
Abstract
Although there have been major improvements in oral health, with remarkable advances in the prevention and management of oral diseases, globally, inequalities persist between urban and rural communities. These inequalities exist in the distribution of oral health services, accessibility, utilization, treatment outcomes, oral health knowledge and practices, health insurance coverage, oral health–related quality of life, and prevalence of oral diseases, among others. People living in rural areas are likely to be poorer, be less health literate, have more caries, have fewer teeth, have no health insurance coverage, and have less money to spend on dental care than persons living in urban areas. Rural areas are often associated with lower education levels, which in turn have been found to be related to lower levels of health literacy and poor use of health care services. These factors have an impact on oral health care, service delivery, and research. Hence, unmet dental care remains one of the most urgent health care needs in these communities. We highlight some of the conceptual issues relating to urban-rural inequalities in oral health, especially in the African and Middle East Region (AMER). Actions to reduce oral health inequalities and ameliorate rural-urban disparity are necessary both within the health sector and the wider policy environment. Recommended actions include population-specific oral health promotion programs, measures aimed at increasing access to oral health services in rural areas, integration of oral health into existing primary health care services, and support for research aimed at informing policy on the social determinants of health. Concerted efforts must be made by all stakeholders (governments, health care workforce, organizations, and communities) to reduce disparities and improve oral health outcomes in underserved populations.
Introduction
“Health inequality is the generic term used to designate differences, variations, and disparities in the health achievements of individuals and groups,” while “health inequity refers to those inequalities in health that are deemed to be unfair or stemming from some form of injustice” (Kawachi et al. 2002). Health disparities are population-specific health differences (in the prevalence of disease, health outcomes, or access to health care) that are avoidable and unfair when regarded from social justice, ethical, and human rights perspectives (Lee and Divaris 2014). Although there have been major improvements in oral health in the past decades, with research leading to remarkable advances in the prevention and treatment of disease, inequalities still remain, with a marked social gradient in oral health, similar to that in general health (Sgan-Cohen et al. 2013). The current pattern of oral disease reflects distinct risk profiles across countries related to living conditions, behavioral and environmental factors, oral health systems, and implementation of schemes to prevent oral disease (Pitts et al. 2011). Globally, the greatest burden of oral disease lies on disadvantaged and poor populations. There are significant differences in the distribution of oral health services, accessibility, utilization, and outcomes between urban and rural areas of both developing and developed countries (Beaglehole et al. 2009; Bayne et al. 2013). Some of the prominent factors among the rural-urban variations include differences in preventive oral health knowledge and practices, including dental visits; differences in health insurance coverage between and within urban/rural communities; inequality in oral health–related quality of life among children, youths, and adults; and inequality in the prevalence of early childhood caries and feeding habits in children, among others.
Considerable variations exist in the distribution of urban-rural dwellings among the various regions of the world (Fig.1), and significant changes are expected in the urban-rural ratio over the next decades (Fig. 2). These variations will continue to have significant impacts on equity in oral health care, services, and research. The purpose of this review is to highlight some of the conceptual issues relating to urban-rural inequalities in oral health, especially in the African and Middle East Region (AMER) of the International Association for Dental Research as defined in 2003 (Behbehani and Honkala 2004).
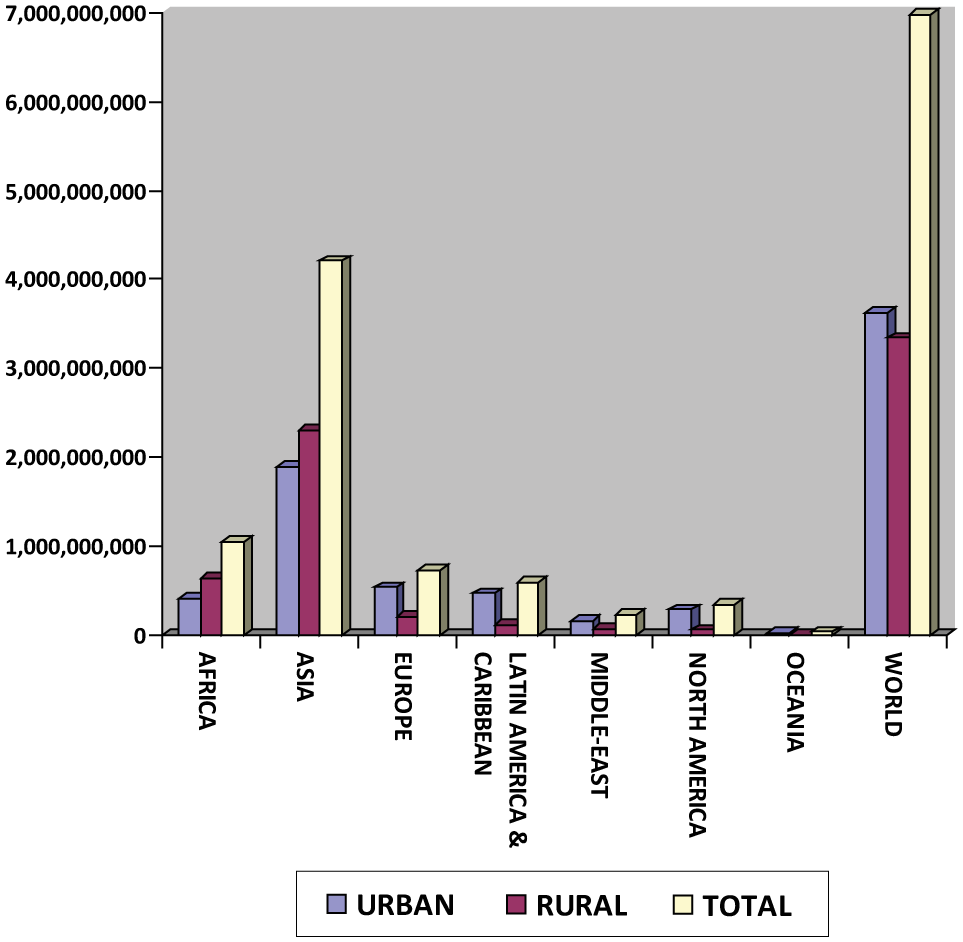
Comparative distribution of populations residing in urban and rural locations in different regions of the world. Source: United Nations, Department of Economic and Social Affairs, Population Division (2012).
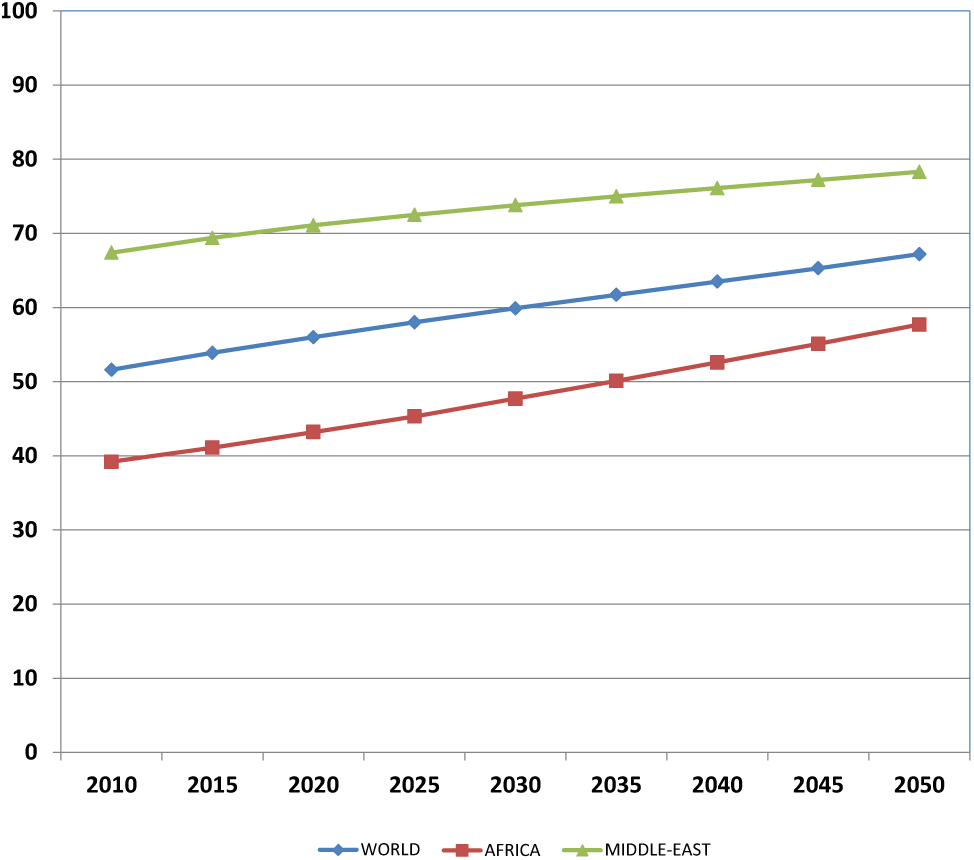
Percentage of the population residing in urban areas of Africa and the Middle East compared with the rest of the world. Source: United Nations, Department of Economic and Social Affairs, Population Division (2012).
Methodology
An extensive literature review on the subject was conducted using the PubMed database, a resource developed and maintained by the National Center for Biotechnology Information at the United States National Library of Medicine. PubMed indexes the largest range of peer-reviewed journals in the world, and the citations and abstracts include the fields of biomedicine and health, covering portions of the life sciences, behavioral sciences, chemical sciences, and bioengineering (http://www.ncbi.nlm.nih.gov). Searches were conducted utilizing the phrase [(oral health OR dental OR dentistry) AND (urban OR rural OR disparity) AND (Africa OR “middle east” OR egypt OR jordan OR iran OR nigeria OR “saudi Arabia” OR “south africa”)]. These 6 AMER countries were included because they had the highest dental publications (above 1,000 each) on PubMed when the search phrase [(oral health OR dental OR dentistry) AND {specific name of country}] was used. The date filter was not used, and flexibility in the year of publication was adopted due to the limited number of publications retrieved (n = 676). Each extracted reference was reviewed (title, author details, and abstract) for relevance to the subject, and those found unrelated were eliminated. Relevant scientific publications from the region that are not indexed in PubMed but known to the authors were also included.
Some of the major factors responsible for the urban-rural inequalities and the possible reasons for the differences were identified. Possible areas for future research and action are discussed and recommendations made to reduce the urban-rural inequalities in oral health care as a way of improving the oral and general health of the population.
Inequality and Poverty
Booysen et al. (2007) analyzed trends in poverty and inequality over a period of 10 to 15 y for 7 sub-Saharan African countries: Ghana, Kenya, Mali, Senegal, Tanzania, Zambia, and Zimbabwe. They found that poverty had declined in urban and rural areas in 5 of the 7 countries: namely, Ghana, Kenya, Mali, Tanzania, and Zimbabwe. The urban-rural decomposition of poverty estimates revealed major differences in the access to assets (Table 1).
Urban-Rural Distribution of Access to Assets in 7 African Countries.
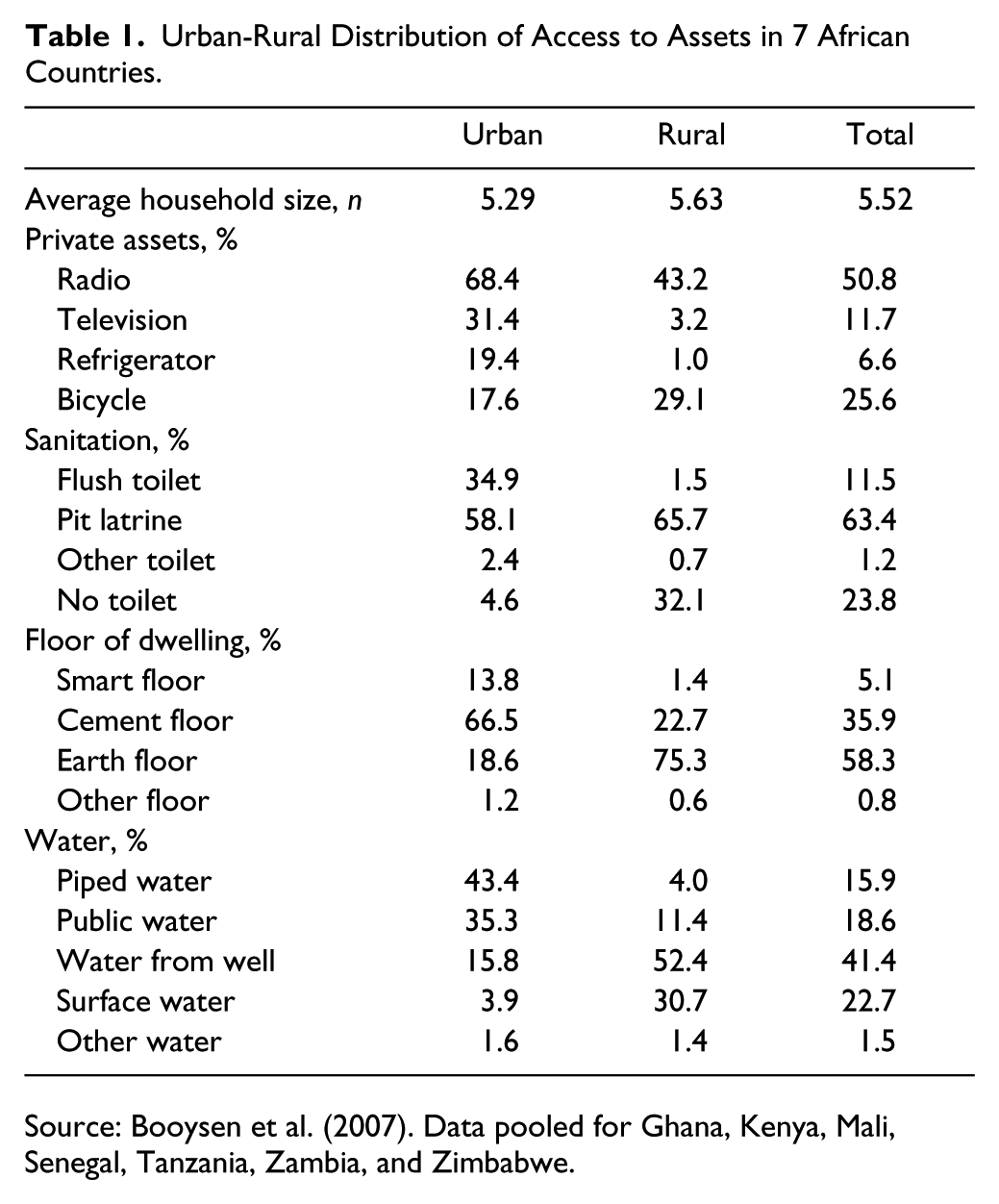
Source: Booysen et al. (2007). Data pooled for Ghana, Kenya, Mali, Senegal, Tanzania, Zambia, and Zimbabwe.
In water provision, urban areas had more access to piped water in the home, and public water with piped water was available to only 4% of the rural population. This makes the feasibility of water fluoridation very poor in these African nations. Similarly, radio broadcasts were available to about 68% of the urban population and only 43% of the rural population, while televisions were available to 31% of urban dwellers and only 3.2% of rural dwellers. This has enormous implications for mass media utilization in oral health education since television or radio broadcasts will provide information to less than half of the sub-Saharan African rural populations.
Ettinger (2007), in a comprehensive review of rural dentistry, concluded that for people living in rural and remote areas, unmet dental care remains one of the most urgent health care needs. Persons living in rural areas are likely to be poorer, be older, be less health literate, use drinking water that is not fluoridated, have more caries, have fewer teeth, and have less money to spend on dental care than persons living in urban areas. A study in Tanzania revealed that urban residents were 5 times more likely than rural residents to use toothpaste (Kikwilu et al. 2008). Since it is impossible to meet all of the unmet needs of such rural populations, it was suggested that prevention must be the focus of any program aimed at improving the oral health of rural dwellers (Ettinger 2007).
Disparities in Preventive Oral Health Knowledge and Practices
There are more positive dental attitudes and knowledge about oral diseases among urban communities compared with the rural areas (Varenne et al. 2006; Kikwilu et al. 2008; Bayne et al. 2013). A higher percentage of the urban population has knowledge that teeth cleaning and regular dental visits may prevent oral diseases compared with rural dwellers. A significant proportion of the rural population was unaware of the effectiveness of fluoride. Varenne et al. (2006), in a study of 12-y-old children, found the following discrepancies in the answers to statements on dental diseases and prevention (urban v. rural, respectively): “tooth cleaning may prevent tooth decay” (81% v. 42%), “tooth cleaning may prevent gum trouble” (67% v. 32%), “dental visits may prevent oral disease” (67% v. 42%), and “using fluoride is a good way to prevent dental decay” (9% v. 1%). The percentages were significantly higher in all cases for the urban locations. These perceptions are likely due to the higher levels of education and relatively easier access to information through the media in the urban areas compared to the rural locations (Booysen et al. 2007). Despite poverty in rural areas, some individuals are still addicted to unprocessed tobacco and alcohol, which are major risk factors for oral cancer. Typically at the initial stages of cancer, they do not seek medical help because of ignorance and poverty (Aulock 2005). Preventable dental diseases such as noma (cancrum oris) are still very common (Ogbureke and Ogbureke 2010).
In a study of the oral hygiene patterns among schoolchildren in Jordan, ALBashtawy (2012) found that 17% of the schoolchildren never brushed their teeth. There was a higher proportion, 22%, of rural children who never brushed their teeth compared with 14% of the urban students. A national pathfinder cross-sectional survey in Tanzania found social demographic disparities in relation to oral health–related behaviors. Urban residents were less likely to drink alcohol or smoke cigarettes, not eat fruit, visit dental clinics, and use factory-made toothbrushes and toothpaste than their rural counterparts. More rural (13.2%) than urban (4.6%) residents used charcoal for teeth cleaning. While chewing sticks remain the mainstay of achieving oral hygiene in rural areas largely due to the inexpensiveness and traditional and religious values, the use of toothbrushes and fluoride-containing paste is increasing in popularity as a sign of the modern lifestyle in urban centers (Oke et al. 2011).
Disparities in the Prevalence of Dental Caries
Dietary practices and nutrition are undergoing changes in most developing countries including those of the AMER. Moreover, the consumption of sugars is increasing rapidly. Among children, the daily consumption of sweets is relatively higher for urban areas compared with rural areas (11% and 6%, respectively), whereas the consumption of fresh fruits is more common among the rural population, with 42% of the rural population reporting the daily consumption of fruits compared with 31% of the urban population (Varenne et al. 2006). Hence, early childhood caries was more prevalent in urban areas than in rural populations (Varenne et al. 2006; Masumo et al. 2012). Advertisements and marketing of sweets and sugary beverages, which are more prevalent and accessible in urban centers, have influenced caregivers toward feeding their children sweets and snacks (Masumo et al. 2012).
There was a higher prevalence of tooth loss due to caries among urban residents compared with rural residents in Tanzania (Kida et al. 2006a). In a nationwide survey of the oral health status of children in Iran, the mean decayed, missing, and/or filled deciduous teeth/decayed, missing, and/or filled permanent teeth (dmft/DMFT) indices were 1.9/— for 3-y-old, 5.0/0.2 for 6-y-old, 3.6/0.9 for 9-y-old, and 0.6/1.9 for 12-y-old children (Bayat-Movahed et al. 2011) (Table 2). Significant differences in the prevalence of dental caries were found according to sex, province, family income, parents’ level of education, and urban/rural residence. Similarly, a statistically significant difference was reported among the 12-y-old children, with mean DMFT of 1.9 among those residing in urban areas compared with 1.7 in the rural population. Cleaton-Jones and Fatti (2009) investigated the caries trends in children in South Africa and Swaziland since the first published epidemiological study in 1910. They found variations in caries rates among racial groups and between rural and urban areas. Similarly, in an investigation of the oral health status of 18-y-old Iranians, the mean number of sound teeth was higher in urban residents compared with rural dwellers (P < 0.01) (Hessari et al. 2008).
DMFT and dmft Indices of Children by Area of Residence in Iran.
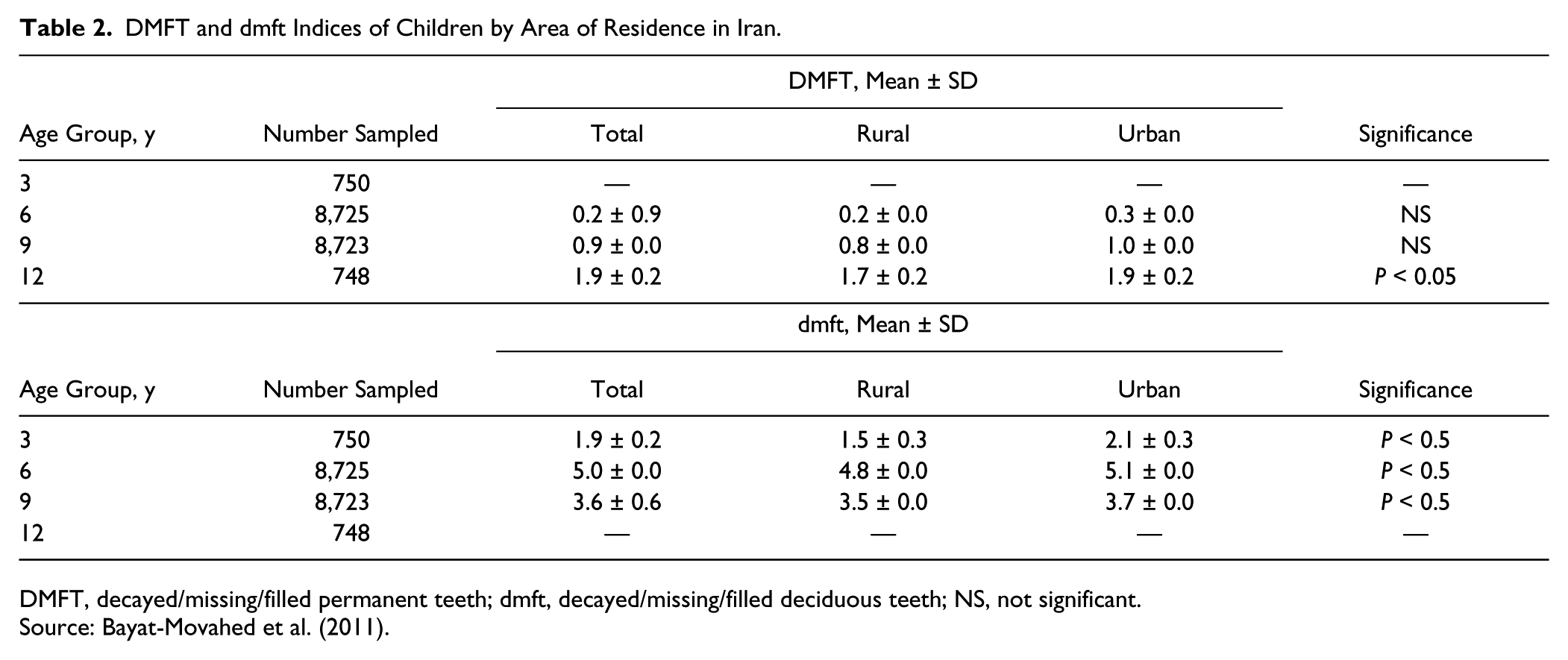
DMFT, decayed/missing/filled permanent teeth; dmft, decayed/missing/filled deciduous teeth; NS, not significant.
Source: Bayat-Movahed et al. (2011).
MacIntyre and du Plessis (2006) compared the diet, nutritional status, and dental caries of 10- and 15-y-old children in an urban town (Malamulele) and a rural village (Mahonisi) in the Limpopo Province, South Africa. They found that the mean dmft/DMFT scores were 1.21/0.65 for 10- and 15-y-old children in urban Malamulele compared with 0.33/0.02 in rural Mahonisi. The percentage of those caries free in Malamulele was 36% compared with 88% in Mahonisi. In an assessment of the frequency of consumption of cariogenic foods, oral hygiene practices, and dental health knowledge among Saudi male primary school children, clinically decayed teeth were diagnosed in 68% of the children, with higher levels in urban and younger students (Amin and Al-Abad 2008). Similarly, the oral health status of children and adults in rural and urban areas of Burkina Faso revealed that at age 6 y, 38% had caries, with the prevalence higher in urban than rural areas. At age 12 y, the mean DMFT was 0.7, with the prevalence significantly higher among urban than rural children. Important factors of high caries included location (urban) and consumption of soft drinks (Varenne et al. 2004). Table 3 shows the prevalence of caries in children in rural and urban areas of some African countries.
Prevalence of Caries in Children in Rural and Urban Areas of Some African Countries.
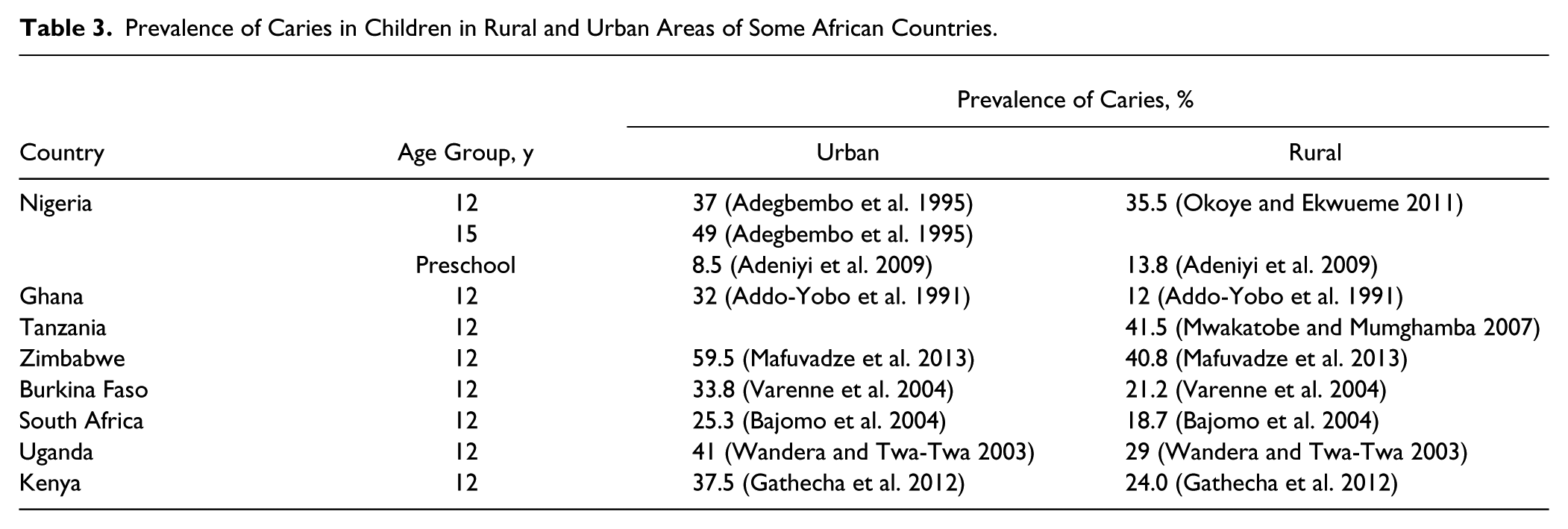
Varenne et al. (2006) noted that the majority of children in urban areas reported that teeth cleaning and regular dental visits may prevent oral diseases, whereas this perception was less among the rural population in whom 57% were not aware that the consumption of sugary products may cause tooth decay. Also, a significant proportion of the rural population doubted the effectiveness of fluorides.
Accessibility and Utilization of Modern Dental Services
Mashoto et al. (2010) looked at sociodemographic influences on oral health perception, behavior, and care utilization among adolescents in rural and urban Tanzania and found that rural adolescents presented more frequently with caries, a high need for dental treatments, and poor oral hygiene and utilized care less often compared with their urban counterparts. Similar results have also been recorded for Burkina Faso (Varenne et al. 2006) and Nigeria (Azodo and Amenaghawon 2013), with all the studies reporting the low utilization of dental services among rural dwellers.
Among the elderly in Ghana, the odds ratio of having a chronic noncommunicable condition for those in rural areas was twice as high as those in an urban area (Ayernor 2012). There was better access to oral care among urban dwellers and to treatment modalities. Those in rural areas had a higher percentage of untreated, decayed (55% v. 46%, respectively), and mobile (22% v. 16%, respectively) teeth than their urban counterparts (Kida et al. 2006a), which could be attributed to poor access to oral health care among those living in rural areas. Other studies showed significant differences in the prevalence of periodontal disease between urban and rural areas (Muwazi et al. 2005; Owino et al. 2010; Azodo and Amenaghawon 2013).
Rural areas are often associated with lower education levels, which in turn have been found to be related to lower levels of health literacy and the poor use of health care services (Booysen et al. 2007). Other important factors include the following:
1. Maldistribution of oral health personnel:
Price and Weiner (2005) found that 76% of South African medical graduates work in large urban areas. Dentists are unwilling to work in rural areas because of lower remuneration, poorer standard of living, poor infrastructure and services to work with, fewer colleagues and less professional support and development, and fewer choices and opportunities for specialization. Hospitals offering dental services are often few and located mostly in urban centers, with rural dwellers having to travel several kilometers to access care. In many African countries, orthodontic services, implants for the replacement of missing teeth, and other modern methods of dental treatment are inaccessible to those living in rural areas. Bakhsh et al. (2012) investigated factors affecting the internal brain drain of health care professionals in Saudi Arabia and found that 71% of respondents intended to return to work within the 2 major urban cities: Riyadh and Jeddah. Respondents who completed their undergraduate studies in a large city were more likely to work in the same city. Furthermore, 51% of the students were willing to work in a rural area for a 50% or more increase in their salary. The authors concluded that realistic financial incentives would probably not suffice to attract Saudi health care providers to rural areas. A significant challenge is to find innovative ways to address these workforce disparities, as well as the urban/rural and private/public sector maldistribution of dental specialists, and to develop a more rational basis for training dental personnel (Lalloo et al. 2006).
2. Discrepancies in health insurance coverage between and within urban/rural communities and groups:
In most countries of the AMER, a reasonably well-established public health system coexists with a private health sector. These systems are however not perfect. In South Africa, for example, wide disparities in health spending, professional staffing levels, and accessibility continue to exist between the public and private health sectors, amid escalating health care costs (Ayo-Yusuf et al. 2013). As there are no publicly funded health insurance schemes, the main criterion for access to health insurance and thus to private health care in South Africa is formal employment. There are no stand-alone dental insurance plans, but most of the health insurance plans include dental benefits, to a varying extent. A visit to a dentist at least once a year for preventive dental care such as dental prophylaxis is covered in most South African health insurance plans and has recently been recommended by the Council for Medical Schemes to be included as part of basic dentistry to be covered under the “prescribed minimum benefit” package, which is recognized by statute in South Africa. The majority of individuals in rural settings lack insurance coverage and cannot afford treatment (Ayo-Yusuf et al. 2013). Many dental procedures require very high financial commitment far beyond the affordability levels of the economically poor population. Additionally, health insurance in the AMER is often employment linked, and rural dwellers may not have the benefit of visiting the dental clinic for preventive dental care (Ayo-Yusuf et al. 2013).
Disparities in Oral Impacts on Daily Performance
Poor oral health can have a significant effect on quality of life. In a study conducted in Tanzania, the reported prevalence of Oral Impacts on Daily Performance (OIDP) among older adults was 55%, with more rural persons being affected. The prevalence of oral impacts was 51% in urban areas and 62% in rural areas. Problems with eating was the performance reported most frequently (42% in urban, 55% in rural), followed by cleaning teeth (18% in urban, 30% in rural) (Kida et al. 2006b). More than half of the urban and rural residents with impacts had impacts of very little, little, and moderate intensity. The most frequently reported causes of impacts were toothache and loose teeth. More rural residents, compared with urban, rated their oral health as poor and had clinically detected poor oral health in terms of decayed and mobile teeth, which might affect their daily performance.
Demographic Location and Composition of Students in Dental Training Institutions
Almost all the dental schools in the AMER are in urban centers, and a large percentage of the dental students are from cities. This is also reflected in the distribution of the oral health care workforce (Lalloo et al. 2006). The health workforce to population ratios provide one gauge of possible health service access disparities. The average dentist to population ratio varies widely across the AMER. Although 1:25,000 for Africa, the ratio in South Africa is 1:14,509, Ghana 1:234,780, and Ethiopia 1:1,278,446. The Middle East has more dentists, with most countries having 1 dentist in a population of less than 4,000 (Beaglehole et al. 2009). Moreover, significant disparities in dentists exist across the rural-urban continuum.
A number of studies have examined programs to increase the recruitment of health care professionals into rural and underserved areas, thereby creating a more equal distribution of providers throughout a state (Brooks et al. 2002; Isabel and Paula 2010). A review of the literature by Brooks et al. (2002) found that, for medical students, having a rural upbringing and specialty preference for rural practice mattered. For schools, a commitment to a rural curriculum and rotations were the most significant factors in encouraging graduates to move to rural areas.
Urban-Rural Disparities in the Distribution of Traditional Healers
Traditional healers are often the first line of contact for the management of oral diseases in rural areas (Rudolph et al. 2007; Agbor and Naidoo 2011). According to the World Health Organization (2002), more than 80% of Africans rely on traditional medicine and indigenous knowledge to meet their health needs. This is because traditional medicine is accessible, affordable, and culturally and socially acceptable, and most people prefer it to the more expensive conventional medical practice. Studies conducted in Africa have shown different distributions and roles for traditional healers in the management of oral disease. Generally, traditional healers treat exposed dental pulps using local herbs obtained from the leaves, bark, or roots of trees. They also use fumes from burnt food spices to remove “worms” from infected teeth and to extract loose teeth (Ogunbodede 1991; Rudolph et al. 2007; Agbor and Naidoo 2011; Adebola et al. 2013). Many patients seek help concurrently from traditional healers and formal health services. In a report from South Africa, traditional healers were the only means of health care delivery available to over 80% of the rural population (Rudolph et al. 2007). There are about 200,000 traditional healers practicing in South Africa compared with 25,000 doctors of modern medicine.
The oral health care workforce in Cameroon consists of 220 dentists, all trained abroad. Nearly all work in the 2 big cities of Douala and Yaoundé, serving just 20% of the country’s population. On the other hand, there are more than 20,000 traditional healers in the country, serving both the rural and urban population (Agbor and Naidoo 2011). Ngilisho et al. (1994) reported that 60% of the villagers in the Tanga region of Tanzania who suffered from toothache sought treatment from traditional healers. They were treated with local herbs and obtained pain relief for more than 6 mo. The presence of modern health facilities did not influence the villagers’ use of traditional healers. Hence, it could be surmised that traditional healers played an important role in the relief of acute dental pain in underserved rural areas.
Conclusions and Recommendations
Socioeconomic factors play significant roles in fostering rural-urban disparity in the use of dental services. Until poverty, education, unemployment, and other macro determinants of health are resolved, there will always be health disparities between urban and rural areas. Hence, research into the complex interactions between poverty, endemic infections, and malnutrition and their relevance to oral health problems should be considered a very high priority.
Concerted efforts must be made by all stakeholders (governments, health care workforce, organizations, and communities) to reduce inequalities and improve oral health outcomes in underserved populations. Approaches employed need to concentrate on 2 key areas: increasing participation in oral health promotion and improving access to oral health care services.
Increasing Participation in Oral Health Promotion
A compelling need exists for national oral health policies and implementation plans that recognize the urban-rural differences in oral health and that emphasize the prevention, early detection, and management of oral diseases (Williams 2011; Watt et al. 2014). Since consuming refined sugary foods and sweetened drinks are significantly linked to dental caries and other dental diseases (Benoist et al. 2014), oral health stakeholders must be prepared to provide guidance on policies regarding the labeling, marketing, and distribution of products containing free sugars.
Prevention strategies should be aimed at empowering communities and individuals with the knowledge and skills for improving their oral health and should ideally target both rural and urban populations. Population-specific oral health promotion campaigns using a common risk factor approach focusing on healthy oral health behaviors and prevention (Watt and Sheiham 2012; Watt et al. 2014) will provide opportunities to disseminate the importance and value of oral health as part of overall health through community-based oral health education programs. It is important to partner with other stakeholders to enhance the oral health contents of school curricula.
Access to Oral Health Care Services
Although methods such as the use of mobile dental clinics, atraumatic restorative treatment, and similar procedures are being employed to mitigate rural-urban differences in the access to oral health care, these have not been able to adequately bridge the widening gap (Kikwilu et al. 2009). Oral health should be fully integrated into primary health care (PHC) services. It is necessary to train and utilize PHC workers, who are mostly nondental health care providers and more accessible in rural areas, to provide basic oral health information and screening while tracking referrals to oral health care professionals. Midlevel providers could offer a full range of dental work, with the exception of treatment for major facial injuries (Achembong et al. 2012).
Outreach models, workforce models, and school-based models are approaches that may be useful in addressing inequalities and bridging the gap between urban and rural communities (Bayne et al. 2013). Employment-linked insurance is a disadvantage to rural populations as most of the population is engaged in farming and other nonmainstream jobs. AMER countries should strive for universal health insurance schemes to create equity in the access to care for rural populations. Consideration should also be given to tax exemption for oral care products to ensure that they are affordable to rural populations that are often less economically endowed.
Links should be created between dental schools and PHC centers to increase the exposure of dental students to rural settings while improving the populations’ access to oral health care (Ogunbodede et al. 2005; Bhayat et al. 2011). Methods to attract dental professionals to serve in rural communities should be explored and could include implementing programs that will encourage students from rural communities to choose dental careers and offering incentives to dental professionals who serve rural populations.
Author Contributions
E.O. Ogunbodede, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; I.A. Kida, H.S. Madjapa, M. Amedari, A. Ehizele, R. Mutave, B. Sodipo, contributed to design, data acquisition, analysis, and interpretation, critically revised the manuscript; S. Temilola, L. Okoye, contributed to design, data acquisition, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
They acknowledge the support of Professor Eino Honkala in coordinating the AMER/GOHIRA workshop that engendered this publication. They are also grateful for pre-review by Professors Aubrey Sheiham and David Williams.
This information was presented at the GOHIRA-AMER Pre-conference workshop, in connection with the IADR/AMER General Session in Cape Town, South Africa on June 24, 2014.
Workshop and supplement sponsored by the
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.