
Abstract
Transplantation of mesenchymal stem cells (MSCs), which possess self-renewing properties and multipotency, into a periodontal defect is thought to be a useful option for periodontal tissue regeneration. However, developing more reliable and predictable implantation techniques is still needed. Recently, we generated clumps of an MSC/extracellular matrix (ECM) complex (C-MSC), which consisted of cells and self-produced ECM. C-MSCs can regulate their cellular functions in vitro and can be grafted into a defect site, without any artificial scaffold, to induce bone regeneration. Accordingly, this study aimed to evaluate the effect of C-MSC transplantation on periodontal tissue regeneration in beagle dogs. Seven beagle dogs were employed to generate a premolar class III furcation defect model. MSCs isolated from dog ilium were seeded at a density of 7.0 × 104 cells/well into 24-well plates and cultured in growth medium supplemented with 50 µg/mL ascorbic acid for 4 d. To obtain C-MSCs, confluent cells were scratched using a micropipette tip and were then torn off as a cellular sheet. The sheet was rolled up to make round clumps of cells. C-MSCs were maintained in growth medium or osteoinductive medium (OIM) for 5 or 10 d. The biological properties of C-MSCs were evaluated in vitro, and their periodontal tissue regenerative activity was tested by using a dog class III furcation defect model. Immunofluorescence analysis revealed that type I collagen fabricated the form of C-MSCs. OIM markedly elevated calcium deposition in C-MSCs at day 10, suggesting its osteogenic differentiation capacity. Both C-MSCs and C-MSCs cultured with OIM transplantation without an artificial scaffold into the dog furcation defect induced periodontal tissue regeneration successfully compared with no graft, whereas osteogenic-differentiated C-MSCs led to rapid alveolar bone regeneration. These findings suggested that the use of C-MSCs refined by self-produced ECM may represent a novel predictable periodontal tissue regenerative therapy.
Introduction
Periodontitis is an inflammatory disease attributed to host immune responses to periodontal pathogenic bacteria, which is characterized by tooth-supporting tissue destruction, including alveolar bone, periodontal ligament, and cementum (Pihlstrom et al. 2005; Kajiya et al. 2010). If left untreated, periodontitis induces irreversible tissue damage that may lead to tooth loss. To date, several regenerative procedures, including guided tissue regeneration (Jepsen et al. 2002), the use of bioactive agents such as enamel matrix derivative (Bosshardt 2008), various growth factors (Larsson et al. 2016), or mediators of resolution of inflammation (Van Dyke et al. 2015), have been tested with the aim of achieving periodontal regeneration. Although it is unclear which common pathways are shared in response to various strategies, these techniques have proven at least somewhat effective in periodontal tissue regeneration. However, periodontal tissue regeneration is still challenging because it requires predictable reconstruction of 3 quite different tissues, including cementum, periodontal ligament, and bone. Therefore, to regenerate the triphasic interface between these diverse tissues, which is indispensable for functional periodontal tissue, novel cell therapies supplying the necessary stem cells are in demand because of their potential to differentiate into multiple lineages.
Mesenchymal stem cells (MSCs) have attracted considerable scientific and medical attention as an effective tissue engineering cell therapy for many years because of their self-renewing capacity and multipotency (Pittenger et al. 1999; Watson et al. 2014; Yousefi et al. 2016). We have previously investigated the effect of autologous bone marrow–derived MSC transplantation using atelocollagen gel as a cell scaffold in a beagle dog class III furcation defect model (Kawaguchi et al. 2004). As a result, MSC transplantation induced successful cementum and periodontal ligament regeneration. Importantly, alveolar bone regeneration in the MSC-grafted group was significantly higher than that of the no-graft group, although the amount of newly formed bone varied widely and successful bone regeneration did not necessarily occur (Kawaguchi et al. 2004). Therefore, to accelerate MSC-induced bone regeneration, we employed an osteointegrative biomaterial, beta-tricalcium phosphate (β-TCP), as a cell scaffold. However, even though the usage of β-TCP supported the contour of alveolar bone formation by MSCs in the early stage, β-TCP remained present even at 8 wk after surgery (Nagahara et al. 2015). In some cases, ankyloses were observed at 4 wk and 8 wk after transplantation.
Clinical success of cell-based tissue regenerative therapy seems to be highly dependent on techniques for transferring cells from the donor site to the target site. Injection of dissociated cell suspensions using gel material, grafting of synthetic/natural biomaterial frameworks seeded with stem cells, and combinations of these methods have been evaluated (Amini et al. 2012; Chen et al. 2012). However, these methods, including our previous approaches, as described above, have failed to produce predictable, controlled, and rapid healing of irreversibly damaged tissue because of the limitations related to the usage of an artificial scaffold and bringing out the transplanted cells’ potential (Bosshardt and Sculean 2009; Chen et al. 2016). To circumvent these drawbacks, we have recently established clumps of an MSC/extracellular matrix (ECM) complex (C-MSC), which consisted of cells and self-produced ECM (Kittaka et al. 2015). C-MSCs can be transplanted into bony lesions without artificial scaffold. Moreover, the implantation of C-MSCs, cultured with osteoinductive medium (OIM) in vitro, demonstrated greater new bone formation in a rat calvarial defect model. This finding implied that C-MSCs’ cellular function regulated in vitro can be exerted at the grafted site. Taken together, these findings suggested that C-MSCs can provide a novel cell therapy, which can avoid the problems associated with the biodegradability of artificial scaffolds and also can apply cells with well-regulated functions before transplantation.
Based on our previous success in bone regeneration in a rat calvarial defect model, we hypothesized that C-MSC cultures can be applicable for successful periodontal tissue regenerative therapy. To test this tentative hypothesis, in this present study, we transplanted autologous C-MSCs or OIM-treated C-MSCs without any artificial scaffold into a beagle dog inflamed class III furcation defect model and evaluated the periodontal tissue–regenerative capacities.
Materials and Methods
Animals
Seven beagle dogs, which was the fewest number of animals possible, were maintained in a vivarium, with the room temperature set at 22 ± 2°C and a 12-h light/dark cycle (lights on/off at 8:00 a.m./8:00 p.m.), and were given ad libitum access to food and water. Experimental procedures using dogs were approved by the Committee of Research Facilities for Laboratory Animal Science, Hiroshima University School of Medicine, Japan (protocol number A14-106). This study was performed in accordance with ARRIVE (Animal Research: Reporting In Vivo Experiments) guidelines for preclinical animal studies.
Dog MSCs
MSCs were collected from ilium bone marrow taken from 7 female 12- to 20-mo-old beagle dogs as previously described (Nagahara et al. 2015). Briefly, bone marrow aspirates of 1 mL were taken from the iliac crest of each animal with pentobarbital anesthesia (40 mg/kg body weight; Abbott Laboratories). Cells from the bone marrow were suspended in Dulbecco’s modified Eagle’s medium (DMEM; Sigma-Aldrich) supplemented with 10% fetal bovine serum (FBS; Biowest), 100 U/mL penicillin (Sigma-Aldrich), 100 µg/mL streptomycin (Sigma-Aldrich), and 500 ng/mL amphotericin B (Invitrogen) and were seeded at a density of 2 × 108 cells/100-mm plastic plates (Corning). Floating cells were removed after 72 h, and the adherent cells were subsequently expanded. Cells at the third passage were used in experiments as dog MSCs. The characteristics of MSCs were identified by conducting osteogenic, adipogenic, or chondrogenic induction as described in the Appendix Materials and Methods. Dog MSCs differentiated into osteogenic, adipogenic, or chrondrogenic cells, suggesting their multipotency (Appendix Fig. 1A–C).
Preparation of Dog C-MSCs
C-MSCs were prepared as reported previously with minor modifications (Kittaka et al. 2015). Briefly, MSCs were seeded at a density of 7.0 × 104 cells/well into 24-well plates (Corning) and cultured with high glucose DMEM (Sigma-Aldrich) supplemented with 10% FBS, 100 U/mL penicillin, and 100 µg/mL streptomycin (growth medium), in the presence of 50 µg/mL L-ascorbic acid (Sigma-Aldrich), for 4 d. To obtain C-MSCs, confluent cells that had formed on the cellular sheet, consisting of the ECM produced by MSCs themselves, were scratched using a micropipette tip and then torn off. The MSC/ECM complex was detached from the bottom of the plate in a sheet shape and rolled up to make round clumps of cells. After a 1-d incubation, a 1- to 1.5-mm-diameter clump of C-MSCs was obtained. These cells were transferred into a 24-well ultra-low-binding plate (Corning) and maintained in growth medium or OIM (growth medium supplemented with 10 nm dexamethasone [Sigma-Aldrich], 50 µg/mL L-ascorbic acid, and 10 mm β-glycerophosphate [Sigma-Aldrich]) for 5 or 10 d.
Staining of C-MSCs
C-MSCs were fixed with 4% paraformaldehyde in phosphate-buffered saline (PBS). The samples were embedded in paraffin, and 5-µm-thick sections were cut using a microtome. Then, the samples were stained with hematoxylin and eosin (H&E) or alizarin red S and observed using a light microscope. To detect apoptotic cells, paraffin-embedded samples were assessed by using the DeadEnd Fluorometric TUNEL System (Promega). The fluorescence signals were detected using a Zeiss LSM 510 laser scanning confocal microscope (Zeiss Microimaging). Three independent experiments were performed.
Type I Collagen Expression in C-MSCs
C-MSCs were fixed with 4% paraformaldehyde in PBS. The samples were embedded in Tissue-Tek OTC compound (Sakura), and 20-µm-thick sections were cut using a cryostat. After washing the sections with PBS, nonspecific binding was blocked by incubation for 30 min with PBS containing 1% bovine serum albumin (BSA) and 0.1% Triton X-100. These sections were treated with a rabbit anti–type I collagen IgG antibody (1:500; Abcam) at 4°C overnight. After washing with PBS, the samples were incubated with an Alexa Fluor 594 goat anti-rabbit IgG antibody (1:200; Invitrogen) for 1 h at room temperature. Nuclei were counterstained with 4′,6-diamidino-2-phenylindole (DAPI) (5 µg/mL; Invitrogen). After rinsing the samples with PBS, fluorescence signals were detected using a Zeiss LSM 510 laser scanning confocal microscope (Zeiss Microimaging). Three independent experiments were performed.
Calcium Content in C-MSCs
C-MSCs were lysed using 0.5 N hydrochloric acid solution with sonication. Dissolved calcium was then measured using a Calcium E-test kit (Wako). The absorbance of the resultant solution was measured at 610 nm using a microplate reader. Three independent experiments were performed.
Experimental Periodontitis Model and C-MSC Transplantation Procedures
Seven female beagle dogs (4 dogs for 8-wk observation and 3 dogs for 12-wk observation, aged 12 to 20 mo) were employed as an inflammatory class III furcation defect model, as previously described (Nagahara et al. 2015). Surgery was performed under general anesthesia with pentobarbital and local infiltrated anesthesia with 2% lidocaine (DENTSPLY-Sankin Co.). In total, 24 mandibular premolars on the right and left sides from 7 beagle dogs were randomly selected. After sulcular incisions, full-thickness flaps were elevated, and class III furcation defects, of which height from the cemento-enamel junction to the reduced alveolar crest was 4 mm, were created surgically using slowly rotating round burs and bone chisels. Exposed cementum and periodontal ligaments were completely removed. To indicate the bottom of the defect, reference notches were placed on the both mesial and distal roots. Then, the defects were infused with alginate impression materials (Morita) to induce inflammation. After 1 wk, the alginate was removed surgically, and scaling and root planing was conducted. One week after periodontal treatment, cell transplantation was carried out. Briefly, a total of 768 C-MSCs cultured in growth medium (GM) or OIM for 5 d were generated using MSCs isolated from each of the 7 dogs. Then, after careful scaling and root planing, autologous 48 C-MSCs or OIM-treated C-MSCs were directly transplanted into the defect with no artificial scaffold, as shown in Figure 2A, and a no-graft group was included as a control (n = 4/group for 8-wk and 12-wk observation, respectively). The flap was then closed using 4-0 silk sutures. During the experimental period, good oral hygiene was maintained by swabbing and brushing with 0.2% povidone-iodine (Meiji-seika Co.). These procedures did not affect healthy status of all animals.
Tissue Preparation and Micro–Computed Tomography and Histological Analysis
At 8 and 12 wk after transplantation, anesthetized beagle dogs were perfused with 4% paraformaldehyde in 0.1 M sodium phosphate buffer (pH 7.2). The mandibles containing the premolars were dissected and subjected to micro–computed tomography (CT) analyses with SkyScan-1176 (Bruker). Three-dimensional reconstructions were generated using CTV-OX software (Bruker), and the newly formed bone volume and bone mineral density inside the bony lesion was determined using CT-An software (Bruker). Because the periodontal ligament space and bone marrow cavity were present in normal periodontal tissue, the percentage of bone volume in normal specimens was 60%. Then, samples were decalcified with KCX (Falma) for 4 wk. After decalcification, the samples were dehydrated through graded ethanol, cleared with xylene, and embedded in paraffin. Serial sections (5 µm thickness) were cut in the mesial-distal plane throughout the buccal-lingual extension of the teeth. These sections showing the center of the furcation site were then stained with H&E or Azan and observed using a light microscope.
Morphometrical Analysis
The length of newly formed cementum and bone area in H&E-stained samples were measured using ImageJ Java-based image processing software (National Institutes of Health). New cementum formation was represented as a percentage of the length of new cementum formed along the denuded root surface on the specimen to the total root surface length from notch to notch (Nagahara et al. 2015). The area of newly formed bone in each specimen was calculated as the percentage of the area surrounded by the reference notches at the mesial and distal root surfaces facing the bone defect (Nagahara et al. 2015). Three sections from buccal, central, and lingual sides of each tooth were chosen for morphometric analyses. Because the periodontal ligament space was present in normal periodontal tissue, the percentage of bone area in normal specimens was 83%.
Statistical Analysis
Data were analyzed using Student’s t test or analysis of variance (ANOVA). Values of P < 0.05 or P < 0.01 were considered significant.
Results
Biological Properties of C-MSCs In Vitro
Dog C-MSCs were generated as described in the Materials and Methods section (Fig. 1A). At the beginning of C-MSC culture, the cells and ECM complex produced a sheet shape, and the cell sheets were rolled up to form round cell clumps in a time-dependent manner (Fig. 1B). Immuno-fluorescence analysis revealed that abundant type I collagen fabricated the form of C-MSCs (Fig. 1B). OIM treatment apparently elevated calcium deposition, which was identified by alizarin red staining in C-MSCs at day 10, whereas C-MSCs cultured with growth medium did not show red staining (Fig. 1C). Consistent with alizarin red staining, the calcium content was increased significantly in C-MSCs cultured in OIM for 10 d (Fig. 1D). In addition, the number of terminal deoxynucleotidyl transferase (TdT) dUTP nick-end labeling (TUNEL)–positive apoptotic cells was apparently elevated by OIM treatment for 10 d (Fig. 1C). These findings indicated that dog C-MSCs consisted of both cells and self-produced type I collagen and possessed osteogenic differentiation capacity in vitro. Because OIM treatment for 10 d may induce C-MSCs to become calcific, which was characterized by calcium deposition and cell apoptosis, in the following study, we focused on C-MSCs cultured with growth medium or OIM for 5 d.
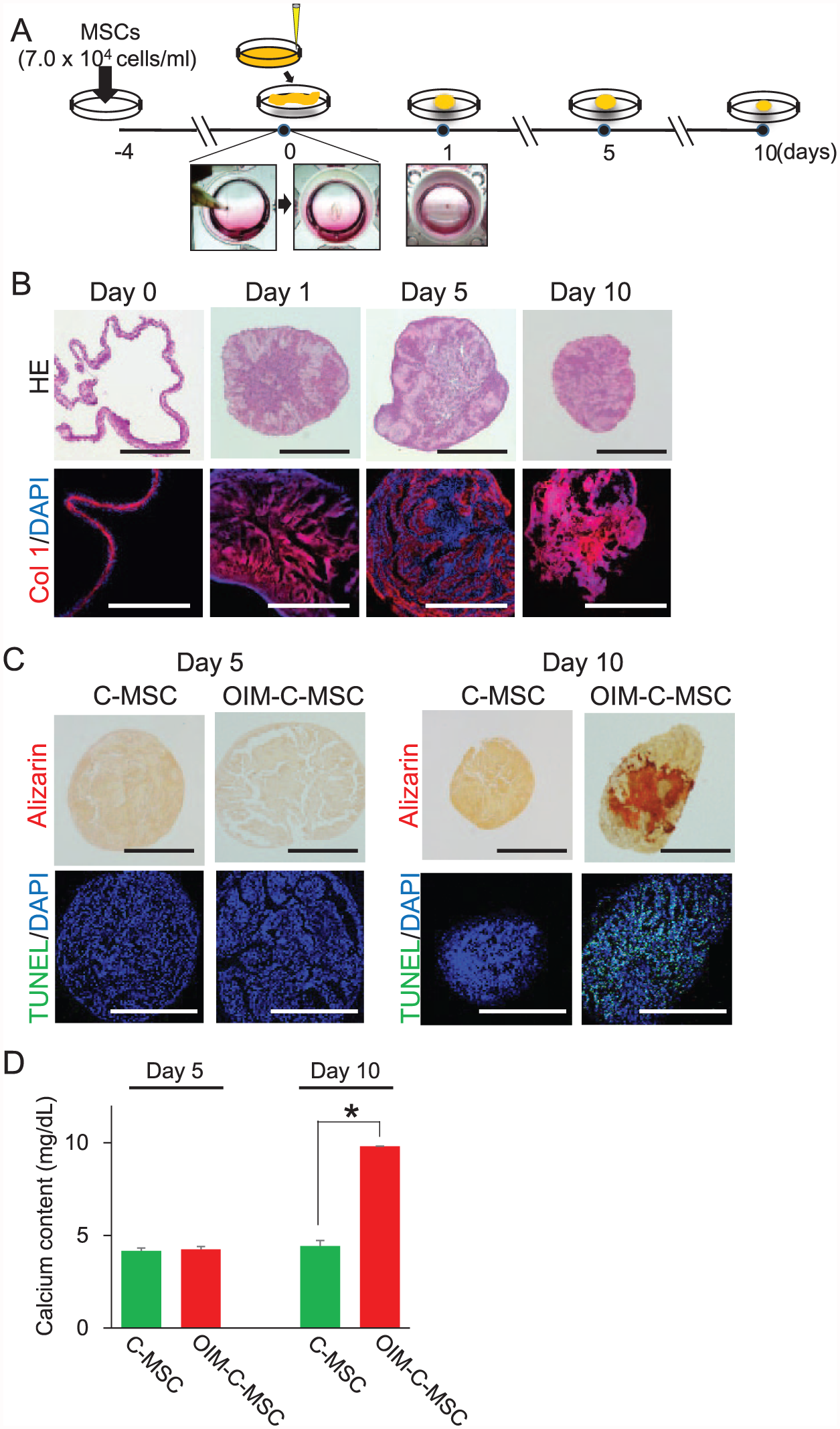
Generation of dog clumps of a mesenchymal stem cell (MSC)/extracellular matrix (ECM) complex (C-MSCs) and their biological properties in vitro. (
Periodontal Tissue Regeneration Induced by C-MSCs Transplantation
To investigate the periodontal tissue regenerative efficacy of C-MSCs, a beagle dog class III furcation defect model was employed. C-MSCs (cultured with growth medium for 5 d) or OIM–C-MSCs (cultured with OIM for 5 d) were grafted into the defect with no artificial scaffold and were stable in the lesion area (Fig. 2A). Micro-CT 3-dimensional reconstructed and single cut images showed unsuccessful bone regeneration in the no-graft groups at 8 and 12 wk after surgery (Fig. 2B, C). C-MSC and OIM–C-MSC implantation induced bone regeneration along the denuded root surface surrounding the lesion area but not from the bone defect edge at 8 wk after surgery (Fig. 2B). In addition, the newly formed bone observed in the OIM–C-MSC transplanted groups seemed to be denser than that of the C-MSC grafted group (Fig. 2B). However, at 12 wk after surgery, successful bone regeneration was induced in both C-MSC and OIM–C-MSC transplanted areas (Fig. 2C).
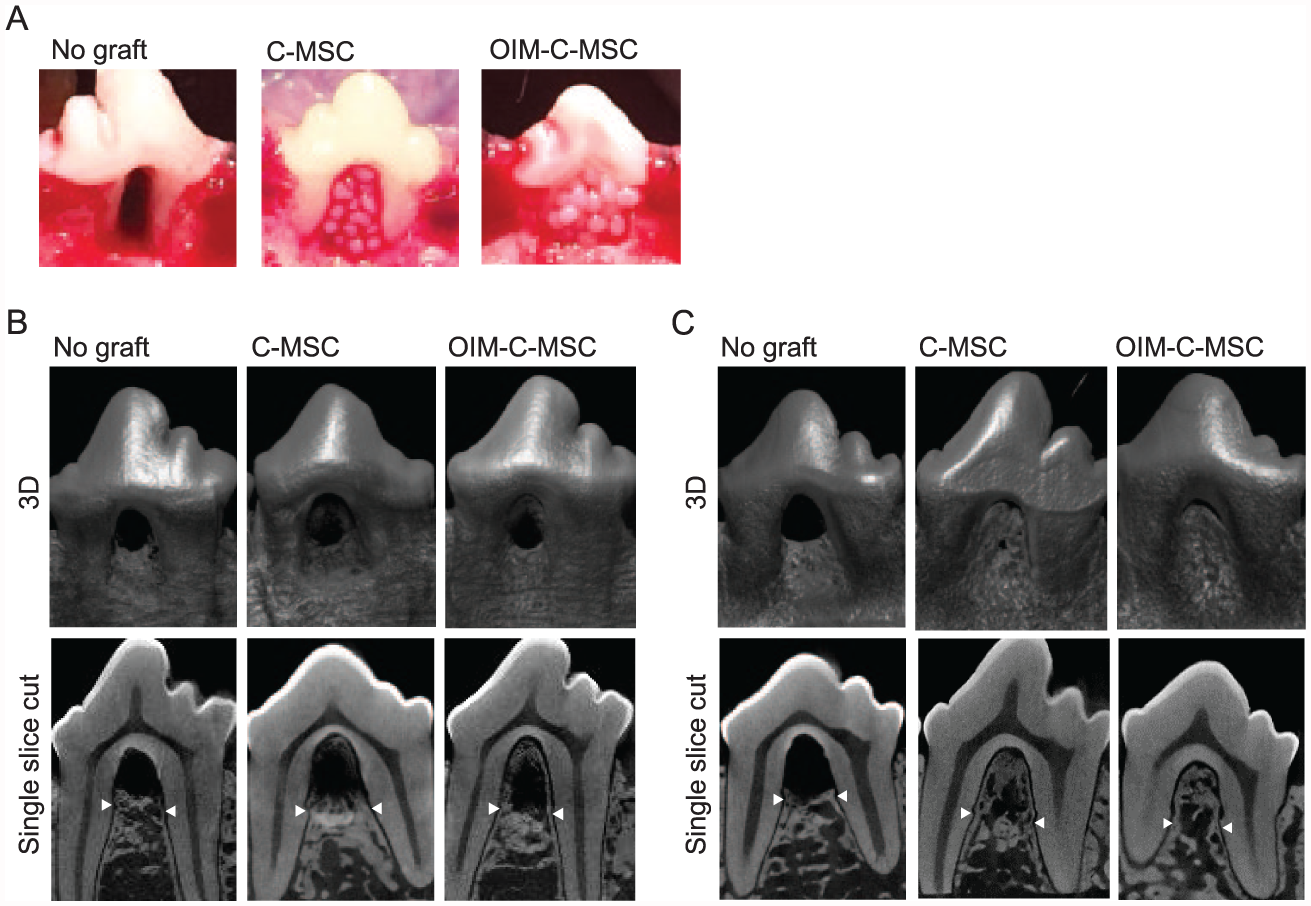
Transplantation of clumps of a mesenchymal stem cell (MSC)/extracellular matrix (ECM) complex (C-MSCs) without artificial scaffold induced periodontal tissue regeneration in a beagle dog class III furcation defect model. (
To evaluate periodontal tissue regeneration more precisely, histological analysis was conducted (Figs. 3 and 4). Consistent with the micro-CT analysis, the no-graft group showed unsuccessful bone regeneration at 8 and 12 wk after surgery (Figs. 3A and 4A). Moreover, epithelium invasion including inflammatory cell infiltration was observed at the top of the furcation where no cementum and periodontal ligament were formed (Figs. 3B and 4B). On the other hand, at 8 wk after C-MSC transplantation, almost of all denuded root surface was covered by periodontal tissue, which consisted of cementum, periodontal ligament, and bone (Fig. 3C, 3D-(d), and 3D-(e)), although the new bone formation in the regenerated periodontal tissue was not complete (Fig. 3C). OIM–C-MSC implantation also showed a similar pattern of periodontal tissue regeneration accompanied with considerable new bone formation (Fig. 3E, 3F-(g), and 3F-(h)). Of note, in the area surrounded with the new bone, eosin densely stained bone-like tissue, and mononuclear cells were observed in C-MSC and OIM–C-MSC grafted groups (Fig. 3D-(c) and Fig. 3F-(f)). At 12 wk after transplantation, both C-MSCs and OIM–C-MSCs achieved successful periodontal tissue regeneration (Fig. 4C, E) consisting of mature alveolar bone, periodontal ligament, and cementum (Fig. 4D-(d), 4D-(e), 4F-(g), and 4F-(h)). Importantly, Sharpey’s fibers connecting bone and cementum were also observed in both the C-MSC and OIM–C-MSC grafted groups, suggesting the presence of a functional periodontium (Fig. 4D-(d), 4D-(e), 4F-(g), and 4F-(h)). In addition, even in areas where bone regeneration did not occur, immature bone-like tissue was also seen in both groups (Fig. 4D-(c) and 4D-(f)). Quantitative analysis of new cementum length showed that C-MSCs as well as OIM–C-MSCs induced significantly longer new cementum than that of no-graft group (Fig. 5A). Morphometric analyses of new bone area demonstrated that bone regeneration in the OIM–C-MSC group was significantly higher than in C-MSCs as well as the no-graft group at 8 wk after surgery (Fig. 5B). However, measurements of the net volume and density of regenerated alveolar bone using micro-CT images showed that significantly higher bone volume and bone mineral density were induced in the C-MSC group than in the no-graft group, and OIM–C-MSCs demonstrated the highest bone volume and mineral density at 8 wk (Fig. 5C, D). At 12 wk after surgery, morphometric and micro-CT analysis indicated that OIM–C-MSCs as well as C-MSCs caused similar amounts of new bone formation, which were approximately at the maximum level (Fig. 5B–D).
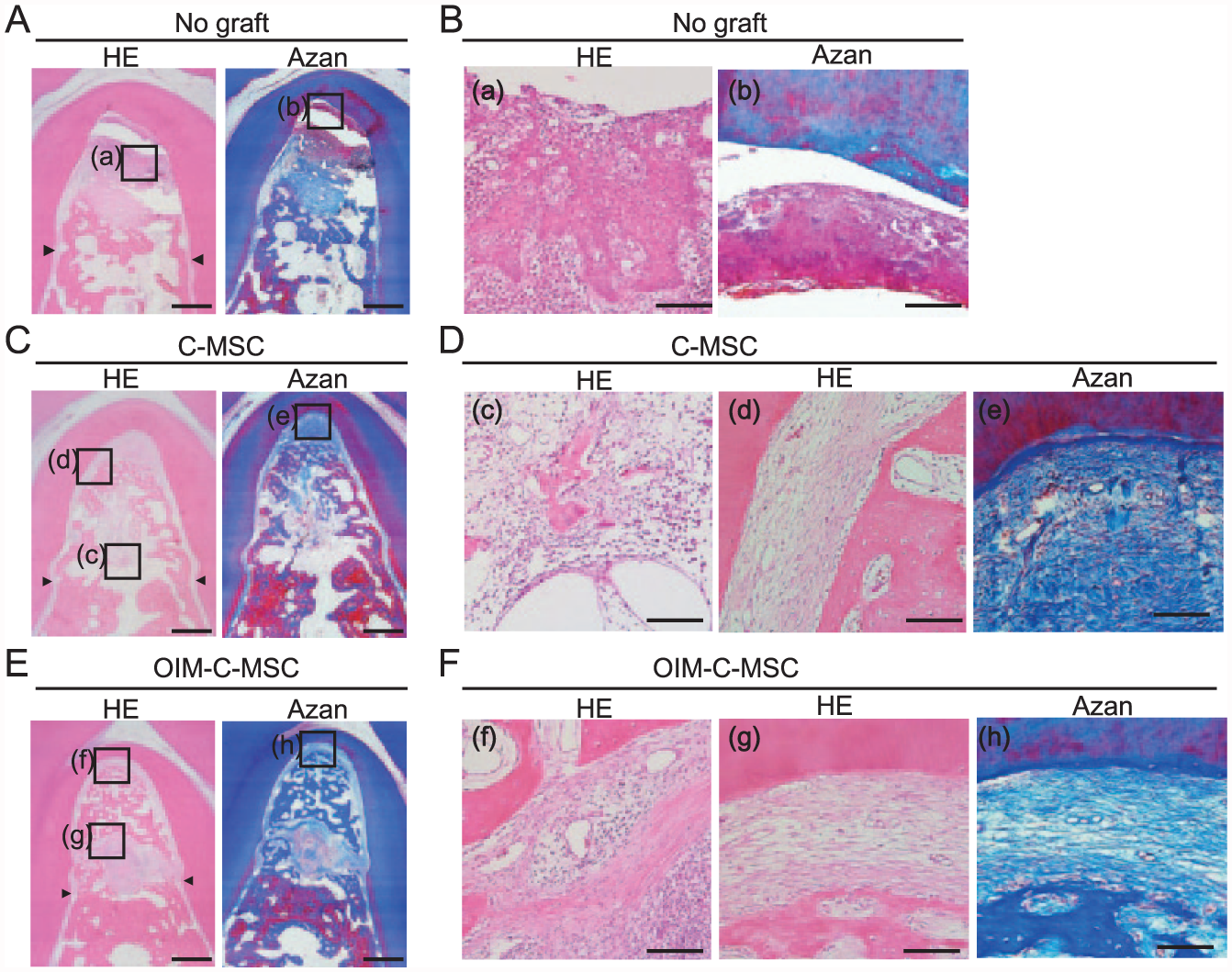
Histological analysis of class III furcation defects at 8 wk after surgery. (
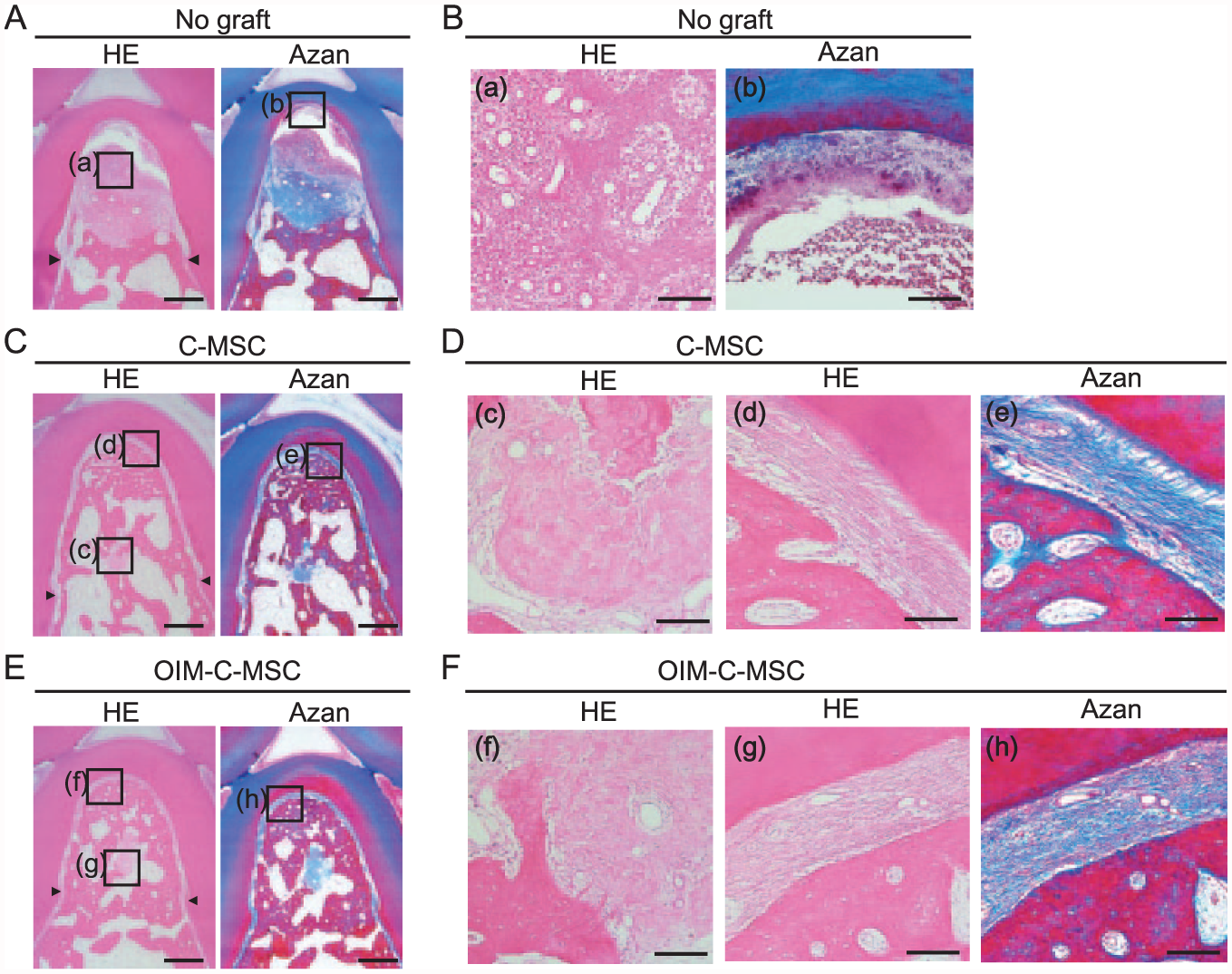
Histological analysis of class III furcation defects at 12 wk after surgery. (
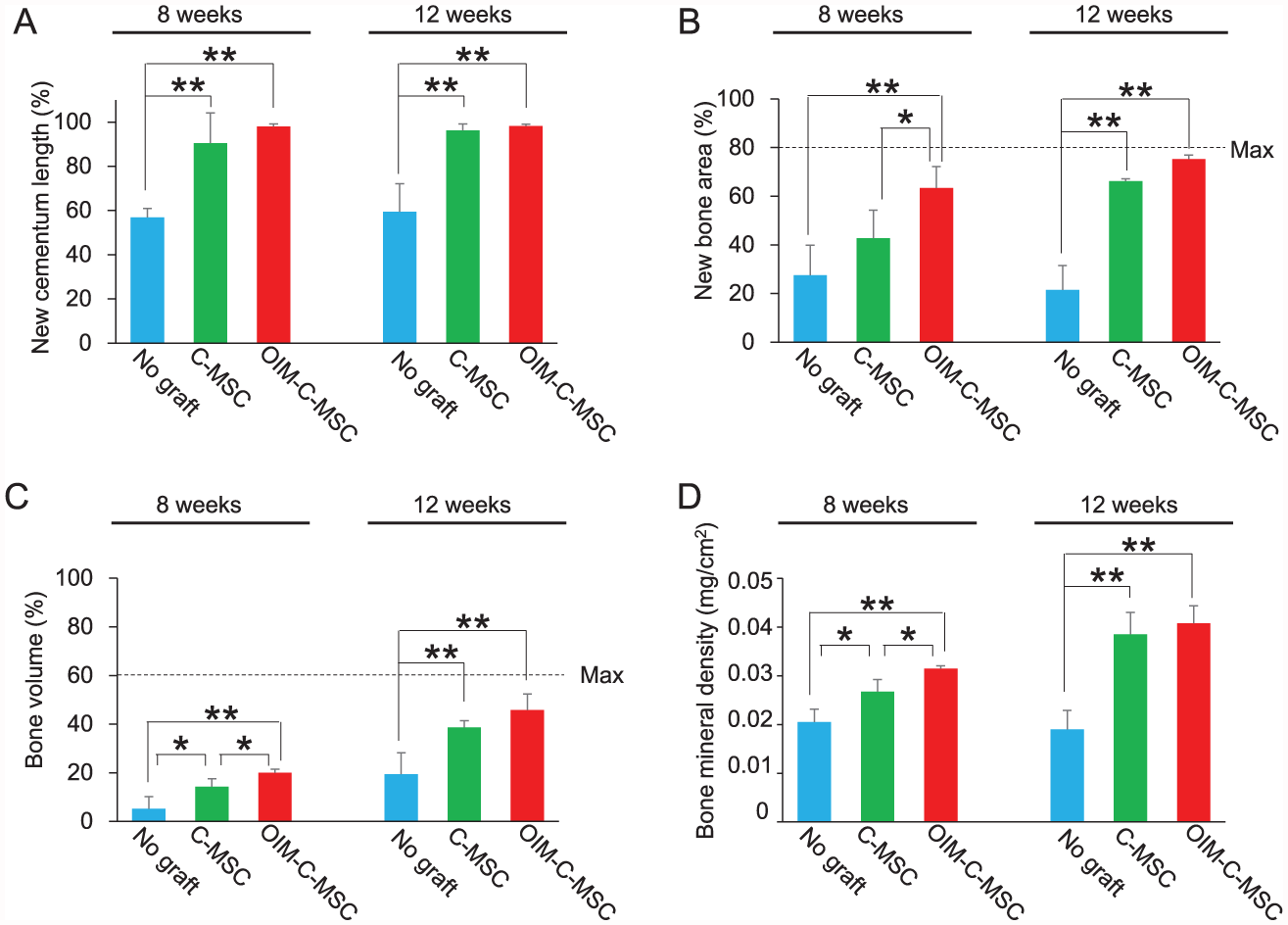
Percentage of new cementum length, new bone area, and bone volume determined by morphometric and micro–computed tomography analyses. The graphs show the percentage of new cementum length (
Discussion
This present study demonstrated that C-MSC transplantation induced successful periodontal tissue regeneration in a beagle dog furcation class III defect model. Although it is unclear whether the preparation of the “clumps” affected the MSCs function, the advantage of C-MSCs may be that an artificial scaffold is not required for MSC transplantation. This is because the therapy using C-MSCs will be untroubled by the anticipated problems of artificial scaffolds, including biocompatibility, infection, or inflammation (Oreffo and Triffitt 1999; Bose et al. 2012). However, because the dog class III furcation defect model may not reflect the human case, larger bone defects in clinically advanced periodontitis still seem to be a challenge for C-MSC transplantation therapy. For instance, human class III furcation defects, which could be larger defects than those of beagle dogs, will require the transplantation of approximately 200 to 300 C-MSCs. It is unclear if all transplanted C-MSCs remain in the lesion area. Accordingly, to graft more than several hundred C-MSCs appropriately into larger damaged tissue areas, combined use of some artificial scaffold may be needed.
At 12 wk after implantation, both C-MSCs and OIM–C-MSCs showed mature successful periodontal tissue regeneration. However, the new alveolar bone formation in the OIM–C-MSC grafted group was obviously faster than in the C-MSC transplanted group at 8 wk after surgery. Consistent with this finding, our previous study also reported that OIM–C-MSCs induced robust bone formation in a rat calvarial defect model (Kittaka et al. 2015). These facts implied that OIM–C-MSCs possess greater bone formation capacity and may be a better candidate to treat more critical periodontitis such as 1-wall periodontal defects.
In this C-MSC transplantation study, it was possible that self-produced ECM but not the grafted cells play a role in periodontal tissue regeneration. To test this possibility, we transplanted C-MSCs cultured with OIM for 15 d, which was composed of a self-produced ECM scaffold without living cells (Appendix Fig. 2A). Of note, implantation of C-MSCs cultured with OIM for 15 d failed to induce periodontal tissue regeneration at 12 wk after surgery (Appendix Fig. 2B–D). This finding implied that live MSCs in C-MSCs were indispensable in inducing periodontal tissue regeneration.
Previous reports, evaluating the effect of growth factors or MSC transplantation for periodontal tissue regeneration (Takeda et al. 2011; Nagahara et al. 2015), consistently demonstrated that new bone formation occurred from the edge of the defect rapidly, and then the regeneration reached the top of the furcation at a later period. These studies led us to speculate that signals provided from the remaining bone may stimulate osteogenic differentiation of MSCs and that signals from soft tissue such as gingiva or periodontal ligament may inhibit osteogenesis. To support this hypothesis, we revealed previously that a humoral factor of periodontal ligament cells ameliorates MSC osteogenic differentiation in vitro (Mizuno et al. 2008). However, this present study showed that both C-MSCs and OIM–C-MSCs first formed the contour of alveolar bone, and then the inside surrounded with the newly formed bone was filled by mature cells. As far as we know, such a unique healing process has not been reported. There might be an unknown interaction between grafted C-MSCs and host residual cells.
Regarding this healing process, it is of note that the cementum and periodontal ligament regeneration pattern was very similar in previous studies and with a similar C-MSC transplantation approach. Briefly, successful filling of the periodontal space consisting of cementum and periodontal ligament was observed before new bone maturation, although it was unclear if host or grafted cells contributed to form the periodontal ligament space in this study. However, it was reported that brain-derived neurotrophic factor induced cementum and periodontal ligament formation before successful alveolar bone regeneration, suggesting the cementum and periodontal ligament regenerative capacity of host cells (Konishi et al. 2016). In addition, it is widely accepted that MSCs can facilitate bone repair based on their multiple regenerative abilities, which include direct cell differentiation effects (Nilsson et al. 1999), and on indirect paracrine effects, such as the activation of host tissue repair (Granero-Moltó et al. 2009). Therefore, it might be possible that host residual cells stimulated by C-MSCs may play a crucial role in periodontal ligament and cementum regeneration, although additional studies investigating the interaction between host cells and grafted C-MSCs will be required.
In conclusion, the use of C-MSCs refined by self-produced ECM, which can be induced to undergo osteogenic differentiation in vitro, may represent a novel periodontal tissue regeneration cell therapy.
Author Contributions
M. Takewaki, contributed to conception, design, data acquisition, analysis, and interpretation, drafted the manuscript; M. Kajiya, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; K. Takeda, contributed to design and data analysis, drafted the manuscript; S. Sasaki, S. Motoike, N. Komatsu, contributed to design and data acquisition, drafted the manuscript; S. Matsuda, K. Ouhara, contributed to conception and data interpretation, critically revised the manuscript; N. Mizuno, contributed to conception, data analysis, and interpretation, critically revised the manuscript; T. Fujita, H. Kurihara, contributed to the conception, design, data analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
We thank Daniel Mrozek, who provided English-language editing services on behalf of Medical English Service (Kyoto, Japan).
This work was supported by JSPS KAKENHI grants JP15H05053 (Grant-in-Aid for Scientific Research (B)) and JP2681814 (Grant-in-Aid for Young Scientist (B)).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.