
Abstract
Secondary caries lesions are the main late complication of dental restorations, limiting their life span and generating costs by repeated reinterventions. Accurate detection of secondary lesions is crucial for estimating the true burden of the disease and allocating appropriate treatments. We aimed to assess the accuracy of detection methods for secondary caries lesions. Clinical or in vitro studies were included that investigated the accuracy of 5 detection methods—visual, tactile, radiography, laser fluorescence, quantitative light-induced fluorescence—of natural or artificially induced secondary lesions, as verified against an established reference test. Sensitivity, specificity, positive and negative likelihood ratios, as well as diagnostic odds ratios were calculated and publication bias assessed. From 1,179 screened studies, 23 were included. Most studies were performed in vitro, on permanent posterior teeth, and had high risk of bias or applicability concerns. Lesions were on proximal (14 studies) or other surfaces and adjacent to amalgam (16 studies) or tooth-colored materials. Visual (n = 11), radiographic (n = 13), and laser fluorescence detection (n = 8) had similar sensitivities (0.50 to 0.59) and specificities (0.78 to 0.83), with visual and laser fluorescence assessment being more accurate on nonproximal surfaces and adjacent to composites, respectively. Tactile assessment (n = 7) had low accuracy. Light-induced fluorescence (n = 3) was sensitive on nonproximal surfaces but had low specificities. Most analyses seemed to suffer from publication bias. Despite being a significant clinical and dental public health problem, detection of secondary caries lesions has been assessed by only a few studies with limited validity and applicability. Visual, radiographic and laser-fluorescence detection might be useful to detect secondary lesions. The validity of tactile assessment and quantitative light-induced fluorescence remains unclear at present.
Keywords
Introduction
Secondary caries lesions are the most frequently stated late complication of dental restoration (Burke et al. 1999; Al Negrish 2001; Forss and Widström 2004; Gordan et al. 2012). Such lesions are found adjacent to restorations and have been traditionally thought to be associated with gaps between the tooth and the restoration (Cenci et al. 2009; Diercke et al. 2009; Nassar and González-Cabezas 2011). However, increasing evidence indicates that many “secondary” lesions are in fact primary caries lesions adjacent to restorations—that is, not caused by a defective (leaking) restoration (Kidd et al. 1994). However, the term secondary caries lesion is still frequently used, and within the present article, no discrimination is made between secondary lesions and lesions adjacent to restoration.
Based on the frequency of restoration replacement due to secondary lesions and the costs associated with this cycle of reinterventions, increasing attempts are made to reduce the propensity of restoration materials for secondary caries development (Wang et al. 2014). The detection of secondary lesions, however, has received lesser attention, while it might in fact be decisive both to estimate the true burden of the disease and to provide appropriate management for presumable lesions. Currently, there is no standard to be recommended for performing such detection, with dentists using a variety of methods, with even greater heterogeneity of subsequent treatment decisions. However, there are indications that the criteria on which restoration replacement are based have limited accuracy, potentially leading to false-positive diagnoses and unnecessary (invasive) reinterventions (Kidd et al. 1994; Rudolphy et al. 1995). Consequently, hard tissues are sacrificed, costs generated, and teeth potentially retained for shorter time due to a lack of agreed accurate and reliable detection standards for secondary caries lesions.
A variety of conventional and newer methods are available to detect secondary lesions. Visual or visual-tactile examinations, often combined with bitewing radiography, are still most common (Boston 2003; Ando et al. 2004). For proximally located lesions in posterior teeth, radiographic examination is even the primary method of detection (Gordan et al. 2012). Methods using the principle of laser fluorescence have been suggested and applied as aid to detect secondary lesions (Boston 2003). Quantitative light-induced fluorescence (QLF) generates images of the analyzed areas, with presumable carious tissues being less fluorescent than sound areas or restoration materials (González-Cabezas et al. 2003).
We aimed to systematically collect, appraise, and synthesize the accuracies of detection methods (visual or tactile assessment, radiography, laser fluorescence, or QLF) for secondary lesions from in vitro and clinical studies, answering the following question: For secondary caries lesions, what is the accuracy of various detection methods?
Material and Methods
This review follows international guidelines for performing and reporting systematic reviews and meta-analyses (Deville and Buntinx 2002; Moher et al. 2009).
Selection Criteria
Study selection
We selected clinical, in situ, or in vitro studies, investigating the detection of natural or artificially induced secondary caries lesions—namely, any lesions adjacent to direct or indirect restorations. Only studies investigating human teeth of the primary or permanent dentition were included. Studies investigating the detection of residual lesions—that is, lesions not in relation to the restoration margin—were excluded.
Index test
Studies needed to have applied 1 of the following index tests:
Visual examination—discolorations or texture change of the tooth surface, staining of the tooth-restoration interface, or any other visual change
Tactile assessment—ditching or overhanging restoration margins indicating secondary lesions
Intraoral radiography—radiolucencies detected by bitewing or periapical radiography, used on its own or in combination with visual assessments
Laser fluorescence (e.g., Diagnodent)—detectable changes in the detected fluorescence signal
QLF
Diaphanoscopy or fiber optic transillumination
No studies using the latter techniques were eventually included. Studies using other techniques that were not generally available in primary care dentistry (e.g., cone beam tomography) or not clinically applicable were excluded.
Reference test
The accuracy of the index tests needed to have been ascertained against a reference test. As there is no gold standard for assessing secondary caries lesions, studies using 1 of the following reference tests were included: 1) histologic examination and/or microradiography or 2) restoration removal and tactile examination of dentin beneath the margin interface (detectable softening of the dentin). For studies that had 3) artificially induced lesions or 4) deliberately left carious tissue along the margin area beneath the restoration, this was regarded as reference.
Outcomes
Studies needed to report on accuracy measures to allow calculating of the proportion of true or false positive or negative detections.
Search Strategy
Electronic databases (Medline via PubMed, Embase via Ovid, Cochrane Central Register of Controlled Trials) were systematically searched on January 5, 2015, with the search being updated on February 28, 2015. Screening procedure used a 2-pronged approach, combining the target condition (secondary caries OR recurrent caries OR caries adjacent to restoration OR residual caries) and the objective of the study (diagnosis OR detection OR diagnostic OR detect) via Boolean operators, without controlled vocabularies (e.g., MeSH). To not decrease sensitivity, search terms for the different index tests were not applied, as we expected these to be irregularly used to index studies.
Additionally, we searched Medion database for diagnostic reviews. Gray literature was retrieved via opengrey.eu and screening abstracts of the International Association for Dental Research and European Organisation for Caries Research. Cross-referencing from retrieved full-text studies was used to identify further articles for assessment. The search was not restricted to any language; no time limits were applied; and neither authors nor journals were blinded to reviewers. Title and abstract of identified studies were independently screened by 2 calibrated reviewers (F.B., H.A.) for potential eligibility, with studies mentioning ≥1 of the defined index tests having been used to detect secondary lesions as validated against a reference test being assessed full-text. In case of differences, consensus was obtained by discussion or consultation of a third reviewer (F.S.).
Data Extraction
Data from eligible studies were extracted independently by 2 reviewers (F.B., H.A.) using piloted electronic spreadsheets (Excel, Microsoft, Redmond, WA, USA). Consensus was achieved by discussion between the reviewers. Data were recorded according to guidelines outlined by the Cochrane Collaboration (Higgins and Green 2011) and another source (Deville et al. 2000). The following items were collected: study; year/country of study conductance; study type (clinical, in vitro, in situ); dentition (primary or permanent); tooth surface (proximal or nonproximal; i.e., occlusal, cervical, smooth surface); tooth location (anterior, posterior); lesion depth (extending only into enamel or extending into dentin, as determined via the reference test); restoration material (i.e., amalgam/other metals, composites/other tooth-colored materials); index test; reference test; number of examined teeth, surfaces, and patients. Accuracy data (true/false positive/negatives) were extracted in 3 data sets: the most sensitive reported set (i.e., the most sensitive applied cutoff or method specification), most specific (vice versa), and most accurate (i.e., highest combined value of sensitivity and specificity).
Risk of Bias Assessment
Risk of bias was assessed with the QUADAS-2 tool (Whiting et al. 2011). The following domains were recorded:
Selection—no inappropriate exclusions, no case-control design, random or consecutive inclusion
Index test—assessment blinded for and independent of reference test, defined cutoffs
Reference test—valid reference test, assessment independent from index test
Flow and timing—sufficient time between index and reference, all lesions submitted to same reference and all included in analysis
In addition, 3 of these domains were used to assess the applicability of the used methods according to the review question:
Selection—suitable lesions, realistic prevalence, and lesion spectrum
Index test—test, conduct, and interpretation matches to the review question
Reference test—identified condition matches the review question
Studies that had been performed in vitro were mostly found to have limited applicability in the domains “index test” and “test selection,” while for studies investigating artificially induced lesions, applicability concerns were assumed for the domain “reference test.” A prevalence of secondary lesions >15% in the test population was also found to limit applicability in the domain “test selection.” Studies with “low risk of bias” or “no applicability concerns” in all domains were categorized as “low risk of overall bias.” All other studies with “high” or “unclear” risks or concerns were rated “high overall risk.”
Summary Measures and Data Synthesis
Our unit of analysis was the assessed site. Sensitivity, specificity, positive and negative likelihood ratios, as well as diagnostic odds ratios (DORs) and their 95% confidence intervals were calculated as summary measures from the primary data set (most accurate). The DOR is the ratio of the odds of a positive test result in the diseased group relative to the odds of positive test result in the nondiseased group (Glas et al. 2003), and it ranges from zero (the worst possible diagnostic value) to infinity, with values of 1 indicating random accuracy and values >1 indicating useful test performances (Glas et al. 2003). We used DORs, as they are independent from prevalence and summarize accuracy data in 1 estimate. Data synthesis was performed via the Moses-Shapiro-Littenberg model (Moses et al. 1993). Given the limited number of studies, no subgroup analyses were performed. However, the location of the lesion (proximal/nonproximal) and the used cutoff (e.g., any or only ditches >200 µm) were graphically coded within summary receiver operating characteristic curves, which were used to graphically display potential sensitivity-specificity trade-offs.
Cochran’s Q and I2 statistics (Higgins and Thompson 2002) were used to evaluate potential heterogeneity among studies, with heterogeneity being assessed via DORs. Funnel plot analysis and 1-sided Egger regression test were performed to assess small study effects or publication bias (Egger et al. 1997; Higgins and Green 2011). To calculate adjusted DORs accounting for possible publication bias, we imputed DOR values not missing at random (Duval and Tweedie 2000) and reassessed pooled DORs. Meta-regression analyses were used to explore the influence of the following potential confounders: setting (clinical or in vitro), dentition (primary or permanent), surfaces (nonproximal or proximal), restoration material (amalgam or tooth colored), lesion depths (all lesions or only lesions extending into dentin; i.e., advanced lesions). Metaregression (subgroup comparison) was performed on diagnostic accuracy (DORs) based on the unrestricted maximum-likelihood method, with relative DORs as relative effect estimates for differences between groups. Data were analyzed with MetaDisc 1.4 (Unidad de Bioestadistica Clínica del Hospital Ramón y Cajal, Madrid, Spain) and Comprehensive Meta-analysis 2.2.64 (Biostat, Englewood, NJ, USA).
Results
Searching 1 database (Medline) yielded 1,179 studies, of which 60 were potentially eligible and assessed full-text (Fig. 1). Screening of other databases (Embase/Central) and cross-referencing did not yield further full-text records to be assessed. Twenty-three studies were eventually included (Table 1); reasons for exclusion can be found in Appendix Table 1. Included studies were published between 1991 and 2015 in the United States (n = 4), the Netherlands (n = 4), Brazil (n = 5), Switzerland (n = 2), United Kingdom (n = 3), Sweden (n = 2), Thailand (n = 1), Turkey (n = 1), and Norway (n = 1). Most were performed in vitro (n = 21); only 2 studies investigated caries detection under clinical conditions. The majority assessed caries lesion detection in permanent teeth (n = 21); only 2 assessed primary teeth. Evaluated lesions were mostly located on proximal surfaces (14 studies), with the majority of studies assessing mainly posterior teeth (n = 22). The materials adjacent to the assessed surfaces were amalgam (n = 13) and composites or other tooth-colored materials (n = 7); 3 studies assessed both materials and did not specify the number of differently restored teeth. The number of assessed teeth varied between 15 and 161; the mean number of assessed sites was 114.
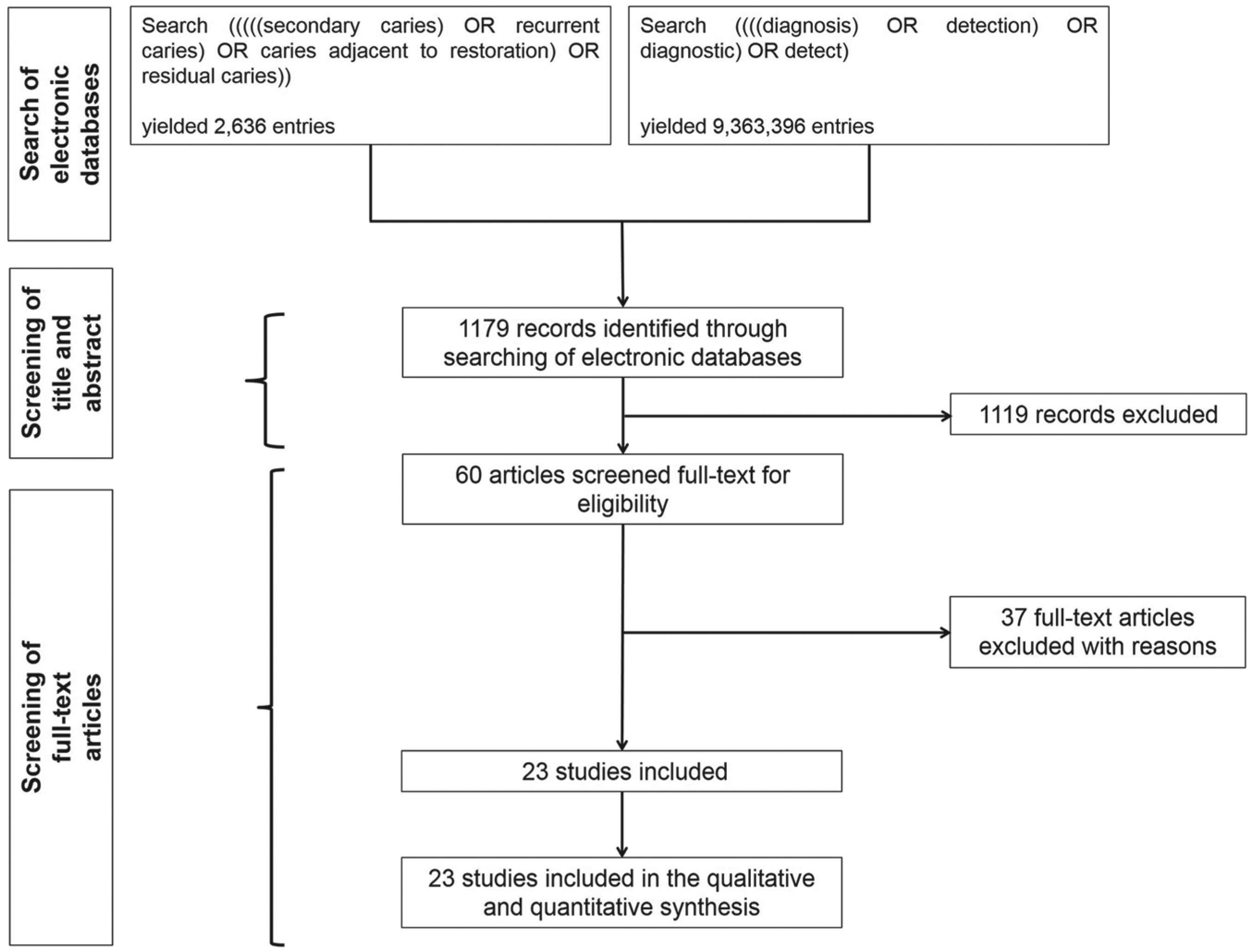
Flowchart of the search.
Included Studies.
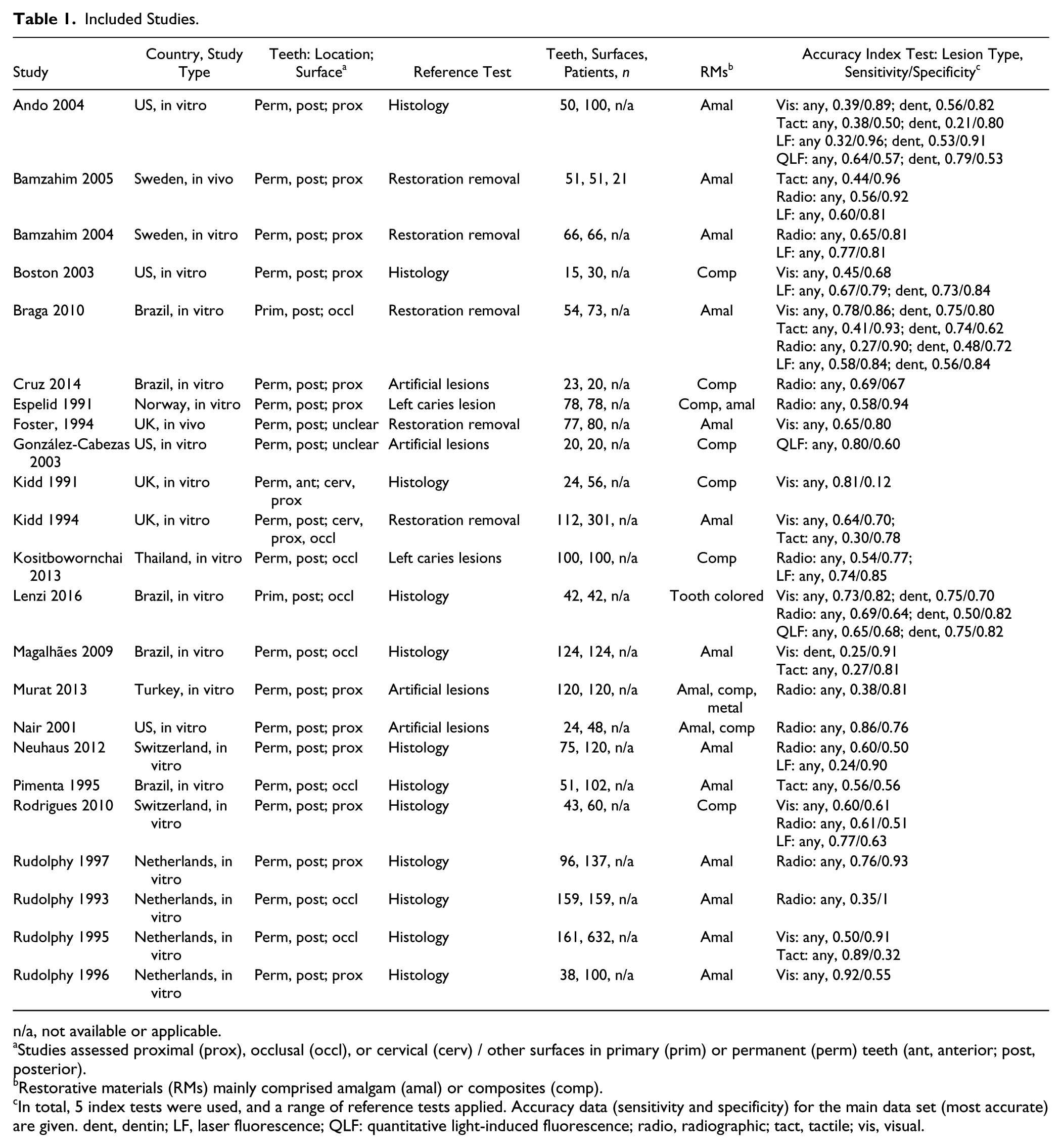
n/a, not available or applicable.
Studies assessed proximal (prox), occlusal (occl), or cervical (cerv) / other surfaces in primary (prim) or permanent (perm) teeth (ant, anterior; post, posterior).
Restorative materials (RMs) mainly comprised amalgam (amal) or composites (comp).
In total, 5 index tests were used, and a range of reference tests applied. Accuracy data (sensitivity and specificity) for the main data set (most accurate) are given. dent, dentin; LF, laser fluorescence; QLF: quantitative light-induced fluorescence; radio, radiographic; tact, tactile; vis, visual.
The following index tests were used: visual (i.e., assessment of discoloration; n = 6), staining (n = 3), or other visually detectable changes (n = 3); tactile (i.e., assessment of ditching; n = 8); radiographic assessment (i.e., only radiographic; n = 12) or combined visual-radiographic assessment (n = 1); laser fluorescence (n = 8); and QLF (n = 3). Used reference tests were histologic assessment (n = 12) or removal of the restoration and assessment for possible dentin softening (n = 5); 6 studies used artificially induced lesions or intentionally left carious tissue beneath the restoration.
Sensitivity was highest and specificity lowest for QLF; these estimates were supported by only 3 studies (Table 2). In contrast, sensitivity was lowest while specificity was highest when tactile detection methods were used. Visual, radiographic, and laser fluorescence detection had similar sensitivities (from mean 0.50 to 0.59) and specificities (from mean 0.78 to 0.83). All methods yielded positive likelihood values >1 but also showed negative likelihood values significantly <1. Heterogeneity was high in studies investigating established methods (visual-tactile and radiographic assessment) and low in studies investigating newer methods.
Validity and Subgroup Analysis for Different Detection Methods of Secondary Caries Lesions.
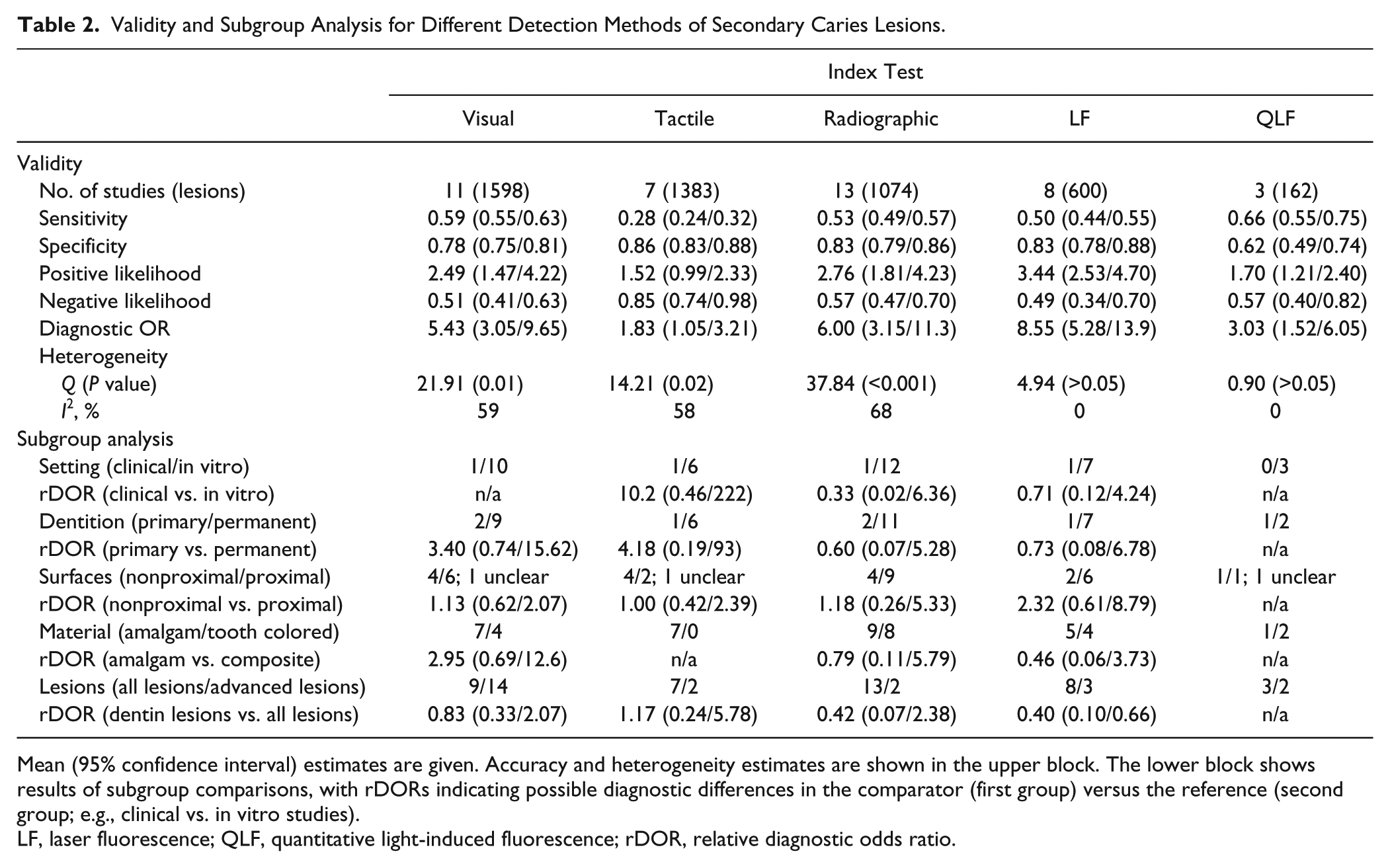
Mean (95% confidence interval) estimates are given. Accuracy and heterogeneity estimates are shown in the upper block. The lower block shows results of subgroup comparisons, with rDORs indicating possible diagnostic differences in the comparator (first group) versus the reference (second group; e.g., clinical vs. in vitro studies).
LF, laser fluorescence; QLF, quantitative light-induced fluorescence; rDOR, relative diagnostic odds ratio.
Metaregression found only limited impact of effect modifiers (Table 2), with no significant differences between subgroups of studies (in vitro vs. clinical), dentitions (primary vs. permanent), or materials (amalgam vs. tooth colored). There was a trend that detection on nonproximal (occlusal, cervical) had higher diagnostic value than detection on proximal surfaces (relative DOR [95% confidence interval] was between 1.00 [0.42 to 2.39] and 2.32 [0.61 to 8.79]).
Sensitivities and specificities were subsequently reflected by summary receiver operating characteristic curves (Figs. 2, 3). Visual detection was more accurate than tactile detection, which had poor overall accuracy (Fig. 2a, c). For visual detection, no clear pattern emerged if staining as criterion was more sensitive/specific than other visual criteria. For tactile detection, increasing the cutoff to significant ditching (>200 µm) decreased sensitivity but increased specificity. For both analyses, there was strong indication for publication bias by statistical analysis and funnel plot assessment (Fig. 2b, d).
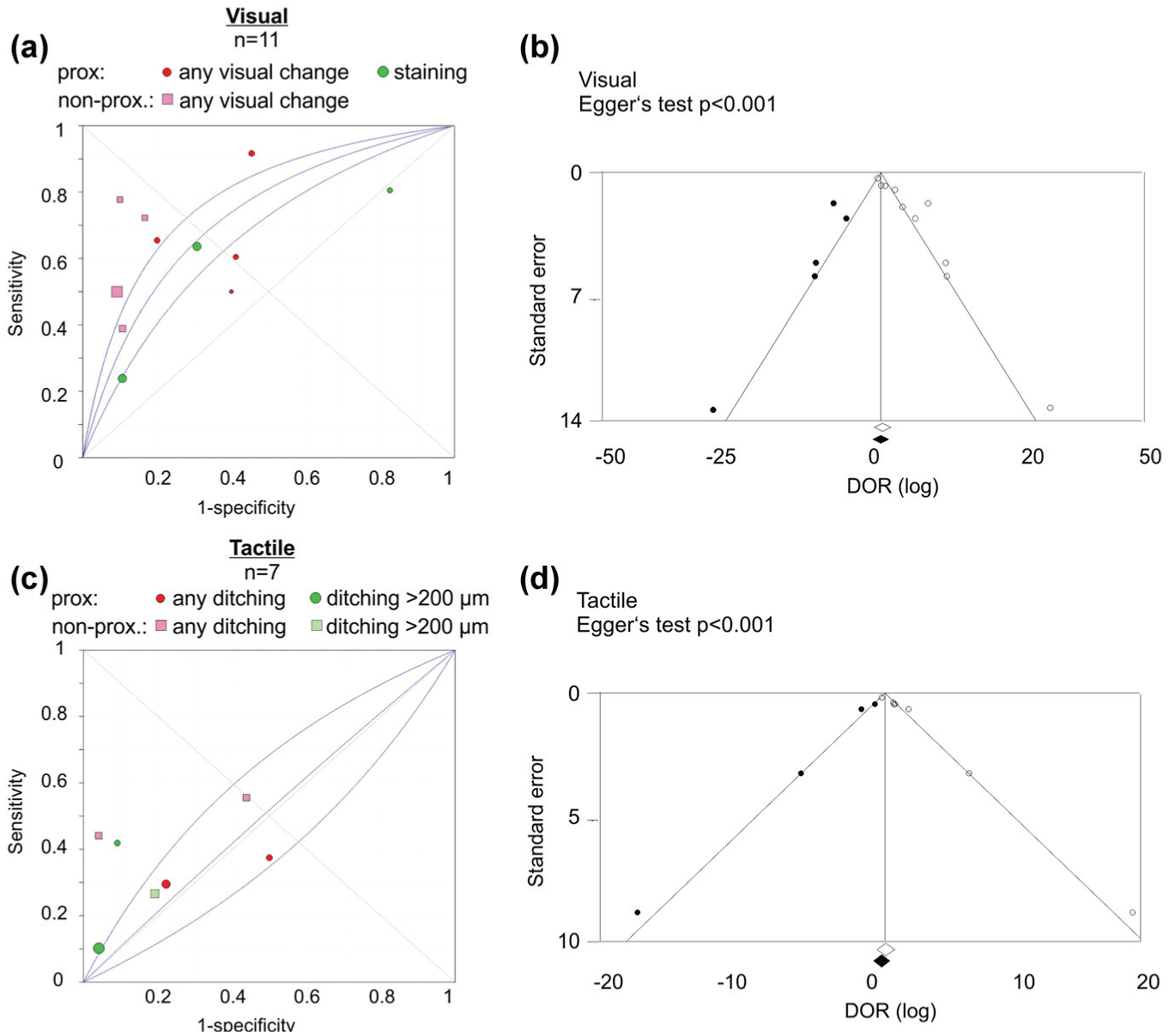
Summary receiver operating characteristic (sROC) curves (left) and funnel plots (right) for visual (
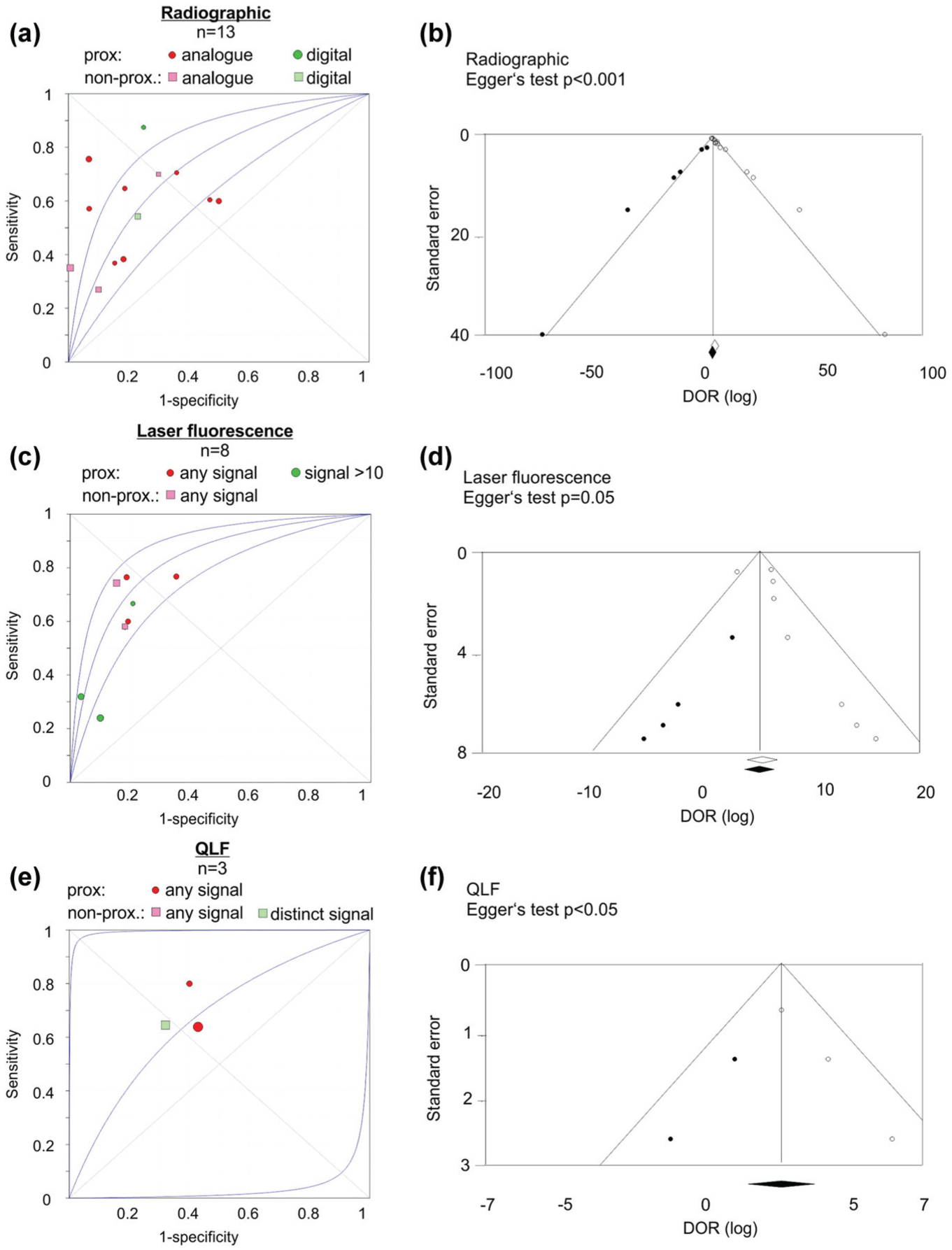
Summary receiver operating characteristic (sROC) curves (left) and funnel plots (right) for radiographic (
More advanced detection methods had only limited advantages when compared with only visual assessment, with radiographic, laser fluorescence, and QLF detection being similarly, more, and less accurate than visual detection, respectively (Fig. 3a, c, e). For laser fluorescence, using a higher cutoff value increased specificity but decreased sensitivity. For radiography and QLF, there was strong indication for publication bias (Fig. 3b, d, f).
Overall risk of bias was high in all studies (Fig. 4). The full documentation of risk of bias can be found in Appendix Table 2. Given that most studies were in vitro, the applicability of the lesion selection process was frequently rated as unclear, while the study flow was often unclear due to poor reporting. Risks of test selection bias varied among studies applying different detection methods and was highest for studies using visual assessment and laser fluorescence, and lowest for QLF (Appendix Table 3). Risk associated with index or reference tests were limited in the majority of trials regardless of the method (only for visual assessment, 64% studies were prone for bias by reference test choice or conduct). Flow and timing were least prone for bias in QLF studies. Nearly all studies had high risk of applicability concerns regarding test selection, regardless of the detection method investigated. The conduct of index tests was least prone to bias in studies involving radiographic methods, while reference standards were least prone for bias in laser fluorescence and QLF studies.
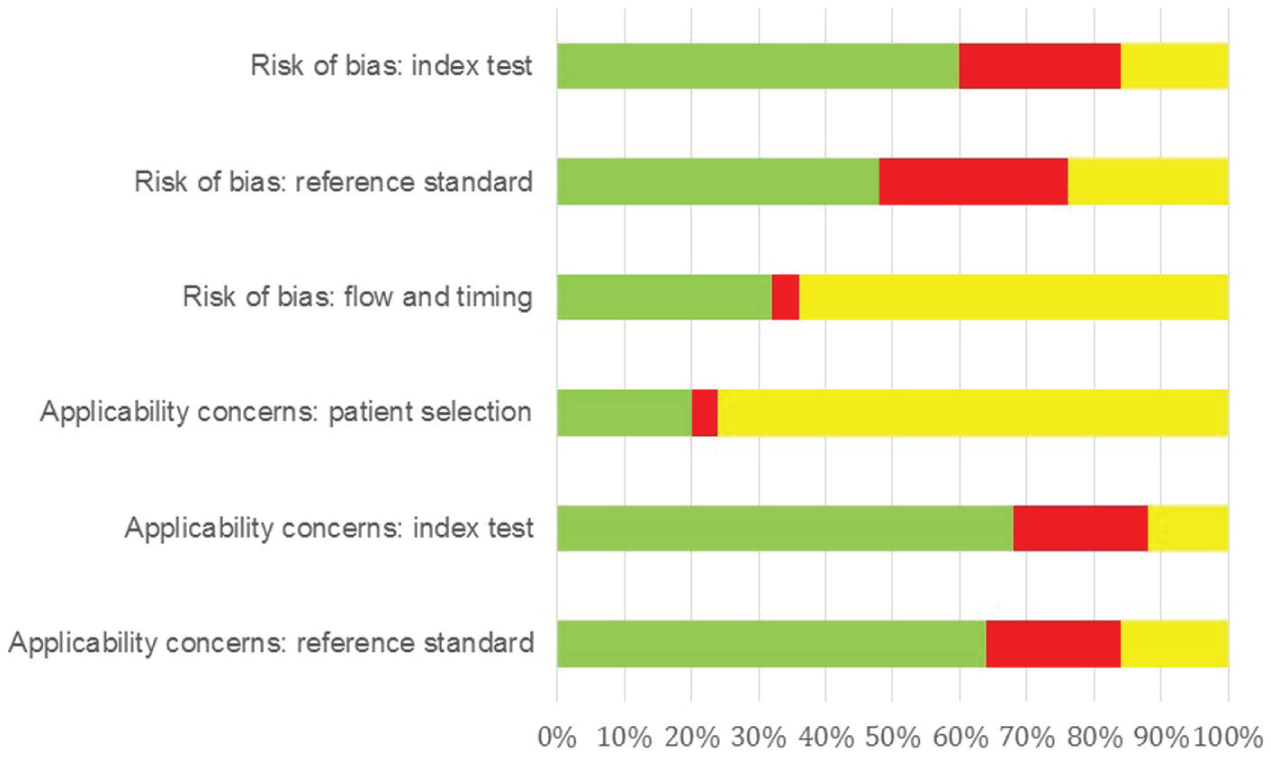
Risk of bias. Studies were assessed for risk of bias and applicability concerns. The proportion of studies with low (green), high (red), and unclear bias or concerns in each domain are shown (in percentages). This figure is available in color online at http://jdr.sagepub.com.
Discussion
The present study systematically reviewed different methods for detecting secondary caries lesions. While early detection of such lesions might be important to guide minimally invasive mending of the restoration and prevent further loss of dental tissues in critical (e.g., equi- or subgingival) areas, false-positive diagnoses could translate into unnecessary and costly retreatments. Only few studies investigated secondary lesion detection, most of them with high risk of bias and applicability concerns. The latter was not particularly concentrated on studies using a specific index tests—that is, the limitations of the available data apply to all methods evaluated by the present review.
Visual change adjacent to restorations (i.e., discolorations, staining, or dentinal shading) may be caused by a lot of factors, only 1 of them being secondary caries lesions (Ando et al. 2004). Overall, performing visual assessment had moderate sensitivity (0.59) and relatively high specificity (0.78), the latter being especially high on occlusal or smooth compared with proximal surfaces. In clinical terms, using visual assessment only would mean around 40% of secondary lesions to be missed, while 20% of sound surfaces might be diagnosed as carious. We separately investigated studies assessing (peri)margin staining, as this criterion has been criticized before to lack validity (Kidd et al. 1995; Kidd and Beighton 1996). We could not confirm significantly increased or decreased validity when using this instead of other visual criteria. Visual assessment seemed to yield higher accuracy adjacent to amalgam than composite restorations, with staining or discoloration having potentially limited validity adjacent to composite. However, even for amalgam, it remains unclear if absence of any staining or shade is a good predictor for the absence of secondary caries (Rudolphy et al. 1995) or not (Kidd et al. 1995). It should be further noted that all but 2 studies applying visual criteria were performed in vitro and might thus have limited generalizability, with potentially decreased accuracy in clinical settings given the presence of saliva, plaque, or gingival tissues. While the setting affects the applicability of our findings, the use of in vitro studies might be justified for assessing diagnostic test accuracy given the lack of a clinical noninvasive “gold standard” reference. Future research might overcome this dilemma by establishing such a standard test (best with a widely accepted and valid outcome parameter) or by using different study designs, such as prospective clinical studies for evaluating predictive, not criterion, validity. In summary, visual inspection might be useful for detecting secondary caries on nonproximal surfaces adjacent to amalgams. For other surfaces or tooth-colored materials, the lack of reliability and accuracy might limit its suitability for detecting secondary lesions.
Traditionally, secondary caries lesions were assessed via tactile examination. This method seemed to be specific (specificity increased even further if only clearly detectable ditches were regarded as lesions) but insensitive. In clinical terms, only few secondary lesions would be detected, while the risk of false-positive detections was not drastically decreased compared with, for example, visual detection. Significant ditching in restoration margins were found to be correlated with secondary caries lesions, harboring great numbers of bacteria (Kidd et al. 1995). Accuracy of tactile assessment seemed similar on proximal and occlusal surfaces. Again, adjusting for potential publication bias significantly decreased diagnostic accuracy. Overall, tactile assessment might be unsuitable to reliably detect secondary caries lesions of the spectrum used in included studies. For clearly cavitated secondary lesions, tactile assessment might well be a useful method, as both sensitivity and specificity are presumably increased.
Radiographic assessment is regularly performed to screen for proximal primary or secondary caries lesions. Based on this review, the accuracy of radiographic detection of secondary lesions varies greatly among studies, while assessment of confounders (e.g., analogue versus digital detection methods, location of the assessed surface, restoration material adjacent to the lesion) could not indicate reasons for such heterogeneity. Overall, sensitivity of this method was moderate (0.53) while specificity was high (0.83), limiting the risk of overdiagnosis and overtreatment. Nevertheless, nearly half the lesions would not be detected if only radiographic detection was used. That said, the risk stemming from such nondetection largely depends on the progression speed of such lesions, which is so far not fully understood. Visual and radiographic assessment might be complementary when nonproximal and proximal surfaces are checked, respectively. Again, most studies were performed in vitro; however, the impact of such artificial setting on generalizability could be lower for this than other (e.g., visual) methods given its relative independence from clinical parameters. The associated ionizing radiation limits the applicability of this method, especially in certain settings and populations (e.g., children).
Laser fluorescence–based instruments have been developed as an adjunct to visual lesion detection (Boston 2003), not causing any radiation and allowing easy reexamination and monitoring of lesions and their activity. This method had useful accuracy, not only but especially on nonproximal surfaces and with a certain numeric threshold (e.g., >10 fluorescence units). Overall accuracy was similar to that of radiographic detection, which makes it a potential alternative, especially in children. It should be noted that available studies indicated a potentially limited accuracy when detecting lesions adjacent to amalgam, which might be due to absorption, scattering, or reflections caused by the material.
QLF showed the highest sensitivity (0.66) and lowest specificity (0.62), supported by only 3 studies. Given that QLF is currently available just for visible (nonproximal) surfaces, the value of this method for detecting secondary lesions might be limited in clinical routine. Moreover, given the fact that even on these visually assessable surface, QLF led to false-positive detections in nearly 4 of 10 cases, there should be severe doubts toward the suitability of this method for the outlined purpose.
This review has several limitations. First, a relatively small number of studies were included, most of them having been performed in vitro, with high risk of bias and limited applicability. While our search strategy was built on a combination of the target condition (secondary lesion) and the study objective (assessment of diagnostic test accuracy), some studies with insufficient indexing, which can be expected in this field, might not have been retrieved. However, by searching several databases and performing hand and gray literature searches, we aimed to search as sensitive as possible to identify relevant studies. Moreover, most comparisons seemed to suffer from publication bias, casting doubts on the true accuracy of some methods. It should be noted that for DORs, statistical tests for publication bias are prone for type II error, with funnel plot inspection being more robust (Deeks et al. 2005). Second, a great number of potential confounders might have affected our results and might have caused the reported heterogeneity. We tried to account for these using graphic or statistical tools. The latter was performed via metaregression (subgroup comparison), with very limited power for detecting significant difference between groups given the number of assessed studies. Such confounders include the setting or the dentition—that is, most studies were performed in permanent teeth, and so the generalizability of our findings into the primary dentition cannot be assumed. Moreover, a variety of reference tests were used, all having limited accuracy, too. Another confounder was the index tests themselves, which were subsumed into the described 5 categories, while within each category, the applied tests differed as well (e.g., different devices and applied thresholds). We tried to account for this by extracting the most accurate but also the most sensitive and specific data set; readers can thus evaluate how the differential application of each test affects the sensitivity-specificity tradeoff. A last possible confounder is the used restoration material, which affects both the development of secondary caries lesions and their detection (e.g., different surface textures, margin adaptions, radio-opacities; Ben-Amar and Cardash 1991; Lai et al. 2013). Third, this review was not registered a priori, which introduces risk of bias during the review process. Fourth, the yielded meta-analytic results pooled sensitivities and specificities from studies with different thresholds, resulting in an average estimate. This was done because too few studies were available for pooling results at different thresholds. The separate inspection of summary receiver operating characteristic plots is required to fully assess the impact of a detection method being used at different cutoffs. Moreover, the applied model for meta-analysis is widely established for synthesis of diagnostic test accuracies but does not fully account for heterogeneity among studies and is suitable for exploratory analyses only. In future reviews that attempt statistical comparison of different methods and their accuracies, hierarchical models might be better suited (Rutter and Gatsonis 2001). Last, this study focused on the accuracy of tests according to a gold standard, which has limited benefit for patients: Patients might not care for the “true” status of their restoration but rather the treatment decisions stemming from certain diagnostic findings and the associated costs, benefits, or risks (Baelum et al. 2012; Schwendicke et al. 2015).
In conclusion, although secondary caries lesions are a significant clinical and dental public health problem, their detection has been assessed by only a few studies. In contrast, a relative high number of different detection methods was applied. Based on the limitations of this review and the internal validity and applicability of the included studies, visual, radiographic, and laser fluorescence detection might be useful to detect secondary lesions. Tactile assessment of (peri)margin areas had limited value in the used lesion spectrum. QLF has only sparsely been investigated and does currently not seem to convey any diagnostic benefit. There is great need for more studies in this field; such studies will require an agreed reference standard and should use comparable designs with robust internal and external validity to ease synthesis and evidence translation into practice.
Author Contributions
F. Brouwer, F. Schwendicke, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; H. Askar, contributed to data acquisition and interpretation, critically revised the manuscript; S. Paris, contributed to data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
This study was funded by the authors and their institutions. F.S. received a grant from the German Research Foundation (DFG Schw-1766/2-1).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.