
Abstract
The scientific evidence concerning prosthodontic care for the shortened dental arch (SDA) is sparse. This randomized multicenter study aimed to compare two common treatment options: removable partial dental prostheses (RPDPs) for molar replacement vs. no replacement (SDA). One of the hypotheses was that the follow-up treatment differs between patients with RPDPs and patients with SDAs during the 5-year follow-up period.
Two hundred and fifteen patients with complete molar loss in one jaw were included in the study. Molars were either replaced by RPDPs or not replaced according to the SDA concept.
A mean number of 4.2 (RPDP) and 2.8 (SDA) treatments for biological or technical reasons occurred during the 5-year observation time per patient. Concerning the biological aspect, no significant differences between the groups could be shown, whereas treatment arising from technical reasons was significantly more frequent for the RPDP group. When the severity of treatment was analyzed, a change over time was evident. When, at baseline, only follow-up treatment with minimal effort is required, over time there is a continuous increase to moderate and extensive effort observed for both groups (Controlled-trials.com number ISRCTN97265367).
Keywords
Introduction
One main goal in dentistry is to improve the decision-making processes in clinical situations on a strong evidentiary basis (Richards, 2004). The use of objective scientific criteria to guide treatment decisions should help to achieve more predictable treatment outcomes. However, in complex clinical situations – for example, with periodontally involved maxillary molars – treatment decisions vary, due to scientific uncertainty and differences in practitioners’ backgrounds, or depending on the availability of external evidence (Zitzmann et al., 2011). These sorts of problems have recently been discussed in relation to a fractured root-canal-treated maxillary incisor (Turp et al., 2007).
For the shortened dental arch (SDA) with complete molar loss in one jaw, decision-making is shifting from the evaluation of a single tooth to the evaluation of the whole arch, taking into account potential adverse effects such as temporomandibular joint disorders, insufficient chewing ability, malocclusion, and compromised oral-health-related quality of life (Applegate, 1954; al-Ali et al., 1998; Korduner et al., 2006). Essentially three viable approaches exist: (1) preserving or restoring a premolar occlusion; (2) molar replacement with a removable dental prosthesis (RPDP); and (3) fixed restoration with dental implants. A premolar occlusion is a limited treatment goal, according to the principles of the SDA concept. Only RPDPs and implant restorations allow for the replacement of all missing molars.
The SDA concept was originally introduced by Käyser and has been further documented by the Nijmegen group (Käyser, 1981; Witter et al., 1999). In a review of the SDA concept, most of the papers that were cited were based on questionnaires measuring different outcomes, or were retrospective clinical trials (Kanno and Carlsson, 2006). Very few data are available from comparative studies of the outcomes of different treatment approaches (Jepson et al., 2003; Thomason et al., 2007). Therefore, the need for randomized clinical trials is apparent.
This study aimed at generating reliable outcome data with regard to treatment following the SDA concept compared with molar replacement with RPDPs. The three-year interim analyses (Walter et al., 2010) showed no significant differences between groups for the primary outcome measure: first tooth loss. Therefore, the importance of the secondary outcome measures, such as quantitative and qualitative analyses of the follow-up treatment, has become greater, and requires more thorough analysis.
The null hypothesis of this prospective study was that the two treatment options of the SDA will not result in differences in the frequency and severity of required maintenance.
Materials & Methods
Study Design
The study was designed as a multicenter randomized controlled clinical trial with 14 participating dental schools (Luthardt et al., 2010). The trial and the clinical protocol were approved by the Institutional Review Board (TU Dresden, EK 260399). The study has been registered at http://www.controlled-trials.com/isrctn under ISRCTN97265367.
Participants
Any patient over 35 yrs old who requested prosthetic treatment and exhibited dental status matching the following inclusion criteria was considered for participation. All molars had to be missing in one jaw (study jaw), with at least the canine and one premolar present on each side. Further inclusion and exclusion criteria were described previously (Walter et al., 2010).
Once a patient had given informed consent, randomization was conducted by tables with randomly permuted blocks stratified for center and age. The allocation concealment was warranted because randomization was conducted centrally (at the Department of Medical Informatics and Biomathematics, University of Münster). The two treatment options allowed for no blinding.
Interventions
Patients were allocated either to:
(1) RPDP treatment: molar replacement, whereby molars and, if needed, second premolars were replaced by an RPDP. This RPDP was retained by precision attachments (Mini SG No. 055 675, CMSA, Biel, Switzerland) with a plastic retention insert. Attachments were connected to either splinted crowns or a FDP abutment on the posterior-most tooth on each side.
or to
(2) SDA treatment: no molar replacement, whereby, if the posterior-most tooth was the second premolar, no extension of the dental arch for molar replacement was conducted. If it was the first premolar, a cantilever FDP for the replacement of the missing second premolar was incorporated. If all premolars and anterior teeth were present, no prosthetic treatment was provided.
In both treatment groups, missing anterior teeth in the study jaw were replaced by FDPs. Any endodontically treated abutment tooth was restored with a cast post and core. The opposing jaw had to be sufficiently restored up to the first molar, for RPDP treatment, or the second premolar, for SDA treatment.
In most cases, an appropriate pre-treatment had to precede prosthetic treatment. Periodontal conditions were considered acceptable in case of pocket depths ≤ 4 mm and bleeding on probing rates ≤ 25%. All restorations were made according to a standardized protocol (Walter et al., 2001; Luthardt et al., 2010).
Outcomes
This study has recorded numerous secondary outcome measures (Walter et al., 2001; Wolfart et al., 2005). The subject of the present investigation was the evaluation of the follow-up treatment that was performed within an observation time of 5 yrs.
Procedure for Follow-up Visits
Independent and calibrated investigators from one of the participating universities were chosen at random to perform the follow-up visits. The visits were scheduled 6 wks after treatment (baseline), at 6 mos, and then annually over 5 yrs.
The examination, which lasted approximately 60 min, included a general and specific anamnesis as well as a dental, periodontal, and functional examination. This information was documented on a specially developed follow-up examination form (Luthardt et al., 2010). Any required treatment resulting from the examinations was carried out in the local dental school.
Analysis of Follow-up Treatment
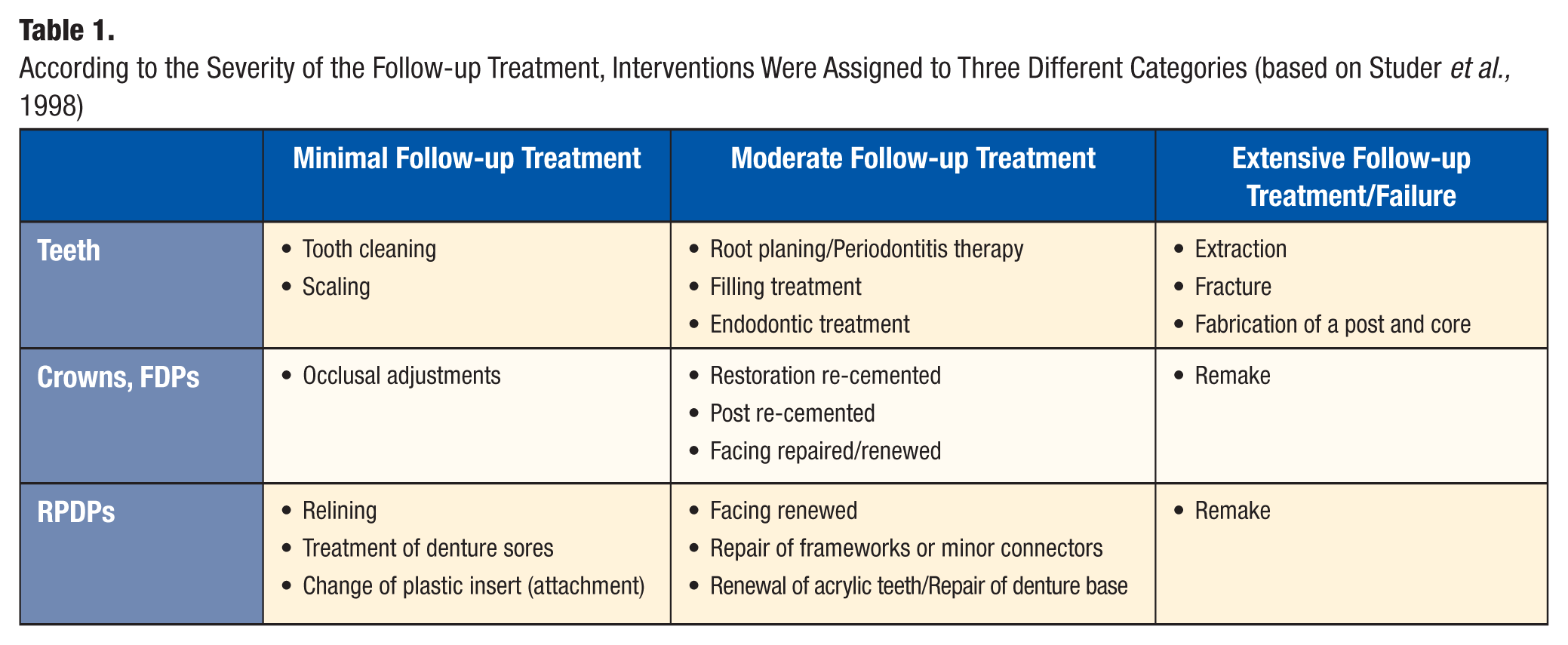
All interventions were recorded in a database on the basis of the treatment performed: (1) for quantitative analysis, the interventions were grouped according to preventive, biological, and technical aspects; and (2) for qualitative analysis, all interventions were assigned to three different categories according to the severity of the follow-up treatment: “minimal”, “moderate”, and “extensive” (Table 1). This categorization was based on a classification by Studer et al. (1998) and was previously modified (Wolfart et al., 2007).
According to the Severity of the Follow-up Treatment, Interventions Were Assigned to Three Different Categories (based on Studer et al., 1998)
Statistics
For the first part of the quantitative analysis, all follow-up treatments performed in the study arch were included; for the second part, only the first-occurring event of each type of treatment (e.g., filling treatment, endodontic treatment) per patient was included.
For the qualitative analysis, only the first event of the worst category occurring in the study arch was used. The Kaplan-Meier analyses used, as censored events, either “extensive” follow-up treatments or “extensive” plus “moderate” follow-up treatments.
All statistical analyses were based on the intention-to-treat principle. The survival distributions were compared with the Mantel-Cox log-rank test (SPSS, Version 15.0.1, SPSS Inc., Chicago, IL, USA). The significance level was set at α = 0.05.
Results
Flow of Participants
The enrollment period was 01/2001 to 02/2004. Of 215 enrolled patients, 109 were allocated to RPDP treatment and 106 to SDA treatment. Eighty-one patients received RPDP treatment, and 69 patients received SDA treatment between January 2002 and March 2005. Details on the dental and prosthetic status of the patients and on the patients who withdrew from the study have already been published (Walter et al., 2010). The number of patients who withdrew from the study prior to treatment did not differ significantly between the groups (Fig. 1).
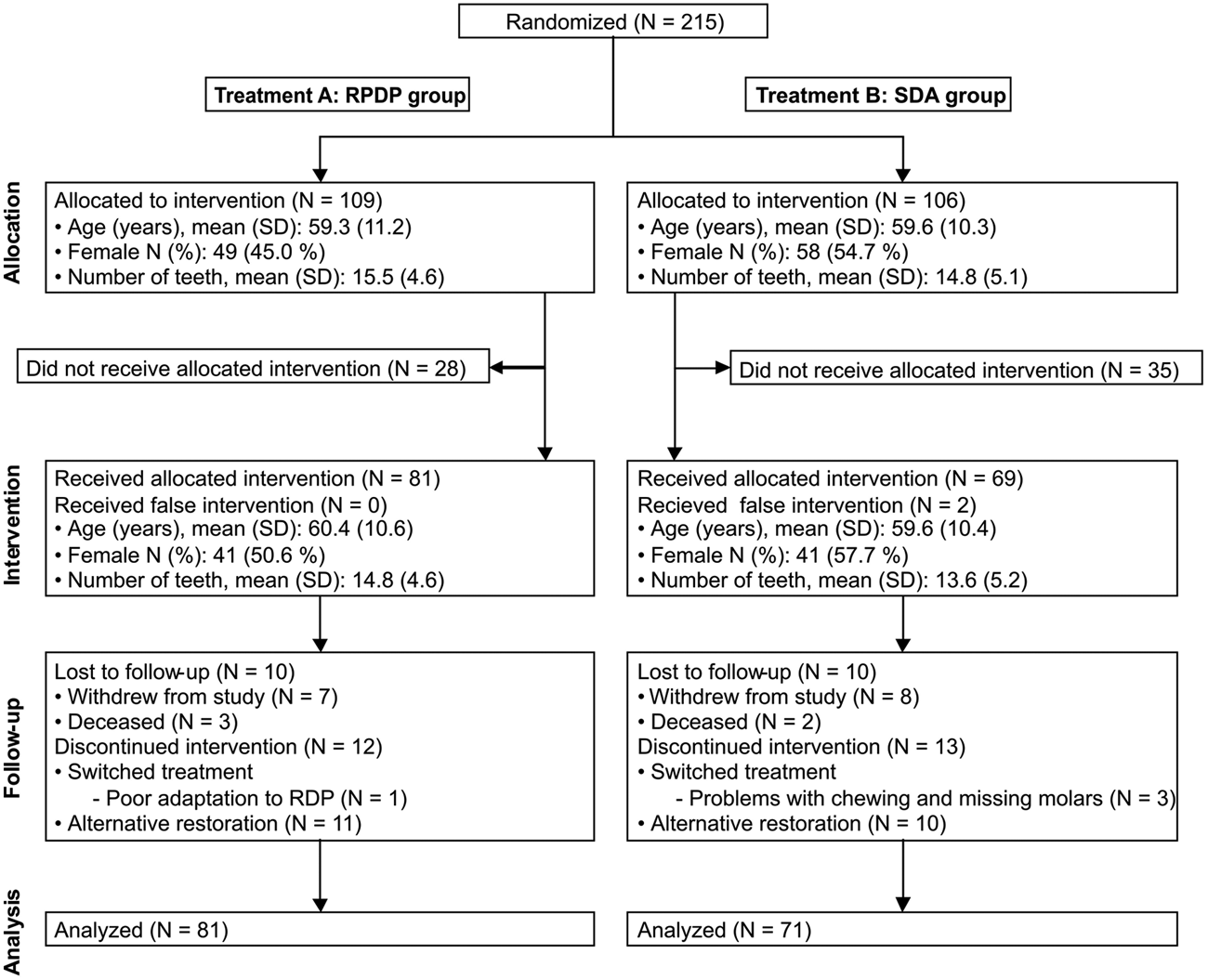
Flow of participants.
Quantitative Analysis of the Follow-up Treatment Performed in the Study Arch
The first part of the quantitative analysis evaluated the treatment events that occurred during the 5-year observation time per patient (Table 2, part A): A mean number of 1.4 (RPDP group) and 2.2 (SDA group) treatments occurred for preventive reasons, 2.1 (RPDP group) and 2.3 (SDA group) treatments occurred for biological reasons, and 2.1 (RPDP group) and 0.5 (SDA group) treatments for technical reasons occurred in the study arch.
Different Reasons for Treatment in the RPDP and the SDA Groups
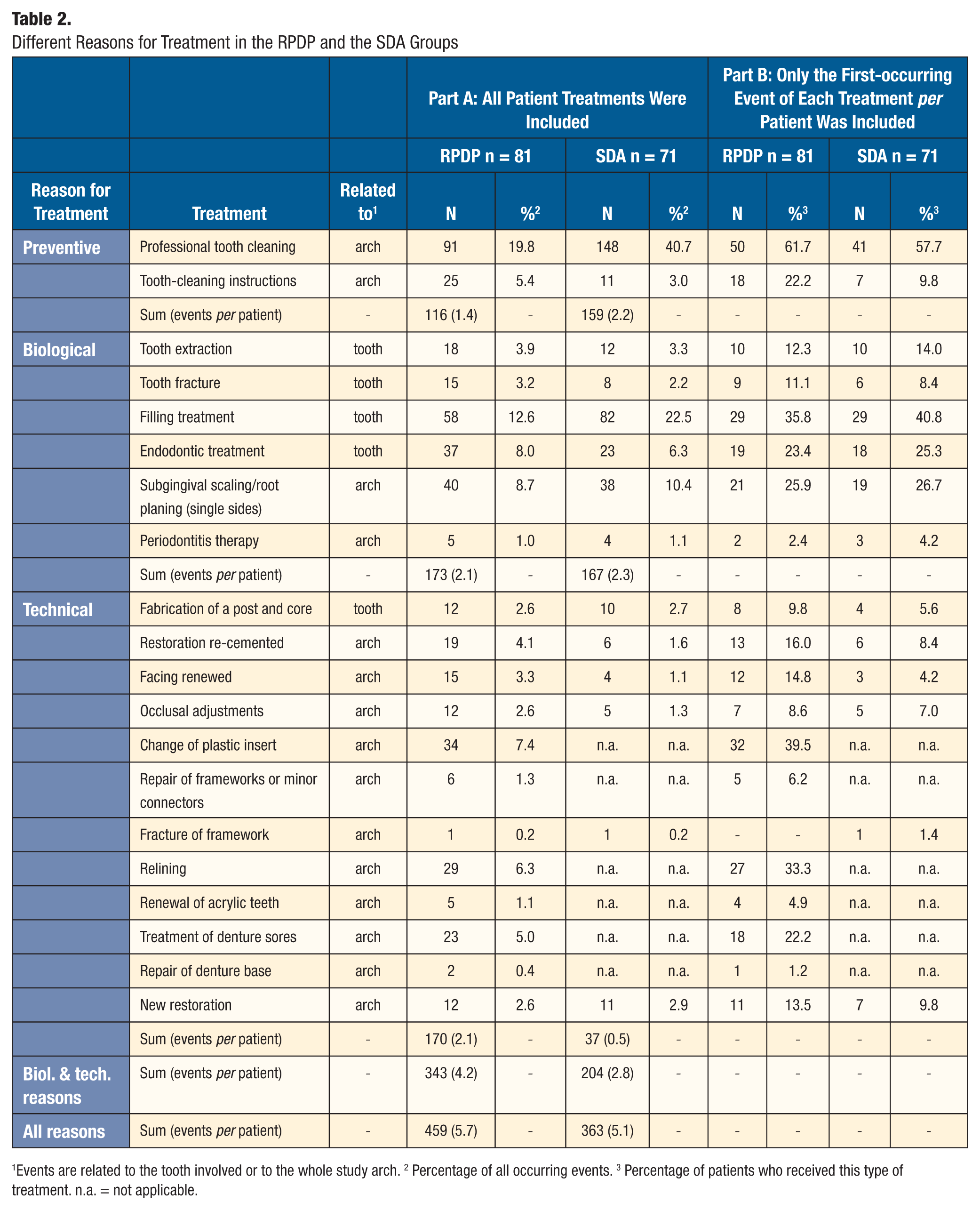
Events are related to the tooth involved or to the whole study arch. 2 Percentage of all occurring events. 3 Percentage of patients who received this type of treatment. n.a. = not applicable.
The second part of the quantitative analysis showed which type of treatment happened at least once per patient. Interventions affecting more than 25% of the patients were as follows (for details, see Table 2, part B): (RPDP group) 61.7% professional tooth-cleaning, 39.5% “change of plastic insert”, 35.8% filling treatment, 33.3% relining, and 25.9% subgingival scaling; and (SDA group) 57.7% professional tooth-cleaning, 40.8% filling treatment, 26.7% subgingival scaling, and 25.3% endodontic treatment.
Qualitative Analysis of the Follow-up Treatment in the Study Arch
The severity of the follow-up treatment is shown in Fig. 2. Fig. 2A shows the percentage of patients who did not receive extensive treatment, and Fig. 2B shows patients who received neither moderate nor extensive treatment. After 5 yrs, the percentage of patients who did not receive extensive treatment was 77% (RPDP group) or 75% (SDA group). The percentage of patients who did not receive moderate or extensive treatment was 27% (RPDP group) or 42% (SDA group). Differences between groups were not statistically significant (p > 0.05).
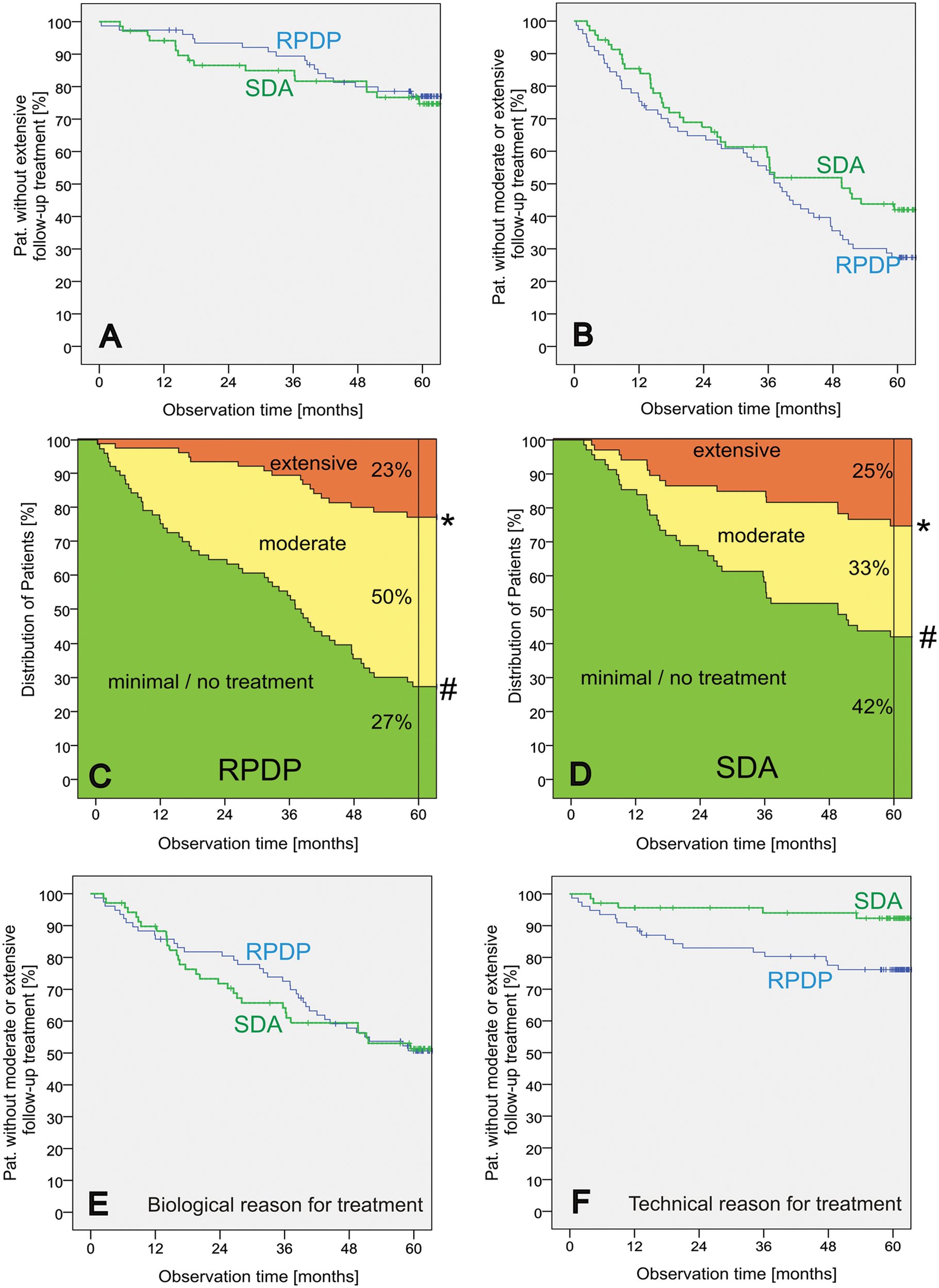
Severity of follow-up treatment.
Figs. 2C and 2D illustrate that, at the beginning of the observation period, only minimal follow-up treatment was required, followed by a continued increase in the proportion of moderate and extensive follow-up treatment for both groups. In the RPDP group, at the end of 5 yrs, 27% of patients required only minimal follow-up treatment, while the proportion that required moderate follow-up treatment had increased to 50%, and the proportion that required extensive follow-up treatment had increased to 23%. In the SDA group, the distribution of follow-up treatments changed to 42% (minimal), 33% (moderate), and 25% (extensive), respectively.
Furthermore, the data were analyzed according to biological and technical aspects (Figs. 2E, 2F). After 5 yrs, the percentage of patients who received moderate or extensive treatment for biological reasons was 49% for both groups (p = 0.880). However, where treatment given for technical reasons was concerned, the RPDP group showed a significantly higher percentage of treatment rate (24%) than the SDA group (8%; p = 0.010).
Discussion
The synopsis of the key findings shows that a mean number of 4.2 (RPDP) and 2.8 (SDA) treatments due to biological or technical reasons occurred during the 5-year observation time per patient. As far as the biological aspects were concerned, no significant differences could be shown to exist between the groups, whereas treatment due to technical reasons was significantly more frequent for the RPDP group. An analysis of the severity of treatments involved (Figs. 2C, 2D) clearly shows the shift between categories. When, at baseline, only minimal follow-up treatment was required, over time there was a continuous increase in the proportion of moderate and extensive follow-up treatment observed for both groups.
One reason for the high treatment rate in both groups might be the regular and frequent follow-up appointments which were arranged, ensuring that any small problems would be detected. The patients themselves were often not aware of a need for further treatment, or were not troubled by the small problems involved. These problems included, for example, small caries lesions, small fractures of facings, abraded occlusal surfaces, and – the most frequent technical treatment – “change of plastic retention insert” (Table 2). Consequently, restorations should not be described as “poor” per se simply because considerable follow-up treatment was required. In this context, Wöstmann et al. (2007) reported on a group of patients who received RPDP restorations and participated regularly in a follow-up program. The survival rate of the RPDPs was 10% to 15% lower than in a comparable group involving unmonitored restorations. However, in the long term, these regular adjustments or even the remakes should help maintain oral health. Other studies reported that the majority of patients with unmonitored restorations required extensive oral treatment after a few years. In some cases, the restoration had even become non-functional and had accelerated deterioration of the residual dentition (Creugers and Kreulen, 2003).
In a previous study (Wolfart et al., 2007), our group found that the follow-up treatment required was more extensive with RPDPs than with fixed prosthetic restorations, with the same follow-up treatment categories as in the current study. The authors showed, 5 yrs after treatment, a distribution according to the three categories of treatment (minimal/moderate/extensive) of 25%/38%/37%, respectively, for RPDPs and 83%/11%/6%, respectively, for fixed restorations. It is remarkable that, for the RPDP group, the distributions in the three categories are comparable with the results of the current study (Fig. 2C). However, for the SDA group, there is clearly a strong shift toward moderate and extensive treatment (Fig. 2D). These negative results in the SDA group also offer a contrast to meta-analyses concerning the outcome of metal-ceramic FDPs, which report a 95% survival rate after 5 yrs (Creugers et al., 1994; Scuria et al., 1998). The reasons for the higher treatment rate in the current study might be: (1) the higher masticatory impact on a reduced premolar occlusion in contrast to an impact which is distributed to a full arch; (2) the fact that patients did not tolerate the SDA concept (n = 2, 3%); and (3) the fact that 92% of all restorations were cantilever FDPs. In this context, Karlsson (1989) reported a higher incidence of failure for cantilever FDPs than for end-abutment FDPs.
A review article (Luthardt et al., 2000) reported a general consensus across various studies that patients wearing RPDPs showed a greater incidence of plaque accumulation, caries, gingivitis, and periodontitis, and also required much more follow-up treatment than patients with FDPs. This was not confirmed in our results, when all follow-up treatments (Figs. 2A, 2B), especially that due to biological reasons (Fig. 2E), were taken into account. However, if the focus is placed on the technical aspects (Fig. 2F), a significant difference between the two groups can be found. The reasons might be: (1) that a RPDP has more parts susceptible to wear than does an FDP; (2) that RPDPs are removable, and therefore more susceptible to mishandling or accidents (e.g., RPDPs can fall into the sink during cleaning); or (3) that the acrylic teeth used are not as stable as natural teeth or metal ceramic restorations and can be abraded more easily (Ghazal and Kern, 2009). As a result, particularly of problems relating to the technical aspects, the null hypothesis can be rejected.
In drawing conclusions about the non-significant aspects of this study, one must consider that the required sample size was calculated in advance for the primary outcome measure – first tooth loss. Seventy patients per group were required to provide 75% power of detecting treatment differences (Walter et al., 2010). The power analysis was not calculated for the secondary outcome measures. Therefore, one limitation of the study is that the analysis of the follow-up treatment is underpowered.
The strength of this multicenter randomized controlled clinical trial is that it showed, for the first time, different outcome measures in the treatment of the SDA. One element of this study has been the quantitative and qualitative analysis of follow-up treatment. We have also analyzed the preventive, biological, and technical aspects of follow-up treatment, and how the severity of treatment changed over time. All these elements will help the clinician make future decisions about treatment on a strong evidentiary basis.
Footnotes
This study was supported by the
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.