
Abstract
Biological mediators have been used to enhance periodontal regeneration. The aim of this prospective randomized controlled study was to evaluate the safety and effectiveness of 3 doses of fibroblast growth factor 2 (FGF-2) when combined with a β-tricalcium phosphate (β-TCP) scaffold carrier placed in vertical infrabony periodontal defects in adult patients. In this double-blinded, dose-verification, externally monitored clinical study, 88 patients who required surgical intervention to treat a qualifying infrabony periodontal defect were randomized to 1 of 4 treatment groups—β-TCP alone (control) and 0.1% recombinant human FGF-2 (rh-FGF-2), 0.3% rh-FGF-2, and 0.4% rh-FGF-2 with β-TCP—following scaling and root planing of the tooth prior to a surgical appointment. Flap surgery was performed with EDTA conditioning of the root prior to device implantation. There were no statistically significant differences in patient demographics and baseline characteristics among the 4 treatment groups. When a composite outcome of gain in clinical attachment of 1.5 mm was used with a linear bone growth of 2.5 mm, a dose response pattern detected a plateau in the 0.3% and 0.4% rh-FGF-2/β-TCP groups with significant improvements over control and 0.1% rh-FGF-2/β-TCP groups. The success rate at 6 mo was 71% in the 2 higher-concentration groups, as compared with 45% in the control and lowest treatment groups. Percentage bone fill in the 2 higher-concentration groups was 75% and 71%, compared with 63% and 61% in the control and lowest treatment group. No increases in specific antibody to rh-FGF-2 were detected, and no serious adverse events related to the products were reported. The results from this multicenter trial demonstrated that the treatment of infrabony vertical periodontal defects can be enhanced with the addition of rh-FGF-2/β-TCP (ClinicalTrials.gov NCT01728844).
Keywords
Introduction
Periodontal regeneration is a complex process involving multiple hard and soft tissues. It is an unrealistic expectation that significant regeneration can occur after treatment of periodontally diseased teeth without the addition of some type of graft materials. Furthermore, if the graft material is biologically passive and serves only as a space filler, limited regeneration may occur (Reynolds et al. 2010). Increasing evidence suggests that biologically active graft materials such as protein growth factors are required to stimulate increased amounts of cementum, periodontal ligament, and bone (Kao et al. 2015). Only 2 protein materials are approved by the U.S. Food and Drug Administration to treat infrabony periodontal defects. These products include a mixture of heterogeneous proteins from the enamel organ (Sculean et al. 2011) and a recombinant growth factor (Nevins et al. 2005; Nevins et al. 2013). The latter protein therapy requires a β-tricalcium phosphate (β-TCP) carrier for delivery. The role of the carrier is not well understood, and the enamel matrix proteins have been shown to stimulate significant regeneration with and without bone graft carriers in various-sized periodontal defects (Cochran, Jones, et al. 2003; Cochran, King, et al. 2003). Furthermore, a member of the bone morphogenetic protein family, growth and differentiation factor 5, has also been shown to stimulate significant periodontal regeneration in baboon defects when combined with β-TCP (Emerton et al. 2011) and in humans (Stavropoulos et al. 2011). Thus, it appears that the regeneration of periodontal defects is best achieved when an active biological factor is present, and in some cases, it requires the presence of a solid scaffold carrier.
One prerequisite of any tissue formation is the presence and growth of new blood vessels or angiogenesis. This complex but coordinated process involves the migration, proliferation, and differentiation of several cell types and is regulated by a number of factors, including matrix proteins, growth factors, cytokines, and chemokines (Barrientos et al. 2008). One important molecule in this process is fibroblast growth factor 2 (FGF-2) or basic fibroblast growth factor. This growth factor is increased in acute wound healing and plays a role in granulation tissue formation and tissue remodeling (Bikfalvi et al. 2009). FGF-2 acts by binding to heparin and has broad mitogenic and angiogenic actions. It also acts early in the differentiation of osteoprogenitor cells to increase bone formation, and it stimulates periodontal ligament cell proliferation and migration, which makes it an attractive candidate for periodontal regeneration therapy (Murakami 2011). Furthermore, FGF-2 has been shown to significantly stimulate periodontal regeneration in large multicenter double-blinded randomized controlled studies when combined with a gel-like hydroxypropyl cellulose (HPC) viscous solution (Kitamura et al. 2008; Kitamura et al. 2011; Kitamura et al. 2015).
The purpose of this study was to evaluate the safety and effectiveness of 3 doses of FGF-2 when combined with a β-TCP scaffold carrier placed in vertical infrabony periodontal defects in adult patients.
Materials and Methods
Trial Design
This multicenter randomized controlled clinical trial was designed as a prospective, double-blinded, dose-escalation study in patients who required surgical intervention to treat a qualifying periodontal defect. The duration of the trial was 6 mo following implantation of the investigational device. A total of 94 patients were anticipated to be randomized to obtain at least 80 evaluable patients based on an assumed 15% dropout rate. Six sites in the United States participated in the trial. The study received Institutional Review Board approval at each investigational site or at a centralized Institutional Review Board prior to commencement of the study. No significant changes occurred in the trial design after commencement of the study.
Participants
Men and women >25 years old who could read, understand, and agree to provide consent and who were able and willing to follow study procedures and instructions were evaluated for study inclusion. The patient also had to have a tooth (target) with a pocket depth ≥7 mm with a ≥4-mm infrabony defect and at least 1 bony wall. Sufficient keratinized tissue for complete tissue coverage had to be present, and the radiographic base of the defect had to be at least 3 mm coronal to the apex of the tooth. The sites of the study included 3 universities—The University of Texas Health Science Center at San Antonio, the University of Michigan School of Dentistry, and the University of Alabama at Birmingham—plus 3 private periodontal practices in Fullerton, California; Aurora, Colorado; and Houston, Texas.
Investigational Device and Interventions
This trial used recombinant human FGF-2 (rh-FGF-2; Kaken Pharmaceutical Co., Ltd., Tokyo, Japan) produced by genetic recombination that transformed Escherichia coli with the human gene FGF2. The lyophilized rh-FGF-2, β-TCP, and 1% HPC solution were supplied to a contract manufacturing facility (Fisher Clinical Service, Mount Prospect, IL, USA), assembled into a kit, and labeled with a randomization code generated by the contract facility. After signing an informed consent form, being screened, having scaling and root planing (≥2 wk before baseline visit), and having baseline measurements taken, patients meeting inclusion and not meeting any exclusion criteria were randomized to 1 of 4 treatment groups—β-TCP plus lyophilized placebo (the active control) and β-TCP plus 0.1%, 0.3%, or 0.4% rh-FGF-2—so that treatment was balanced within each investigational site and according to smoking status.
Outcomes
The primary outcome measure was a composite end point combining the amount of radiographic linear bone growth (LBG) and clinical attachment gain from baseline at 6 mo postimplantation. The thresholds were 1.5 mm for change in attachment level and 1 mm for LBG. LBG threshold at 2.5 mm was also used to be consistent with the LBG observed from a systematic review of the literature of other leading products (Reynolds et al. 2010). Secondary outcome measures included the following: mean clinical attachment level (CAL) change at 3 and 6 mo, LBG and percentage bone fill at 6 mo, probing depth reduction at 3 and 6 mo, changes in gingival recession at 3 and 6 mo, wound healing at 2 and 4 wk, and bleeding on probing at 3 mo. Safety was monitored throughout the study by assessing the incidence, timing, and severity of adverse events (AEs) as well as by analyzing serum at 2 and 4 wk for antibody formation against rh-FGF-2.
Sample Size, Blinding, Calibration, and Statistical Analyses
Sample size was based on a 2-sided 2-sample unequal variance Student’s t test with an overall 5% significance level for comparison of test versus active control. With a minimum of 20 patients per treatment group, the power is at least 80% to detect a difference of 1.70 mm in LBG, which was referred to as the result of a previous clinical trial (Nevins et al. 2005). The randomization was performed intraoperatively after surgeons confirmed target site inclusion. The investigator and all study personnel were blinded to treatment. Calibrated examiners who performed evaluations were different from the surgeons administering the device and were blinded to the investigational device implantation of all patients for the length (6 mo) of the study. The radiographs were sent to the central reader (the University of Alabama at Birmingham), where they were processed and analyzed. All examiners from the investigational sites went through a training and calibration exercise at The University of Texas Health Science Center in San Antonio before they participated in the study. All statistical analyses were performed with SAS 9.3 (SAS Institute, Cary, NC, USA). The probability level of statistical significance was set to P < 0.05.
Results
A total of 143 subjects were assessed for eligibility at 6 study sites. In total, 88 eligible subjects were randomized in almost equal proportions to 1 of 4 treatment groups—β-TCP alone (control), 0.1% rh-FGF-2, 0.3% rh-FGF-2, and 0.4% rh-FGF-2 with β-TCP treatment—ranging from 21 to 23 subjects each (Fig. 1). One subject was dropped from the study due to a head injury that resulted in his death after 2 wk postsurgery. Two subjects were lost to follow-up after 4 wk and 3 mo postsurgery, respectively. In total, 85 patients completed the study, and the data were analyzed for baseline characteristics and safety analyses according to the intent-to-treat population. The per-protocol population consisted of 83 patients after 2 were removed for lack of compliance with the study protocol. Effectiveness was analyzed with per-protocol population. The study began on November 26, 2012, and enrollment was closed on December 16, 2013.
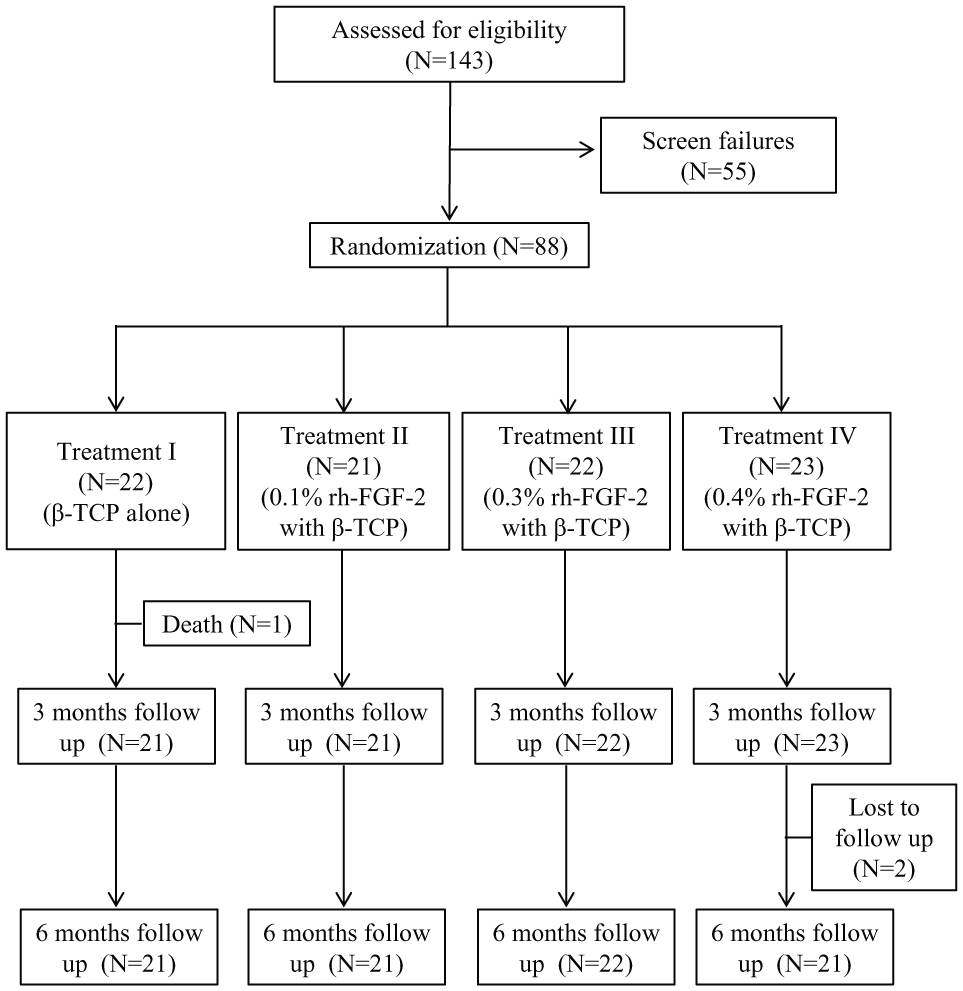
Trial flowchart for the 6-mo study. β-TCP, β-tricalcium phosphate; rh-FGF-2, recombinant human fibroblast growth factor.
There were no statistically significant differences in subject demographics and baseline characteristics among the 4 treatment groups, with most patients (81% to 87%) being nonsmokers (Table 1). Most teeth (71% to 82%) were treated in the mandibular arch. Averages of approximately 3 mm of CAL gain and pocket depth reduction were achieved in all treatment groups at 3 mo after surgery (Table 2). There was no statistically significant difference in frequency distribution of CAL gain ≥3 and <3 mm among the 4 treatment groups (data not shown). This means that the standard treatment was successfully provided at all clinical sites through the study period.
Patient and Study Site Characteristics at Baseline.
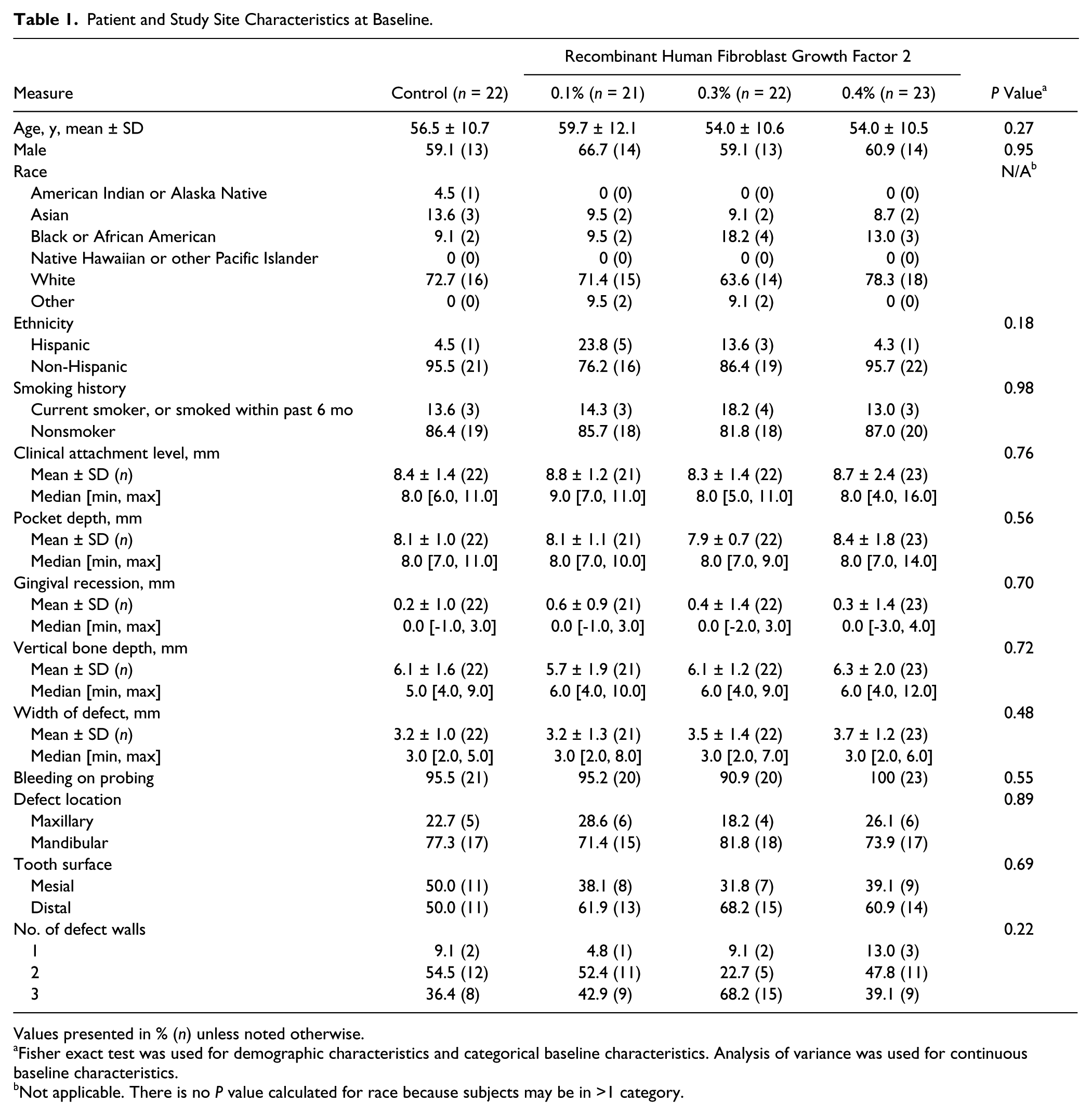
Values presented in % (n) unless noted otherwise.
Fisher exact test was used for demographic characteristics and categorical baseline characteristics. Analysis of variance was used for continuous baseline characteristics.
Not applicable. There is no P value calculated for race because subjects may be in >1 category.
Clinical Outcome.
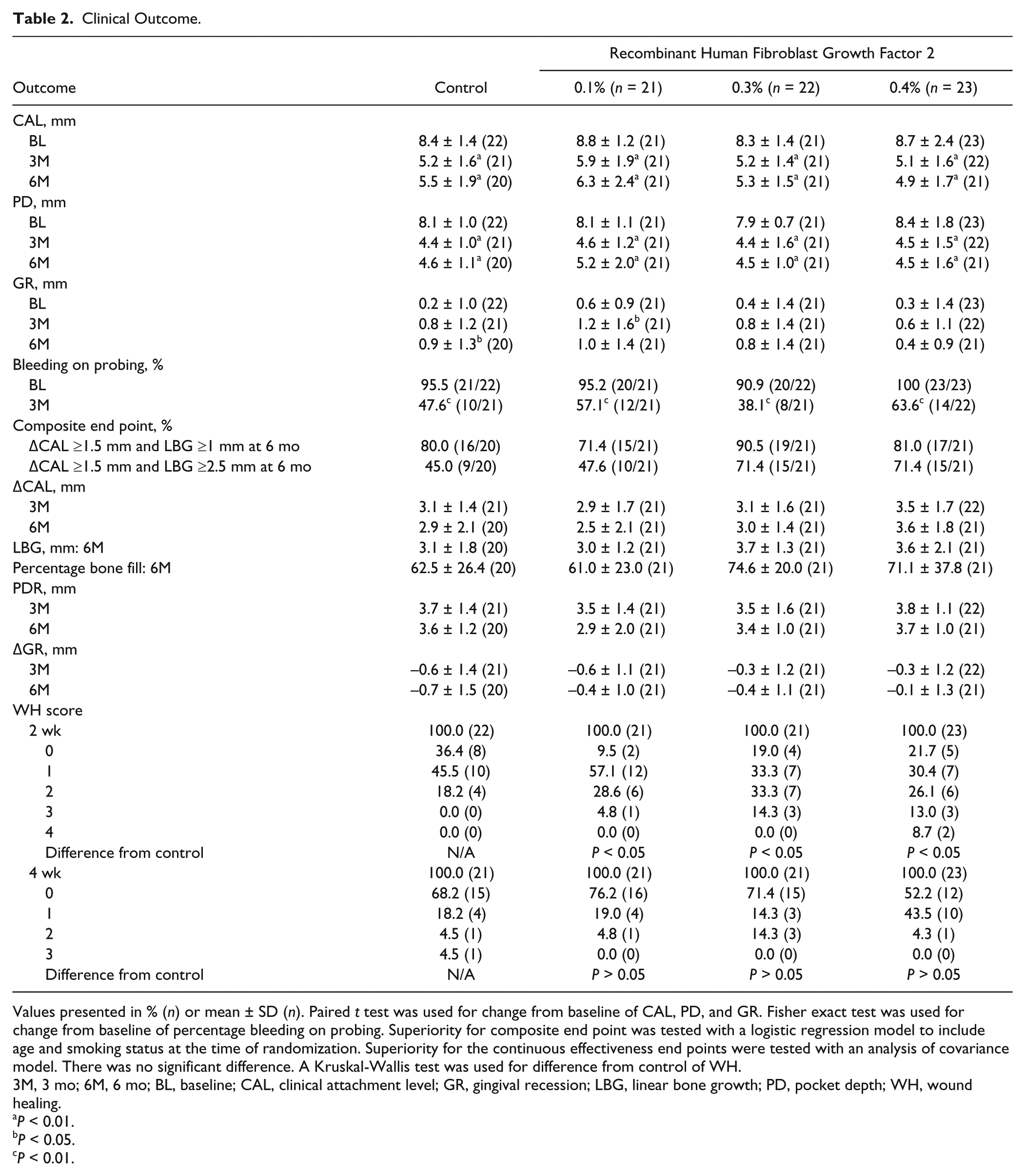
Values presented in % (n) or mean ± SD (n). Paired t test was used for change from baseline of CAL, PD, and GR. Fisher exact test was used for change from baseline of percentage bleeding on probing. Superiority for composite end point was tested with a logistic regression model to include age and smoking status at the time of randomization. Superiority for the continuous effectiveness end points were tested with an analysis of covariance model. There was no significant difference. A Kruskal-Wallis test was used for difference from control of WH.
3M, 3 mo; 6M, 6 mo; BL, baseline; CAL, clinical attachment level; GR, gingival recession; LBG, linear bone growth; PD, pocket depth; WH, wound healing.
P < 0.01.
P < 0.05.
P < 0.01.
Statistically significant differences were not detected between the control group (β-TCP alone) and test groups in the primary composite end point when the threshold setting of LBG was 1 mm, because the majority of subjects in all treatment groups met the success criteria. When the LBG threshold was changed to 2.5 mm, the increase of the success rates of the 0.3% rh-FGF-2 group (71.4%) and 0.4% rh-FGF-2 group (71.4%) became more apparent when compared with the control group (45%); however, a statistically significant difference was not confirmed (P = 0.076 and P = 0.087, respectively; Table 2). When the threshold of LBG is 2.5 mm, the dose response pattern detected by a dose selection analysis showed a plateau in the 0.3% rh-FGF-2 group, with similar performance in 0.4% rh-FGF-2 group.
The mean change in CAL was greater than the historically based success criterion in open flap debridement (1.5 mm; Laurell et al. 1998) of clinical effectiveness in all treatment groups at 3 mo (2.9 to 3.5 mm) and 6 mo (2.5 to 3.6 mm) postimplantation (Table 2). Linear bone growth was 3.7 and 3.6 mm in the 0.3% and 0.4% rh-FGF-2 groups, compared with 3.1 mm in the control and 3.0 in the 0.1% rh-FGF-2 group. Percentage new bone growth was 75% and 71% in the 0.3% and 0.4% rh-FGF-2 groups, compared with 63% in the control and 61% in the 0.1% rh-FGF-2 group. At 3 mo postsurgery, pocket depth reduction was similar (3.5 to 3.8 mm) among all treatment groups and there was not a significant change between 3 and 6 mo. Furthermore, after 3 mo, the change in gingival recession was less in the 0.3% and 0.4% rh-FGF-2 groups (–0.3 mm) compared with the control group (–0.6 mm). Bleeding on probing was also reduced from baseline to 3 mo by 40% to 50% in all treatment groups. The wound healing scale at 2 wk after treatment was significantly greater in the rh-FGF-2 treatment groups than in control (P < 0.05); however, by 4 wk, there were no statistically significant differences among all groups (Table 2). No subjects experienced an increase of specific antibody during the study. Of the 75 AEs reported, 4 were serious AEs. All 4 serious AEs were determined by the principal investigators to be non-device-related AEs. Furthermore, although 17 patients reported 24 AEs in the control group—which was twice the number reported in the 0.3% rh-FGF-2 group—there were no significant differences in the number of patients who reported AEs among the 4 treatment groups. No hard tissue abnormalities, including ankylosis, were observed through radiographic assessment. Representative radiographic images for 0.3% and 0.4% rh-FGF-2 and control groups are shown in Figure 2B—D.
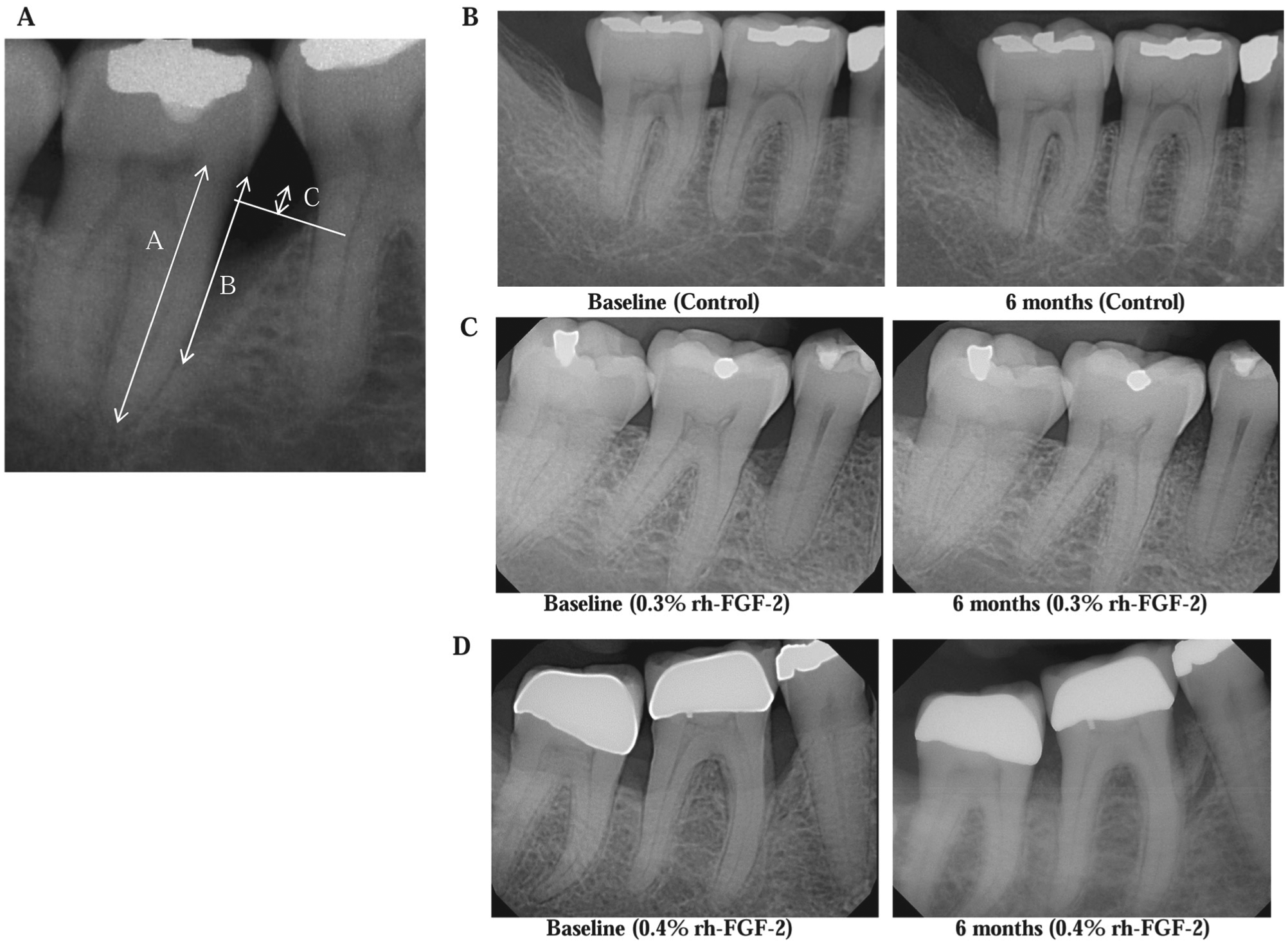
Radiographic assessment. (
Dose evaluation was based on a number of factors, with one of which being the primary composite end point but using success criteria for LBG ≥2.5 mm as noted above. Five dose response patterns were examined and modeled statistically with the Wald statistic. This analysis indicated that the dose response pattern is considered to reach a plateau in 0.3% rh-FGF-2 and that the performance of 0.3% rh-FGF-2 will be similar to that of 0.4% rh-FGF-2. A post hoc exploratory analysis examined the additional value of rh-FGF-2 when added to β-TCP by defect type based on percentage bone fill. This analysis demonstrated that the addition of rh-FGF-2 resulted in a statistically significant improvement of approximately 20% in bone fill in 1- and 2-wall defects (P < 0.05; Fig. 3). No differences occurred in 3-wall defects compared with control in this post hoc analysis.
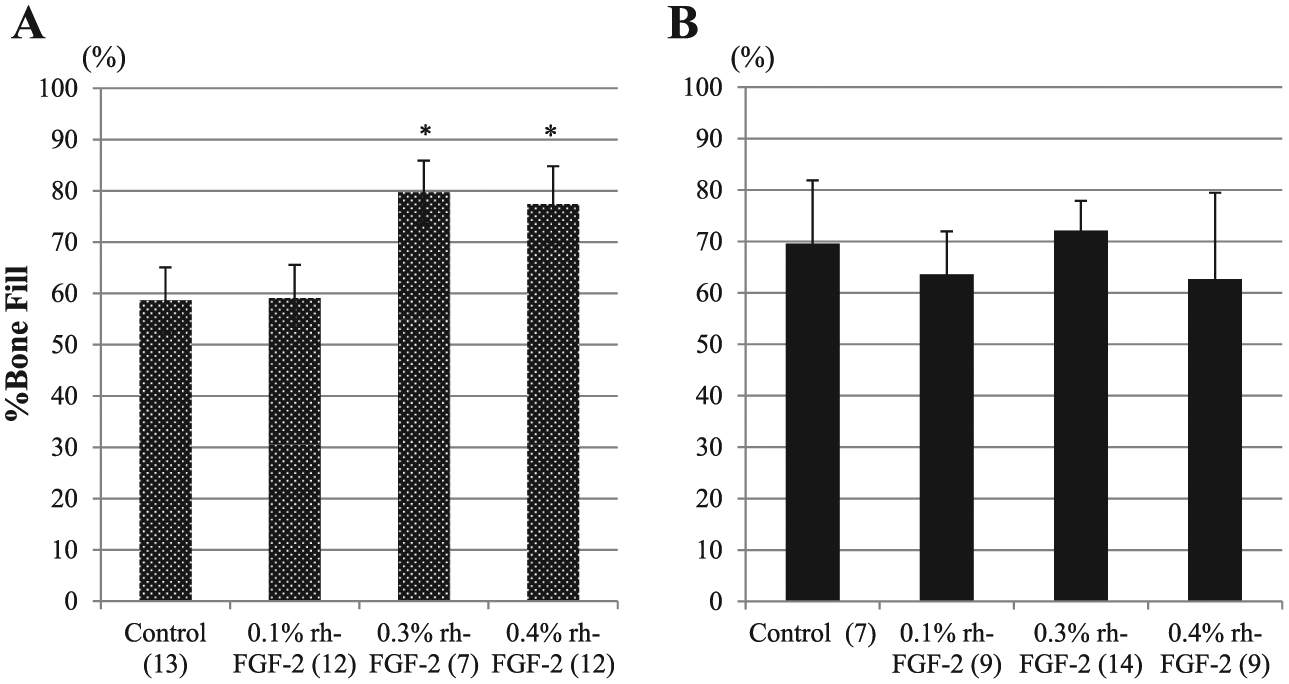
Percentage bone fill based on defect type. Values are shown as the mean ± SE. (
Discussion
This prospective randomized controlled multicenter clinical study was double-blinded with dose verification and external monitoring in patients who required surgical intervention to treat a qualifying periodontal defect with a bone graft substitute and a biological protein. Many bone graft substitutes have been used to treat such defects (Sculean et al. 2015), but few have been examined under the strict clinical trial conditions as performed in this clinical study. A similar clinical study supports the use of a U.S. Food and Drug Administration–approved recombinant platelet-derived growth factor and β-TCP (Nevins et al. 2005; Nevins et al. 2013). In addition, a group of enamel matrix proteins isolated from the crowns of developing teeth, either alone or combined with various bone graft materials (Koop et. 2012), has been approved by the same body. The results of this rigorous randomized controlled clinical trial indicate that the rh-FGF-2 combined with β-TCP behaves in a similar fashion. This conclusion is supported by multiple randomized controlled clinical trials in Japan where this same biological factor, combined with a HPC solution (without bone grafting), also significantly stimulates LBG compared with the vehicle control or enamel matrix proteins (Kitamura et al. 2008; Kitamura et al. 2011; Kitamura et al. 2015).
The rh-FGF-2 is a biological stimulant that has been reported to promote proliferation and migration of certain kinds of cells, including osteoblasts, endothelial cells, and periodontal ligament cells. It is a unique molecule in that it prohibits the proliferation of epithelial cells; thus, its cellular effects suggest that rh-FGF-2 would make an effective periodontal regeneration agent. Furthermore, rh-FGF-2 is well known as a potent angiogenic factor to generate new blood vessels, which are important for enhancing the wound-healing process and supporting new tissue formation.
Histologic animal studies were conducted with FGF-2 to evaluate periodontal regeneration, since histologic proof is required to claim periodontal regeneration (Murakami et al. 1999; Takayama et al. 2001; Murakami et al. 2003; Anzai et al. 2010; Shirakata et al. 2010; Nagayasu-Tanaka et al. 2015). In a 1-wall defect study based on a dog model, significant new cementum formation occurred as compared with the active control (β-TCP alone) and the sham group (nongrafted sites; Anzai et al. 2010). In 2001, rh-FGF-2 was approved in Japan as the active agent in a drug for dermal ulcers. In addition, 2 phase II and a phase III clinical trials for periodontal regeneration with rh-FGF-2 in a gel formulation were conducted where 0.3% rh-FGF-2 gel was most effective in stimulating periodontal clinical regeneration (Kitamura et al. 2008; Kitamura et al. 2011; Kitamura et al. 2015). The current clinical trial utilized a solid synthetic bone graft material (β-TCP) that is known as an effective synthetic bone substitute intended to fill, augment, or reconstruct periodontal or bony defects, and it serves as a biocompatible scaffold for bone cells for osteoconduction and is absorbed and replaced over time (Reynolds et al. 2015).
This study used a composite primary outcome variable that combined a clinical outcome (CAL) and a radiographic outcome (LBG) to measure the effectiveness of the product (Lynch et al. 2006). The combining of outcome measures for hard and soft tissue components of the periodontium was preferable to evaluate the effectiveness of a biological factor that has effects on both types of tissue. Similar to a previous trial with β-TCP as the protein carrier (Nevins et al. 2005; Nevins et al. 2013), the results here demonstrated that β-TCP as an active control in the periodontal defects had a good response in the lesions. Thus, a more stringent value was needed to discriminate a difference in the patient outcomes. Under these conditions, it was clear that adding the rh-FGF-2 had a clear and a significant effect on enhancing the amount of clinical periodontal regeneration achieved. Various bone graft materials have been used in the past, and the results have often been variable. This is likely due to the fact that in those cases, the bone graft material predominantly served as a space filler in a large bony void and provided a solid matrix for osteogenic cells to elaborate osteoid and new bone formation. Although β-TCP used in this study achieved a high-percentage bone fill (62.5%) without rh-FGF-2, the addition of 0.3% rh-FGF-2 increased bone fill >10%. The percentage bone fill at 6 mo in the active control was 3.5 times greater than that of the β-TCP treatment group in the previous trial (62.5% vs. 18%; Nevins et al. 2005). The difference between the 2 studies could be explained by the lower distribution of 1-wall defects in the present study than the previous study (9.1% vs. 32.2%). When a biologic factor such as rh-FGF-2 is added, cell behavior is directly affected, resulting in enhanced cell migration, proliferation, and differentiation. In addition, because FGF-2 is a potent stimulant of new blood vessel growth, new periodontal tissue formation is enhanced. No new cementum, periodontal ligament, or bone tissue can form without blood supply; thus, FGF-2 is a logical choice for enhancing periodontal regeneration. The effect of this molecule was particularly observed in this trial in the wound-healing scores where inflammation was enhanced at 2 wk—when it should be with an angiogenic factor such as rh-FGF-2—in the growth factor–treated lesions as compared with control. This study also confirmed the safety of this product.
In summary, the 0.3% and 0.4% rh-FGF-2 investigational devices increased the success rate of subjects based on the primary composite end point in the change of CAL and LBG. Furthermore, the 0.3% and 0.4% rh-FGF-2 treatment improved LBG by approximately 1 mm as compared with the control treatment when 2 outliers were excluded from the analysis. This additional 1 mm of LBG is clinically meaningful when considering that it increases the alveolar bone supporting the study tooth by 30% more than the control group.
Gingival recession following periodontal surgery was negligible in the 0.4% rh-FGF-2 group versus the control group. Gingival recession can not only be an aesthetic problem following periodontal flap surgery but also be associated with increased root sensitivity. In addition, the subgroup analysis of percentage bone fill in 1- and 2-wall defects indicated that the addition of rh-FGF-2 to β-TCP contributes to additional bone fill in these defects where healing is typically less predictable. Therefore, an additional benefit of the investigational device may be to increase the predictability of the treatment success in less predictable defects.
In conclusion, enhanced clinical periodontal regeneration was achieved in this randomized controlled double-blinded multicenter clinical trial using a defined protocol for the evaluation of rh-FGF-2 combined with a β-TCP scaffold matrix. The use of rh-FGF-2 combined with a scaffold matrix offers potential as a treatment option for a variety of periodontal osseous defects. Further investigations may also consider the ability of rh-FGF-2 to promote periodontal wound repair through different delivery approaches.
Author Contributions
D.L. Cochran, contributed to conception, design, and data interpretation, drafted and critically revised the manuscript; T.-J. Oh, M.P. Mills, D.S. Clem, P.K. McClain, R.A. Schallhorn, M.K. McGuire, E.T. Scheyer, W.V. Giannobile, M.S. Reddy, R.V. Abou-Arraj, P.J. Vassilopoulos, contributed to data acquisition, critically revised the manuscript; R.J. Genco, contributed to conception and data interpretation, critically revised the manuscript; N.C. Geurs, contributed to design, data acquisition, and analysis, critically revised the manuscript; A. Takemura, contributed to conception, design, data analysis, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
This study was supported by Sunstar Americas, Inc. The authors greatly thank Marie A. Wilson from Sunstar Americas, Inc. for supporting the project. W.V.G. and R.J.G. currently serve on the Science Advisory Board of Sunstar, although the board was not involved in the design of the present investigation. A.T. is an employee of Sunstar Americas, Inc.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.