
Abstract

Keywords
Non nobis solum nati sumus – [translation] — “Not for ourselves alone are we born” by the Roman philosopher, Marcus Tullius Cicero. For our JDR readership, that includes investigators engaged in new knowledge generation in oral, dental, and craniofacial research – an ultimate duty to promote oral health at the global level. Our professional association, the International Association for Dental Research (IADR), recently reported, in the March issue of the Journal of Dental Research, on the recent progress of the IADR Global Oral Health Inequalities Research Agenda (IADR-GOHIRA®): A Call to Action (Sgan-Cohen et al., 2013) that underscores our organization’s commitment to promoting oral health, with priorities in reducing inequalities that exist globally, but particularly in emerging and developing populations. Further in alignment with this initiative, we provide another series of reports in our second clinical research supplement that serves as a companion to this month’s JDR. Here we showcase advances in oral health from clinical trials to health services research and to large-scale oral epidemiological studies.
Also this month, we highlight a special article on the global burden of oral conditions (Marcenes et al., 2013). This work reports advances that have been made in the dental and public health professions in reducing disease and where in other areas we have failed to have a significant impact on disease reduction. The global distribution of the most common chronic dental conditions is based on the 2012 Lancet reports of the Global Burden of Disease (GBD) study, the only comprehensive effort to examine the health of the world’s population (Murray et al., 2012a, 2012b; Wang et al., 2012). The GBD study catalogs nearly 300 diseases, injuries, and risk factors from 1990 until 2010. Of particular emphasis are the contributions of untreated dental caries, advanced periodontitis, and severe tooth loss affecting the people’s overall well-being. Marcenes and co-workers focused on the use of disability-adjusted life-years (DALYS) and years lived with disabilities (YLDs) to measure the burden. Oral conditions have affected nearly 4 billion people and accounted for 15 million DALYs globally (Marcenes et al., 2013). The statistics from these studies are quite sobering in showing that, over the 20-year period, there was a 20.8% increase in DALYs, although much of the increase is due to aging and population growth. Tooth loss, in contrast, decreased over time.
The World Health Organization (WHO) has done a great deal to partner with dentistry to help address and bring to the attention of both patients and the medical community information on many of these burdens related to oral health challenges (Petersen, 2010). The policy basis has been set on a strong foundation to continue to promote that: oral health is integral to general health, oral health is a determinant for quality of life, and oral health reduces premature mortality (Petersen, 2003, 2005a,b). The support of such initiatives by the oral health care communities offers solid potential to improve patients’ oral health and quality of life.
While dentistry has demonstrated major technological improvements in dental biomaterials, prevention, oral cancer detection, and related areas, the translation and implementation of these advances globally are significant challenges in light of the overwhelming social gradients that exist (Marmot, 2011; Sheiham et al., 2011). Some encouraging advancements affecting oral health include the treatment of infectious diseases such as HIV/AIDs. While these remain largely life-threatening, intense humanitarian efforts have led to improvements in access to antiretroviral drugs and community-based programs that are extending the lifespan and reducing oral health–related disabilities for affected individuals (Coogan and Challacombe, 2011; Rachlis et al., 2013). The WHO reported that, in 2010, approximately 2.7 million individuals were infected with HIV − 15% less than the 3 million newly infected in 2001 (World Health Organization, 2012). The access to antiretroviral therapy in low- and middle-income countries has greatly increased, significantly reducing the numbers of individuals dying from AIDS-related causes (Fig.). As dentistry continues to partner with public health policymakers to improve access to care to address infectious diseases, burdens of the more common chronic dental diseases can be reduced. The top-line preventive regimens may pave the way for more sophisticated and personalized therapies to treat patients using patient-based stratification approaches for customized oral health care delivery (Kornman and Duff, 2012; Garcia et al., 2013).
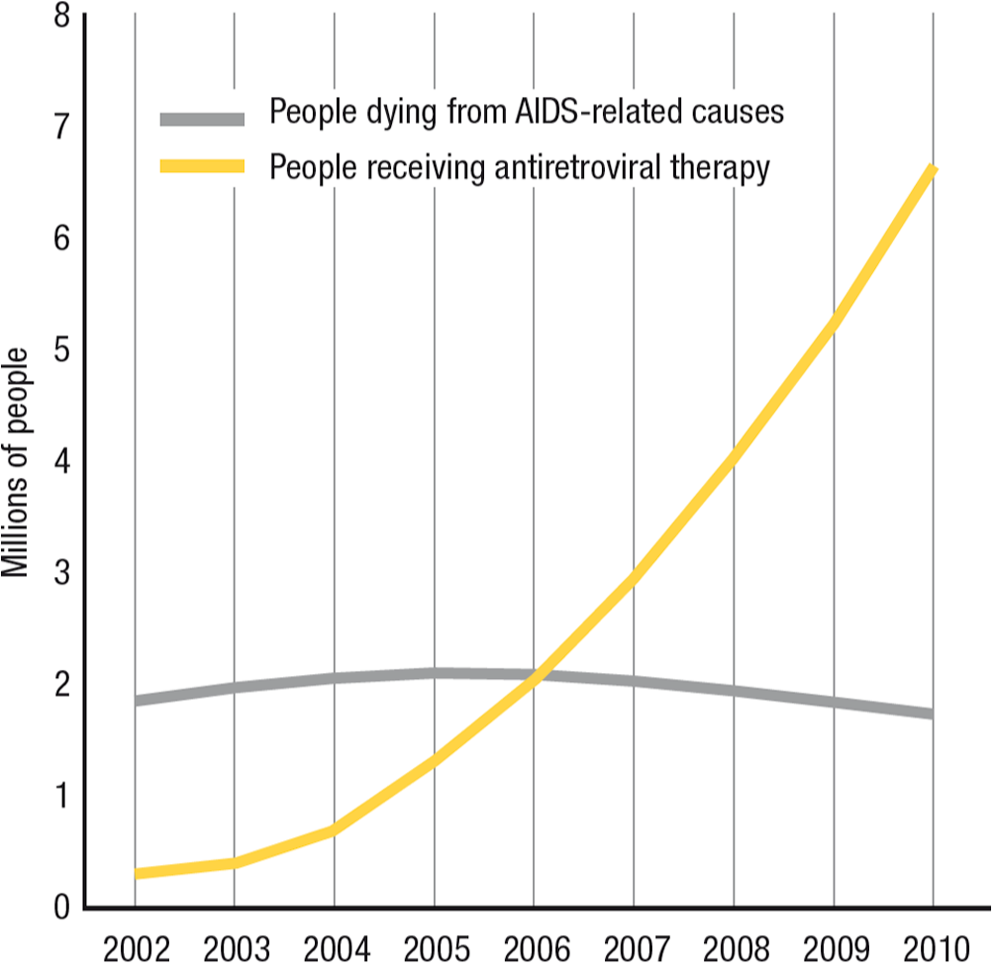
The number of people with access to antiretroviral therapy and the number of people dying from AIDS-related causes in low- and middle-income countries, 2002 to 2010 (reproduced with permission from the World Health Organization, 2012).
So let us work together on the mutual goals of the oral health research community and our IADR-GOHIRA® to meet these many challenges, so we can partake in improving oral health across the globe. The JDR will remain fully committed to the dissemination of oral health research advances to reach and affect educators, researchers, public health agencies, and patients!
Footnotes
The author declares no potential conflicts of interest with respect to the authorship and/or publication of this article.