
Abstract
Although bone morphogenetic protein 2 (BMP-2) is known to stimulate osteogenesis, there is evidence that high doses of BMP-2 can lead to side effects, including inflammation and carcinogenesis. The supplementation of other bone-augmenting agents is considered helpful in preventing such side effects by reducing the amount of BMP-2 required to obtain a sufficient amount of bone. We recently showed that a receptor activator of nuclear factor κB ligand (RANKL)–binding peptide promotes osteoblast differentiation. In the present study, we aimed to investigate whether OP3-4, a RANKL-binding peptide, promotes BMP-2–induced bone formation in the murine maxilla using an injectable gelatin hydrogel (GH) carrier. A GH carrier containing OP3-4 with BMP-2 was subperiosteally injected into the murine maxillary right diastema between the incisor and the first molar. The mice were sacrificed 28 d after the injections. The local bone formation in the OP3-4-BMP-2–injected group was analyzed in comparison to the carrier-injected, BMP-2–injected, and control-peptide-BMP-2–injected groups. The GH carrier containing OP3-4 with BMP-2 enlarged the radio-opaque area and increased the bone mineral content and density in the radiological analyses in comparison to the other experimental groups. Interestingly, fluorescence-based histological analyses revealed that the mineralization had started from the outside, then proceeded inward, suggesting that the size of the newly formed bone had already been set before calcification started and that the effects of OP3-4 might be involved in accelerating the early steps of osteogenesis. Actually, OP3-4 enhanced the BMP-2–induced 5-bromo-2′-deoxyuridine (BrdU)–positive cell numbers at the injected site on day 7 and the expression of Runx2 and Col1a1, which are early osteogenic cell markers, on day 10 after the subperiosteal injections. In summary, we demonstrated, for the first time, that the application of OP3-4 by subperiosteal injection promoted BMP-2–induced bone formation, which could lead to the development of an easy and noninvasive means of promoting alveolar ridge formation.
Introduction
Alveolar bone loss may lead to tooth loss, and the resulting loss of alveolar ridge dimensions may make prosthetic rehabilitation challenging (Von Arx et al. 1996). Moreover, malformations, such as cleft lips and palates, cause functional and aesthetic problems (Vargervik 1981; Mossey et al. 2009). Alveolar bone augmentation is therefore expected to be useful in various dental situations.
Although recombinant human bone morphogenetic protein 2 (BMP-2) is a well-known stimulator of osteogenesis (Carreira et al. 2014), several studies have revealed that high doses of BMP-2 can lead to inflammation (Woo et al. 2013) and carcinogenesis (Feeley et al. 2006); the side effects by BMP-2 were considered dose dependent (Carragee et al. 2013; Neovius et al. 2013). To reduce the amount of BMP-2 used to induce bone formation, it may be necessary to supplement BMP-2 with other bone-augmenting drugs.
Several studies have proposed fibroblast growth factor (FGF)–2 (Nakamura et al. 2005), FGF-4 (Kubota et al. 2002), transforming growth factor (TGF)–β1 (Tachi et al. 2011), and peptide drugs (Khan et al. 2013) as candidates for enhancing BMP-2–induced osteogenesis. Among these agents, peptide drugs have many advantages because of their properties, which include a low production cost, a low incidence of antigen-antibody reactions, and a structure that can easily be changed to fit a drug target (Aoki et al. 2012).
A receptor activator of NF-κB ligand (RANKL) binding peptide WP9QY not only inhibits bone resorption but also accelerates the bone formation that is induced by BMP-2 both in vitro and in vivo (Furuya et al. 2013; Khan et al. 2013; Mamun et al. 2013). WP9QY binds to RANKL on osteoblasts and enhances BMP-2 signaling and osteogenic gene expression, resulting in osteoblast differentiation (Furuya et al. 2013). We recently developed another RANKL binding peptide, OP3-4 (YCEIEFCYLIR), which was designed to mimic soluble osteoprotegerin (OPG) (Cheng et al. 2004; Heath et al. 2007). OP3-4 promotes osteoblast differentiation in vitro and inhibits bone resorption (Kato et al. 2015).
Furthermore, the need for surgical implantation can be circumvented if an injectable biomaterial can be designed for bone regeneration application (Kent et al. 1982, 1983; Block and Degen 2004; Mankani et al. 2006; Hasson 2007; Kfir et al. 2007; Mazzocco et al. 2008; Tamimi et al. 2009; Nevins et al. 2009). It will therefore be valuable if bone augmentation can be induced by an injection procedure in an easy and minimally invasive manner without soft tissue exposure. Although local bone regeneration has previously been achieved via a single injection in vivo (Seo et al. 2015), we are still a long way from being able to induce sufficient bone formation in the alveolar region.
In the present study, to develop a method for inducing osteogenesis by injection, an injectable gelatin hydrogel (GH) was used as a carrier. As a result, we found that a single injection of OP3-4 into the murine maxilla could accelerate BMP-2–induced bone formation on the alveolar ridge at the site of injection.
Materials and Methods
Animals
Twenty-four 8-wk-old male C57BL/6 mice were obtained from Nippon CLEA (Tokyo, Japan) and maintained in our animal care facilities, as described elsewhere (Nagano et al. 2011). The experimental procedures were reviewed and approved by the Animal Care and Use Committee of Tokyo Medical and Dental University (Tokyo, Japan; authorization numbers: 0140070C, 0150203C2, 0160182A). All sections of this report adhere to the ARRIVE (Animal Research: Reporting of In Vivo Experiments) Guidelines.
Experimental Design
The mice were anesthetized before surgery with subcutaneous injections of medetomidine hydrochloride (0.5 mg/kg, Domitor; Zenoaq, Fukushima, Japan) and ketamine hydrochloride (50 mg/kg, Ketalar; Sankyo, Tokyo, Japan) as previously described (Kato et al. 2015). Twenty-four mice were divided into 4 groups (n = 6) randomly depending on the materials that were incorporated in the GH carrier: 1) vehicle, 2) BMP-2, 3) BMP-2 + OP3-4, and 4) BMP-2 + control peptide. The materials were subperiosteally injected into the maxillary right diastema between the incisor and the first molar using a 24-gauge, 15° tip Hamilton needle attached to a 25-µL Hamilton syringe (Fig. 1A). The preparation of the injected materials, including OP3-4 and the control peptide syntheses, is described in the Appendix. At 12 and 26 d after the injection, the mice were subcutaneously injected with calcein (20 mg/kg; Sigma-Aldrich, St. Louis, MO, USA) and demeclocycline (25 mg/kg; Sigma-Aldrich), respectively (Fig. 1B). The mice were sacrificed under anesthesia by cervical dislocation at 28 d after the subperiosteal injections (Fig. 1B). The cranial bones of the mice were then dissected and fixed in phosphate buffered saline (PBS)–based formaldehyde (10%) fixative (pH 7.4) for 2 d at 4°C, washed with PBS for 1 d, and then used for radiological and histological analyses.
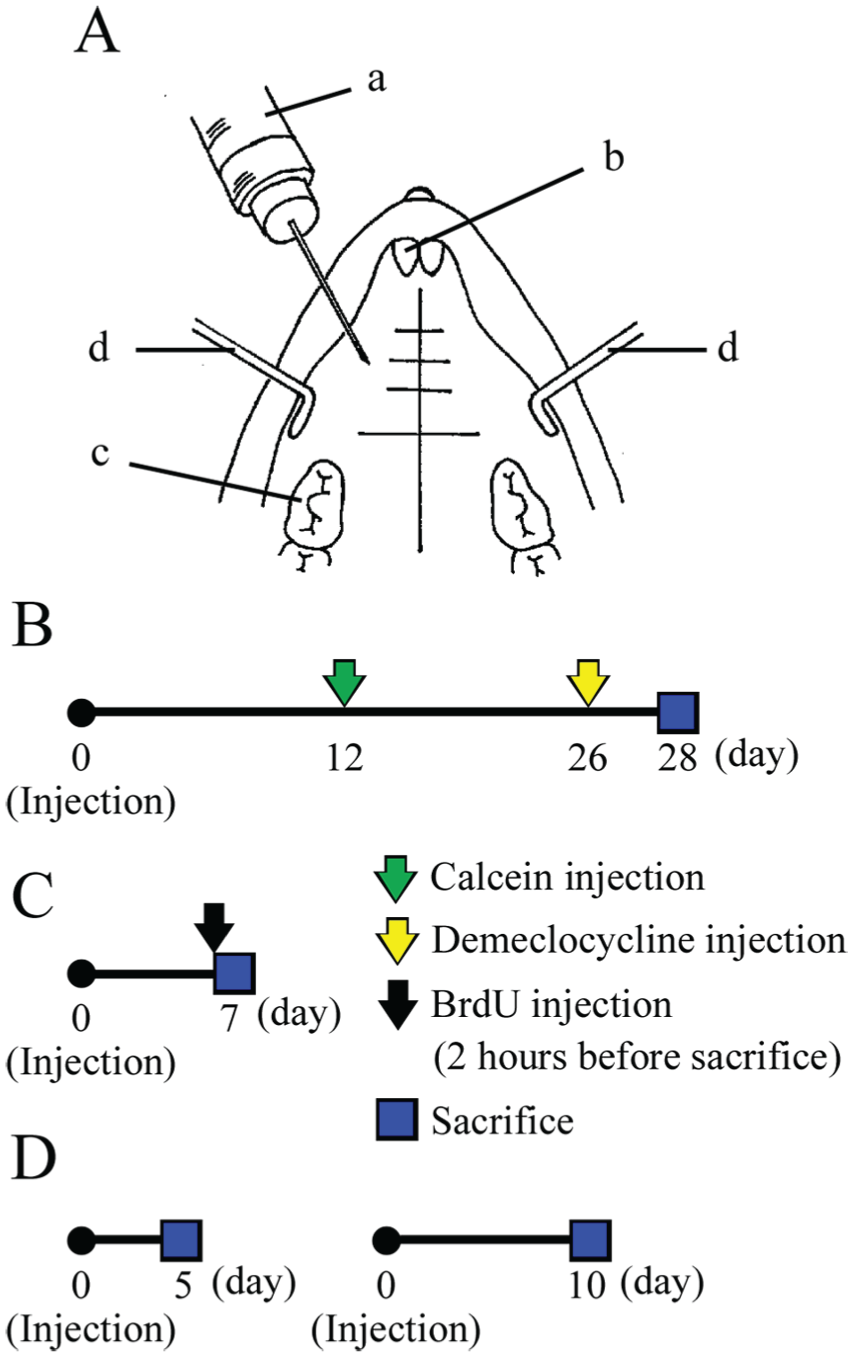
Experimental designs. (
Radiographic Assessments
Three-dimensional reconstruction images of the newly formed bones were obtained by micro-focal computed tomography (µCT) (Scan Xmate-E090; Comscan, Yokohama, Japan). The Tri/3D-View software program (RATOC System Engineering, Tokyo, Japan) was used to generate a 3-dimensional reconstruction from the obtained set of scans. The bone mineral content (BMC) and the bone mineral density (BMD) of the newly formed bones were measured by peripheral quantitative computed tomography (pQCT) (XCT Research SA+; Stratec Medizintechnik GmbH, Pforzheim, Germany). The data obtained from pQCT were further calculated to obtain the average value of 7 slices, with 6 symmetrical slices centering on the injected site with a 0.25-mm interval. To measure the total BMC and BMD, the region of interest (ROI) in the cross section, which covered the whole area of newly formed bone, was determined. In the ROI, the calcified tissue in which the BMD was from 267 to 690 mg/cm3 was defined as the newly formed bone area. The BMC and BMD were calculated as previously described (Kimura et al. 2014).
Histological Assessments and Bone Histomorphometry
The cranial samples were embedded in SCEM compound (Section-Lab, Hiroshima, Japan) and frozen at −100°C using a freezing system (UT2000F; Leica Microsystems, Tokyo, Japan). The undecalcified frozen sections (3 µm in thickness) were made with a microtome (CM3050sIV; Leica Biosystems, Nussloch, Germany) with the help of adhesive Kawamoto films (Cryofilm type 2C [9], Section-Lab) according to a previously described method (Kawamoto 2003). The sections were stained according to the von Kossa method and counterstained with the modified van Gieson method to detect calcified tissue. Fluorescence-labeled images were used to analyze the area of calcification in the newly formed bones. The ROI for the fluorescence labeling analyses in the newly formed protrusion was determined based on the calcein labeling at the injected site, which made a border between the newly formed bone and the original bone. A bone histomorphometric analysis was performed using an image analyzing system (KS 400; Carl Zeiss, Jena, Germany).
Cellular Proliferation and Messenger RNA Analysis in Early Stage of Bone Formation
To detect cellular proliferation in the early stage of bone formation, the mice were injected with the GH carrier containing vehicle alone or with the BMP-2–containing GH carrier either with or without the above-described peptides. 5-bromo-2′-deoxyuridine (BrdU) labeling reagent (50 µg/g body weight; Takara, Kusatsu, Japan) was injected intraperitoneally 2 h before euthanasia at 7 d after the injection (Fig. 1C). The undecalcified frozen sections were made as described above. The sections were stained with a BrdU detection kit (Takara) and alkaline phosphatase (ALP) to detect osteogenic cells. Some sections were stained by toluidine blue.
The mice were injected with GH carrier containing BMP-2, with or without the peptides, into the maxilla of both the right and left diastemas for a messenger RNA (mRNA) analysis. The mice were sacrificed at 5 and 10 d after the injections (Fig. 1D), and the tissues around the injection site were dissected and frozen using liquid nitrogen. Total RNA was prepared by using TRIzol (Invitrogen, Grand Island, NY, USA) and treated with DNase I (Invitrogen). Complementary DNA (cDNA) was synthesized using Prime Script II reverse transcriptase (Takara) according to the manufacturer’s instructions. A quantitative reverse transcription polymerase chain reaction (qRT-PCR) was performed using SYBR Premix Ex Taq II (Takara) and a LightCycler 2.0 (Roche, Basel, Switzerland). For normalization, the expression of hypoxanthine guanine phosphoribosyl transferase (Hprt) was measured as an endogenous reference gene. Runx2 and Col1a1 were used as early osteoblast differentiation markers, and Sox9 was used as an early differentiation marker of chondrocytes. Col2a1 and Col10a1 were used as markers of mature chondrocytes. The primer sequences are described in the Appendix. The gene expression levels were calculated using the delta-delta Ct method.
Statistical Analysis
All of the data are presented as the means ± standard deviation (SD). Multiple intergroup comparisons were performed using a 1-way analysis of variance (ANOVA). When a significant F ratio was identified, the groups were compared using Fisher’s protected least significant difference (PLSD) post hoc test. P values of <0.05 were considered to indicate statistical significance.
Results
OP3-4 Accelerates BMP-2–Induced Bone Formation
OP3-4 with BMP-2 was injected subperiosteally into the murine maxilla. The body weight changes of the mice were similar in the experimental period. OP3-4 has been shown to accelerate BMP-2–induced bone formation, and no complications, such as inflammation and swelling, were observed in this study. The mice were sacrificed at 28 d after the injection, and the local bone formation was radiologically analyzed. Micro-CT images showed almost no radio-opaque area at the site injected with GH containing vehicle only (Fig. 2A, B). Although a small radio-opaque area was observed in the mice that were treated with GH containing BMP-2 (Fig. 2C, D), the largest radio-opaque area was observed (among 4 experimental groups) in the mice that were treated with GH containing BMP-2 and OP3-4 (Fig. 2E, F). The control peptide appeared to promote the BMP-2–induced radio-opaque area, although the area was smaller than that of the BMP-2/OP3-4 group (Fig. 2G, H). To clarify the mineral density of the newly formed bone, pQCT was used. The mice that were treated with GH containing BMP-2 and OP3-4 had a massive areas of newly formed bone defined by regions in which BMD was >464 mg/cm3 (Fig. 3C). The inside of the bone mass consisted of trabecular bone in which the BMD was <395 mg/cm3. In contrast, only trabecular bone was observed around the injection site in the mice that were treated with GH containing BMP-2 only or with the control peptide (Fig. 3B, D). Newly formed bone was not observed in the vehicle-only group (Fig. 3A). The BMC of the newly formed bone was significantly higher in the group treated with BMP-2 and OP3-4 than in the other experimental groups (Fig. 3E). In addition to showing the largest bone area on µCT reconstruction images, the BMD that was observed in the BMP-2– and OP3-4–treated mice was significantly higher than that in the other experimental groups, indicating that the bones that formed were more compact (Fig. 3F).
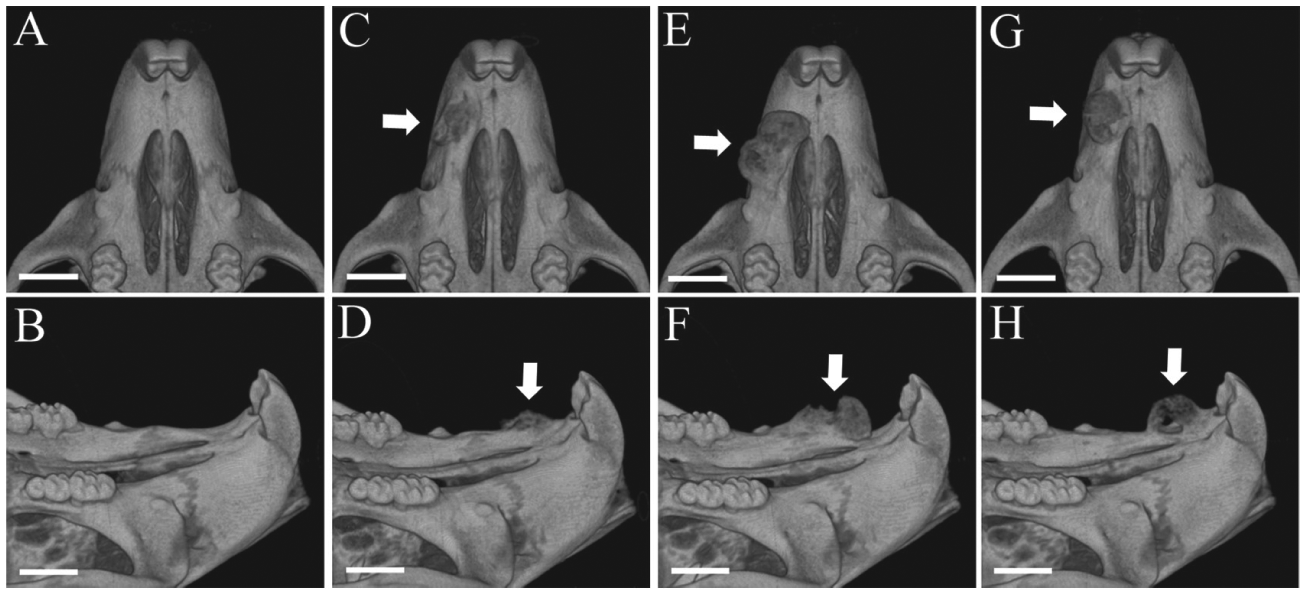
Representative 3-dimensional reconstruction images of the murine maxilla and the newly formed bone by micro–computed tomography (µCT) at day 28 after the injection. The materials incorporated in the gelatin hydrogel (GH) carrier were vehicle (
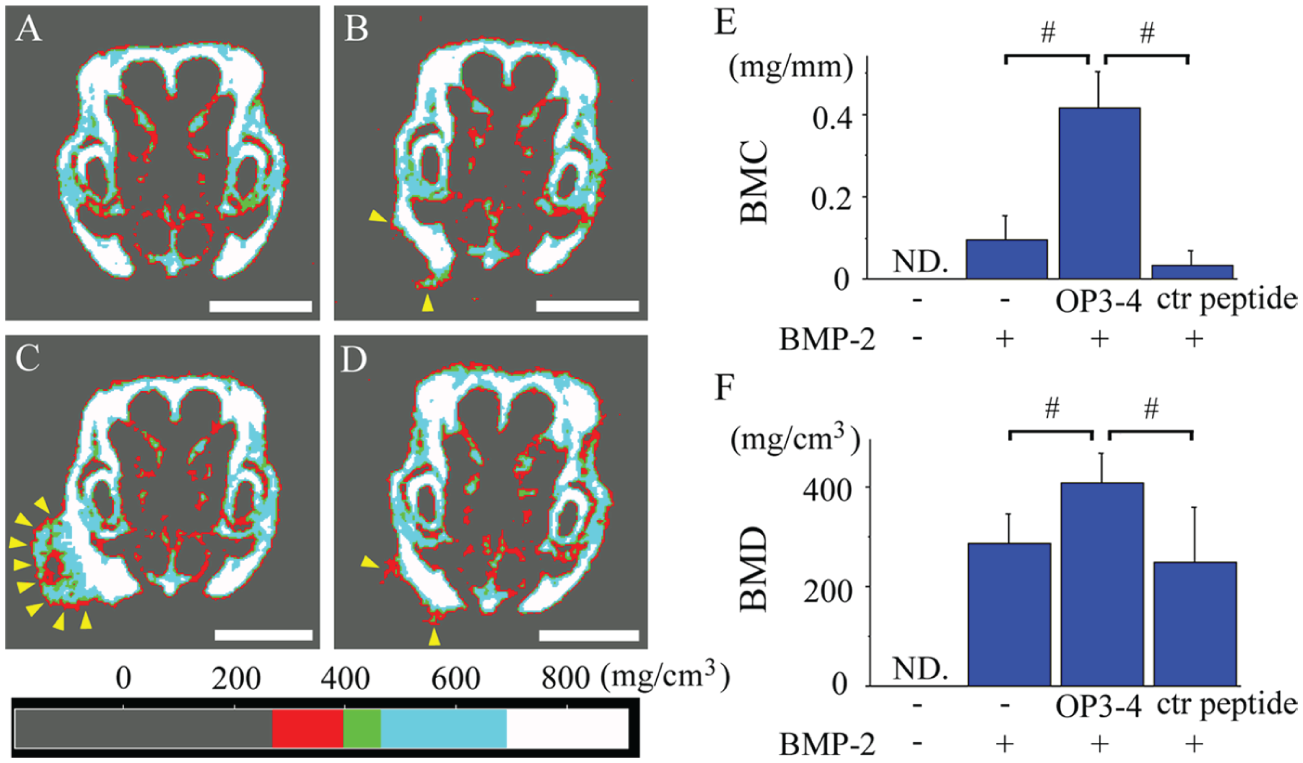
The quantitative computed tomography (pQCT) analysis data of the newly formed bones. (
OP3-4 Induces Mineralization All Over the Newly Formed Bone
Undecalcified frozen sections were prepared for the histological analysis of the newly formed bone as described in the Materials and Methods. Von Kossa staining revealed that mineralization occurred all over the protrusion in the mice that were treated with BMP-2 and OP3-4 (Fig. 4C), in contrast to the mice that were treated with BMP-2 only or with the control peptide, in which mineralization only occurred in the outer region (Fig. 4B, D). No apparent mineralization was induced by GH containing vehicle only (Fig. 4A). In the mice treated with BMP-2 and OP3-4, the outer surface of the protrusion was clearly labeled with calcein, which had been injected on day 12, while the inner area was labeled with demeclocycline, which had been injected on day 26 (Fig. 4G). In contrast, the mineralization was only detected in the outer areas in the mice that were treated with BMP-2 only or with the control peptide (Fig. 4F, H). No extra labeling on the periosteal surface at the site of injection was observed in the vehicle-only group (Fig. 4E). To compare bone formation activity at the injection site among experimental groups, we measured the demeclocycline-labeled areas. The demeclocycline-labeled area in the group treated with BMP-2 and OP3-4 was significantly larger than that in the other groups (Fig. 4I).
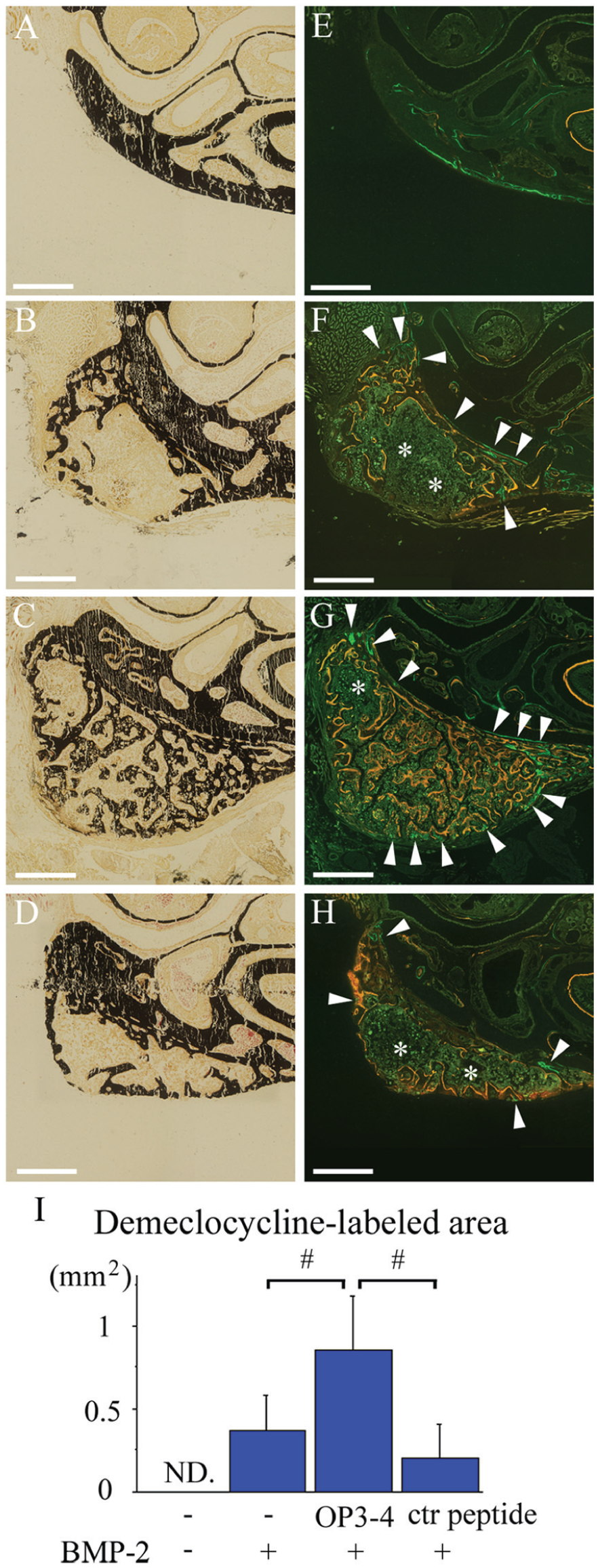
Histological images and bone histomorphometry of the newly formed bones. (
OP3-4 Enhances Proliferation and Osteogenic Gene Expression
To clarify the effects of OP3-4 in the early stage of the bone formation, we investigated cellular proliferation and osteogenic gene expression. BrdU-labeled proliferating cells were more abundant in the mice that were treated with GH containing BMP-2 and OP3-4 than in any other experimental group (Fig. 5A–E). A few cells were positively labeled in the GH carrier control group since the small protrusion at the injected site existed even in the carrier control group on day 7 (Fig. 5A). Although we could not detect mature chondrocytes in the histological section on day 7, a very small amount of immature cartilage-like tissue (which showed metachromasy in some toluidine blue–stained sections) appeared in a very small region at the injected site in the OP3-4-BMP-2–injected group.
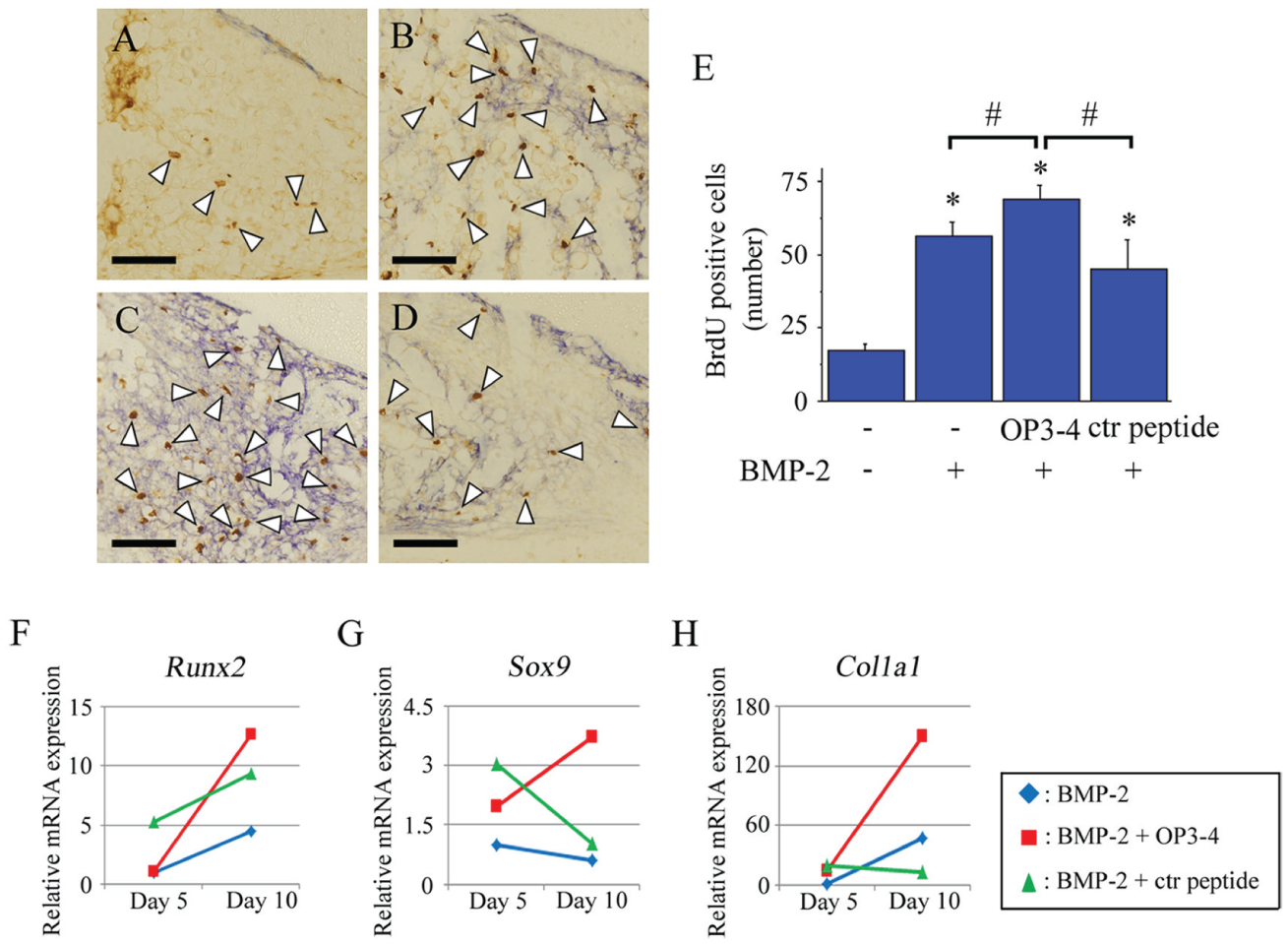
Cellular proliferation and the messenger RNA (mRNA) expression levels in the early stage of bone formation. (
Furthermore, a qRT-PCR was conducted to investigate whether OP3-4 with BMP-2 promoted bone and cartilage formation at the early stage of the bone formation since ectopic bone formation by BMP-2 in mice was considered to be induced by a combination of intramembranous and endochondral processes (Volek-Smith and Urist 1996; Stoeger et al. 2002). The qRT-PCR data on day 10 after the injection showed that the expression levels of Runx2, Sox9, and Col1a1 were remarkably increased in the group that was treated with GH containing BMP-2 and OP3-4 in comparison to the group that was treated with GH containing BMP-2 only (Fig. 5F–H). The data at day 5 showed the weak expression of Runx2, Sox9, and Col1a1. The expressions of Col2a1 and Col10a1, markers of mature chondrocytes, were nondetectable levels on day 5 or 10 (data not shown).
Discussion
In this study, we used GH as an injectable carrier for a peptide drug. A previous study revealed that a GH carrier could achieve the sustained release of another RANKL-binding peptide, WP9QY, over a 28-d period (Mamun et al. 2013). In this study, it seemed that the GH carrier was able to sustain the release of the peptide agent OP3-4 for a duration that was sufficient to induce osteogenesis. The GH carrier holds the agents through molecular interactions, such as hydrogen binding, hydrophobic binding, and Coulomb’s force, and may release the drugs due to increased ionic strength and/or through its biodegradation (Ikada and Tabata 1998). The GH carrier is already known to be a suitable carrier for the controlled release of BMP-2 (Yamamoto et al. 2003; Asamura et al. 2010). A large dose of peptide might act as a carrier of controlled BMP-2 release. This is, however, difficult to hypothesize since the same dose of the control peptide did not induce massive bone formation. Further studies are necessary to clarify the synergistic mechanism of BMP-2 and OP3-4. We herein showed, for the first time, that granular-type GH is appropriate as an injectable carrier for a peptide agent to promote BMP-2–induced bone formation.
Several lines of evidence have shown that various doses of BMP-2 are necessary to induce bone formation in human studies. One report showed that 100 µg/kg is sufficient to induce bone regeneration patients (Fourman et al. 2014), while another report showed that approximately 667 µg/kg BMP-2 is necessary to induce bone formation (Carragee et al. 2013). A former case has been reported to cause no adverse effects, but the latter case had severe complications. We used approximately 40 µg/kg BMP-2 in this study, and 40 µg/kg BMP-2 did not induce sufficient bone formation in the murine maxilla with no complications. The same dosage of BMP-2 was not reported to induce such complications in previous studies (Khan et al. 2013; Mamun et al. 2013). Further studies are necessary to clarify which factors, such as age of the recipient and the applied site, are related to the development of adverse effects.
The GH carrier incorporated with OP3-4 accelerated BMP-2–induced osteogenesis. The observations of calcein- and demeclocycline-labeled surfaces, especially in the OP3-4-BMP-2–injected group, revealed that mineralization inside the newly formed bone occurred after mineralization of the outer region since the demeclocycline-labeled area was primarily located inside the bone protrusion on the maxilla, and the calcein-labeled area was primarily observed outside of the bone protrusion (Fig. 4G). These observations suggest that the size of the bone protrusion at the injected site had already been set when the calcification began. This process is similar to the ectopic bone formation that occurs when another RANKL-binding peptide, WP9QY, is implanted in combination with BMP-2 (Khan et al. 2013). We postulated that the reason why the size of the bone protrusion was set before calcification could be explained by the acceleration of the proliferation of osteogenic cells by the RANKL-binding peptide. At the early stage of bone formation at the injected site, OP3-4 enhanced the cellular proliferation induced by BMP-2 (Fig. 5E). Recently, the mesenchymal stem cells that were observed as satellite cells, which are precursors of muscle cells, were shown to accelerate cellular proliferation through mTORC1 signaling (Rodgers et al. 2014). It is therefore possible for osteogenic cells to accelerate proliferation through mTORC1 signaling, since mesenchymal stem cells are the common source of both muscle cells and osteoblasts. Taken together, our data suggest that the RANKL-binding peptide OP3-4 accelerated cellular proliferation at the site of injection and increased the size of the BMP-2–induced bone tissue.
We also showed that OP3-4 promoted Runx2 and Col1a1 expression, which are genetic markers of bone formation (Fig. 5F, H). Although we observed the increased expression of Sox9, a master gene for chondrogenesis, in the groups treated with BMP-2 and OP3-4 (Fig. 5G), we could not detect the expression of either Col2a1 or Col10a1 or observe mature chondrocytes in the histological images. Thus, it is possible that cartilage is induced but does not undergo maturation. Although the mechanism underlying the promotion of bone formation by OP3-4 remains under investigation, it might be explained as RANKL-reverse signaling. Another RANKL-binding peptide, WP9QY, has been shown to stimulate osteoblast differentiation partially through a RANKL-dependent mechanism (Furuya et al. 2013). We hypothesize that the RANKL-binding peptide binds to the membrane-bound RANKL on osteoblasts and/or preosteoblasts and stimulates osteoblast differentiation through RANKL-intracellular signaling, which we have termed RANKL- reverse signaling. Furthermore, mTORC1 signaling has been shown to promote the activation of Runx2 (Singha et al. 2008). We have recently found that OP3-4 stimulated the phosphorylation of S6k1, an effector molecule of mTORC1 (Sugamori Y, Mise-Omata S, Maeda C, Aoki S, Tabata Y, Murali R, Yasuda H, Udagawa N, Suzuki H, Honma M, Aoki K, 2016, unpublished data). Our data therefore indicate that a RANKL-binding peptide could accelerate the early differentiation markers of osteoblasts, which might be involved in mTOR signaling.
In summary, we showed the first application of OP3-4 in the promotion of BMP-2–induced osteogenesis. In addition, we showed a valuable injection method, which is an easy and minimally invasive means of inducing a certain amount of bone production at the site of injection. The combination therapy of a RANKL-binding peptide, OP3-4, with BMP-2 might become a promising regimen for alveolar ridge augmentation since the peptide promoted the BMP-2–induced local bone formation. This could lead to the reduction of the severe side effects caused by the administration of large amounts of BMP-2. Furthermore, the single injection of a RANKL-binding peptide with BMP-2 might be an innovative method for augmenting the alveolar ridge.
Author Contributions
T. Uehara, S. Mise-Omata, K. Aoki, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M. Matsui, Y. Tabata, R. Murali, M. Miyashin contributed to design and data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
We are grateful to the participants and their families for their participation and contributions. We thank Dr. Masashi Honma and Dr. Hiroshi Suzuki (Department of Pharmacy, University of Tokyo Hospital, Faculty of Medicine, University of Tokyo, Tokyo, Japan) for their valuable discussions on RANKL reverse signaling.
This study was supported by grants-in-aid to K.A. from JSPS KAKENHI (25293377 and 23659867).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.