
Abstract
The aim of the study was to test whether implants of 6 mm in length perform equally well as 10-mm implants in terms of survival and marginal bone-level changes when supporting single crowns. Patients with a posterior single-tooth gap were randomly allocated to either the placement of a 6-mm (test) or 10-mm implant (control). The treatment protocol allowed for internal sinus lift but not for lateral bone augmentation. After a healing period of 10 wk, implants were loaded with screw-retained single crowns. Survival rates, number of pockets ≥5 mm, and bleeding-on-probing were assessed clinically. The change of marginal bone level and crown-to-implant ratios were analyzed by 2 examiners. Longitudinal intragroup analyses for marginal bone levels were performed applying the Wilcoxon signed rank test. Intergroup differences at baseline and at 3 y were compared using the Mann-Whitney U test. The effect of implant length and crown-to-implant ratio on changes of marginal bone level also was determined. Of 94 implants placed (47 test and 47 control), 78 implants (40 test and 38 control) were available for follow-up examination at 3 y of loading. One test implant was lost during the second year. Hence, implant survival was not significantly different between the 2 groups after 3 y (98% test; 100% control). We found no significant change in the crestal bone level from baseline to 3 y for test and control implants with −0.19 ± 0.62 mm and −0.33 ± 0.71 mm, respectively. The intergroup difference was not significant. Crown-to-implant ratios were not associated with a statistically significant difference in marginal bone loss. However, the number of sites with pockets ≥5 mm was significantly higher in the test group. Based on the 3-y assessment, the use of 6-mm implants can be considered a viable option when reconstructing posterior single tooth gaps (German Clinical Trials Registry: DRKS00006290).
Keywords
Introduction
Constant efforts are aiming at the reduction of the invasiveness of implant surgery. These have led to decreased patient morbidity, shorter surgical treatment time, and a minimized risk of damaging neighboring anatomical structures (Thoma et al. 2015). Thus, there is a trend favoring the use of shorter implants, especially in cases with limited vertical bone dimensions.
The use of short implants, however, may implicate the risk of increased load on the peri-implant bone, potentially resulting in enhanced loss of marginal bone or even in premature implant loss (Anitua et al. 2014; Rossi et al. 2015). However, whether a high crown-to-implant ratio may lead to a higher degree of occlusal load, resulting in a negative influence on successfully osseointegrated implants, is controversially discussed (Chang et al. 2013).
A considerable number of clinical studies assessed implant survival rates as well as marginal bone-level changes for short implants. Retrospective and prospective studies show survival rates of at least 92.2% after follow-up periods between 2 and 7 y (ten Bruggenkate et al. 1998; Renouard and Nisand 2005; Slotte et al. 2014). One of these clinical studies even reported on a success rate of 94.3% after an observation period between 1 and 6 y (ten Bruggenkate et al. 1998). However, in most of these studies, the short implants were splinted with either short or long implants. One retrospective clinical trial reporting on 970 implants restored with single crowns in the maxillary molar region with lengths of ≤9 mm showed a cumulative survival rate over 84 mo of 95.1% (Fugazzotto et al. 2004). There are also several studies reporting on short implants supporting removable dentures, thus limiting the validity of the outcome to that respective kind of loading.
There are only few data available for implants supporting unsplinted single crowns. However, the fact that short implants perform well when loaded with single crowns is based on data over short time periods only. Hence, there is a need for randomized controlled clinical trials comparing the outcomes of short and long implants supporting single crowns over long periods of time. Therefore, it was the aim of this randomized controlled clinical 2-center trial to assess survival and marginal bone loss of 6-mm and 10-mm implants supporting single crowns in the posterior jaws. The null hypothesis was that implants of both lengths would perform similarly with regard to survival and change in marginal bone level.
Materials and Methods
This study was designed as a randomized controlled 2-center clinical trial (Appendix Fig. 1). All procedures and materials were approved by the local ethics committee (StV Nr. 07/13). Eligible patients were informed in detail about the aim as well as possible risks and benefits of the study. Patients were free to refrain from study participation at any time point without disclosure of a reason. All patients signed an informed consent before they were included in the study.
To meet the inclusion criteria, patients had to present themselves with a single-tooth gap in the premolar or molar region of the upper or lower jaw and an existing antagonist (tooth or implant-borne reconstruction). The missing tooth had to be extracted at least 6 mo prior to implant placement. No periodontal probing depths (PPDs) exceeding 5 mm in the residual dentition were accepted. A minimum of 2 mm of keratinized mucosa had to be present at the prospective implant site. Regarding bone dimensions, a minimal vertical bone height of 10 mm in the lower jaw (alveolar crest to the mandibular canal) and 6 mm of bone height in the maxilla (alveolar crest to the sinus floor) was required. Internal sinus floor augmentation (modified Summer’s technique) but no lateral guided bone augmentation procedures were allowed when placing the implants. All patients had to be systemically healthy.
Exclusion criteria comprised general contraindications against surgical interventions and smoking of more than 19 cigarettes per day (Lang and Tonetti 2003). The need for a preceding lateral bone augmentation with radio-opaque filler materials, prior therapeutic radiation of the jaw, severe bruxism or clenching habits, and any mucosal disease except sporadic localized gingivitis were further exclusion criteria. Insufficient oral hygiene and inadequate compliance were additional reasons for exclusion.
Surgical Intervention
Implant placement was performed at 2 clinics at the University of Zurich by calibrated surgeons who were well trained with the implant system. The randomization of the patients to either the test (6-mm implant) or control group (10-mm implant) was determined using a computer-generated randomization list (www.random.org). After administration of a local anesthetic (Septanest 1:200,000; Septodont [Niederkassel, Germany] or Rudocaine forte [Streuli Pharma AG, Uznach, Switzerland]), sulcular incisions at the adjacent teeth and a midcrestal incision were performed, allowing to raise a full-thickness flap. At this stage, the randomization concealment was broken and the surgical site was prepared according to the manufacturer’s instructions (SLActive standard plus soft tissue level implants; Straumann AG, Basel, Switzerland). The minimum primary stability had to reach 20 Ncm. All implants were covered with a healing cap. Flaps were closed with nonresorbable sutures (Supramid [B.Braun Medical AG, Sempach, Switzerland] or GoreTex suture [Gore, Flagstaff, AZ, USA]), leaving the implants for transmucosal healing. Patients had to refrain from brushing at the surgical site and instead had to rinse with a 0.2% chlorhexidine solution (Kantonsapotheke Zurich, Zurich, Switzerland) twice a day for 1 min until suture removal. Analgetics (Mefenacid 250/500-mg tablets; Kantonsapotheke Zurich, Zurich, Switzerland) were provided for optional intake during the first postoperative days. After a healing period of 6 to 10 d, sutures were removed. Three weeks later, oral hygiene was monitored, instructions for site-specific hygiene were repeated, and supragingival tooth cleansing was performed. Eight weeks after implant placement, impressions were taken using a standardized tray and a polyether impression material (Permadyne; 3M ESPE, Rüschlikon, Switzerland). The impression of the opposite jaw was taken with alginate. No provisional restorations were inserted. Screw-retained porcelain fused to metal (PFM) crowns were incorporated with a torque of 35 Ncm. After insertion of the reconstruction, a clinical examination (baseline) was performed measuring peri-implant and periodontal probing pocket depths, presence or absence of plaque, and bleeding on probing at 6 sites per implant and the neighboring teeth. In addition, a standardized x-ray was taken with a parallel technique using an individualized x-ray tray (Fig. 1).
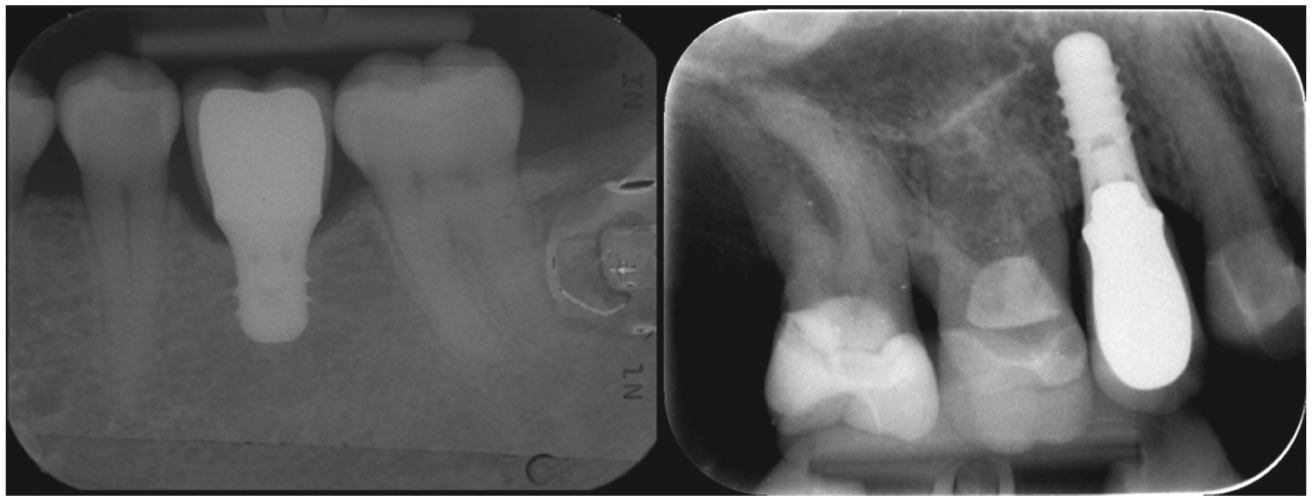
Radiographs of (left) test and (right) implant groups.
Follow-up
After 6 mo, oral hygiene was controlled and reinstructed if needed. Thereafter, patients were recalled at regular intervals between 6 and 12 mo for dental hygiene treatments according to their individual needs. At 1 y of loading and once every year thereafter, patients underwent a clinical examination of the study implant and the neighboring teeth. These appointments were conducted by 1 examiner per clinic and included measurements of peri-implant and periodontal probing pocket depths, presence or absence of plaque, and bleeding on probing at 6 sites per implant and at the adjacent teeth. At these follow-up appointments, technical failures such as chippings or loosening of abutment screws were recorded. In addition, intraoral photographs as well as an x-ray applying the parallel technique using the above-mentioned individualized tray were taken.
History of periodontitis was determined as general attachment loss exceeding 5 mm at more than 30% of the periodontal sites or tooth loss due to periodontitis.
Evaluation of Radiographs
Digitalized x-rays of all implants were magnified 10-fold and size-calibrated by their known length, width, and interthread distance. Mesial and distal bone levels as well as the crown lengths were determined. Distances of the mesial and distal bone levels were measured at a right angle from the implant neck to the first visible bone-to-implant contact (Fig. 2). These distances and the crown lengths were assessed using a shareware-measuring software (ImageJ, Image J64; National Institutes of Health, Bethesda, MD, USA). Clinical lengths of crowns and implants were calculated by adding the supra-osseous part of the implant (composed of 1.8 mm of machined implant neck and potential bone-level changes from the nominal bone level at the margin of rough and machined implant neck of the standard plus implant type) to the measured (technical) crown length and subtracting that distance from the length of the whole implant.
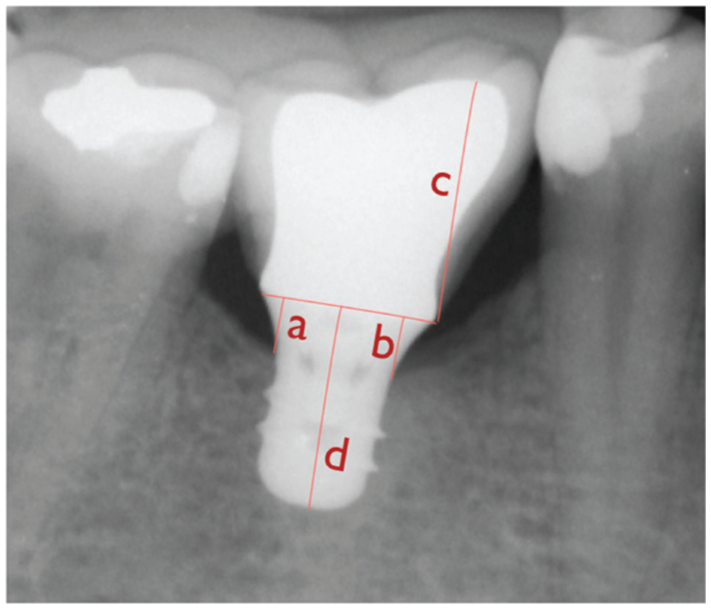
Distance measuring concept on the standardized radiographs.
When analyzing the bone-level changes by regression analysis, we adjusted for the baseline crown-to-implant ratio as one of the relevant confounders (Blanes 2009).
All measurements were performed by 2 independent examiners who had previously been calibrated. Statistical analyses were performed with the average values of both examiners’ measurements.
Statistics
To determine the minimal number of patients for the present study, a sample size calculation had previously been performed. To detect a potential difference in bone loss of 0.38 mm between the groups (Roccuzzo et al. 2010) with an assumed standard deviation of 0.5 mm for each group with a power of 80% at a level of significance of 5% after 10 y, a minimal sample size of 28 patients for each group was calculated. With regard to a planned follow-up period of 10 y, a minimum initial number of 45 participants per group was considered reasonable.
Descriptive statistics included medians and interquartile ranges or mean ± standard deviations (SDs) for the ordinal and continuous variables. Categorical variables are presented as counts of total. Statistical analyses included comparison within test and control group at baseline and at the 3-y follow-up. Data from the x-ray measurements by the 2 different examiners were examined for concordance. A multiple linear regression model was fitted to marginal bone-level change to assess the effect of implant length and crown-to-implant ratio, adjusted for the potential confounders of smoking, history of periodontitis, and bone level at baseline. P values below 5% were considered statistically significant. All analyses were performed with R (R_CoreTeam 2015).
Results
Initially, 96 patients could be included in the study. Two patients of the control group, however, did not receive the complete treatment according to the study (see Appendix Fig. 1), thus being excluded from further assessment. At 3 y of loading, 81 patients could be reassessed, while 13 patients did not show up for the appointments, skipped their recall due to personal reasons, or had moved abroad in the meantime. Of the remaining patients, 78 x-rays could be analyzed.
All patients were in good general health at the follow-up appointments. One implant from the test group got mobile during the second year of loading without any radiographically detectable marginal bone-level change and had to be removed. All implants from the control group were still in place at the 3-y follow-up. This resulted in an overall survival rate of 98% for test and 100% for control implants. This difference was not statistically significant. No implant displayed peri-implantitis in terms of pocket depths >5 mm in combination with suppuration and/or progressive marginal bone loss. The mean crown-to-implant ratio in the test group (1.48 ± 0.33) was significantly higher (P < 0.001) than in the control (0.86 ± 0.18).
Over 3 y, the marginal bone-level changed by −0.19 ± 0.62 mm (test) and −0.33 ± 0.71 mm (control). These values for the bone levels at baseline and at 3 y showed no statistically significant difference for each group. No significant intergroup difference was found at 3 y (Fig. 3). For the assessment of distances on the x-rays, an interexaminer correlation coefficient of 0.94% for differences <0.1 mm was calculated. A significantly higher number of implants with PPD of ≥5 mm was found in the test group (P = 0.023). These probing depths, however, had already been observed during the baseline examination and showed neither progression nor suppuration at any later time point (Table 1). Regression analysis of the changes of the marginal bone level at the 3-y follow-up showed a nonsignificant effect of implant length (estimated effect 0.38 for more bone loss for the long implants with P = 0.152) when adjusting for the set of potential confounders (smoking, history of periodontitis, bone level at baseline, crown-to-implant ratio; Table 2). With decreased initial bone level at baseline, regression analysis showed a distinct effect on future bone loss (see “Bone level at baseline” in Table 2). No chipping of the veneering ceramic occurred and loosening of the abutment screw happened in 3 cases.
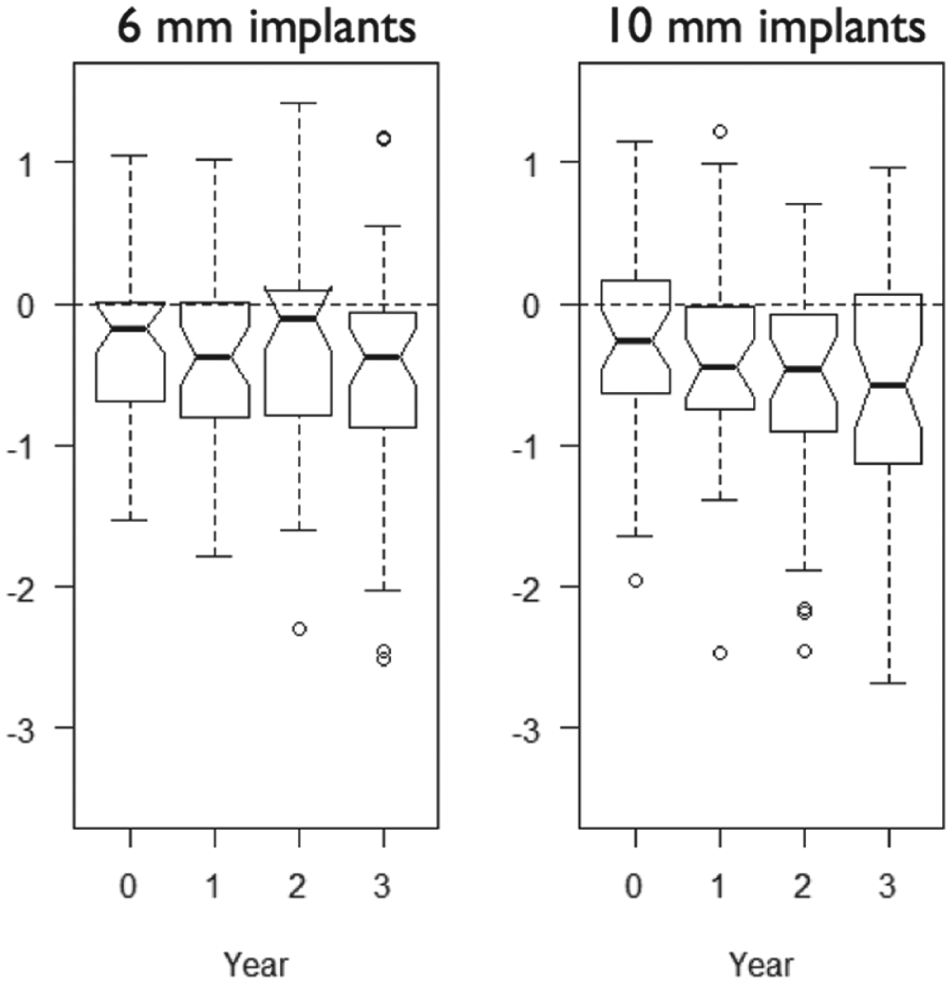
Change in marginal bone level from baseline to 3 y.
Baseline Patient Characteristics and Outcome Characteristics at the 3-y Follow-up.
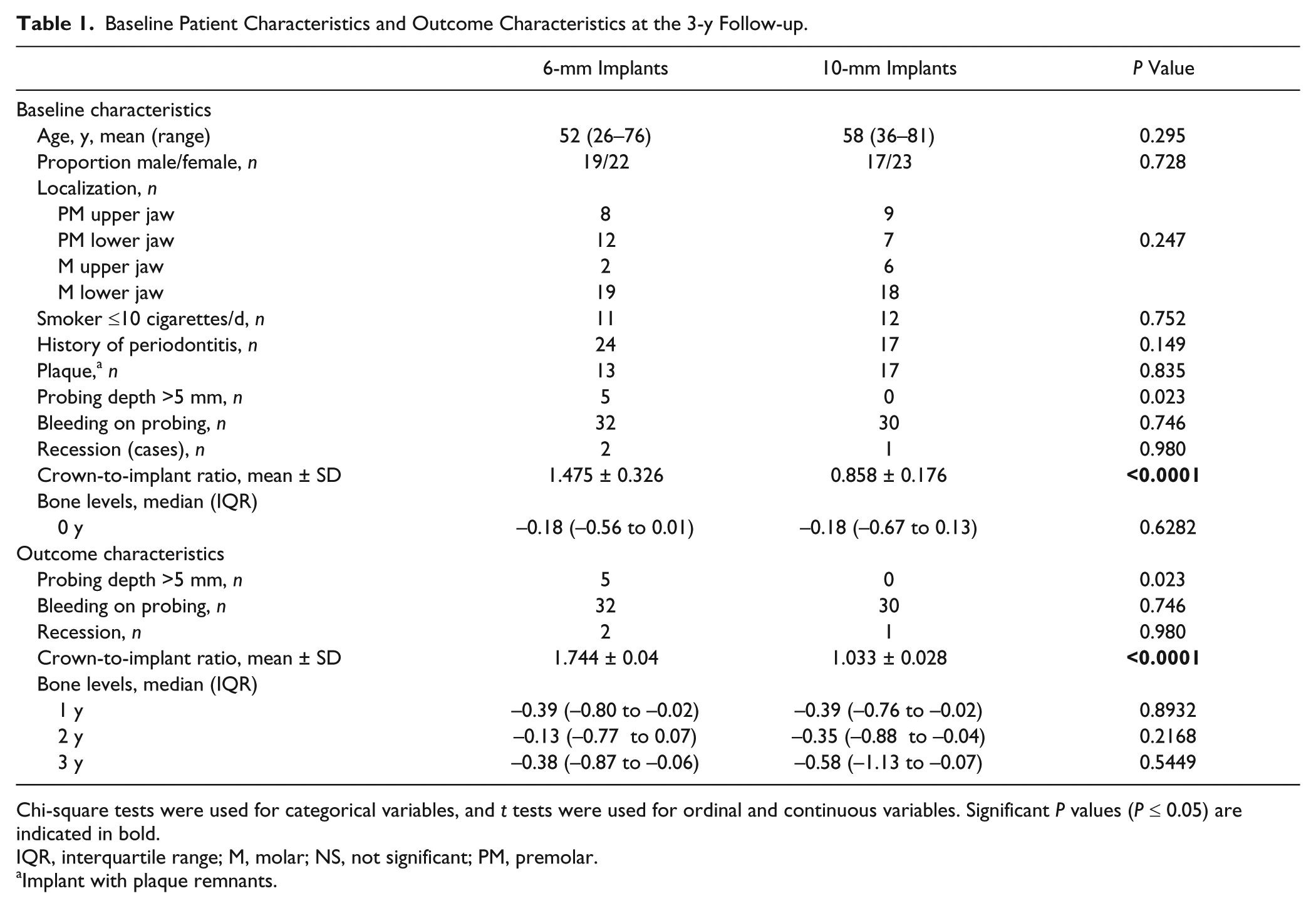
Chi-square tests were used for categorical variables, and t tests were used for ordinal and continuous variables. Significant P values (P ≤ 0.05) are indicated in bold.
IQR, interquartile range; M, molar; NS, not significant; PM, premolar.
Implant with plaque remnants.
Multiple Linear Regression Model Predicting Bone Loss.
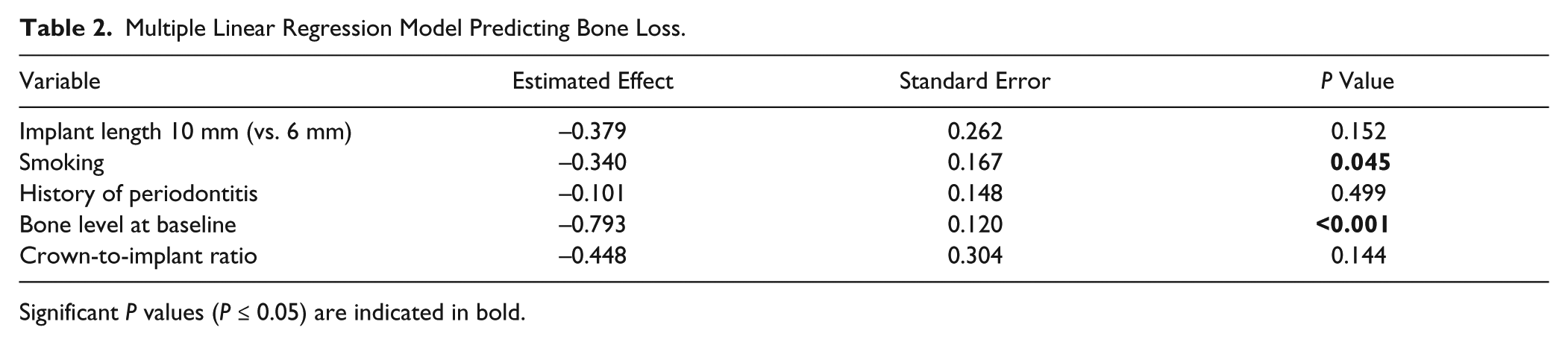
Significant P values (P ≤ 0.05) are indicated in bold.
Discussion
Based on the results of the 3-y follow-up data, the hypothesis that implants of both lengths perform equally regarding survival and marginal bone level change was not refuted, as no statistically significant differences with regard to survival and bone-level changes at 3 y of function were found.
The survival rates of 98% (test) and 100% (control) of this study are slightly above the reported survival rates of previously published clinical studies ranging from 86.7% to 95.1% (Fugazzotto et al. 2004; Rossi et al. 2015) at 5 and 7 y. A recently published 5-y prospective clinical study using an almost identical study design and implants of the same manufacturer with the same lengths reported slightly lower survival rates of 86.7% for 6-mm and 96.7% for 10-mm implants (Rossi et al. 2015). The marginal bone-level change in that study was in accordance with the results of the present investigation. However, there are some relevant differences with regard to implant surface (SLA instead of SLActive), loading protocol (insertion of crown after 7 instead of 8 wk), and supracrestal implant design (standard instead of standard plus). Likewise, the cohort in the above-mentioned study was slightly smaller, and there were fewer smokers included. Furthermore, the study reported neither the periodontal status of the included patients nor whether the patients had a history of periodontitis.
In the present study, the change of the marginal bone level ranged from 0.19 ± 0.62 mm (test) to 0.33 ± 0.71 mm (control) and did not show to be statistically significant. Similar results for marginal bone loss of 0.18 mm with similar standard deviations were reported in the previously mentioned study during the first 3 y of loading (Rossi et al. 2015). Hence, bone loss was below 0.2 mm for both groups and corroborates results from previously published data for the same type of implant (Filippi et al. 2013; van Velzen et al. 2014). Accordingly, the measured marginal bone-level change is within the range of previously stipulated implant success criteria (Albrektsson and Isidor 1994; Ganeles et al. 2008).
Peri-implant probing depths of ≥5mm in the test group demonstrated to be significantly higher in number compared with the control group. These probing depths, however, were already present at baseline and did not change during the observation period. As comparable information is missing from other clinical studies, it is difficult to estimate the importance of this finding.
Regarding short implants, there is still a controversial discussion about the influence of the crown-to-implant ratio on loss of marginal bone level. While some studies and an older review pointed out that there might be no association (Tawil et al. 2006; Blanes 2009; Schneider et al. 2012), more recent literature seems to indicate the opposite: Two review articles from 2014 addressed this issue and evaluated 7 retrospective and 6 prospective clinical studies and found a significant negative association between a crown-to-implant ratio of 0.6 to 2.36 and the marginal bone level (Monje et al. 2014; Garaicoa-Pazmino et al. 2014).
As a matter of course, the crown-to-implant ratio in the short implant group with 1.48 ± 0.32 was significantly higher than that of the control implants (0.86 ± 0.18). These values are very similar to those published in a similar study (0.54 for 10-mm and 0.96 for 6-mm implants) by Rossi et al. (2015). Maximal crown-to-implant ratios of up to 2.2 reflect the fact that in some individuals of the study population, the remaining alveolar bone height was significantly reduced prior to implant placement, presumably as a consequence of preceding periodontal destruction. Crown-to-implant ratio, however, turned out not to have an effect on implant survival or marginal bone-level change as calculated by the regression analysis.
Crown lengths have been measured from the implant shoulder to the most coronal extension of the metal base of the crowns. It is most likely that the crown lengths were therefore slightly underestimated, as we thereby ignored the thickness of the veneering ceramic. There are 2 reasons for this approach: the functionally relevant crown length is determined by the location of the occlusal contact point. However, the latter cannot exactly be determinable on the x-ray but is more likely to be located not on the tip or slopes of the cusps but close to the central fissure. Second, in some of our x-rays, the extent of the veneering ceramic was not exactly determinable due to a radio-opacity being very close to the silicone of the individualized x-ray splints. To rely on distances by clearly determinable end points, we have therefore chosen the most coronal extension of the crowns’ metal framework. Evident residual discrepancies were likely to be equaled out by applying the same method to both treatment groups.
The literature on implant success and survival suggests a negative association of survival and success when associated with a history of periodontitis (Heitz-Mayfield and Huynh-Ba 2009; Mombelli et al. 2012). No such relation could be found in the present study after 3 y. This might be due to the fact that the observation period is too short to detect peri-implantitis as the main biologic reason for implant failure (Roos-Jansaker et al. 2006; Jung et al. 2008; Jung et al. 2012).
The inclusion of smokers in the present study might be a limitation for the general validity of our findings, as an association of tobacco consumption and implant failure has previously been demonstrated (Strietzel et al. 2007; Heitz-Mayfield and Huynh-Ba 2009; Kasat and Ladda 2012). Although heavy smokers (>19 cigarettes/d) were excluded from study participation, 20% of the patients in this study population were moderate smokers. Nevertheless, due to an equal smoker ratio in both groups, the intergroup comparison remains valid.
The present study aimed to compare the clinical performance of implants of different lengths. In clinical situations where operators may be obliged to use short implants due to atrophic alveolar bone of limited height, short implants are most likely to be loaded with crowns of considerably greater lengths: to reach the occlusal plane, these crowns will have to compensate for the bone resorption. This may lead to an additionally enhanced crown-to-implant ratio and thus might not show results equally to those found in the present study.
In conclusion, this randomized controlled trial found no difference between test and control implants supporting single crowns in the posterior jaw at 3 y with regard to the primary outcome parameters of survival and change in the marginal bone level. Technical complication rate was low, measuring 3.8%, whereas no biological complications were observed.
Author Contributions
P. Sahrmann, contributed to conception and design, drafted the manuscript; N. Naenni, contributed to data acquisition, analysis, and interpretation, drafted the manuscript; R.E. Jung, T. Truninger, C.H.F. Hämmerle, T. Attin, contributed to conception and design, critically revised the manuscript; U. Held, contributed to conception, drafted the manuscript; P.R. Schmidlin, contributed to data acquisition, analysis, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
The clinical trial was supported by a grant by the International Team for Implantology, Basel, Switzerland (ITI Nr 517-2007).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.