
Abstract
The aim of this study was to evaluate the orthodontic retention of maxillary skeletal stability after surgically assisted rapid palatal expansion (SARPE). Ninety digitized plaster casts from 30 adult patients who underwent SARPE were assessed. Thirty patients were divided equally into two groups: the No Retention Group (n = 15) and the Retention Group (n = 15) with a Transpalatal Arch [TPA]). After the end of expansion, the expander appliance was stabilized and remained in place for 4 months. The additional retention period began in the Retention Group as soon as the expander was removed and replaced by a TPA. During the same period, the No Retention Group remained without retention. The casts were created pre-operatively, at 4 months and 10 months post-expansion. The models were digitized by means of a 3D Vivid 9i laser scanner. The palatal area and volume were assessed. Both variables increased after 4 months compared with pre-operative values (p < .05). At 10 months, patients’ palatal areas and volumes were stable in both groups (p > .05). In conclusion, no retention other than the expander appliance is needed after SARPE (ClinicalTrials.gov, NCT01770782).
Keywords
Introduction
Surgically assisted rapid palatal expansion (SARPE) is an optional treatment in adult patients with a transverse maxillary deficiency greater than 5 mm (Betts et al., 1995). However, a common concern post-SARPE is whether the result is stable (Aloise et al., 2007).
Fixed or removable devices used to ensure transverse dimension stability (“retainers”) are used to maintain the result of SARPE (Bays and Greco, 1992). The use of such devices for post-operative retention has been debated in the scientific literature, and no consensus has been reached (Lagravère et al., 2006; Aloise et al., 2007; Suri and Taneja, 2008; Tiago and Gurgel, 2011).
Many of the studies on stability have assessed the dental and/or skeletal effects produced by SARPE in two-dimensional (2D) methods as well as casts and/or cephalometric radiographs (Chamberland and Proffit, 2008; Suri and Taneja, 2008; Magnusson et al., 2009; Marchetti et al., 2009; Sokucu et al., 2009; Zemann et al., 2009; Al-Ouf et al., 2010; Kurt et al., 2010; Seeberger et al., 2010).
Cast model measurements provide an indirect means of evaluating dental arches and are considered the gold standard because casts are easy to produce, are inexpensive, and provide a detailed perspective of dental arches (Rheude et al., 2005). However, important information can be lost when three-dimensional (3D) measurements are evaluated by 2D methods that may introduce analytical errors (Oliveira et al., 2004).
An alternative method for the indirect analysis of cast model surfaces is to use laser scanning, which is a technique used in both industry and medicine. Laser scanning is non-invasive and reproduces accurate 3D images of a cast on a computer. In addition, laser scanning facilitates calculations of the cast model’s area and volume, which is impossible with 2D methods (Foong et al., 1999; Kusnoto and Evans, 2002; Oliveira de Felippe et al., 2008; Gracco et al., 2010; Ivanov et al., 2011).
More precise and reproducible 3D studies with digitized casts would play an important role in enhancing the understanding of maxillary skeletal changes in terms of the palatal area and volume following SARPE. Therefore, the aim of this study was to use a laser scanner to assess the effect of orthodontic retention on transverse skeletal stability of the maxilla following surgically assisted rapid palatal expansion (SARPE).
Methods
This study was approved by the Ethics Committee in Research of the Federal University of São Paulo (Universidade Federal de São Paulo - UNIFESP), protocol number 0949/09. All patients signed a Free and Informed Consent Form. We assessed 90 digitized plaster cast images from 30 patients who underwent SARPE at the outpatient clinic in the Craniomaxillofacial Surgery Sector, Division of Plastic Surgery of UNIFESP.
The estimated sample size was based on a sample of five patients in each treatment group and on the observation of the 2 main measures to be evaluated. Assuming that no difference in relapse between patients wearing and those not wearing the retainer does not exceed 1 mm, with α = 0.05 and power of 80%, the necessary sample in each group was four patients. However, for even smaller differences between the two treatment groups to be detected, at least 15 patients per group were evaluated.
Adult healthy patients with bilateral cross-bite and bilateral transverse maxillary deficiencies greater than 5 mm were included. Patients with previous histories of maxillary surgery, congenital craniofacial malformations, and unilateral transverse maxillary deficiencies were excluded.
In this block-randomized study design, the sample was divided into 2 groups of 15 patients. Thirty individuals were divided among 3 blocks of 10 patients each. Every block randomization of 10 patients was performed with the use of sealed opaque envelopes. The No Retention Group consisted of 15 patients, eight men (53.3%) and seven women (46.7%), with a mean age of 26.3 yrs (SD = 5.3). Six Class I patients, six Class II patients, and three Class III patients were included in this group. Members of this group did not receive a retainer following removal of the expander. The Retention Group also consisted of 15 patients, 10 men (66.7%) and five women (33.3%), with a mean age of 25.3 yrs (SD = 5.0). Four Class I patients, four Class II patients, and seven Class III patients were included in this group. Members of this group were fitted with a soldered transpalatal arch (TPA) retainer following removal of the expander.
All patients were fitted with a modified Hyrax device (Leone® A2620-12; Sesto Fiorentino, Florence, Italy) an average of 1 wk prior to surgery by the same orthodontist, and each device was produced by the same technician. The first casts were produced with Type IV plaster prior to pre-operative cementing of the expanders.
The same surgeon (MDP) operated on each of the 30 patients using the same surgical technique, a subtotal LeFort I osteotomy with separation of the pterygomaxillary fissure (Betts et al., 1995) and bilateral osteotomy from the piriform rim to the pterygomaxillary fissure. This osteotomy is parallel to the maxillary occlusal plane with a step at the buttress, and bone is removed in the buttress to allow for expansion. The nasal septum was released, and a mid-line palatal osteotomy was also performed. An osteotomy of the anterior 1.5 mm of the lateral nasal wall and a bilateral release of the pterygoid plates from the tuberosity of the maxilla were performed. The procedure was performed while the patients were under general anesthesia by endotracheal intubation. Following the osteotomies, the expander screw was activated to 1.6 mm intra-operatively until a small diastema was observed between the upper central incisors. The incision was sutured along 2 planes.
On the fourth post-operative day, the screw expander was expanded by a quarter of a turn (0.2 mm) twice daily according to the protocol. The active phase of expansion was monitored weekly until the desired pre-established expansion was produced. The arches were not over-expanded. The expansion was determined through a transverse maxillomandibular width differential index (Betts et al., 1995). This index is the difference between an effective mandibular and maxillary width measured in a posterior-anterior (PA) cephalogram. The landmarks used for maxillary width were JR (jugale right) and JL (jugale left). The mandibular landmarks used were AG (antegonion left) and GA (antegonion right).The expander screw was then fixed by means of a stainless steel wire.
The expander was maintained for retention for 4 mos following screw fixation and was then removed. In the Retention Group, additional retention provided by a TPA was used for a period of 6 mos. The Hyrax appliance was immediately replaced by a TPA. The Hyrax was removed, the impression was made to manufacture the TPA retainer, and the Hyrax was re-cemented while the lab fabricated the TPA. The second cast (4 mos) was also made of Type IV plaster and was produced immediately after removal of the expander.
The same technician in the same laboratory manufactured the TPA retainer using a 1.2-mm-diameter stainless steel wire, and the TPA was cemented by the same orthodontist using glass-ionomer cement. The TPA was removed 6 mos after expander removal, after which the third cast (10 mos) was produced from each member of both groups.
Prior to evaluation, the anonymity of the casts was preserved by means of labels with codes computer-generated by an independent researcher. The dental cast models produced at pre-operative, 4-month, and 10-month periods were digitized by means of a surface laser scanner (Vivid 9i 3D, Minolta, Wayne, NJ, USA).
A 25-mm-focus digital scanning lens was used for digitization. Following installation, the Vivid 9i laser scanner was calibrated. The scanner was fixed onto a specific tripod angled at approximately 45o and 60 cm away from the center of the rotating table on which the casts were positioned. A fluorescent light source (100 W, 120 V) was used to illuminate the object.
The Vivid 9i scanner emits a red laser (690-nm wavelength) with a maximum power of 30 mW. During the scanning process, the laser emits a beam of light over the object, which should be located within the capture zone. The 3D camera, which is equipped with interchangeable lenses, should be positioned at a 45º angle relative to the cast, to produce the ideal illumination geometry during image acquisition.
Six images were acquired from each cast in 6 different positions: occlusal surface facing the camera, right oblique, left oblique, right lateral, left lateral, and frontal.
The data from the digitized casts were stored for analysis via a cable connected to a computer (Sony Vaio PCG-81311X) equipped with 3D software (Geomagic Qualify 12.0) to generate a polygon that represents a virtual copy of the original cast.
Palatal area and volume measurements were acquired from the digital images of the pre-operative, 4-month, and 10-month casts from both groups (Retention and No Retention).
Palatal Area and Volume Measurements
(A) Palatal Area – First, a distal cut was made in the first upper molars by use of the “Trim with Plane” function, followed by an outline of the cervical margins of the teeth from the right to the left sides. The teeth were then removed to leave only the palate, which facilitated calculation of the palatal area (Fig. 1).
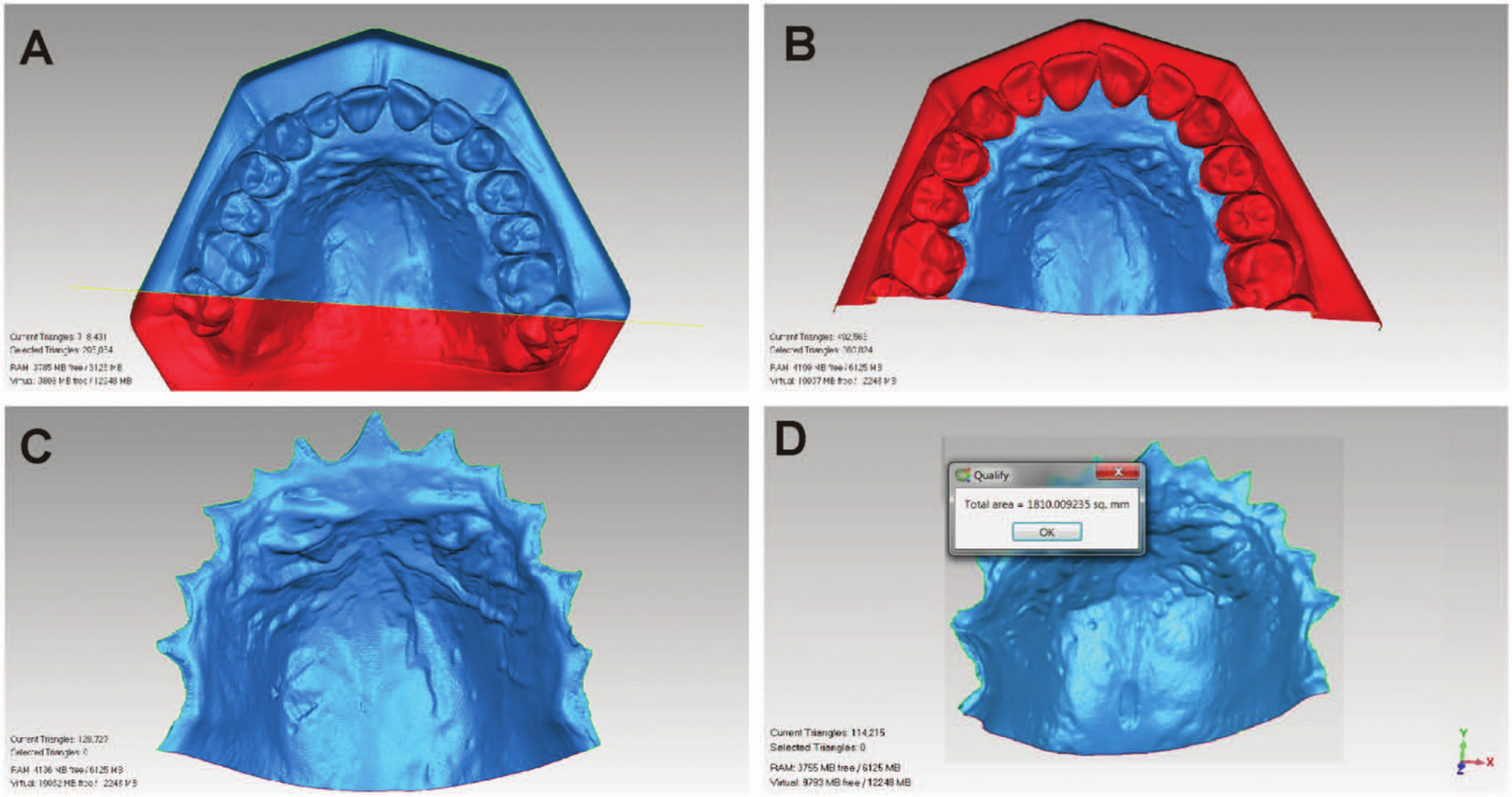
Palatal area measurement.
(B) Palatal Volume – After the palatal region of the cast was selected for the area calculation, the resulting image was closed to produce a solid for volume calculation. The posterior area was partially closed by means of the “Fill Single Flat Partial” function and was then completely closed with the “Fill All Complete” function (Fig. 2).
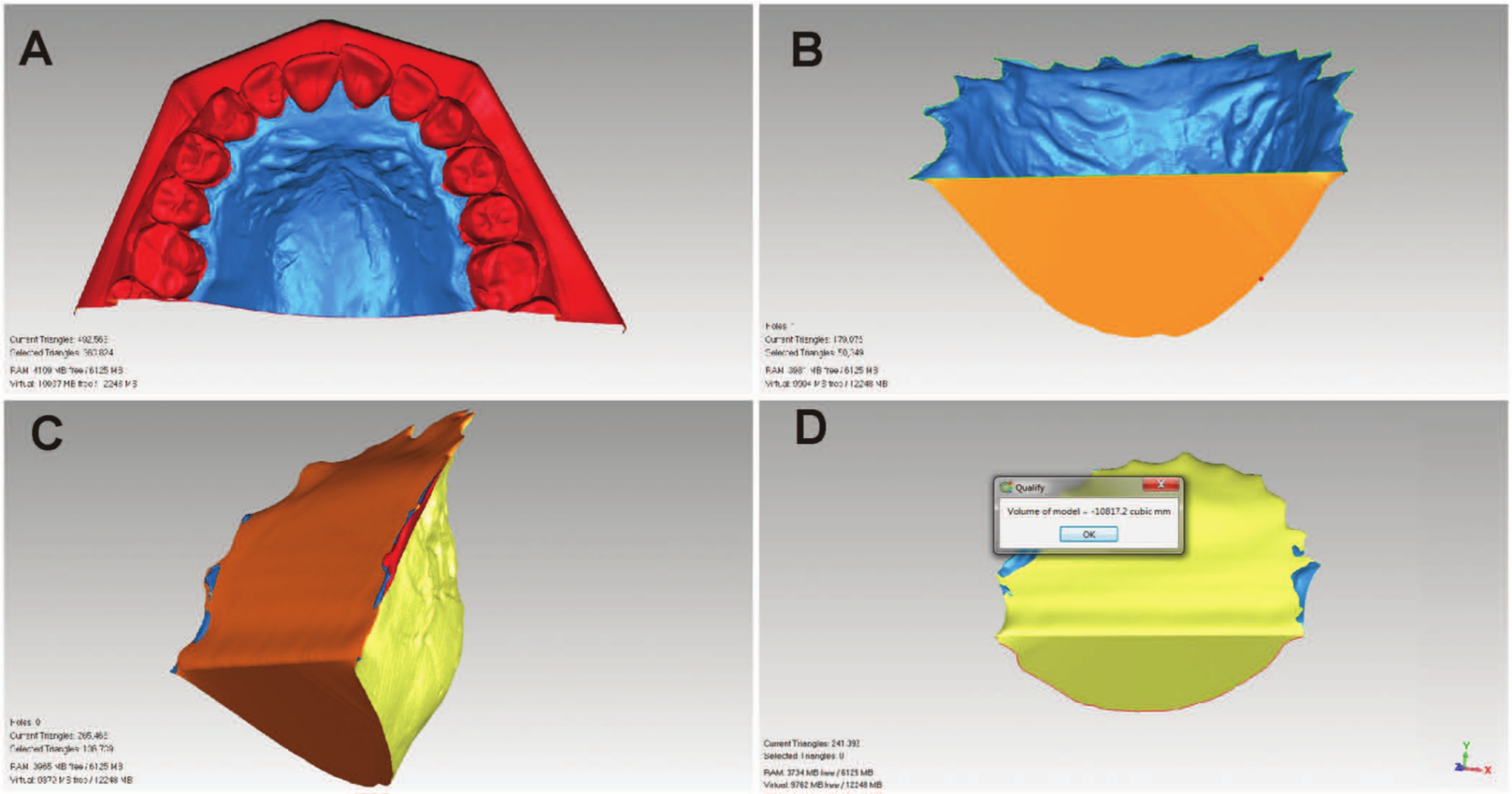
Palatal volume measurement.
Two researchers performed the measurements. Researcher 1 performed 2 evaluations with a 15-day interval between evaluations, and Researcher 2 performed the measurements on a single occasion.
The Kolmogorov-Smirnov test was used to assess the normality of the sample distributions (Kirkwood and Sterne, 2006). Age and expansion were grouped and compared by the Student’s t test (Kirkwood and Sterne, 2006). Associations between the groups and the patient genders were assessed by the chi-squared test (Kirkwood and Sterne, 2006).
Intra- and inter-examiner agreement for the 3D scanning method was assessed by an intra-class correlation coefficient (ICC), which produces 95% confidence intervals (Fleiss, 1986).
The measurements were categorized by group (No Retention and Retention) and assessment stages (pre-operative, at 4 and 10 post-operative mos) and then treated by two-way analysis of variance (ANOVA) and repeated measurements of the “stage” factor (Singer and Andrade, 2000). A first-order auto-regressive correlation matrix was assumed between the assessment stages (Singer and Andrade, 2000). For measurements that exhibited significant differences, a Tukey’s test for multiple comparisons (Neter et al., 1996) was used to verify the existence of differences among groups or stages.
The null hypothesis was rejected when p ≤ .05.
Results
The No Retention and Retention Group patients exhibited mean expansions of 8.40 mm (SD = 1.46) and 8.95 mm (SD = 1.22), respectively. There was no significant difference in the average age (p = .609), expansion (p = .272), or gender (p = .456) of the groups.
Six patients from the No Retention group and three from the Retention group have already undergone a second orthognathic surgery after the end-point follow-up period.
The intra- and inter-examiner agreement was high for both measurements, with ICCs greater than 0.9.
The palatal areas and volumes in the 3 stages revealed no significant differences between the No Retention and the Retention Groups (p > .05; Fig. 3).

The mean values and respective standard errors of the palatal areas (mm2) and volumes (mm3) of the Retention and No Retention groups. Tukey’s test for multiple comparisons. *Findings are considered significant with p < .05.
A significant increase in the mean palatal area and volume was observed at 4 mos compared with the pre-operative values, with p < .05. However, no significant difference was observed at 10 mos compared with 4 mos (p > .05) in either group (Fig. 3, Table).
Means and Standard Deviations (SD) of the Palatal Areas and Volumes in the ‘Retention’ and ‘No Retention’ Groups Pre-operatively, at 4 mos after the End of Expansion and at 10 mos after the End of Expansion
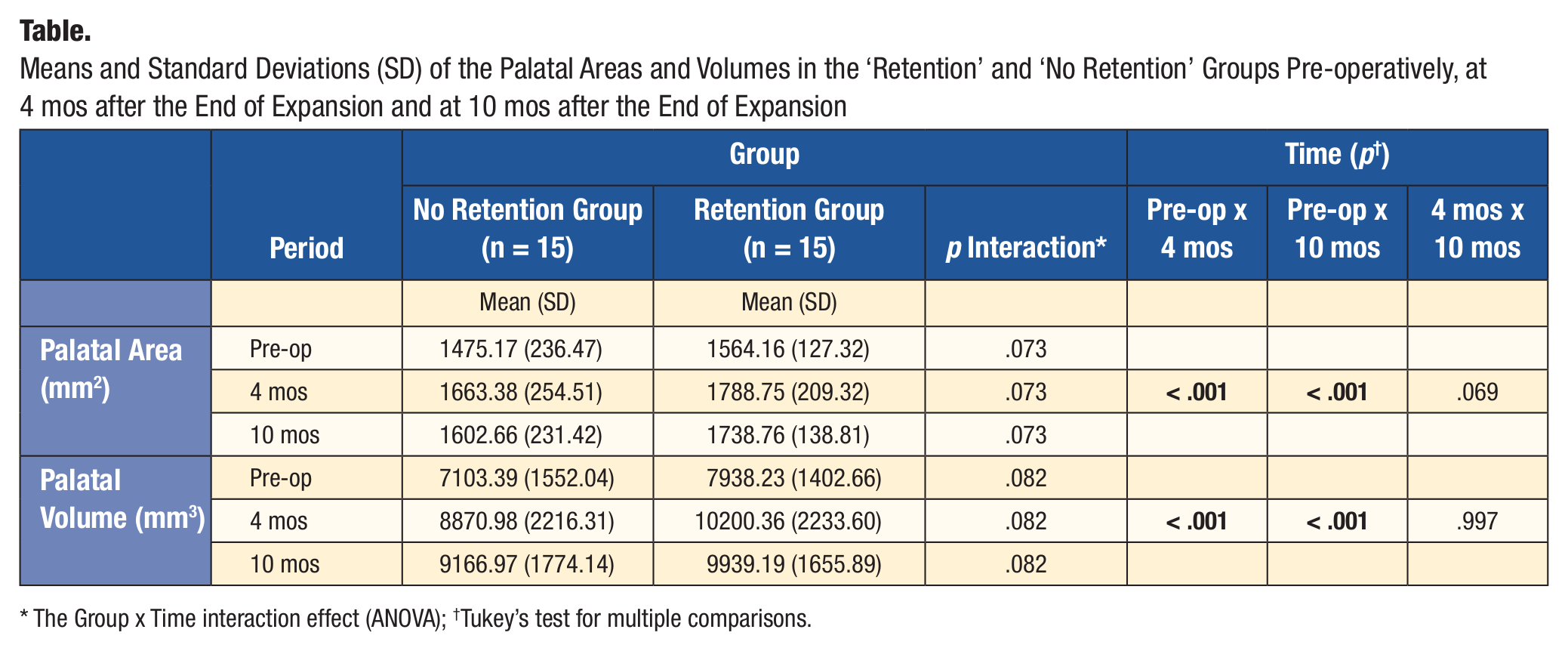
The Group x Time interaction effect (ANOVA); †Tukey’s test for multiple comparisons.
Discussion
Orthodontic retention is not necessary to maintain skeletal stability following SARPE. Relapse is closely linked to the stability of the results of SARPE. The stability of the result can be assessed using the distance of relapse following expander removal (Aloise et al., 2007; Koudstaal et al., 2009). In this study, the expander remained in place for 4 mos after the final activation of the expander screw.
The literature provides no consensus regarding retainer necessity, type, or retention time following expander removal. The justification for the use of a retainer following SARPE would be transverse maxillary relapse in the initial 6 mos following expander removal (Proffit et al., 1996). Removable and fixed retainers are the predominant types of retainer. The former is advantageous in its versatility, but because patients must comply with its use, control and efficiency are difficult to guarantee (Byloff and Mossaz, 2004). As a result, many researchers have adopted fixed retention because the result is more predictable; the best-known fixed retention is the transpalatal arch (TPA) (Aloise et al., 2007; Magnusson et al., 2009; Sokucu et al., 2009; Kurt et al., 2010).
Certain authors have suggested that TPA use following SARPE is unnecessary, which would accelerate the onset of fixed retainer use to immediately after expander removal (Chamberland and Proffit, 2008; Suri and Taneja, 2008; Magnusson et al., 2009; Kurt et al., 2010) or after expansion is completed (Bays and Greco, 1992; Marchetti et al., 2009; Zemann et al., 2009; Al-Ouf et al., 2010). Certain studies have utilized a fixed orthodontic treatment prior to SARPE (Al-Ouf et al., 2010; Seeberger et al., 2010). Some studies agreed that TPA is necessary for retention (Aloise et al., 2007; Magnusson et al., 2009; Sokucu et al., 2009; Kurt et al., 2010). However, some studies reported that there was no need of fixed retention after SARPE. These studies used a fixed appliance after or during expansion, which may have affected the stability of the results (Bays and Greco, 1992; Chamberland and Proffit, 2008; Koudstaal et al., 2009).
However, it is important to note that, in observation of the effects of retention on SARPE results and stability, fixed orthodontic therapy during the evaluation period may influence the analysis and interpretation of the results. Therefore, we did not use a fixed orthodontic device during the assessment period.
Less extensive surgical techniques can be associated with higher relapse, especially in cases of large transverse maxillary deficiencies (Koudstaal et al., 2009; Seeberger et al., 2010). In this study, the parts of the maxilla were mobilized by Le Fort I osteotomies, including a midline palatal cut and bilateral pterygomaxillary fissure disjunction but just omitting the down fracture (i.e., maxillary mobilization). This surgical technique, although less conservative, produces more consistent results and may be responsible for their stability (Byloff and Mossaz, 2004; Aloise et al., 2007; Chamberland and Proffit, 2008).
A significant increase in the palatal area was observed from the pre-operative to the later assessment stages. On average, the palatal area increased by 205.90 mm2 (13.54%) at 4 mos and by 150.55 mm2 (9.9%) at 10 mos. A 55.35 mm2 relapse was observed (3.21%) at 10 mos compared with 4 mos, but this relapse was not significant. A significant increase in the palatal volume was also observed from the pre-operative to the later assessment stages. On average, the palatal volume increased by 2,014.86 mm3 (26.79%) at 4 mos. After 10 mos, no palatal volume relapse was observed (-0.18%). It is impossible to compare the area and volume results from this study with those from other studies using similar methods, because our patients were adults and other studies involved patients with developing oral structures (Oliveira et al., 2004; Oliveira de Felippe et al., 2008; Primozic et al., 2009, 2012). These results show that both the palatal area and volume are responsible for stability following SARPE, and our palatal area and volume measurements remained stable, with no relapse in the 6 mos after removal of the expander.
In conclusion, orthodontic retention is unnecessary to maintain maxillary skeletal stability following SARPE.
Footnotes
This study was supported by the
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.