), did not demonstrate a significant difference regarding clinical morbidity and stability. However, they did not use bone healing as the primary outcome measure. The primary outcome measure ‘bone healing after 8 wks’ used in the present study was chosen since the mechanical characteristics of biodegradable plates and screws were less favorable compared with titanium ones (Buijs et al., 2007a,b, 2009). This may result in insufficient and delayed bone-healing percentages. In addition, the reviewed studies included limited numbers of patients. Titanium plates and screws show high success rates (95%) according to the opinions of clinical experts and in large patient series (Iizuka and Lindqvist, 1992; Bhatt et al., 2005). Taking these results into account, it is a prerequisite to obtain ‘non-inferior’ bone healing when using biodegradable plates and screws. Until now, there has been no thorough scientific evidence that biodegradable plates and screws will result in more incomplete or delayed bone healing. A remarkable difference is that the systematically reviewed studies did not report any switches, in contrast to the present study.
Regarding the ITT analysis, the outcome data for the seven ‘inclusion error’ patients and the four ‘lost to follow-up’ patients were ‘imputed’ to remain an ITT population. Counting these patients as failures does not seem to be reasonable, given the overall low failure rate and also the fact that most patients with problems would be more likely to return than not. By contrast, the ‘switchers’ to the titanium group were defined as failures of the biodegradable system. The vast majority of these failures were related to material failures (see Results). If the system could not be applied initially, the system failed to obtain bone healing 8 wks after surgery. The ‘switchers’ were excluded from further analyses. Inexperience and lack of confidence in a still ‘unknown and new’ biodegradable system, handling differences, and having a sense of certainty and confidence regarding the titanium system may have contributed to the relatively high number of switches. The primary outcome measure was not stratified for indication, since it could be expected that the bone segments would be healed after 8 wks, independent of the indication. The post hoc analysis provided a non-significant result between the groups. However, the relatively low number of Le Fort I fractures impedes the power of the results for this indication. By contrast, the high number of inclusions of the other indications implies good eloquence of the results. In the Materials & Methods section, it is stated that the evaluation of outcome measures was planned to be performed by a colleague of the OMF surgeon who performed the surgery. Despite the intended protocol, in too many cases this was not practical. This phenomenon may have introduced observer bias. The study was performed in 4 hospitals, and different surgeons did the operations. This implies good generalizability. In contrast, several surgeons could imply diminished power of the study as a result of a possible learning curve factor. However, it appeared that the switches from the biodegradable to the titanium system took place over the entire study. Moreover, the switches were made by all participating surgeons and at all centers. It can therefore be expected that the performance of the Inion CPS biodegradable system in other hospitals will be similar to that found in our study.
In summary, it is concluded that, in terms of bone healing after 8 wks, the performance of the Inion CPS biodegradable system is inferior compared with that of the titanium system for the treatment of mandibular, zygoma fractures, and BSO, and/or Le Fort I osteotomies. Despite this ‘inferior’ primary outcome result, biodegradable plates and screws could be safely used without MMF in selected cases. The benefits of using biodegradable systems (fewer plate removal operations) should be confirmed during a follow-up of minimally 5 yrs. The presented results are part of a longer-running follow-up study.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.