
Abstract
Periodontitis is an inflammatory disease that causes loss of the tooth-supporting apparatus, including periodontal ligament, cementum, and alveolar bone. A broad range of treatment options is currently available to restore the structure and function of the periodontal tissues. A regenerative approach, among others, is now considered the most promising paradigm for this purpose, harnessing the unique properties of stem cells. How to make full use of the body’s innate regenerative capacity is thus a key issue. While stem cells and bioactive factors are essential components in the regenerative processes, matrices play pivotal roles in recapitulating stem cell functions and potentiating therapeutic actions of bioactive molecules. Moreover, the positions of appropriate bioactive matrices relative to the injury site may stimulate the innate regenerative stem cell populations, removing the need to deliver cells that have been manipulated outside of the body. In this topical review, we update views on advanced designs of biomatrices—including mimicking of the native extracellular matrix, providing mechanical stimulation, activating cell-driven matrices, and delivering bioactive factors in a controllable manner—which are ultimately useful for the regenerative therapy of periodontal tissues.
Keywords
Overview
Structure of Periodontal Tissues
Periodontal tissue surrounds and supports the tooth structure and consists of 4 components: gingiva, cementum, alveolar bone, and periodontal ligament (Fig. 1). The gingiva is a mucous membrane covering the tooth-bearing border of the jaw. The crown enamel and the root cementum meet at the marginal gingival (cemento-enamel junction), and the space between these structures is termed the gingival sulcus. The cementum is a hard tissue that covers the root dentin and anchors one side of the periodontal ligament (PDL) fibers. The other side of the PDL interfaces with the alveolar bone. Alveolar bone, which has properties similar to those of bone elsewhere in the body, supports the teeth and the gingival tissues. The root side of the alveolar bone consists of a thin layer of dense compact bone, appearing as a thin radiopaque line surrounding the root, called the lamina dura, into which the Sharpey’s fibers of the PDL insert deeply (Nanci and Bosshardt, 2006). The PDL consists of functionally oriented collagen fibers (primary), elastic fibers (secondary) that have a vaguely anarchic orientation arranged around vessels, reticulin and oxitalan fibers, blood and lymphatic vessels, and nerves. As a functional unit, the PDL provides tooth fixation in the socket via dense connective tissue and is usually exposed to mechanical forces during occlusion and mastication. The functional stimulus of the mechanical forces to PDL and alveolar bone play an important role in the biological properties of periodontal cells to maintain healthy physiology (Weidenhamer and Tranquillo, 2013). Recently, several studies have reported that mechanical forces affect the synthesis of numerous mechanoresponsive osteotropic cytokines and growth factors, which are beneficial in mediating cellular and molecular events (Marchesan et al., 2011).
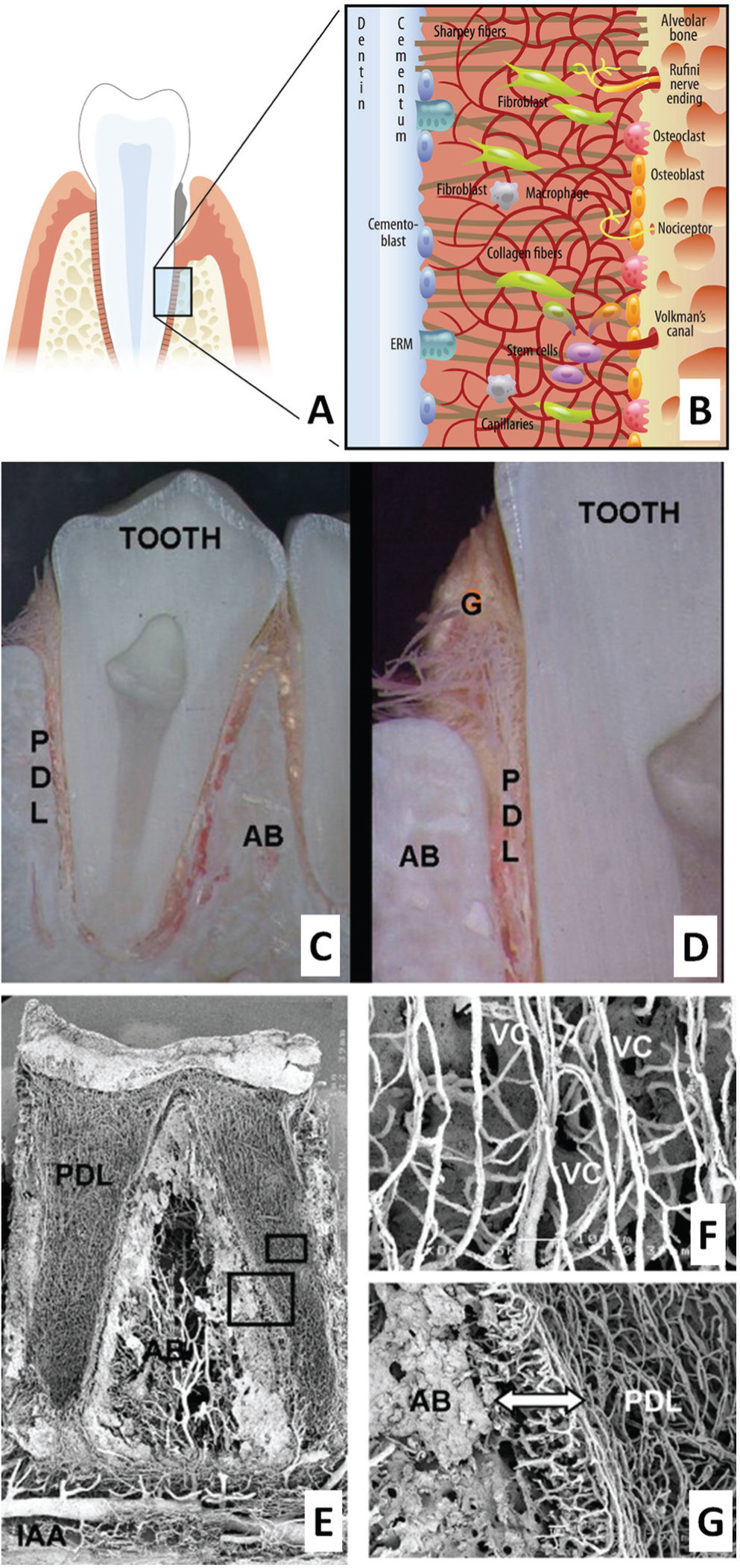
Structure of periodontal tissues.
Periodontal Diseases/Damage and Current Surgical Approaches
Periodontitis is an inflammation with destruction of the elements of the periodontium. It is characterized by the formation of a periodontal pocket by (i) irreversible destruction of the junctional epithelium from the tooth surface, (ii) loss of periodontal attachment between the cementum and alveolar bone, and (iii) pathologic deepening of the gingival sulcus (Pihlstrom et al., 2005). The ultimate goal in the treatment of periodontal disease is to use periodontal-regenerative techniques to achieve restoration of all periodontal attachment apparatus, including soft (gingival attachment and periodontal ligament) and mineralized (alveolar bone and cementum) tissues, to their original form, function, and consistency. Many researchers have provided evidence that most periodontal diseases can be treated with a broad range of interventions, but thus far, periodontal regeneration has not been satisfactory in humans (Chen et al., 2010).
Bone regeneration, fibrous connective tissue formation, and new attachment of connective tissue from the tooth root surface to bone are critical for successful periodontal regeneration. For the past few decades, some effective surgical techniques have been developed for periodontal regeneration. These include bone grafting, root biomodification, guided tissue regeneration (GTR), and a combinatory approach with biological factors (Darby and Morris, 2013). While those periodontal therapies have been widely used and documented, the clinical outcome is still not optimal for many reasons.
Importance of Regenerative Approaches and Biomatrices for Periodontal Tissues
There is a huge conceptual shift from restoration to regeneration of tooth structure, including periodontal tissues. The discovery of stem cells, particularly mesenchymal stem cells (MSCs), spurred interest in regenerative therapies for damaged and diseased periodontal tissues (Mao et al., 2006; Satija et al., 2007). MSCs, residing in many adult tissues, are stimulated to migrate to injured sites and to acquire active biological functions for repair and regenerative processes, such as immune regulation, tissue-specific differentiation, and secretion of a cocktail of cytokines and growth factors (Lin et al., 2009). This innate regenerative capacity via MSCs is often limited in the injured and diseased sites, particularly due to the severity of disease, large volume of defects, and the patient’s health conditions (Kaigler et al., 2013). Therefore, aiming to help MSCs function properly in vivo to regenerate tissues is a rational strategy, and this is possible through re-establishment of the microenvironments of MSCs.
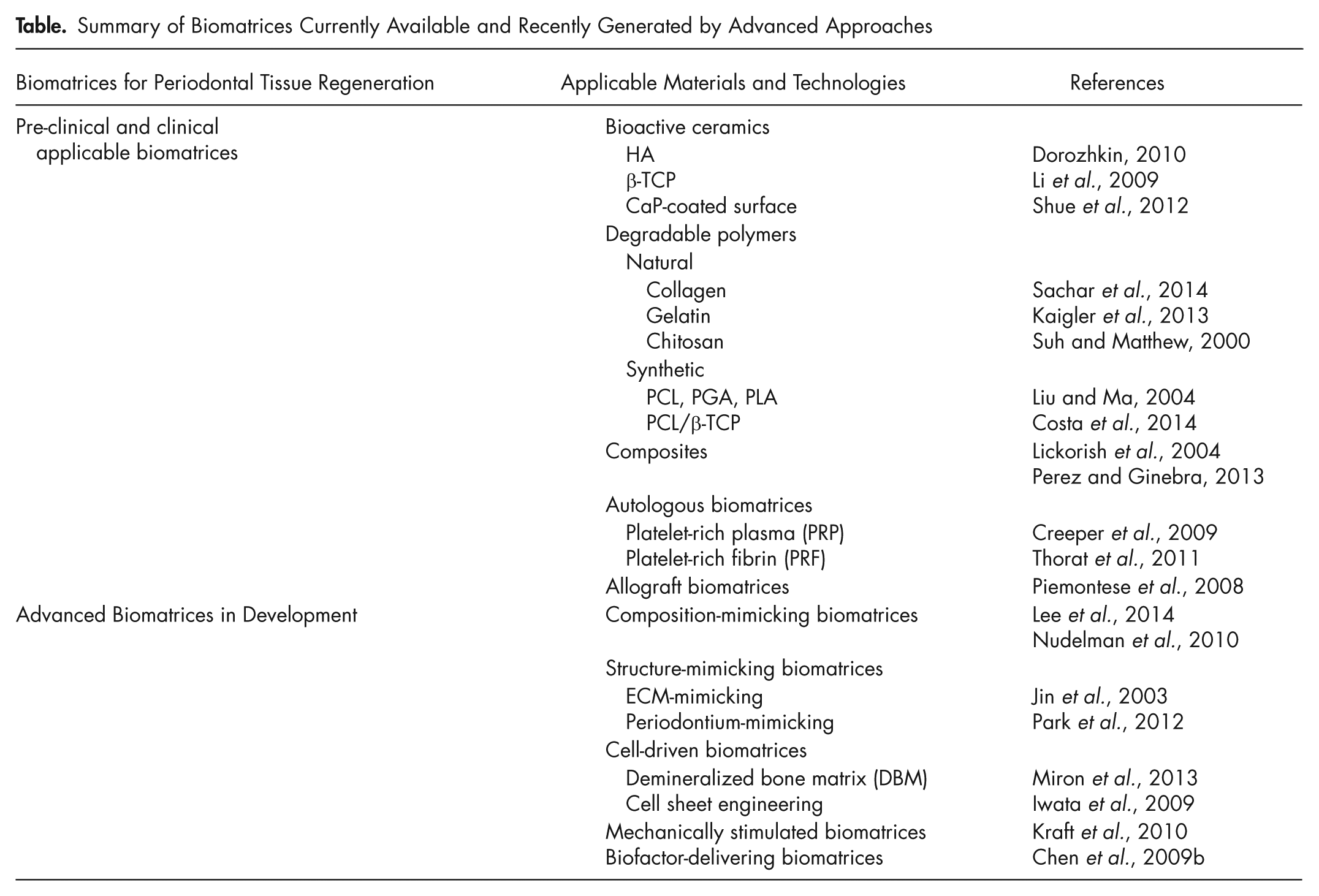
Biomatrices play crucial roles in reconditioning the microenvironments of stem cells, providing key matrix cues for anchoring and spreading, to support self-renewal and appropriate differentiation (Horst et al., 2012). As mentioned above, the grafting method is in fact the most clinically available technique utilizing matrices; it is simple, yet can provide suitable environments to support cell-mediated repair and regeneration. Motivated by technological advances and the regenerative concept, several functional biomatrix designs have been proposed. Control over the physical and chemical traits of the matrix surface determines cellular recognition to ligands and the consequent fate of cells (Lee et al., 2014). A surface that mimics native tissue extracellular matrix (ECM) in terms of composition, topography, and rigidity is better recognizable to stem cells and more effective in driving them to differentiate into target tissues. Some recent technological advances have facilitated the development of tissue-mimicking designs of biomatrices (Jin et al., 2003; Liu and Ma, 2004; Liu et al., 2006). Cell-secreted biomatrices are also considered a promising platform, since they produce new biologic tissue similar to that of native ECM, ultimately enabling the ex vivo production of tissue-engineered constructs (Iwata et al., 2009). Mechanical regulation of stem cells is another important yet often underestimated consideration, particularly in periodontal tissues, since they have a dynamic mechanical environment, which is key for maintaining tissue functions (Kraft et al., 2010). Last, the biomatrices that exogenously deliver bioactive factors in a controllable manner will improve the regenerative capacity of tissues, due to a range of potential therapeutic actions including anti-inflammation, enhanced progenitor cell recruitment, angiogenesis, and tissue differentiation. The Table summarizes the biomatrices currently available and recently generated by advanced approaches, which will be discussed in detail in this review.
Summary of Biomatrices Currently Available and Recently Generated by Advanced Approaches
Advanced Biomatrix Designs
Compositional Control to Mimic Native ECMs
While many different biomaterials are currently available for periodontal regeneration—including bioactive ceramics, biodegradable polymers, composites, allografts, and autologous materials (Appendix)—designing biomatrices that mimic native tissue ECMs, particularly the composition, is of importance. The bone phase is particularly sophisticated, with many organic ingredients organized with inorganic mineral crystals. A primary route is the mimicking of mineral-phase hydroxyapatite (HA), which is enabled by the biomimetic synthesis of HA, including low-temperature solution-based methods (Tas, 2000; Moreau et al., 2009). HA with poorly crystallized form has better bone bioactivity, such as protein adsorption, cellular osteogenesis, bone formation, and bone remodeling, due to its higher dissolution properties (Sawyer et al., 2005). However, most synthetic routes involve only ionic-buffered medium in the absence of biological proteins. Since the mineralization of HA in vivo is mainly induced by cellular processes and the interactions with bone ECM proteins, such as collagen, osteopontin, and osteocalcin (Nudelman et al., 2010), the biomimetic route to prepare HA needs to involve those kinds of proteins. Some studies have utilized protein molecules in the creation of HA minerals (He et al., 2003). Moreover, in situ mineralization of HA within the collagen fibrils is an effective means of preparing bone-ECM-mimicking biomatrices (Lickorish et al., 2004).
In addition to tailoring bulk properties of biomatrices, controlling the surface to mimic native bone ECM composition is an attractive approach because cells first recognize the surface to adopt subsequent behaviors like osteogenesis and bone formation. In fact, many types of bone ECM proteins (e.g., fibronectin and collagen) have been introduced to the surfaces of scaffolds made from biopolymers and bioceramics by either weak chemical interactions or tight covalent links (Teixeira et al., 2010). One recent approach involving a fibronectin-osteocalcin fusion protein is noteworthy, where the fusion protein was designed to accelerate initial stem cell adhesion via fibronectin and subsequently to accelerate osteogenesis and mineralization by osteocalcin at a much later stage. Importantly, tethering of the fusion protein was possible thanks to the affinity binding of osteocalcin to the HA crystal lattice, i.e., molecular recognition of carboxyglutamic acid sequences in osteocalcin to 5 calcium ions in HA (Lee et al., 2014). Aside from bone, a recent attempt to construct a cementum-like biomineralized layer has also been carried out (Gungormus et al., 2012), where amelogenin-derived peptides were used to control HA mineralization and to mimic ECM composition of cementum. The specific region identified showed the formation of a mineral phase that supported attachment of periodontal ligament cells. Fig. 2 depicts the aforementioned approaches to compositional mimicking biomatrices.
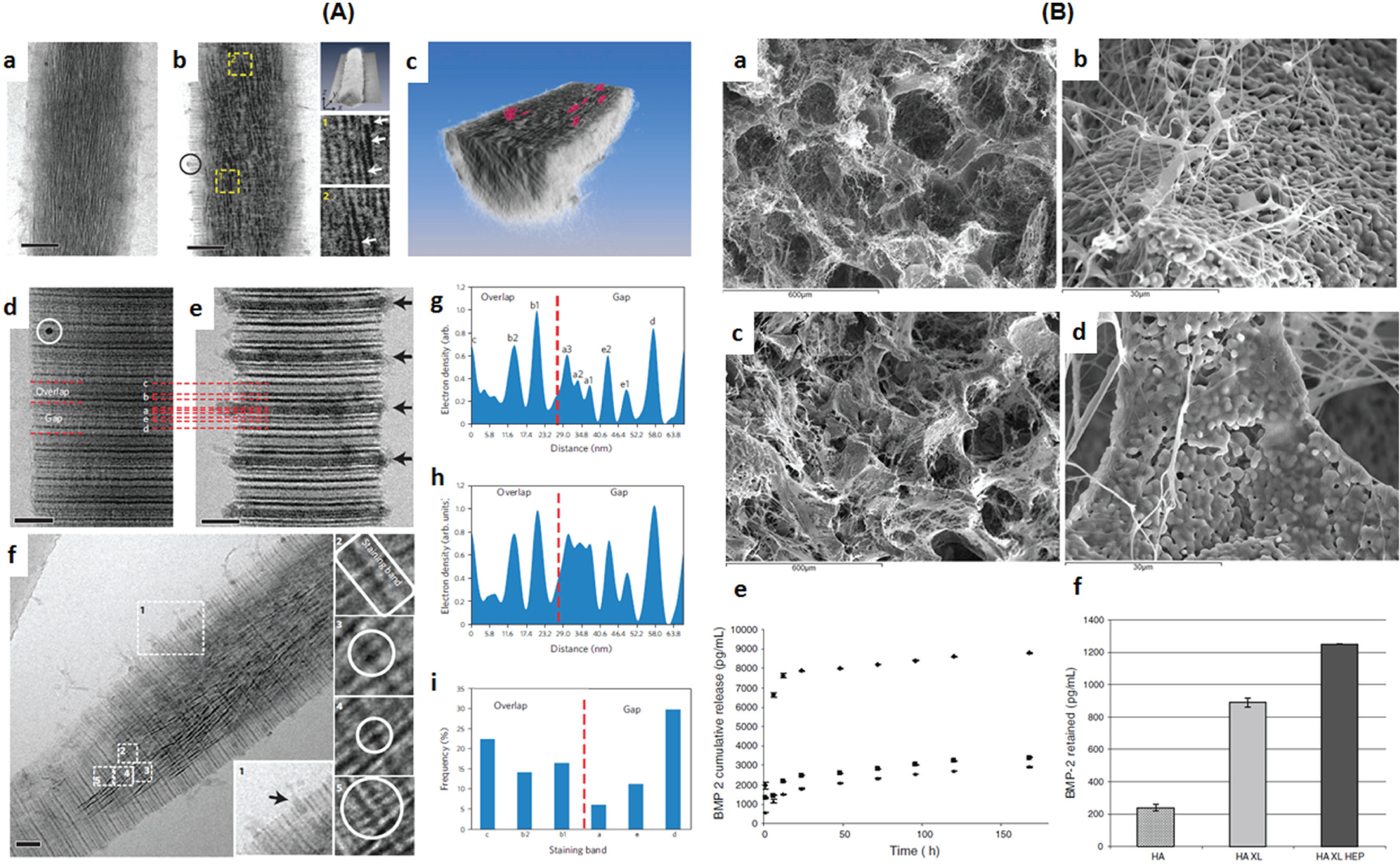
Biomatrices designed to mimic the native extracellular matrix (ECM) compositions.
Advanced Technologies to Mimic the Nano-/Microstructure of Native ECMs
The main challenge in periodontal tissue engineering is the hierarchical formation of sub-micron-scaled, multiple interfaces with maturation of alveolar bone, PDL orientation, and tissue integration. Recently, architecturally mimicking or anatomically adaptable constructs have been highlighted for periodontal tissue regeneration. Technological advancements have led to the development of structural mimicry within 2 types of scaffolds; ECM-mimicking nanofibrous scaffolds, and periodontium-mimicking scaffolds with nanoscopic and microscopic focuses.
ECM is the natural cell-supportive platform with nanofibrous structures and different types of proteins to promote cell activities (Wei et al., 2007). By different methods, including electrospinning, phase separation, and peptide self-assembly, a nanofibrous form of polymeric scaffolds with different compositions has been successfully generated (Jin et al., 2003). The structurally mimicking ECM constructs are often combined with bioactive molecules on the surface or within the structure to improve cellular activities (Franceschi, 2005). The nanofibrous structured matrices supported cells related to periodontal tissues, including PDL cells, bone cells, and stem cells, and stimulated them to engage in proper ECM synthesis and maturation, even better than their densely structured and/or microfibrous counterparts (Jin et al., 2003).
Mimicking perpendicular or oblique orientations of PDL in the 200- to 300-micron PDL interface has been challenging by conventional methods. The spatially oriented PDL plays a significant role in mechanical functioning against regular occlusal or masticatory loading. Recently, however, computer-designed 3D printing technology made possible the creation of microscopically tailored scaffolds to anchor tooth roots to alveolar bone surfaces (Park et al., 2014). The developed scaffolds microscopically mimicked the architecture of natural PDL, and successfully guided the orientation of regenerated fibrous connective tissues, perpendicularly and obliquely. The image-based, fiber-guiding scaffolds resulted in: (i) bone tissue formation; (ii) PDL orientation with cementogenesis on the tooth root surface; and (iii) functional regeneration of periodontal complexes, highlighting the advancement of current state-of-the-art technology to mimic hierarchical periodontal tissue structure (Park et al., 2014). The aforementioned approaches to structural mimicking biomatrices are illustrated in Fig. 3.
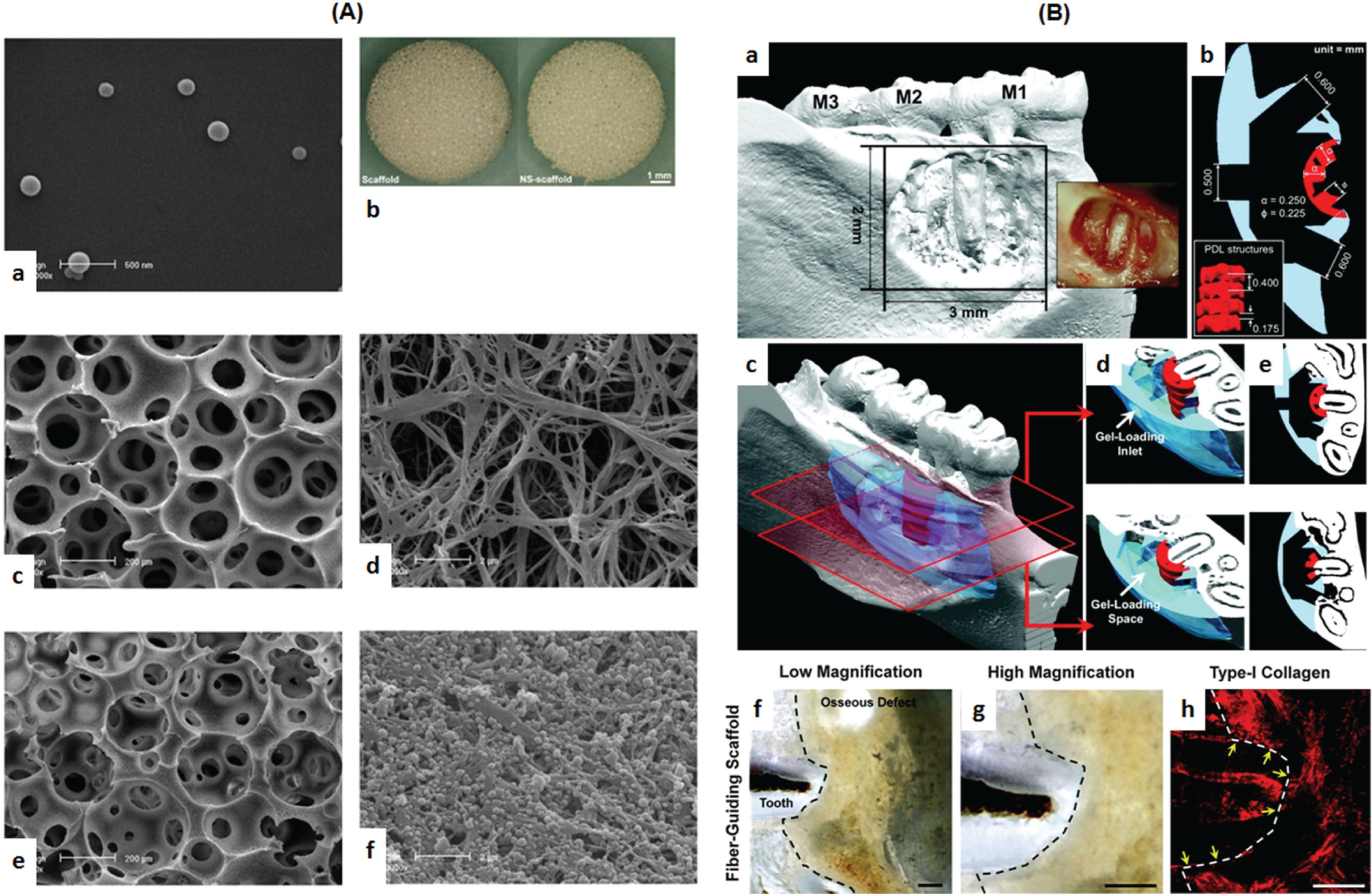
Biomatrices designed to mimic the native extracellular matrix (ECM) micro/nano-structures.
Cell-driven Biomatrices
Among the sources of cell-driven biomatrices, demineralized freeze-dried bone matrix (DFDBM) has been widely utilized for bone formation and periodontal treatments, pre-clinically and clinically, due to its clinical safety and capacity for bone formation, osteoconductivity, and osteoinductivity (Gurinsky et al., 2004; Piemontese et al., 2008; Banjar and Mealey, 2013). Moreover, commercialized DFDBMs have been combined with various biological factors for periodontal tissue regeneration, including enamel matrix derivative (EMD) (Gurinsky et al., 2004; Miron et al., 2013), BMP-2 (Schwartz et al., 1998), platelet-rich plasma (PRP) (Piemontese et al., 2008), and platelet-rich fibrin (PRF) (Bansal and Bharti, 2013).
Demineralized dentin was developed similarly. The demineralized dentin matrix promoted periodontal ligament cell proliferation and differentiation, since it contains a large amount of growth factors, and when exogeneous growth factors such as BMP were combined, the demineralized dentin matrix enhanced periodontal regeneration, leading to a cementum-like tissue formation (Miyaji et al., 2010).
Cell-sheet engineering has great promise as a tissue-engineering strategy (Iwata et al., 2009). The engineered PDL cell sheets were layered and placed on the periodontal defect site in a canine model for periodontal complex regeneration (Tsumanuma et al., 2011). The cell culture plates were chemically modified by means of a temperature-responsive polymer, poly(N-isopropylacrylamide) (pNIPAAm). During cell culture at 35° to 37°C, cell-cell and cell-matrix interactions were generated to form a mono-layered sheet. However, when the polymer-coated surface was incubated at 32°C, polymer chains became hydrophilic and too swollen to push the cultured cell sheet from the surface. For the periodontal complex, three-layered PDL cell sheets were placed on the exposed tooth-root surface, and then β-tricalcium phosphate (β-TCP) was filled in the canine defect (Iwata et al., 2009). The methodology demonstrates surgical simplicity, effective dimensional compartmentalization (bone-PDL-tooth), and interfacial isolation for individual tissue growth and maturation, with high clinical relevance (Iwata et al., 2009).
Recently, advanced combinatory technologies assembling cell sheets with 3D scaffolds have also been reported to construct periodontal complex mimics (Vaquette et al., 2012, 2013). Constructs were composed of a bone compartment manufactured by fused deposition modeling (FDM), three-layered cell sheets for PDL, and then an electrospun poly-ϵ-caprolactone (PCL) membrane between bone and PDL interfaces to provide physical stability to the cell sheets. The periodontium-mimicking complexes were transplanted to induce limited hierarchical periodontal tissue regeneration ectopically (Vaquette et al., 2012). To improve osteoconductive properties, FDM PCL scaffolds were surface-modified with bone-mimetic calcium phosphate (CaP). These engineered scaffolds enhanced bone infiltration, vascularization, and fibrous tissue attachment to the mineralized tissue surface featuring tooth-supportive structures (Costa et al., 2014). Combinatory technology thus offers improved spatially predictable and controllable tissue compartmentalization with micron-/nano-scaled, specific periodontal interfaces (Costa et al., 2014). Fig. 4 presents the exemplar studies on creating cell-driven biomatrices.
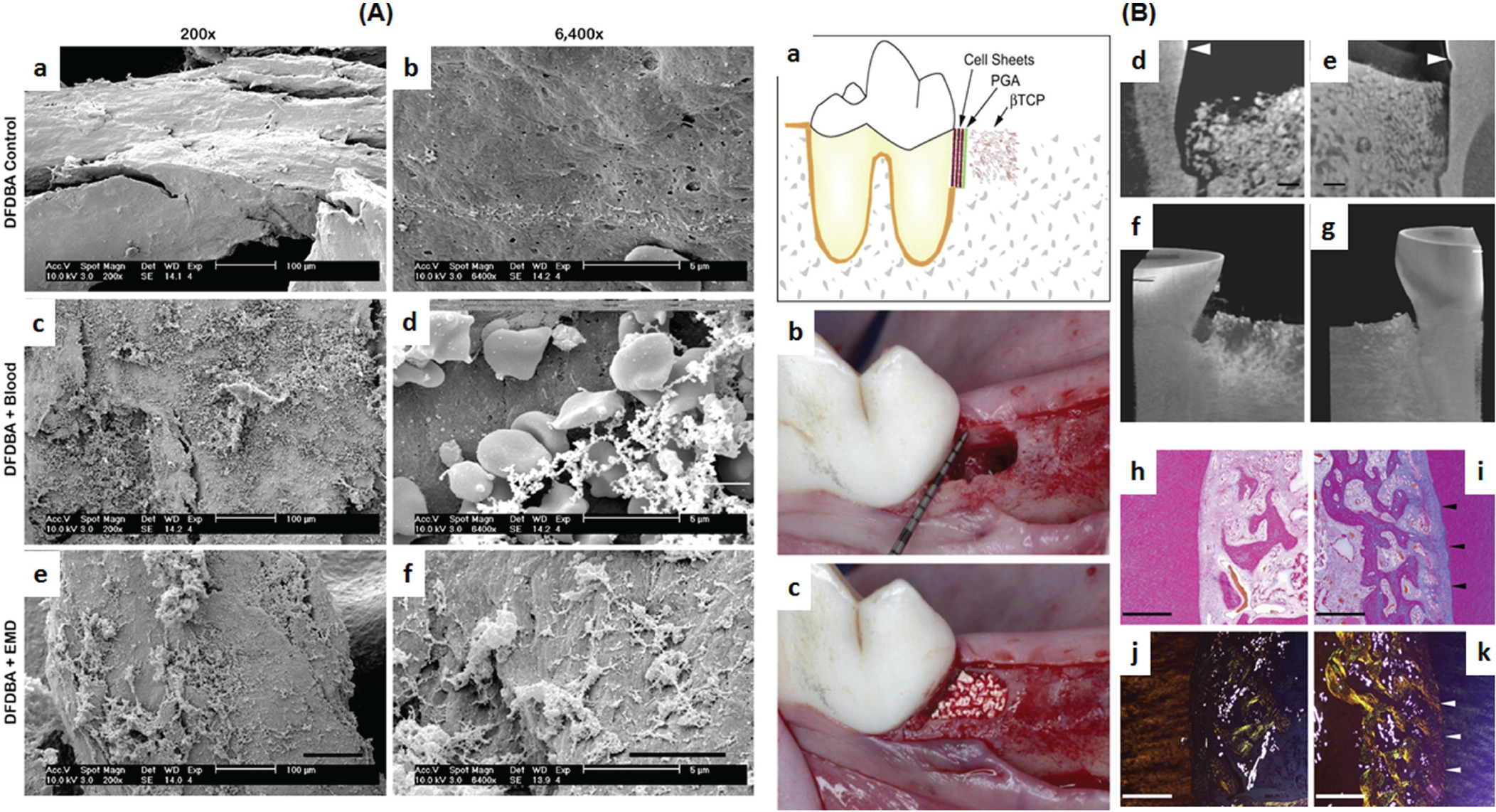
Biomatrices driven by cells.
Mechanically Stimulated Biomatrices
Recently, mechanical stimuli have been highlighted in the repair and regeneration of tissues, including periodontal tissues. The mechanical loads significantly alter the PDL and bone responses, activating tissue remodeling at the periodontal interfaces and leading to bone resorption through osteoclastic factor release (Mayahara et al., 2007). In vitro mechanical shear stress has been shown to promote the osteogenic differentiation of dental stem cells, including those derived from pulp, alveolar bone, and PDL (Kraft et al., 2010). However, most in vitro studies have focused on osteogenic differentiation of different dental stem cells rather than on ligament or bone-ligament interfacial tissue regeneration. Because of complicated, sub-micron interfacial structures, periodontal tissue regeneration requires precise control of stem cell activation and integration into multiple tissues, which needs further study. Moreover, most studies on the effects of mechanical stimuli on stem cells have been performed in 2D culture dishes (Raab et al., 2010), which do not accurately translate to 3D gel-like tissue environments. Therefore, further investigation into mechanical-cell interactions needs to be carried out under environmental conditions analogous to native tissue characteristics, such as 3D hydrogel matrices with matched stiffness (Raab et al., 2010). Ultimately, the combinatory approach of biomimetic matrices with mechanical stimuli may deliver optimal culture conditions for stem cells to direct their fate into tissue-equivalent constructs ex vivo. The mechanical pre-stimulation and pre-differentiation of stem cells on biomimetic matrices prior to cell transplantation will be the next step to generate stem-cell-based engineered periodontal tissues that better mimic in vivo microenvironments. This remains a promising future technology for periodontal tissue regeneration.
Biofactor-delivering Biomatrices
While the immobile ECM molecules are the first design criterion producing biomimetic scaffolds, a cocktail of soluble bioactive molecules, such as growth factors and cytokines, should also be considered as critical in the regeneration of periodontal tissues. Therefore, strategies to exogenously deliver bioactive molecules provide a rational platform for the creation of therapeutic biomatrices. Above all, the bioactive molecules need to be protected from the in vivo environment and released at specific time points during the healing process.
Some possible elegant designs for this protective and controllable delivery system have recently been proposed. Fig. 5 summarizes the designs to produce therapeutic biomatrices for periodontal regeneration. In fact, the simplest approach is to tether the molecules to the surfaces of biomatrices. This approach is relevant when rapid release is needed, leading to direct contact with the cells and consequent initial cellular activation (Cooke et al., 2006). While surface-tethering of bioactive molecules can be improved via stronger bonds to slow the release rate, a better approach is to incorporate within the biomatrices. However, many types of biomatrix do not allow for safe incorporation, mainly due to the necessary processing conditions, e.g., the use of organic solvents and high-temperature processes, which limit the incorporation of bioactive molecules in native form (Chen et al., 2010). In situ gelling natural polymers and self-setting inorganic cements are some candidates for this direct incorporation of bioactive molecules. Therefore, a more general and powerful method to incorporate bioactive molecules within the structure of biomatrices has been proposed. Micro-/nanoparticles encapsulating the molecules can be combined with biomatrices. Alginate microspheres preloaded with BMP-6 were incorporated into chitosan porous matrix, enabling more sustained release of the BMP-6 and stimulation of osteogenesis by MSCs for periodontal tissue engineering (Soran et al., 2012). Along with the proteins, genetic molecules have also been delivered to cells via viral or non-viral vectors for periodontal regeneration (Chen et al., 2009a). The target gene sequences are encoded and delivered by modified vectors for internalization of genetic information. Gene-transfected cells have already been reprogrammed for local production of the proteins desired for periodontal tissue regeneration (Taba et al., 2005).
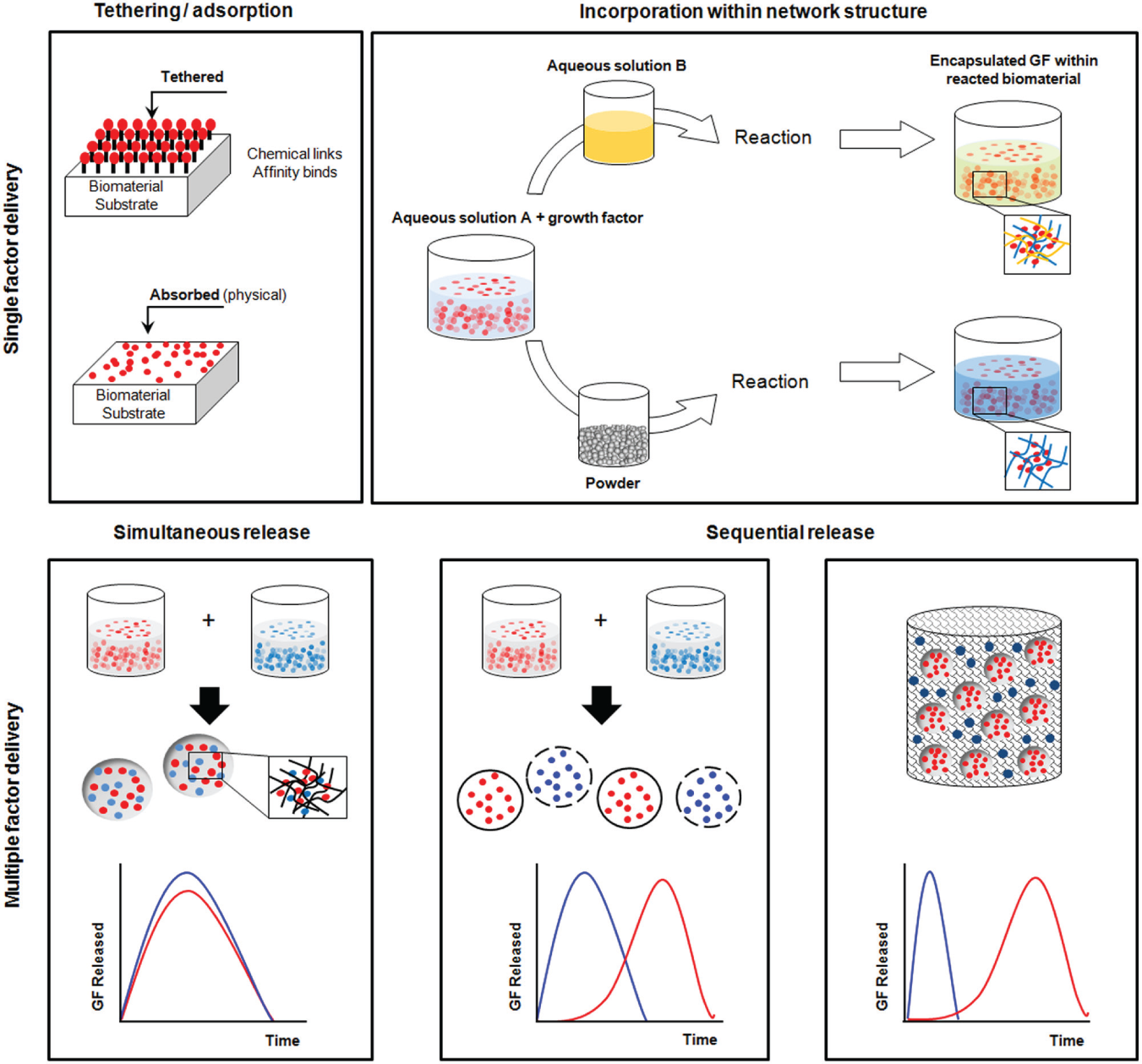
Designs of therapeutic biomatrices to load and deliver bioactive molecules.
In addition to single-factor delivery, the delivery of multiple bioactive molecules is gaining great interest for the functional design of therapeutic biomatrices. Because the tissue repair and regeneration process is a complex series of events involving growth factors and cytokines that have temporal and dose-dependent activities, delivery of multiple factors in a controlled manner is a rational approach. Administration of 2 different growth factors often involves their partitioned incorporation within micro-/nanocarriers, enabling the simultaneous release of 2 different factors. More advanced is the use of different nano-/microcarriers, where the carriers have different release kinetics based on properties such as degradability, size, and permeability, enabling the independent/sequential release of molecules (Chen et al., 2009b). For instance, scaffolds prepared by the incorporation of microspheres that contain BMP-2 or insulin-like growth factor (IGF)-1 facilitated prolonged release for both of the growth factors in an independent manner (Chen et al., 2009b). A combinatory approach of using nano-/microcarriers loaded with one factor and scaffolding biomatrices loaded with the other factor is also possible, to allow for sequential delivery (Yilgor et al., 2009). In such delivery systems, one factor is released rapidly, while the other factor is released much more slowly, enabling the bi-phasic delivery of factors. This sequential delivery concept can be profoundly utilized in periodontal regeneration via delivery of anti-inflammatory mediators in the initial phase, followed by regenerative molecules later, or angiogenic factors followed by osteogenic mediators at a later time, or chemotactic recruitment of stem cells initially, followed by stimulation of their tissue-specific differentiation (Yilgor et al., 2009; Sundararaj et al., 2013). For example, the use of 2 different nanocapsules with different degradation rates made of PLGA and PHVB allowed for a sequential release of BMP-2 followed by BMP-7 (Yilgor et al., 2009). Additional recent work described an elegant design made of multilayer materials that allowed for the release of 4 different drugs in a degradation-dependent sequential manner (Sundararaj et al., 2013). While multiple and sequential delivery strategy has not yet been fully realized for periodontal tissue regeneration, the concept can be potentially useful to achieve significant therapeutic effects, improving the regenerative capacity of damaged and diseased periodontal tissues.
Concluding Remarks
A regenerative approach utilizing stem cells holds great promise for the successful treatment of periodontal tissues, including periodontal ligament, cementum, and alveolar bone. The role of biomatrices is thus of special importance in guiding, altering, and regulating the behaviors of stem cells toward regenerative processes. Although clinically proven techniques, including bone grafting and guided tissue regeneration, use conventional available biomatrices, advanced biomatrices that ultimately function to engage in anti-inflammation, stem cell homing, angiogenesis, and bone/PDL integration are required for successful periodontal regeneration.
Biomimetic approaches to native periodontal tissue ECMs in terms of composition and tissue architecture will possibly create biomatrices that have mechanical and biological properties comparable with those of autologous tissues. In this way, technological advances contribute significantly to the design of sophisticated tissue architecture at the micro-/nanoscale. Not only are structural ECM components important, but also soluble molecules such as growth factors, which are essential components of microenvironments that promote tissue repair and regeneration. Multiple biological factors are involved and need to be delivered in the correct temporal fashion at relevant doses, which can be reflected in the design of biomatrices, to enable therapeutically active biomatrices to perform. Conversely, designed biomatrices synthesized by living cells, i.e., stem-cell-derived biomatrices, are considered to better mimic the native ECMs where the cells’ innate capacity for ECM generation can be fully utilized, ultimately creating tissue-equivalent products. For this, biomimetic and therapeutic ECMs can better function in driving stem cell differentiation toward lineages of interest. Another consideration, important yet often ignored, is the mechanical-stimulating strategy, i.e., to mimic the in vivo mechanically dynamic environments to achieve ex vivo functional tissues cultured with stem cells.
The designs and technologies for biomatrix engineering outlined herein offer considerable promise for clinical application in the future. However, further advancements are needed to unite fundamental science, pathophysiology, and engineering capabilities for the successful generation of complex periodontal tissue architectures for regenerative therapies.
Footnotes
This work was supported by the Priority Research Centers Program through the National Research Foundation of Korea (NRF) funded by the
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.