
Abstract
Anxiety regarding dental and physical health is a common and potentially distressing problem, for both patients and health care providers. Anxiety has been identified as a barrier to regular dental visits and as an important target for enhancement of oral health–related quality of life. The study aimed to develop and evaluate a computerized cognitive-behavioral therapy dental anxiety intervention that could be easily implemented in dental health care settings. A cognitive-behavioral protocol based on psychoeducation, exposure to feared dental procedures, and cognitive restructuring was developed. A randomized controlled trial was conducted (N = 151) to test its efficacy. Consenting adult dental patients who met inclusion criteria (e.g., high dental anxiety) were randomized to 1 of 2 groups: immediate treatment (n = 74) or a wait-list control (n = 77). Analyses of covariance based on intention-to-treat analyses were used to compare the 2 groups on dental anxiety, fear, avoidance, and overall severity of dental phobia. Baseline scores on these outcomes were entered into the analyses as covariates. Groups were equivalent at baseline but differed at 1-mo follow-up. Both groups showed improvement in outcomes, but analyses of covariance demonstrated significant differences in dental anxiety, fear, avoidance, and overall severity of dental phobia in favor of immediate treatment at the follow-up assessment. Of the patients who met diagnostic criteria for phobia at baseline, fewer patients in the immediate treatment group continued to meet criteria for dental phobia at follow-up as compared with the wait-list group. A new computer-based tool seems to be efficacious in reducing dental anxiety and fear/avoidance of dental procedures. Examination of its effectiveness when administered in dental offices under less controlled conditions is warranted (ClinicalTrials.gov NCT02081365).
Keywords
Introduction
Dental anxiety and specific phobia of dental procedures are prevalent conditions that can result in substantial distress and oral health impairment, affecting 10% to 20% of adults in various US population groups (Locker et al. 1999; Sohn and Ismail 2005; Tellez et al. 2015). Few computer-aided interventions tested in randomized clinical trials have targeted dental anxiety. Although 1 computer-based treatment for dental injection fear has been evaluated (the CARL Program; Coldwell et al. 1998; Heaton et al. 2013), the current study tests the efficacy of a computerized treatment for a broader range of dental concerns.
Cognitive-behavioral interventions have garnered strong support in the treatment of dental anxiety. A meta-analysis of 38 studies focusing on cognitive-behavioral therapy (CBT; Kvale et al. 2004) provides support for its efficacy in reducing dental anxiety among adults, even when administered in a limited number of brief sessions (de Jongh et al. 1995; Thom et al. 2000; Jöhren et al. 2007; Haukebø et al. 2008; Wannemueller et al. 2011). A recent review that critically appraised 22 randomized treatment trials aimed at reducing dental anxiety and avoidance in adults (Gordon et al. 2013) also provided support for brief CBT interventions. Furthermore, a recent study demonstrated that a brief cognitive-behavioral intervention performed by practicing dentists may help fearful patients overcome their fear and attend dental treatments more regularly (Spindler et al. 2015). However, this intervention would require dentists to receive training in psychotherapy, be comfortable with performing the intervention, and have the necessary tools to distinguish patients who may need more intensive treatment elsewhere. Self-administered treatments have also shown promise (Getka and Glass 1992), and the utility of computerized or online interventions should be investigated.
This study aimed to develop and evaluate a computerized CBT (C-CBT) dental anxiety intervention that could be easily implemented in dental health care settings.
Materials and Methods
Design
This was a single-center parallel study with randomization to either an immediate treatment (IT) group or a wait-list (WL) control group (allocation ratio:1:1). IT participants received C-CBT immediately preceding their scheduled dental appointments. WL participants attended their scheduled dental appointments without receiving C-CBT and were offered the same intervention following all assessments. Data from the later treatment of WL patients are not included in the present analyses. No changes were made to outcomes after commencement of the trial.
Sample Selection
The main hypothesis to be tested (H0: There are no significant differences between IT and WL) was subjected to power analysis. Assuming an average change in Modified Dental Anxiety Scale (MDAS; Humphris et al. 1995) mean scores of 5 ± 10 in the IT group and no change in the WL group, with a power of 0.80, an α level of 0.05, and a 2-tailed test, we determined that 150 participants should be recruited. Recruitment was carried out through the Faculty Practice Clinic at the Temple University Kornberg School of Dentistry (TUKSoD) in 2014. All new patients were identified through the clinic’s electronic scheduling software and invited to participate before their dental appointments if they met screening criteria on the MDAS. There were no restrictions on enrollment in terms of sex, economic status, or ethnic group.
To be included, patients had to be between 18 and 70 y of age, be fluent in spoken and written English, have scheduled a dental treatment appointment at the TUKSoD Faculty Practice Clinic, be willing and able to give informed written consent, participate responsibly in the study protocol, meet criteria for high dental anxiety based on the MDAS, and endorse at least some oral health–related impairment at the administration of a semistructured diagnostic interview. Participants received a $25 money order for completing the baseline questionnaires and telephone interview and, if randomized to IT, for coming to their dental appointment 1.5 h early to complete C-CBT. Furthermore, all participants received an additional $25 payment for completing their 1-mo follow-up questionnaires. The trial was stopped when recruitment targets were reached. The study was approved by the Institutional Review Board at Temple University (protocol 13928). All patients provided informed consent. The trial is registered at ClinicalTrials.gov (NCT02081365).
Procedure
Participation in the study involved completing 1) self-report questionnaires online (or, for individuals without Internet access, by telephone) and 2) a telephone diagnostic interview. The research assistants at the clinic administered the randomization of participants (computer generated) and distribution of appointments. The file was secured and restricted to the time of randomization. Randomization was done after baseline assessments for two-thirds of the sample, while for one-third, it was done before the assessments.
For practical and ethical reasons related to the fact that participants were paying for the dental treatment themselves and the immediacy of treatment to which they were allocated, we could not blind them to the outcome of the randomization. After randomization, each participant was instructed to complete the self-report assessments and the diagnostic interview before coming in for their dental appointment. IT participants were asked to come in 1.5 h before their dental appointment to complete C-CBT, whereas those in the WL group simply attended their dental appointment as normally scheduled. One month after the dental appointment, participants were contacted by phone and asked to complete follow-up assessments. If a participant did not respond to study staff’s initial contact attempt for the follow-up assessment, research assistants continued to call that participant weekly for 1 mo. Participants who never responded to these requests for follow-up assessment were considered lost to follow-up.
Intervention
C-CBT consisted of a single-session 1-h computerized intervention that assisted the participant in building skills for managing his or her dental anxiety. Participants completed C-CBT in a research office near the TUKSoD Faculty Practice Clinic on a desktop computer with headphones. The intervention was delivered with the aid of a research assistant who was available to answer any questions and to assist participants with any aspect of C-CBT that they found difficult.
C-CBT began with a psychoeducation module, which provided participants with basic education about the nature of dental anxiety. Next, patients were guided through a brief motivational interviewing exercise that helped them consider the benefits and drawbacks of working on their dental anxiety. Thereafter, patients were guided through the exposure exercises, which included opportunities to practice coping with their dental anxiety. For the exposure exercises, patients were first asked to select their 3 most feared dental procedures from a list of 6 (drilling and having a cavity filled, cleaning, anesthetic injection, root canal, oral X-ray, and tooth extraction) and rank them from least to most anxiety provoking. Patients then watched video recordings of their top-3 feared procedures, starting with the least anxiety provoking and working up to the most. For each selected procedure, 3 videos were presented:
The first video depicted a dentist and/or hygienist conducting the procedure with a patient and provided a basic explanation of the procedure. Animations of aspects of the procedure that occur within the mouth were included, as were close-ups of the dental tools employed.
The second video presented similar visuals of the dental procedure but was more focused on the patient’s emotional experience during the procedure. The voiceover provided basic training in the nature and use of cognitive coping skills for dental anxiety.
The third video was filmed from the perspective of the patient in the dental chair and provided more intensive exposure to the feared dental procedure. Furthermore, the voiceover was a “dialogue” between the patient from the first 2 videos, who demonstrated how to effectively cope with anxious thoughts, and the participant, who was led through the steps to develop coping thoughts for his or her own dental anxiety.
The intervention closed with a brief module providing additional motivational enhancement for attending future dental appointments. Upon completing the intervention, participants attended their scheduled dental appointments and were encouraged to use the skills that they learned from C-CBT to cope with any anxiety that they experienced during that appointment.
Measures
Primary measure: dental anxiety
Dental anxiety was measured with the MDAS, a 5-item self-report measure that assesses fear of dental procedures, including drilling, scaling and polishing (i.e., cleaning), and local anesthetic injections. Sample items include “If you went to your dentist for treatment tomorrow, how would you feel?” and “If you were about to have your tooth drilled, how would you feel?” Items are rated on a 5-point Likert-type scale ranging from 1 (not anxious) to 5 (extremely anxious). The MDAS has demonstrated good internal consistency (α = 0.89) and test-retest reliability (r = 0.82, interval unspecified; Humphris et al. 1995). A total MDAS score ≥19 has been used as an indicator of high dental anxiety (Humphris et al. 1995; King & Humphris 2010); however, concerns have been raised about this cutoff, as it could exclude individuals who are very or extremely anxious about only 1 of 2 types of dental procedures (Dailey et al. 2002). Therefore, in the present study, we considered patients who scored ≥19 on the MDAS at baseline or endorsed at least 2 MDAS items ≥4 to have high dental anxiety. This method has demonstrated superior sensitivity and specificity compared with the conventional scoring procedure (Schulman et al. 2014).
Secondary measures: semistructured diagnostic interview
The Anxiety Disorders Interview Schedule (ADIS-IV; Brown et al. 1994) is a semistructured diagnostic interview designed to assess criteria per the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association 1994) for current anxiety, depressive, somatoform, and substance use disorders. The ADIS-IV has demonstrated good to excellent interrater reliability for the diagnosis of all assessed disorders (κ = 0.56 to 0.81; Brown et al. 2001), with the exception of dysthymic disorder (κ = 0.31). All diagnosticians were advanced doctoral students or research assistants who were trained to strict reliability standards established by Brown et al. (2001). For the present investigation, only the specific phobia module of the ADIS-IV was administered to assess the presence and severity of a current diagnosis of dental phobia. Details regarding the assessment and computation of each variable are provided below.
Dental phobia
Various aspects of dental phobia were assessed using the specific phobia module of the ADIS-IV. Interviewers assessed participants’ anxiety and avoidance of dental procedures on scales that ranged from 0 (none) to 8 (very severe). They also rated patients’ overall distress and impairment due to their dental phobia symptoms and assigned a clinician’s severity rating that also ranged from 0 (none) to 8 (very severe); a rating ≥4 indicated that the participant met criteria for diagnosis of dental phobia.
Client satisfaction questionnaire
The Client Satisfaction Questionnaire (CSQ-8; Larsen et al. 1979) is an 8-item self-report questionnaire designed to assess client/patient satisfaction in health and human services. Each item is rated on a 4-point scale. Individual item scores are summed, resulting in a total score ranging from 8 to 32, with higher scores indicating higher satisfaction. The CSQ-8 has demonstrated high internal consistency in multiple clinical samples in mental health settings (α = 0.92 to 0.93, Larsen et al. 1979; split-half reliability r = 0.82, Nguyen et al. 1983). The CSQ-8 was administered immediately after patients completed C-CBT to assess their satisfaction with the program.
Statistical Analyses
Differences between the groups on baseline sociodemographic, clinical, and psychological measures were examined using χ2 (Pearson) or Student’s t tests, as appropriate (see Table 1). Moreover, differences on the variables listed above among completers and dropouts were also explored, but no differences were found. Both per-protocol and intention-to-treat (ITT) analyses were then conducted, but only ITT analyses are reported in the Results section.
Baseline Differences by Condition
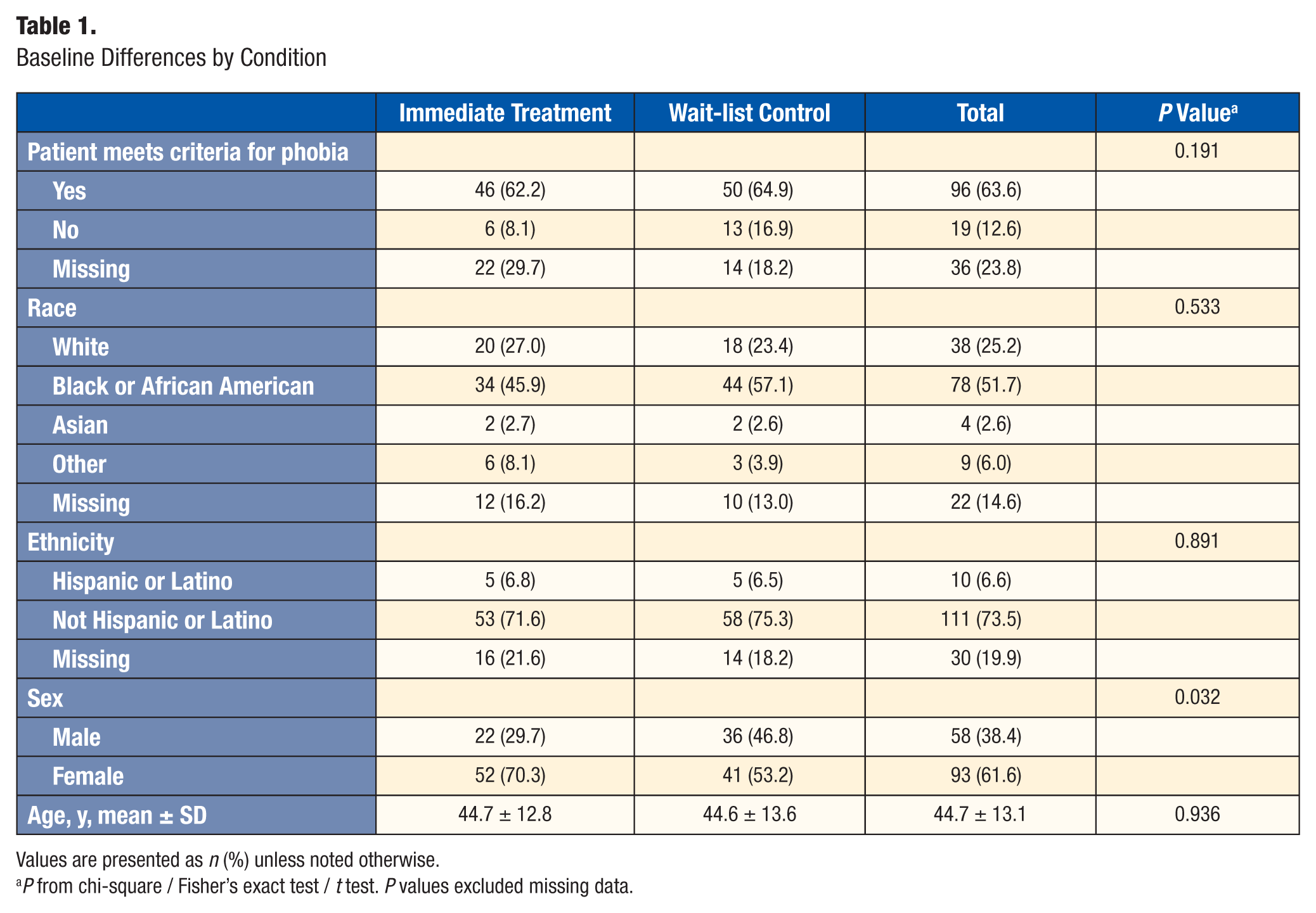
Values are presented as n (%) unless noted otherwise.
P from chi-square / Fisher’s exact test / t test. P values excluded missing data.
To address our aim, analysis of covariance (ANCOVA) was used to compare the 2 groups on primary and secondary outcome measures. Baseline scores on the outcome of interest were entered into the analyses as covariates, as was sex in the analysis of the MDAS scores, as sex differed between IT and WL groups at baseline (P = 0.032; Table 1). Data were analyzed with SPSS 22.0 (IBM Corporation, Armonk, NY, USA).
Multiple imputation
Multiple imputation (MI) was used to handle missing follow-up data. There were 3 steps in the multiple-imputation procedure:
The missing follow-up data were filled in 100 times to generate 100 complete data sets.
The 100 data sets were analyzed by ANCOVAs with follow-up scores as outcomes and with the treatment group as the independent variable (IT vs WL), controlling for baseline scores.
The results from the 100 complete data sets were combined for the multiple-imputation inference (Rubin 1987).
SAS PROC MI and PROC MIANALYZE were used for multiple-imputation analysis using SAS 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Demographics
Of 961 new patients who received recruitment calls, 354 expressed interest and were assessed for eligibility. A total of 151 patients were eligible, consented to participate, and were randomized to IT (n = 74) or WL (n = 77; Fig.). Eighteen WL participants and 28 in the IT group did not receive the allocated intervention. Of the remaining 105 participants who completed the baseline assessment, 5 WL and 2 IT participants were lost to follow-up. The total sample comprised 151 adults seeking dental care at the TUKSoD Faculty Practice Clinic (female, 61.6%; mean age, 44.7 ± 13.1 y; range, 18 to 70 y). The racial/ethnic composition of the sample was generally consistent with that of north Philadelphia (U.S. Census Bureau 2010): approximately 51.7% of participants identified as black, 25.2% as white/Caucasian, 2.6% as Asian or Pacific Islander, and 6.0% as other. As noted above, no significant differences between groups on baseline demographic or clinical measures were found, except for sex (see Table 1).
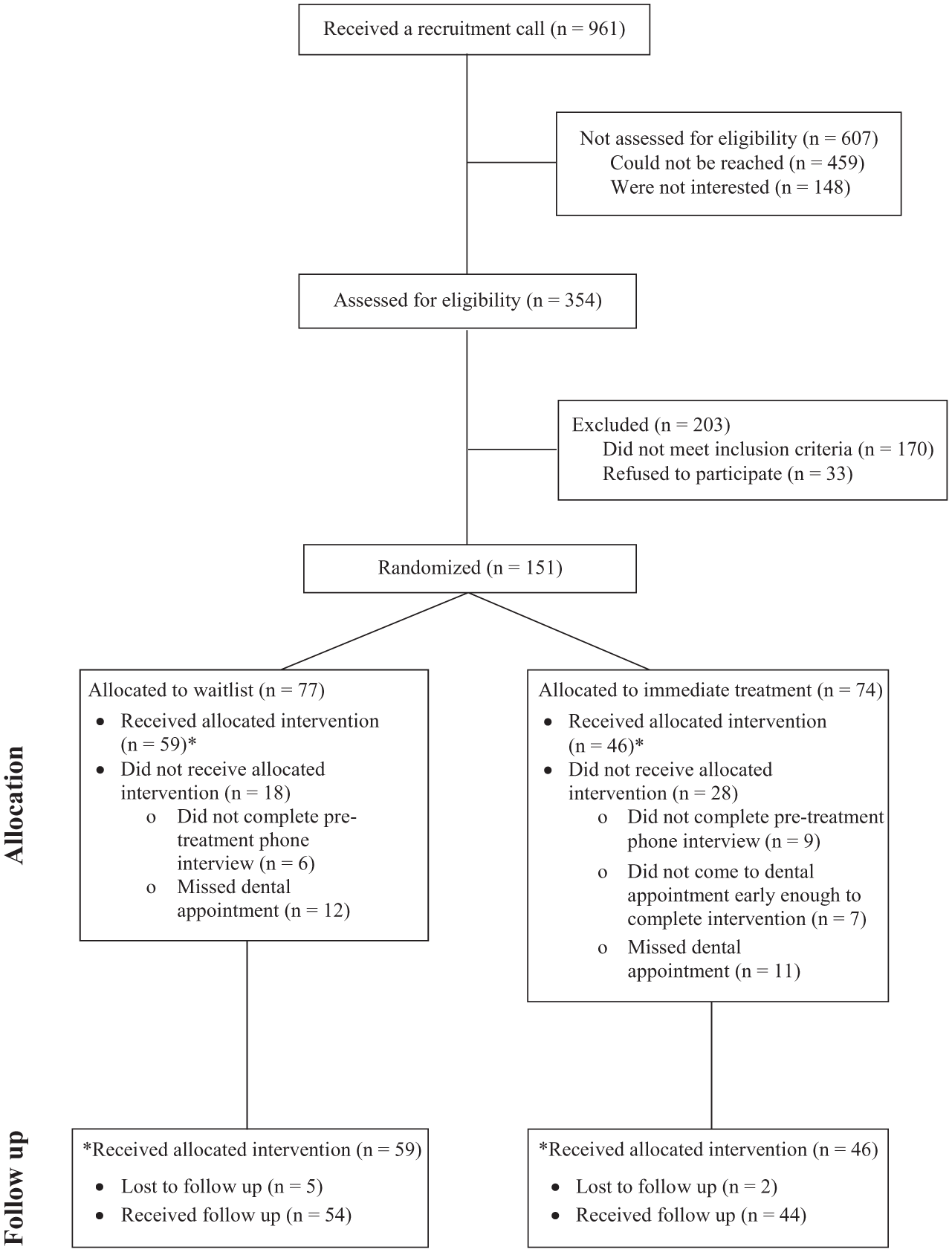
CONSORT flowchart.
Efficacy of C-CBT
Groups were equivalent at baseline but differed at 1-mo follow-up. Both groups showed improvement in outcomes, but ANCOVAs demonstrated significant differences in dental anxiety, fear, avoidance, and overall severity of dental phobia in favor of IT at the follow-up assessment.
Primary measure
MDAS scores decreased from baseline (19.5 ± 0.34) to 1-mo follow-up (15.4 ± 0.74) for the IT group (see Table 2). An ANCOVA with the ITT sample (N = 151) confirmed that the IT group had MDAS scores that were 2.2 points (95% confidence interval [95% CI]: 0.74, 3.55) lower than those of the WL group (P = 0.019) after controlling for the effect of baseline MDAS scores and sex.
Baseline and Follow-up Scores on Primary and Secondary Measures
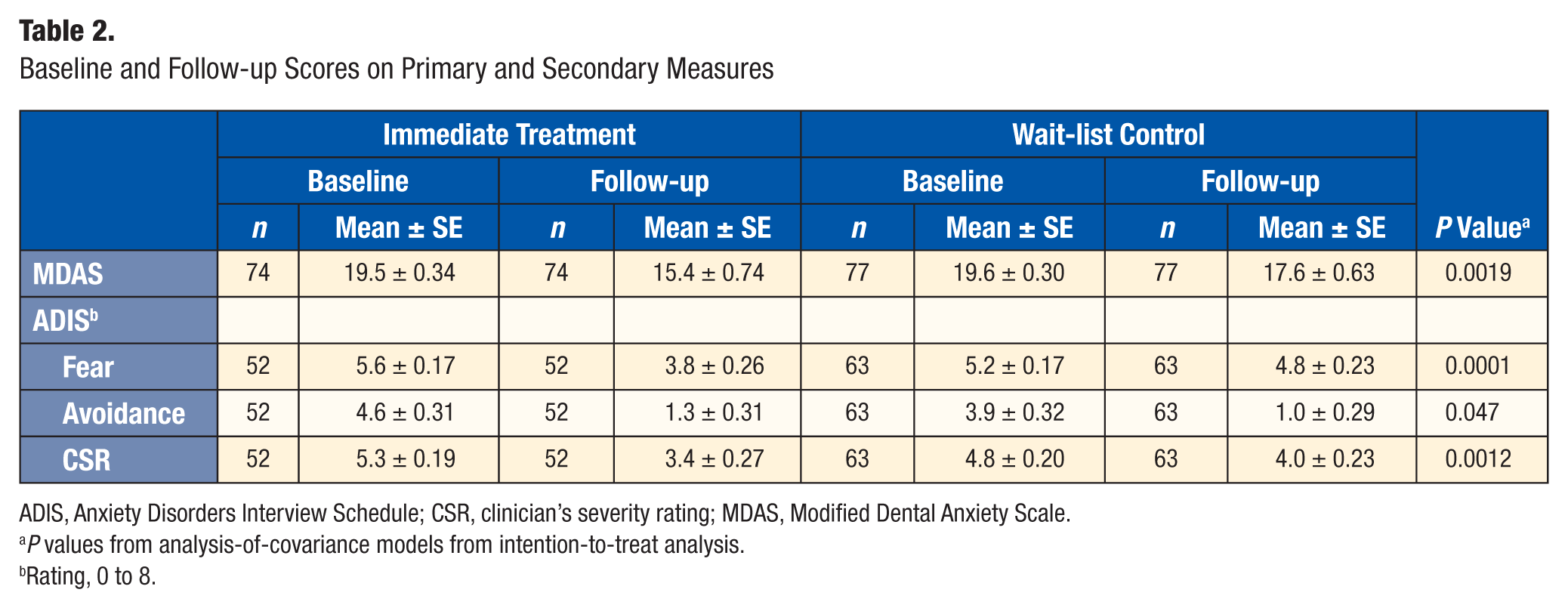
ADIS, Anxiety Disorders Interview Schedule; CSR, clinician’s severity rating; MDAS, Modified Dental Anxiety Scale.
P values from analysis-of-covariance models from intention-to-treat analysis.
Rating, 0 to 8.
Secondary measures
ADIS-IV ratings of dental fear (baseline: 5.6 ± 0.17, follow-up: 3.8 ± 0.26), dental avoidance (baseline: 4.6 ± 0.31, follow-up: 1.3 ± 0.31), and overall severity of dental phobia symptoms (baseline: 5.3 ± 0.19, follow-up: 3.4 ± 0.27) decreased from baseline to 1-mo follow-up for the IT group (see Table 2). ANCOVAs with the ITT sample (N = 115) revealed significant between-group differences on the ADIS-IV—dental fear, 1.23 points (95% CI: 0.61, 1.85), P = 0.0001; dental avoidance, 0.82 points (95% CI: 0.01, 1.64), P = 0.047; and overall severity of dental phobia symptoms, 0.98 points (95% CI: 0.39, 1.57), P = 0.0012—all favoring the IT group after controlling for the corresponding baseline scores. Of patients meeting criteria for phobia at baseline (n = 83), fewer IT patients (51.4%) than WL patients (74.4%) met criteria for dental phobia at follow-up (χ2 = 4.319, P = 0.038). No harms were noted.
Client Satisfaction with C-CBT
The mean CSQ score was 26.4 ± 4.4. Almost 83% of patients were very satisfied with C-CBT.
Discussion
This study examined the effect of a brief computerized dental anxiety intervention on patients seeking dental care at a university setting. Compared with a WL group, the IT group showed a significant reduction in dental anxiety, fear, avoidance, and the presence of dental phobia as measured by a reduction from baseline to follow-up on the MDAS and ADIS-IV.
The use of computer-based therapy reduces the reliance on in-person clinician time (Marks et al. 2007), and it may be as effective as face-to-face psychotherapy for anxiety disorder sufferers (Hedman et al. 2012), speeding access to care. Many individuals with anxiety disorders do not seek professional help (Bijl et al. 1998). When they do, they are commonly put on long waiting lists (Lovell and Richards 2000), and the treatment that they eventually receive is often not evidence based (Andrews et al. 2004). Much less is known about the efficacy of these interventions in dental settings. It is therefore important to develop evidence-based help that patients can access easily and that requires little time from a therapist (Hirai and Clum 2006).
The current results should be interpreted with some caution. Only dental treatment–seeking patients who initiated contact with the TUKSoD dental clinics were recruited into the study, thereby excluding individuals whose anxiety may be present at higher levels and thus prevent them from accessing dental care. There was also considerable attrition from baseline assessment to the day of administration of the dental anxiety protocol. Also, in the current study, assistance from psychology personnel trained in CBT was provided at some points in the delivery of the intervention. To disseminate the intervention in a sustainable way, it is critical that dental personnel are trained in CBT so that they can provide this support to the patients in a regular dental setting, in which highly trained CBT therapists are generally not available. Last, in addition to reductions in dental anxiety, increased attendance at future dental appointments is also an ultimate goal. No analyses were conducted to evaluate this and other oral health outcomes in the current study, as the follow-up period was too brief; clearly, further research is needed. In sum, a new computer-based tool seems to be efficacious in reducing fear of dental procedures. Examination of its effectiveness when administered in dental offices under less controlled conditions is warranted. It will also be important to determine which patients derive sufficient benefit and which require more intense treatment; this protocol might be considered as the first level of intervention in a stepped model of care.
Author Contributions
M. Tellez, R.G. Heimberg, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; C.M. Potter, contributed to design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; D.G. Kinner, D. Jensen, E. Waldron, S. Myers Virtue, H. Zhao, contributed to design, data analysis, and interpretation, drafted and critically revised the manuscript; A.I. Ismail, contributed to conception, design, and data interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
We thank Dr. Steve Ondersma for his contribution to the programming of the dental anxiety management intervention and the dental and psychology students who participated as actors in the videos of the anxiety management program.
This study was funded by a grant from the Pennsylvania Department of Health.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.