
Abstract
The fundamental pathophysiologic response for the survival of all organisms is the process of wound healing. Inadequate or lack of healing constitutes the etiopathologic basis of many oral and systemic diseases. Among the numerous efforts to promote wound healing, biophotonics therapies have shown much promise. Advances in photonic technologies and a better understanding of light-tissue interactions, from parallel biophotonics fields such as in vivo optical imaging and optogenetics, are spearheading their popularity in biology and medicine. Use of high-dose lasers and light devices in dermatology, ophthalmology, oncology, and dentistry are now popular for specific clinical applications, such as surgery, skin rejuvenation, ocular and soft tissue recontouring, and antitumor and antimicrobial photodynamic therapy. However, a less well-known clinical application is the therapeutic use of low-dose biophotonics termed photobiomodulation (PBM) therapy, which is aimed at alleviating pain and inflammation, modulating immune responses, and promoting wound healing and tissue regeneration. Despite significant volumes of scientific literature from clinical and laboratory studies noting the phenomenological evidence for this innovative therapy, limited mechanistic insights have prevented rigorous and reproducible PBM clinical protocols. This article briefly reviews current evidence and focuses on gaps in knowledge to identify potential paths forward for clinical translation with PBM therapy with an emphasis on craniofacial wound healing. PBM offers a novel opportunity to examine fundamental nonvisual photobiological processes as well as develop innovative clinical therapies, thereby presenting an opportunity for a paradigm shift from conventional restorative/prosthetic approaches to regenerative modalities in clinical dentistry.
Introduction
Among all evolutionary traits in biology, the inherent ability of an organism to heal itself is an essential survival response. The anatomic and pathophysiologic functions of the craniofacial complex, specifically the oral cavity, perform rigorous tasks requiring intricate coordination of hard and soft tissues. Many forms of mechanical, chemical, and microbial insults necessitate the key processes of wound healing to maintain physical integrity and specialized functions. Given the key role of the craniofacial complex in overall human health, modalities to improve or promote stalled healing are gaining more attention, as led by rapid progress in stem cell biology and regenerative medicine. This review focuses on one such modality involving the use of biophotonics devices that increasingly have expansive applications in dentistry (Table 1).
Outline of Current Applications of Biophotonics Devices in Clinical Dentistry.
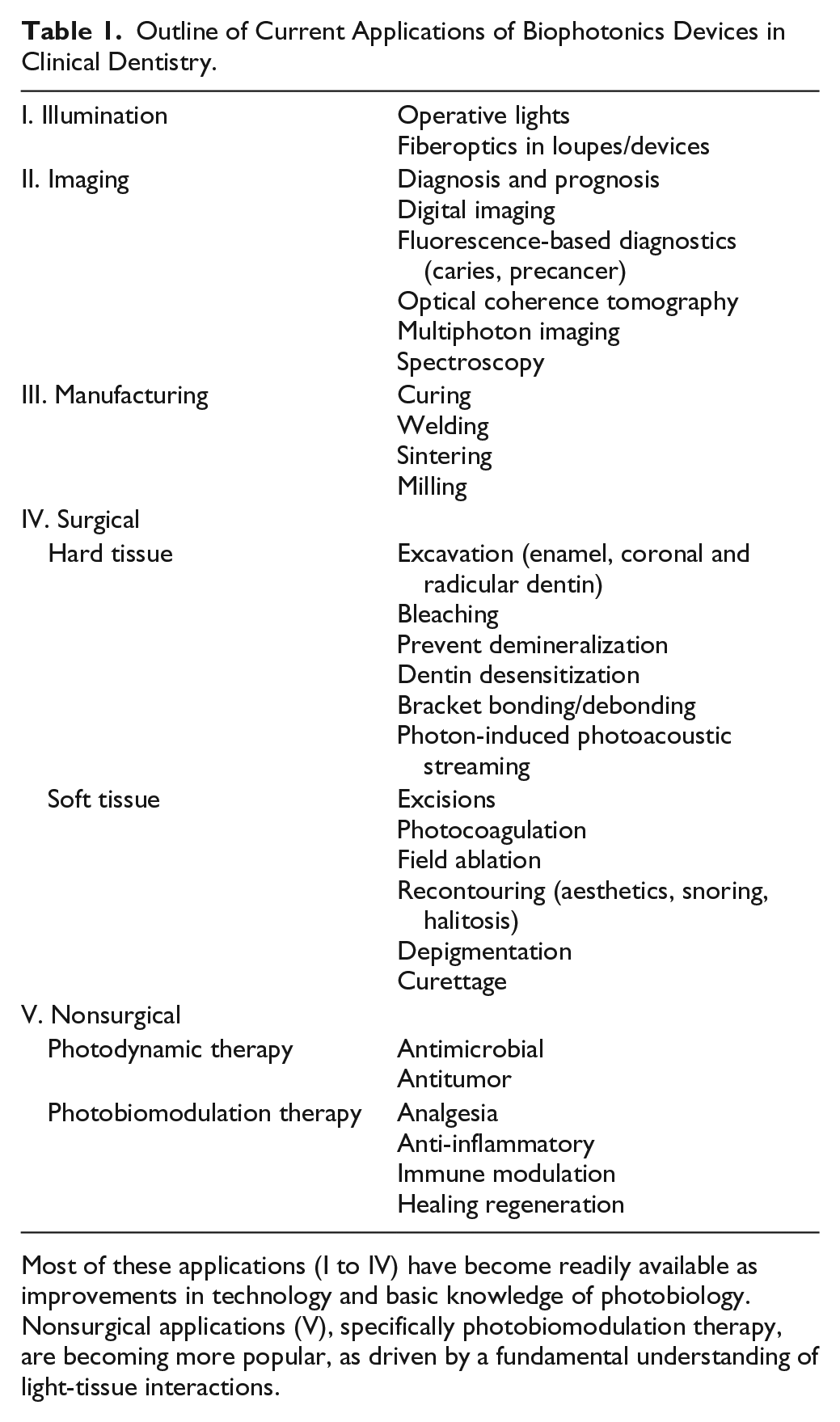
Most of these applications (I to IV) have become readily available as improvements in technology and basic knowledge of photobiology. Nonsurgical applications (V), specifically photobiomodulation therapy, are becoming more popular, as driven by a fundamental understanding of light-tissue interactions.
The use of light for therapy dates back to ancient scriptures from the Egyptians and Hindu civilization, where benefits of sunlight—termed helio, chroma, or simply phototherapy—are described in detail, although the fine line between ritualistic practices and medical treatments appears rather blurred. There were many subsequent descriptions through the ages, but in the late 19th century, Danish physician-scientist Niels Ryberg Finsen demonstrated the beneficial effects of the red and blue spectrum of sunlight to treat mycobacterial skin infection (Lupus vulgaris). His pioneering work was recognized with the 1903 Nobel Prize in medicine and physiology. Around the same time, Oscar Raab and Herman von Tappeiner in Germany noted that phototoxic effects on cells could be enhanced with exogenous dyes. This field of antimicrobial and, eventually, antitumor phototherapy is termed photodynamic therapy (PDT). The role of microbial pathogenesis of human infections was outlined by Leeuwenhoek, Jenner, Pasteur, and Koch. This promoted the discovery of pharmacologic agents with antimicrobial properties by Bertheim, Ehrlich, and Fleming, which dramatically changed the practice of modern medicine as we know it today. The resounding success of modern pharmacology-based medicine, however, appears to have moved attention away from light therapy.
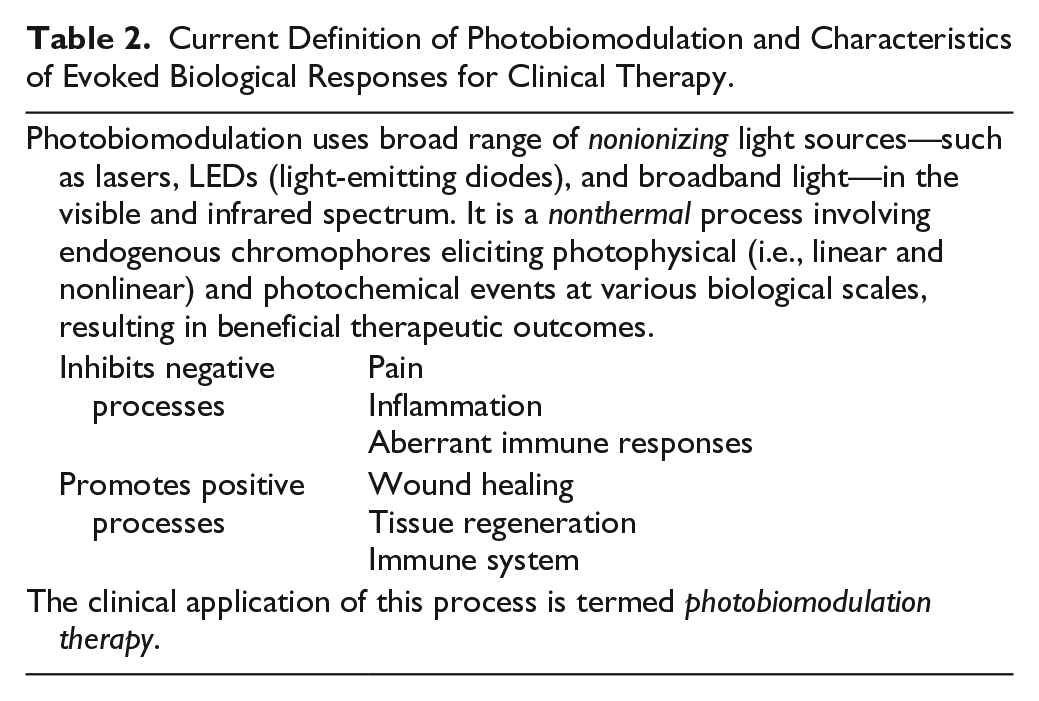
The invention of a new device—the light amplification by stimulated emission of radiation (laser)—brought renewed attention to this field. It was a seminal paper by Albert Einstein in 1917 that postulated the phenomenon of stimulated emission of photons, but it took another 4 decades for the first laser to be built by Theodore Maiman in 1960. It was immediately apparent that this new tool could serve as an excellent precision surgical tool. It was often mentioned, even in these early studies, that healing accompanying these laser surgical procedures appeared clinically improved when compared with similar surgical blade procedures. Laser-dose escalation animal studies soon followed that noted a startling phenomenon, first reported by Endrea Mester (Mester et al. 1973), that low-dose laser treatments appeared to stimulate wound healing, leading to the coining of the term photobiostimulation. Besides stimulating healing, further studies noted the ability of this therapy to inhibit certain deleterious processes, such as pain and inflammation. Many clinical and laboratory studies followed that led to a popular term: low-level laser therapy (Ohshiro 2014). The early laser devices were bulky, expensive, and technically complex, which severely limited their popularity. Development of compact diode lasers as well as light-emitting diodes (LEDs) rekindled enthusiasm in this field because of their low costs, small form factors, and ease of manufacturing and clinical use. Clinical and laboratory observations with LEDs and even broadband light demonstrating comparable effects as lasers led to the replacement of the term laser with a more generic light, resulting in the most popular MeSH term: low-level light/laser therapy. More recently, vagueness of the term level and subjective references to low (dose—energy or power) have led to adoption of the most appropriate MeSH term: photobiomodulation (PBM; Table 2; Anders et al. 2015). Acknowledgment of therapeutic potential of low-dose biophotonics over the past 5 decades has resulted in a plethora of scientific literature from basic research and clinical studies, including systematic reviews, meta-analyses, and blinded randomized controlled clinical trials. A detailed list of citations are included in the online Appendix. However, most of these studies appear to focus on phenomenological effects rather than causal mechanisms. A lack of thorough understanding of PBM mechanisms, along with an inaccurate and incomplete description of key treatment parameters in the literature, has resulted in ineffectual and inconsistent clinical outcomes. This has, unfortunately, relegated PBM therapy to complementary or alternate medicine.
Current Definition of Photobiomodulation and Characteristics of Evoked Biological Responses for Clinical Therapy.
To begin examining challenges in the field of PBM therapy, we can draw parallels from other fields that investigate biomolecular interactions with electromagnetic radiation. Some such examples of light-harvesting biosystems are chlorophylls and carotenoids in plant photosynthesis, antenna complex in photosynthetic bacteria, phycobilisomes in cyanobacteria and red algae, ultraviolet synthesis of cholecalciferol in skin, and rhodopsin-mediated phototransduction in the eye. The latter 2 examples deserve special attention, as they may offer direct insights into potential PBM mechanisms in humans. Photoconversion of 7-dehydrocholestrol (previtamin D3) by UV-B (295 nm) by sunlight involves electrocyclic chemical reactions resulting in isomerization and a hydride shift to generate cholecalciferol (vitamin D3), a key component of calcium homeostasis in the body. The vision-enabling molecule rhodopsin consists of 2 distinct components—the light-receptive chromophore retinal and the protein moiety scotopsin. The latter belongs to the G protein–coupled receptor group termed opsins. Light-induced isomerization of retinal results in concomitant changes in scotopsin conformation that, in turn, activates a secondary messenger molecule, cGMP (Heck et al. 2003). These 2 processes illustrate the ability of light to directly evoke photophysical and photobiochemical responses. Effects of light on circadian rhythm and psychosocial states are also well established. These distinct nonvisual phototransduction pathways are already being harnessed to affect human health, as in seasonal affective disorder, sleep and circadian disorders, and depression among others (Zeitzer et al. 2014; Harrison et al. 2015). Besides these direct examples of beneficial photobiological responses, interaction of electromagnetic radiation and biological molecules is a central focus of spectroscopy and ionizing radiation biology, where interrogation of structure or composition and detrimental cellular damage (oncotherapy) are distinct biological end points. The evidence from these fields indicates that therapeutic PBM mechanisms must also involve distinct light-tissue interactions. Given the biological complexity of molecules, cells, and tissues participating in wound healing, the following sections of this review focus on the major challenges for PBM therapy in craniofacial wound healing (Fig. 1A).
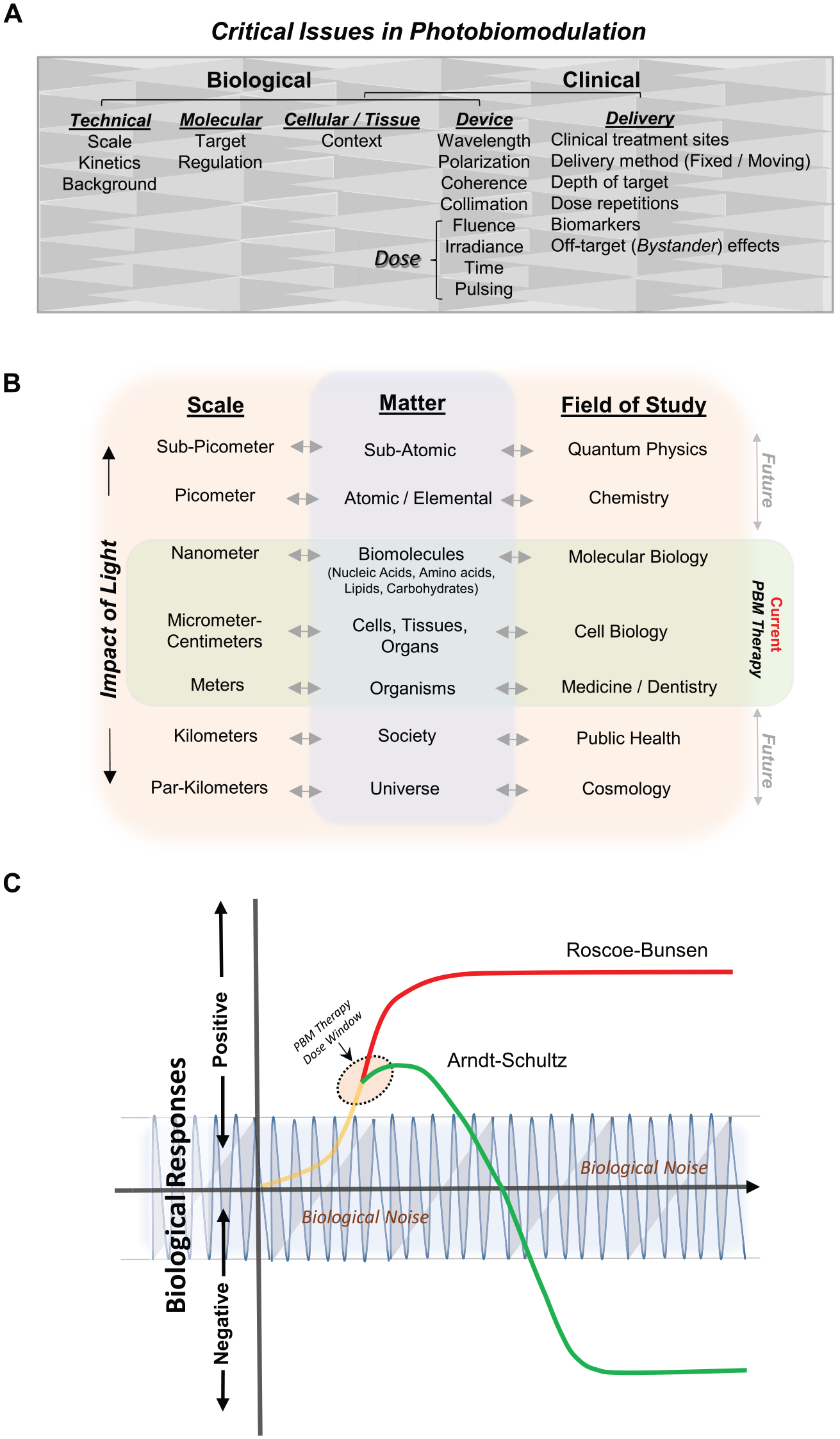
Critical aspects of photobiomodulation therapy. (
Current Challenges
Biological Mechanisms of PBM Therapy
Advances in optics and photonic technologies, along with a better understanding of light-tissue interactions, are spearheading the popularity of biophotonics for surgical and nonsurgical applications. Recent focus on low-dose photon-biological tissue interactions is central to applications in optical imaging and optogenetics with well-known intrinsic or engineered photoacceptors, such as light-activated genomic manipulations (light-activated CRISP-Cas9 effector; Polstein and Gersbach 2015). However, conventional molecular biology techniques are incapable of interrogating the infinitesimally minute nature and rapid kinetics (10−3 to 10−17 s) of endogenous photon-tissue interactions. This is further significantly compounded by the complex heterogeneous nature of biological systems (Fig. 1B). Additionally, the dynamic nature of biological systems resulting from active pathophysiologic processes—such as transcription, translation, signaling, metabolism, vascular and lymphatic flow, and respiratory movements, among others—that all inherently generate routine small to medium perturbations is collectively represented as background biological noise (Fig. 1C). Given the low-dose nature of PBM stimuli, rigorous studies have been challenging because of subtle responses in routine biological assays. Two specific paths forward would be to tease out the nominal PBM responses by employing large biological data sets with rigorous statistical analyses for low-probability events. Another approach is to utilize quantum biophysical and biochemical (subatomic) techniques to precisely assess these temporospatial events. While these quantum technologies are currently available, they are currently ill-equipped to deal with the heterogeneity and dynamic nature of biological systems. To better understand PBM mechanisms, an analogy could be drawn to the physical energy as a drug equivalent, a concept termed photoceuticals (Lin et al. 2010). This premise seems appropriate given that light satisfies both pharmacologic principles—namely, being absorbed and evoking a biological response. Based on the fundamental laws of Grotthuss-Draper (photochemical activation) and Stark-Einstein (photoequivalence), PBM events can be broadly divided into primary and secondary events (Fig. 2). A detailed description of these events with relevant examples is elaborated in the online Appendix.
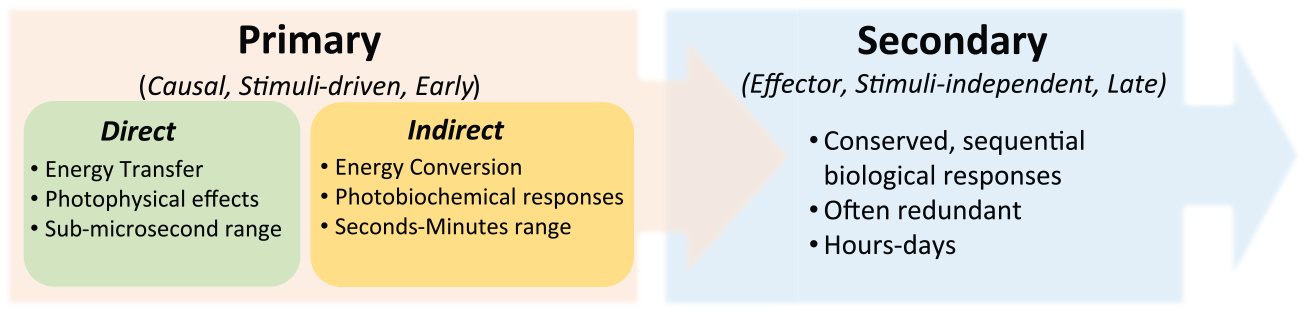
Timeline of photobiomodulation mechanistic events: Temporally phased primary photobiomodulation events involve photophysical, photochemical, and photobiological interactions. The secondary, noncausal photobiomodulation events are conserved biological responses that function as ubiquitous effector responses contributing to the eventual therapeutic outcomes.
Clinical Dosimetry for PBM Therapy
Extrapolating results from simple in vitro laboratory studies (solutions or monolayer cell cultures) to the complexity of in vivo systems predominantly hinges on nuances of light delivery systems. Partly recognizing this, PBM therapy has incessantly focused on device parameters that can be easily manipulated. Unfortunately, this approach has largely ignored the complexities of the photon-biological interactions. Device parameters are largely described around conventional linear photobiological principles—namely, the Roscoe-Bunsen rule dictating inverse reciprocation of intensity and duration. While this is certainly true for specific linear absorption events and within certain dose ranges, PBM biological responses classically evoke a nonlinear biphasic response referred to as the Arndt-Schulz law. These responses demonstrate a linear optimal threshold that, on continued stimuli, results in inhibitory or negative effects (Fig. 1C). This phenomenon potentially arises due to multiple aspects, such as the nonlinear physical process of multiphoton interactions and the inelastic scattering or presence of tightly regulated biological feedback regulation—all of which prevent simple stoichiometric responses. These nonlinear responses (“U” or “J” shaped dose curve) are well documented in a biological phenomenon termed hormesis (Calabrese et al. 2007). This field began amid much controversy, proposing therapeutic use of sublethal doses of ionizing radiation and biological toxins. However, rigorously done studies have countered these skepticisms, enabling specific hormetic concepts to be routinely used in medicine, such as pre- or post-conditioning for physical exercise and ischemic-reperfusion injury (Peake et al. 2015).
A large focus of PBM clinical therapy has been based on absorption, and it is reasonable to assume that there are wavelength-specific biological chromophores. Clinical results from a wide range of photonic sources—coherent (lasers) and noncoherent (LEDs and broadband light)—have remained equivocal. Besides wavelength, coherence, collimation, polarization, and pulsing have all been investigated, albeit not rigorously, as key determinants of PBM therapy (Fig. 1A). Among these, pulsing deserves special attention for multiple reasons. First, the fundamental dual nature of light as a particle (photon) and as a wave essentially implies an intermittent transfer of energy to biological tissues during PBM therapy, even when continuous wave illuminations are employed. Second, repetitive clinical dosing is commonly employed in PBM treatment protocols and can essentially be considered pulsed energy delivery over long durations. Third, practitioners often employ various treatment probe movements to reduce heat buildup and cover large treatment sites, especially with the small laser spot sizes. Finally, pulsing has been specifically noted to be efficacious in PBM treatments of fracture healing, traumatic brain injury, and analgesia (Hashmi et al. 2010; Tzabazis et al. 2011). A more elaborate discussion of these critical clinical variables in PBM dosing is in the online Appendix (Appendix Figs. 1, 2).
Wound Healing in the Craniofacial Complex with PBM Therapy
Wound healing is a central pathophysiologic process that maintains integrity of craniofacial tissues. The healing process consists of successive phases from hemostasis, inflammation, cell migration, matrix synthesis, and remodeling (Eming et al. 2014). As mentioned earlier, among the earliest observed effects of lasers was its ability to promote skin wound healing, and numerous studies, in vitro and in vivo, have subsequently validated this phenomenon (Mester et al. 1971; Yu et al. 1997; Whelan et al. 2001; Medrado et al. 2003; Peplow et al. 2010). Nonetheless, overall efficacy of PBM therapy in wound healing is, surprisingly, still considered equivocal (Posten et al. 2005).
Soft Tissue Healing with PBM Therapy
There are 2 distinct but related laser-associated procedures that cause some confusion with therapeutic PBM effects on wound healing. Clinical reports have noted better healing responses following laser surgery as compared with procedures performed with a surgical blade (Capon and Mordon 2003). This is particularly relevant to richly vascular oral tissue, such as tongue and palate, where improved visibility reduces inadvertent surgical trauma and blood loss, thereby aiding routine healing (Fig. 3). Other distinct current clinical scenarios include 1) the use of lasers to perform surgical curettage (debridement) in periodontal or peri-implant areas and 2) nonsurgical laser-assisted disinfection of pathogenic biofilms performed with an exogenous dye, termed antimicrobial PDT. These approaches are specifically useful in hard-to-instrument pockets and furcation defects (Aoki et al. 2015). While these 2 higher dose procedures (i.e., debridement and antimicrobial PDT) and their benefits (surgical precision, photocoagulation and disinfection) should not be considered PBM effects, it is prudent to point out that there are lower laser doses, within the PBM dose realm, delivered to tissues adjacent (bystander) to these operative sites (Appendix Fig. 3).
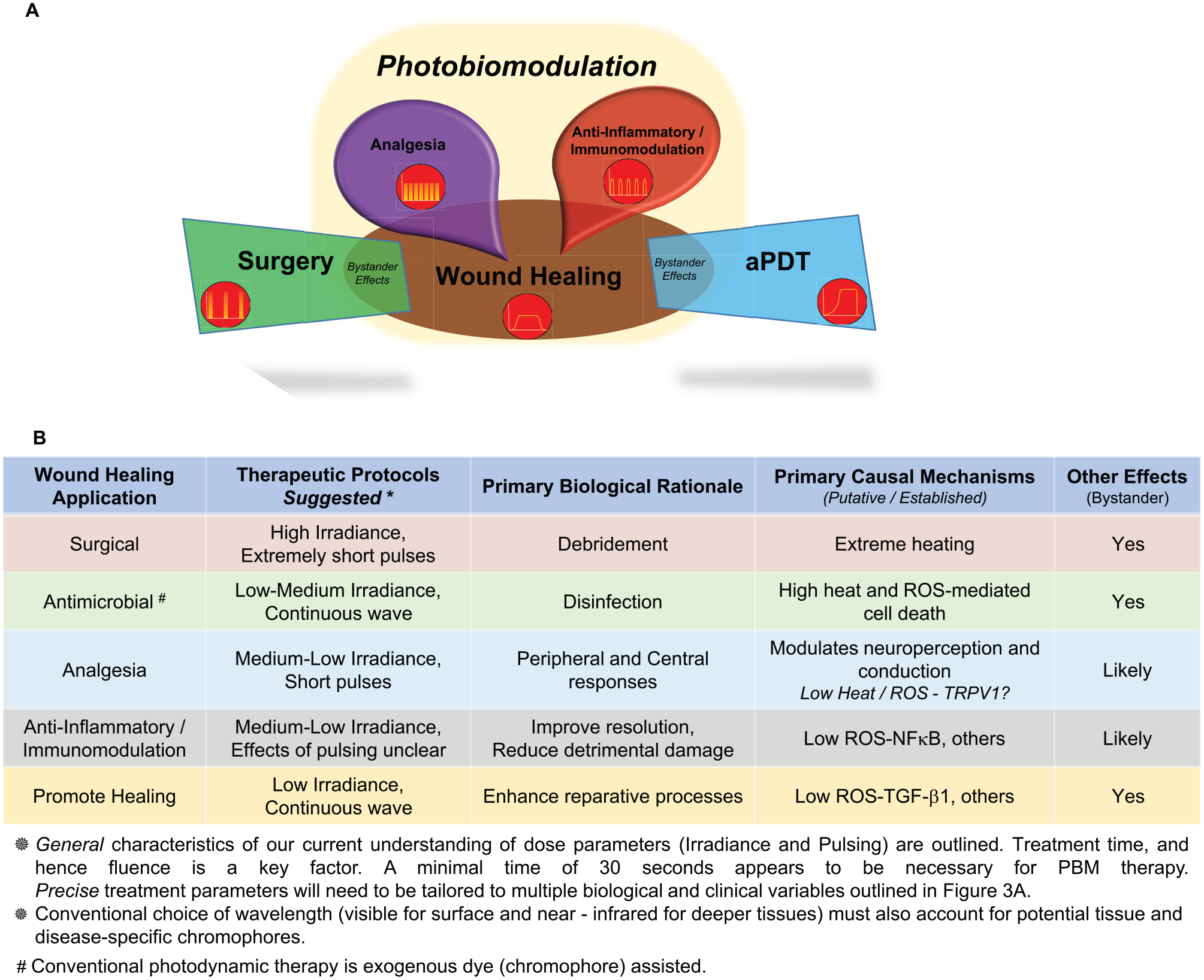
Clinical applications of biophotonics devices. (
Distinct effects of PBM have been noted with individual cell types involved in wound healing. Effects of PBM treatments on platelet biology have included increased mechanical rigidity and improved platelet functions, such as adhesion and sequestration of coagulation factors, which promoted wound healing in a mouse model of hemophilia (Hoffman and Monroe 2012). While this raises potential concerns for thromboembolic events, PBM treatments do not appear to disrupt the protective coagulative mechanisms (Subbotina et al. 2009). Studies combining platelet-rich plasma activated by low-dose laser treatments have noted better healing. However, these protocols have shown inconsistent clinical outcomes attributed to variations in the individual platelet-rich plasma preparations and PBM activation protocols employed (Nagata et al. 2014). Effects of PBM therapy on promoting roles of keratinocytes, fibroblasts, endothelial cells, neutrophils, macrophages, and mast cells in wound healing have also been outlined (Fujimura et al. 2014; Fekrazad et al. 2015). These roles include proliferation and expansion of these cells, promoting physiologic functions such as keratinocyte maturation, collagen synthesis and turnover by fibroblasts, wound contraction mediated by myofibroblast transformation, improved wound angiogenesis, neutrophil migration and functions, mast cell activation, and changes in macrophage subtypes (Burger et al. 2015; Fernandes et al. 2015; Sperandio et al. 2015). It should be noted that many of these studies were performed in vitro with isolated, individual cell types. Future studies could assess PBM responses in complex 3-dimensional coculture systems to more appropriately simulate the heterogeneous in vivo scenarios.
Inflammation has a direct role in clearing wound damage–induced debris and priming the site with potent factors to provide optimal healing environments. Pain is a damage-associated alarm signal that can lead to elaboration of neuroendocrine factors that modulate wound healing. Resolution of persistent pain or inflammation can promote healing responses (Serhan 2014). PBM therapy has been noted to modulate individual wound-healing phases, specifically pain and inflammation, even in nonhealing contexts. However, most current PBM wound protocols do not attempt to treat these individual phases despite growing evidence that these are biologically and mechanistically distinct responses that would benefit from discrete PBM dosing (Fig. 3B; Bjordal et al. 2003; Brondon et al. 2005; Sharma et al. 2011). This has important implications for PBM therapy in many oral diseases that have etiopathologic components of immune dysregulation, pain, and inflammation besides lack of healing. Some examples of these conditions include oral mucositis (postradiation or chemotherapy and graft-versus-host disease), herpes simplex, aphthous, lichen planus, pemphigus, Sjögren’s syndrome, temporomandibular joint disorders, orofacial pain, burning mouth syndromes, and paresthesia postextraction, among others (Sun and Tuner 2004; Bjordal et al. 2011; Lalla et al. 2014).
Our original observation for the role of TGF-β1 in PBM-treated wounds was largely motivated by its roles in wound healing (Arany et al. 2007). In this study, we noted increased active TGF-β1 in oral tooth extraction wounds treated with a near-infrared laser (904 nm, 3 J/cm2, 10 mW/cm2 for 300 s). We went on to note the ability of low-dose near-infrared lasers to induce various reactive oxygen species (ROS) in a dose-dependent manner (Arany, Cho, et al. 2014). These laser-generated ROS are sensed by a specific redox-sensitive methionine, at position 253 on the latency-associated peptide of latent TGF-β1, resulting in direct conformational activation of the latent TGF-β1 complex. Activation of TGF-β1 by low-dose laser treatment was noted in both cell free (ELISA, Western blots) and in the presence of cells (Western blots for phospho-Smad2 and TGF-β reporter assays). The ROS-mediated PBM activation appears to be restricted to TGF-β1 isoform because of a uniquely positioned redox-sensitive methionine that other isoforms (TGF-β2 and TGF-β3) lack and hence are not amenable to this particular mode of activation (Jobling et al. 2006). TGF-β has distinct, often opposite, effects on various phases of wound healing in a context-dependent manner (Ashcroft et al. 1999; Arany et al. 2006; Finnson et al. 2013). The early wound milieu has serum and platelets with abundant latent TGF-β1. As such, PBM-activated TGF-β1 could be harnessed to mediate its roles on various cells in wound healing, such as keratinocyte migration, fibroblast collagen synthesis and remodeling, wound contraction by myofibroblast transformation, angiogenesis, and neurogenesis among others. The specific ability of TGF-β1 to induce FoxP3 TRegs deserves particular attention for PBM treatments in immune-inflammatory ailments (Garlet et al. 2014; Chen and Konkel 2015). Besides microenvironment and distinct cell lineage interactions, PBM-generated ROS pathways initiated concomitantly will also be key determinants of downstream TGF-β1 responses in specific pathophysiological contexts.
Hard Tissue Healing with PBM Therapy
The craniofacial region has a range of mineralized hard tissues with remarkable diversity in composition, structure, and function, including enamel, dentin, cementum and bone. Attempts to regenerate enamel have been greatly limited because of a lack of readily accessible sources of enamel-forming cells (ameloblasts). Recent attempts at remineralizing (i.e., healing) incipient enamel lesions with electric currents as well as lasers combined with fluorides are showing great promise (Ivanoff et al. 2012; Liu et al. 2013). High-power lasers are becoming increasingly popular for excavation of decayed enamel and dentin as well as bone recontouring, with significant improvements in technology making devices more compact, affordable, and user-friendly. High-power lasers have also been used to physically occlude dentinal tubules (outer dentinal barrier) to alleviate tooth sensitivity, with moderately successful temporary outcomes (Sgolastra et al. 2013). Lasers have also been used to disinfect root canals with agitations (photon-induced photoacoustic streaming) and directly ablate contaminated radicular dentin walls (Lee et al. 2004; Olivi et al. 2014). While all these applications utilize varying doses of biophotonics illumination to ultimately promote overall healing, they do not constitute PBM therapy.
The presence of stem cells in the pulp and periodontium provides a great resource for regeneration of dentin, cementum, periodontal ligament, and bone. Prior studies have shown that PBM therapy is capable of promoting the reparative dentin induction (Suzuki et al. 2005; Shigetani et al. 2011). We recently demonstrated that one key mechanism in this process involves directed differentiation of dental and mesenchymal stem cells by low-power laser-activated latent TGF-β1 (Arany, Cho, et al. 2014; Arany, Huang, et al. 2014). These observations indicate that PBM therapy could be applied to promote tertiary dentin in pulp capping and tooth desensitization (internal dentin barrier). As outlined in the earlier soft tissue healing section, high-power laser curettage and disinfection of diseased periodontal tissues have been shown to promote healing and regeneration of the functional periodontal attachment complex (Aoki et al. 2015). Recent efforts have demonstrated the utility of using PBM therapy to promote regeneration of bone and cementum, focusing on extraction socket healing, fracture healing, and distraction osteogenesis (Alsulaimani et al. 2015). These direct effects of PBM on osteogenesis are the fundamental basis of recent clinical protocols to accelerate orthodontic tooth movement (Almpani and Kantarci 2015). This specific scenario is another great example where various nuances of clinical PBM therapy should be carefully optimized to achieve more reproducible and robust clinical outcomes. Specifically, more attention could be focused on delivery protocols for PBM doses to deeper target tissues and specific doses to modulate discrete biological phases, such as pain, inflammation, or immune responses (allowing higher and rapid delivery of orthodontic forces), versus the promotion of soft tissue (PDL) and bone healing followed by remodeling (consolidation). Recent interest in using PBM therapy for bisphosphonate-related osteonecrosis of the jaw has focused on its ability to reduce drug-associated cytotoxicity and promote inherent healing capacity of multiple oral cell types, including keratinocytes, fibroblasts, and osteoblasts (Porcaro et al. 2015). Interestingly, these therapeutic outcomes strikingly parallel ongoing efforts of utilizing PBM treatments to mitigate dysfunctional mitochondrial functions from noxious biological and environmental agents (Huang et al. 2014).
Quantum Mechanics Meets Clinical Dentistry
Dentistry has pioneered the use of biomaterials and surgical techniques for restorative and prosthetic replacements of natural biological structures. Concepts of healing and tissue regeneration have been largely limited to pulp and periodontal defects. Despite the enthusiasm and breadth of potential applications for PBM therapy, it is now critical to move away from its description as a universal panacea for all ailments and to pursue mechanistic precision medicine approaches. A major path forward appears to be development of anatomic site–specific, disease, and biological response–specific PBM clinical protocols. An exciting fundamental avenue is to explore PBM effects as basic interactions of electromagnetic radiation via entanglements within biological systems. Technical development of custom-built biophotonics devices de novo or adaptation of photonic delivery techniques used in optical (multiphoton) in vivo imaging could enable safe and effective PBM clinical delivery protocols. Moreover, naturally occurring molecules mediating PBM effects offer an endogenous optogenetic approach to interrogate and harness biological pathways, such as redox states, endogenous growth factors, and resident (naturally present) stem cells. Strikingly, unlike other current translational barriers in clinical regenerative medicine, widespread availability of clinically approved biophotonics units in dentistry offers a robust practitioner-based research network, potentially facilitating rapid clinical translation. In summary, PBM therapy offers various significant avenues to promote craniofacial healing and tissue regeneration, providing a fascinating new frontier for the next era of regenerative clinical dentistry.
Author Contributions
P. Arany, contributed to conception, design, and data acquisition, drafted and critically revised the manuscript. The author gave final approval and agrees to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The author serves in an honorary capacity in the following relevant positions: president, North American Association for Photobiomodulation Therapy; chair, Lasers in Dentistry, American Society of Lasers in Surgery and Medicine; cochair, Mechanisms of Photobio-modulation Therapy, International Society of Photonics and Optics; chair, University Committee and Academic Committee, Academy of Laser Dentistry; and chair, Awards Committee, Wound Healing Society.
The author acknowledges support from the Department of Oral Biology, School of Dental Medicine, University at Buffalo.
The author declares no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.