
Abstract
Little is known about oral clefts in developing countries. We aimed to identify micronutrient-related and environmental risk factors for oral clefts in Thailand. We tested hypotheses that maternal exposure during the periconceptional period to multivitamins or liver consumption would decrease cleft lip with or without cleft palate (CL ± P) risk and that menstrual regulation supplements would increase CL ± P risk. We conducted a multisite hospital-based case-control study in Thailand. We enrolled cases with CL ± P and 2 live births as controls at birth from the same hospital. Mothers completed a questionnaire. Conditional logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs). Eighty-six cases and 172 controls were enrolled. Mothers who took a vitamin (adjusted OR, 0.39; 95% CI: 0.16, 0.94) or ate liver (adjusted OR, 0.26; 95% CI: 0.12, 0.57) were less likely than those who did not to have an affected child. Mothers who took a menstrual regulation supplement were more likely than mothers who did not to have an affected child. Findings did not differ for infants with a family history of other anomalies or with isolated CL ± P. If replicated, our finding that liver decreases CL ± P risk could offer a low-cost primary prevention strategy.
Introduction
An estimated 348,000 infants are born each year globally with an oral cleft. Over 94% of these are born in a developing country, yet little is known about risk factors for oral clefts in these settings (March of Dimes, 2006). The extent to which environmental risk factors for oral clefts are similar across countries and resource levels is unclear. Given the disproportionate burden in developing countries, identifying risk factors relevant to these populations is essential for devising effective global prevention efforts.
An oral cleft is a complex developmental trait initiated in the first trimester of pregnancy and involves genetic and environmental risk factors, such as smoking (Khoury et al., 1987). Multivitamin or folic acid supplement use in the periconceptional period reduces the risk of oral clefts (Loffredo et al., 2001; Johnson and Little, 2008; Jia et al., 2011). Supplement use of folic acid alone in parts of Europe where there is no fortification of the food supply appears to decrease the risk of oral clefts (Wilcox et al., 2007). However, in the United States and Canada, national folic acid fortification of the flour supply has resulted in minimal drops (0% to 6%) in the birth prevalence of oral clefts (Ray et al., 2003; Yazdy et al., 2007). Both high- and low-dose vitamin A appears to increase oral cleft risk (Rothman et al., 1995; Mitchell et al., 2003; Krapels et al., 2004b; Johansen et al., 2008). Low intake of micronutrient-dense foods (e.g., vegetables, liver) is also positively associated with oral cleft risk (Mitchell et al., 2003; Krapels et al., 2004b). Environmental factors, including having a cold or diabetes in early pregnancy, increases oral cleft risk according to some but not all studies (Krapels et al., 2004a; Wang et al., 2009). Evidence for these associations is primarily from Europe and North America.
We conducted a case-control study in 6 provinces in Thailand to examine the relationship between micronutrients, supplements, and environmental risk factors and cleft lip with or without cleft palate (CL ± P). We hypothesized that periconceptional maternal multivitamin use decreases the risk of having a child with a CL ± P and that vitamin A supplement or retinoic acid use increases a mother’s risk of having an affected child. In contrast, we hypothesized that liver intake, a micronutrient-dense food, decreases the risk of having an affected child. Menstrual regulation supplements may contain alcohol or herbs with estrogenic effects that could increase oral cleft risk (Winuthayanon et al., 2009; Natural Standard, 2013). We examined other environmental risk factors, including maternal diabetes and cold, in relation to CL ± P risk.
Materials & Methods
We conducted a hospital-based matched case-control study in 2003 to 2004 in 40 hospitals in 6 provinces throughout Thailand. The Center of Cleft Lip–Cleft Palate and Craniofacial Deformities at Khon Kaen University was the coordinating center. During the infants’ birth hospitalization, cases and 2 controls per case were enrolled. Controls were matched to cases on hospital of birth. Study participants (mothers) completed an interviewer-administered questionnaire that elicited demographic, behavioral, nutritional, and health data. The periconceptional period was defined as 6 weeks before conception through the first trimester of pregnancy. The study-trained nurse also completed a physical examination to classify the case’s oral cleft phenotype. Only those who spoke Thai were eligible for the study. See Appendix for recruitment details.
We classified case infants as having a CL ± P or a cleft palate only (CPO). All those with CL ± P, were eligible, including those with other anomalies, a genetic condition, or syndrome. A total of 114 cases with any type of oral cleft were enrolled. We excluded 15 cases with CPO since it is believed to be etiologically distinct from CL ± P, 2 cases because their phenotype was missing, and 11 cases with no matched controls. We analyzed 86 cases with a CL ± P and 172 matched controls.
We classified mothers as having “any vitamin use” if they reported periconceptional intake of a multivitamin, folic acid, calcium, iron, iron–B vitamin complex, or other type of vitamin. Mothers were categorized as having taken a folic acid supplement if they reported periconceptional intake of folic acid, an iron–B vitamin complex (which includes folic acid), or a multivitamin. This means that a multivitamin would count as taking a folic acid supplement but an unknown type of vitamin would not. We classified high-dose vitamin A exposure as those who took a vitamin A supplement or retinoic acid in the periconceptional period. We classified women as having eaten liver (typically pork), taken a “menstrual regulation supplement,” or as having a cold, if they reported this in the periconceptional period. Mothers who reported diabetes, regardless of type or date of diagnosis, were categorized as having diabetes.
We classified cases without any other anomalies or a midline cleft as having an isolated CL ± P. We also created a subgroup without a family history of a congenital anomaly. Covariates were operationalized and analyzed as categorized in Tables 1 and 2. For variables with missing data, the proportion missing is indicated in Tables 1 and 2. Too few mothers drank alcohol or smoked cigarettes to analyze dose. No information about frequency of cigarette smoking of family members or work colleagues was collected, so this measure was dichotomous.
Baseline Characteristics by Case and Control Status
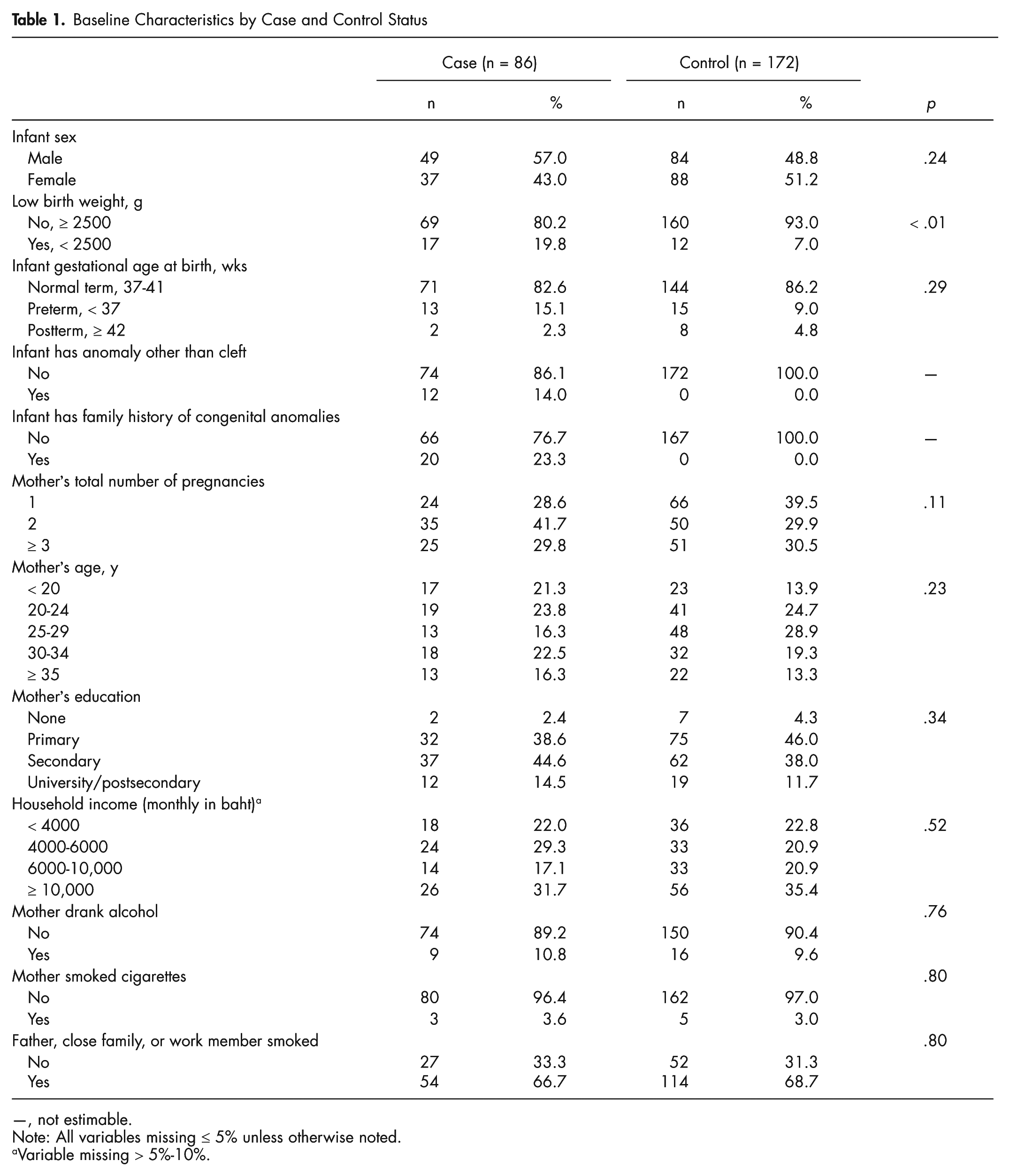
—, not estimable.
Note: All variables missing ≤ 5% unless otherwise noted.
Variable missing > 5%-10%.
Descriptive Statistics for Maternal Exposures of Interest
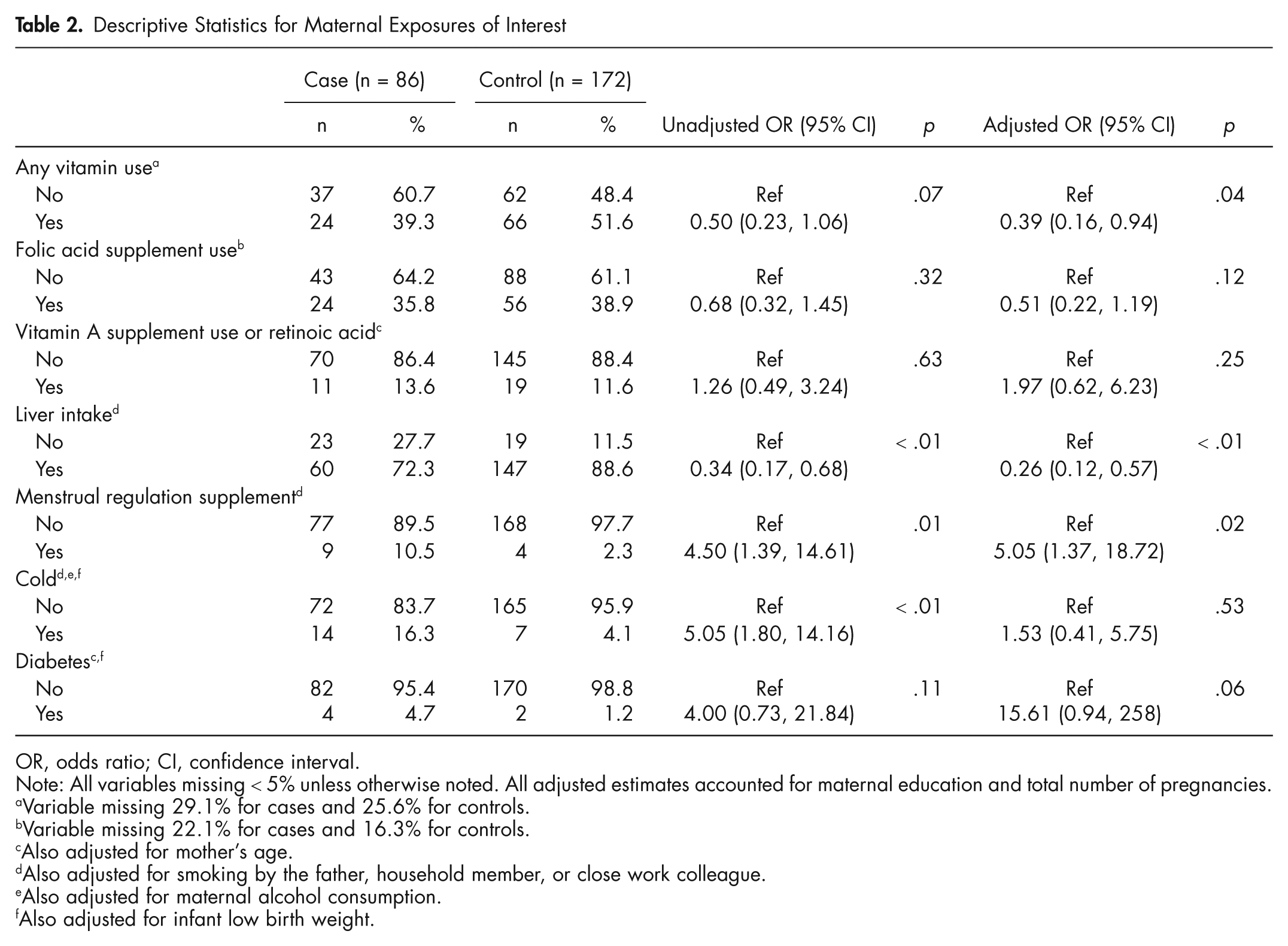
OR, odds ratio; CI, confidence interval.
Note: All variables missing < 5% unless otherwise noted. All adjusted estimates accounted for maternal education and total number of pregnancies.
Variable missing 29.1% for cases and 25.6% for controls.
Variable missing 22.1% for cases and 16.3% for controls.
Also adjusted for mother’s age.
Also adjusted for smoking by the father, household member, or close work colleague.
Also adjusted for maternal alcohol consumption.
Also adjusted for infant low birth weight.
We calculated descriptive statistics and p values for infant birth, maternal pregnancy, and household characteristics across case and control status. Because cases were matched to controls on hospital of birth, conditional logistic regression was used to estimate all p values and unadjusted and adjusted associations between proposed risk factors and CL ± P along with 95% confidence intervals (CIs). We generated separate models for each potential risk factor, adjusting for mother’s age, education, parity, smoke exposure, and other factors identified a priori as potential confounders. We assessed each potential confounder separately and in combination with other potential confounders. Our modeling strategy was to drop potential confounders that did not change estimates to a meaningful degree (generally < 10%) from the initial and combined models. Adjustment variables are noted for each model (Figure, Table 2, Appendix Table).
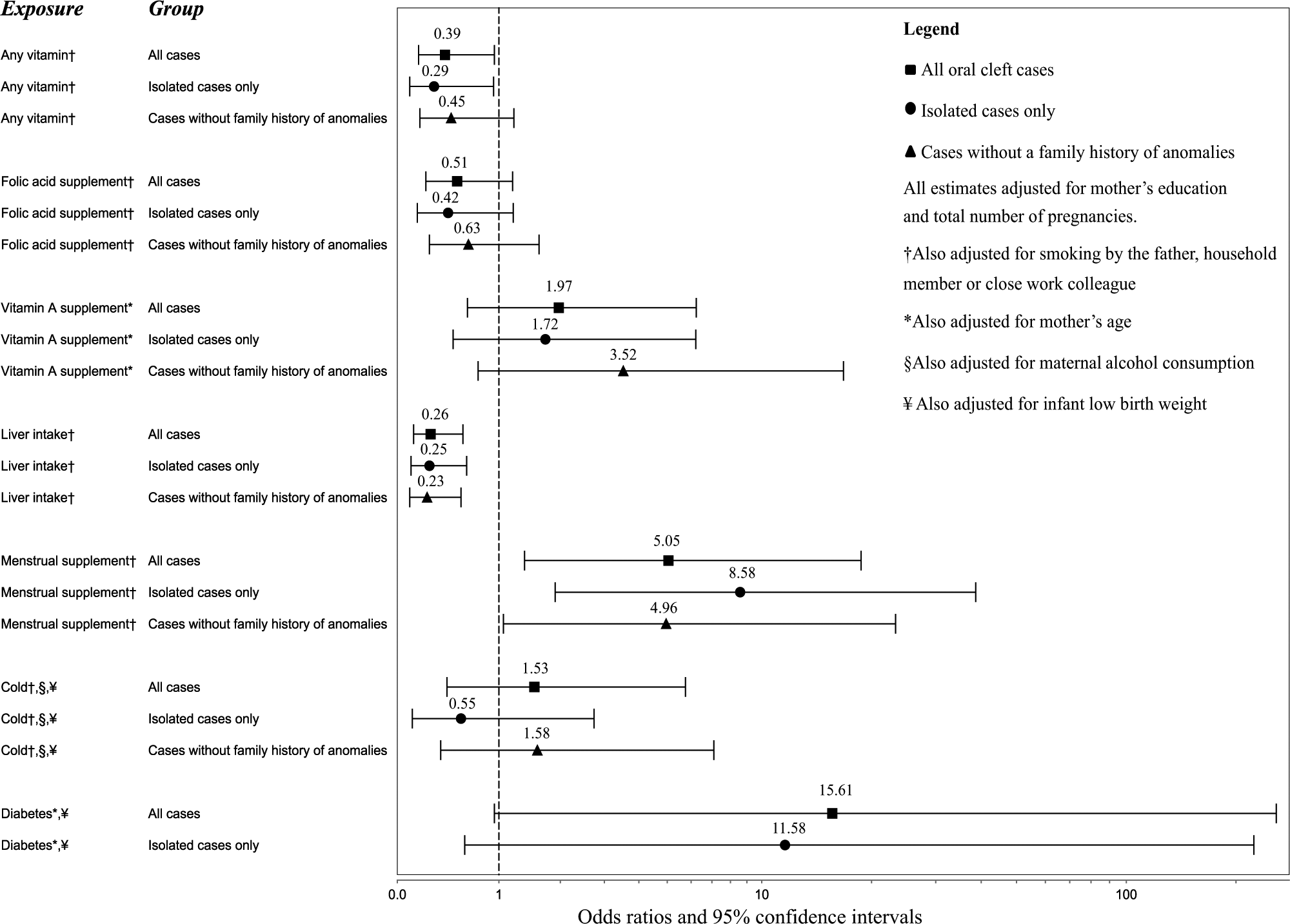
Adjusted estimates for all cases and select case subgroups
To assess whether the subset of cases with a genetic cause could have biased the risk estimates, we estimated unadjusted and adjusted associations for 2 case subsets: those with no family history of congenital anomalies and those with isolated CL ± P. In post hoc analyses, we also compared mothers who ate liver and took a vitamin supplement to those who did neither and estimated associations between low birth weight (LBW) and CL ± P. For subgroup analyses, we adjusted for the same confounders as identified for our primary analysis. All analyses were performed in Stata 11.0. This research conforms to the STROBE guidelines and was approved by the human ethics committees at Khon Kaen University and the University of Washington. Informed consent was obtained before study participation.
Results
CL ± P was more common among male than female infants (Table 1). Compared to controls, cases were more likely to be LBW and preterm and have other anomalies and a family history of anomalies. Proportionately, more cases than controls had mothers < 20 yrs old. Mother’s education level was slightly higher among cases, although controls had a slightly higher household income. The proportion of mothers who drank alcohol, smoked cigarettes, or were exposed to cigarette smoke in pregnancy was slightly higher for cases than for controls, but the number of exposed was small. No characteristics except LBW (p < .01) were statistically significantly different between cases and controls.
Fewer case mothers than control mothers reported taking any vitamin or a folic acid supplement (Table 2). Slightly more case mothers reported taking a vitamin A or retinoic acid supplement. Periconceptional liver intake was lower among case mothers. More case mothers reported taking a menstrual regulation supplement, having a cold, or having diabetes.
Because unadjusted and adjusted associations were similar, we focus on adjusted estimates for brevity (Table 2). Women who took a vitamin in the periconceptional period were 0.39 times as likely as those who did not to have a child with a CL ± P (p = .04). Women who reported taking a folic acid supplement in the periconceptional period were 0.51 times as likely to have an affected child than those who did not, although this finding was not statistically significant. Exposure to vitamin A supplement or retinoic acid was associated with a 1.97-fold increased risk of having a child with a CL ± P, although this estimate lacked statistical precision. We observed a strong, statistically stable inverse association of 0.26 between liver intake and CL ± P risk (p < .01). Mothers who took a menstrual regulation supplement (vs. those who did not) were at a 5-fold increased risk of having an affected child (p = .02). Our findings for having a cold or diabetes were in the direction expected but statistically imprecise.
Compared to all cases of CL ± P, estimates among subgroups of those with isolated CL ± P (n = 68) and those with no family history of anomalies (n = 66) were overall similar, although estimates among cases with isolated CL ± P tended to be a bit stronger (Figure and Appendix Table; Boyles et al., 2011). We were unable to estimate an adjusted association for diabetes for cases with no family history of anomalies, so this was not presented in the Figure. In post hoc analysis, we found that those who ate liver and took a vitamin in the periconceptional period were less likely to have an affected child compared to those who did not eat liver or take a vitamin (unadjusted odds ratio, 0.12; 95% CI: 0.15, 0.97; p = .047; adjusted odds ratio, 0.01; 95% CI: 0.0003, 0.40; p = .01). We adjusted for number of pregnancies, other smoke exposure, and mother’s education in 3 categories. Findings for LBW are in the Appendix.
Discussion
This is the first comparative study to examine micronutrients, supplement use, liver consumption, and oral clefts in Southeast Asia. We found that supplement use and liver intake in the periconceptional period decreases CL ± P risk. We also found that menstrual regulation supplement use increases CL ± P risk. These findings contribute to a growing body of global evidence suggesting that micronutrients play a role in the cause of CL ± P.
Our finding that periconceptional vitamin use decreases CL ± P risk is consistent with other studies in China, Brazil, and elsewhere (Loffredo et al., 2001; Jia et al., 2011). The specific micronutrients responsible for this association are unknown. Evidence suggests that folic acid may be protective, although in our study, estimates for folic acid supplements were not as strong as for all vitamin use. It may be that those who reported taking an unspecified vitamin took a folic acid–containing supplement. Participants who reported taking an unknown type of vitamin were classified as not having taken a folic acid supplement. This could have led to misclassification biasing our estimates on folic acid supplements toward finding no association.
We found that mothers who ate liver periconceptionally were at a decreased risk of having a child with a CL ± P compared to mothers who did not. A 3-oz portion of pork, beef, or veal liver contains more than 600% of the recommended dietary allowance for vitamins A and B12 and more than 50% for folate, zinc, and vitamin B6 (US Department of Agriculture, 2013). Low concentrations of micronutrients abundant in liver, including folate, zinc, and B vitamins, are linked to an increased risk of oral clefts in blood biomarker studies (van Rooij et al., 2003; Munger et al., 2004; Tamura et al., 2005). The only other study to examine this, conducted in Denmark, found no association between liver consumption and oral clefts but found that those with the highest levels of vitamin A estimated from liver intake and supplement use combined had a decreased CL ± P risk (Mitchell et al., 2003). A recent report suggests that the DASH dietary pattern plus multivitamin use may decrease oral cleft risk (La et al., 2013). These reports are consistent with our finding that dietary intake (liver) affects CL ± P risk and our post hoc finding that those who ate liver and took a vitamin supplement had a lower risk of having an affected child compared to those who took neither of these. We were unable to estimate the amount of specific micronutrients taken by mothers through diet or supplement use and did not have information on frequency and portion size of liver eaten. Thus, it remains unclear whether vitamin A or some other micronutrients could be responsible for these findings.
High-dose vitamin A (greater than 10,000 IU per day) is linked to an increased risk of malformations and cranial-neural-crest defects in some but not all studies (Rothman et al., 1995; Khoury et al., 1996; Shaw et al., 1996; Mitchell et al., 2003). It is posited that vitamin A is teratogenic at low or high levels, although specific thresholds are unknown (Ackermans et al., 2011). Our finding of an increased risk with vitamin A supplement use, though statistically imprecise, was opposite of our finding for liver consumption, perhaps because vitamin A from supplements increases plasma concentrations of teratogenic metabolites of vitamin A whereas liver does not (Buss et al., 1994). Our finding is consistent with evidence showing that an increased risk of malformations with high-dose vitamin A is primarily attributable to supplement use (Rothman et al., 1995). If liver is found to be protective in other studies, careful consideration of recommendations related to vitamin A for primary prevention would need to be undertaken.
We are the first to report that menstrual regulation supplement use increases CL ± P risk. Menstrual regulation supplements in Thailand are herbal remedies that come in pills, herbal packets, or liquid. Liquid supplements may contain alcohol. Women who take this supplement could be ingesting alcohol during the first weeks of gestation. High-dose alcohol alters normal embryogenesis and is a known risk factor for oral clefts and one explanation for this association (Munger et al., 1996; DeRoo et al., 2008). Chinese herbs (e.g., curcuma comosa, angelica sinensis) in some supplements may have estrogenic effects, which could alter oral cleft risk (Winuthayanon et al., 2009; Natural Standard, 2013). Some herbs (angelica sinesis) may be prepared in or combined with alcohol (Natural Standard, 2013). The Appendix contains more background information on our rationale for examining menstrual regulation supplements. The extent to which similar supplements are used in Asian populations should be investigated, as this may be an important but unrecognized risk factor for oral clefts in Asian populations.
There are several strengths and limitations to our study. Our results are consistent with findings from studies in predominantly high-income countries and extend knowledge on environmental risk factors to Southeast Asia. That subgroup analyses were similar to overall estimates suggests that the inclusion of cases with genetic conditions or other anomalies did not materially affect our findings. These data were self-reported. Because of missing data, we were not able to calculate frequency or dose of vitamin use. Though less than ideal, other studies on the cause of oral clefts employ similar periconceptional measures of supplement use (Johnson and Little, 2008). Case mothers may have recalled their pregnancy history more completely than controls. Studies of recall bias in pregnancy research in North America have found that this is not a major problem (Mackenzie and Lippman, 1989; Infante-Rivard and Jacques, 2000). The extent to which recall bias affects Thai women is unknown. Given estimates of the birth prevalence of oral clefts in Thailand and number of live births in the recruitment provinces, we suspect that we missed cases during recruitment due to practical and logistic constraints. There is no reason to believe that the recruits were systematically different from those inadvertently missed.
This investigation is the first case-control study to examine micronutrients, supplement use, and environmental risk factors for oral clefts in Thailand. Our finding that vitamin use reduces the risk of oral clefts in Thailand is consistent with a growing body of literature from developing countries suggesting that multivitamins may be an effective global preventive strategy for oral clefts. Liver consumption or menstrual regulation supplement use may have relevance in certain countries where these exposures are prevalent. This study demonstrates that future global studies of the cause of oral clefts should include and examine the timing, frequency, and dose of supplements, micronutrients, and dietary patterns to inform efforts for global prevention.
Footnotes
Acknowledgements
We thank Suteera Pradubwong for her assistance with study logistics. We thank the Plastic Surgery Education Foundation for grant support and the Center of Cleft Lip–Cleft Palate and Craniofacial Deformities, Khon Kaen University, in association with the Tawanchai Project.
Dr. McKinney’s time was funded by the
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.