
Abstract
Oral clefts play an essential role in disturbed odontogenesis of the deciduous and permanent dentition, yet little is known about this relationship. We investigated, within the categories cleft lip with or without alveolus (CL ± A) and cleft lip, alveolus and palate (CLAP), whether different CL subphenotypes based on morphological severity of the cleft show different dentition patterns and whether a more detailed subdivision of the incomplete CL has clinical relevance. In this retrospective study, 345 children with nonsyndromic unilateral CL ± A and CLAP from the Dutch Association for Cleft Palate and Craniofacial Anomalies (NVSCA) registry were included to assess the association between the CL subphenotypes and lateral incisor patterns. Five different deciduous and permanent patterns of the lateral incisor were distinguished: located in normal position (pattern z/Z), in the anterior segment (pattern x/X) or in the posterior segment of the cleft (pattern y/Y), one in each segment of the cleft (pattern xy/XY), and agenesis of the lateral incisor (pattern ab/AB). Analyses were performed by using multinomial logistic regression models. Children born with a vermillion notch or a one-third to two-thirds CL were most likely to have a deciduous pattern x and a permanent pattern X, while children born with a two-thirds to subtotal CL were most likely to have deciduous pattern xy and a permanent pattern X compared to children with a complete CL that predominantly had deciduous pattern y and a permanent pattern AB. Based on the relationship of the CL morphology with the deciduous dentition, subdivision of the CL morphology into vermillion notch to two-thirds CL, two-thirds to subtotal CL, and complete CL appears to be an optimal subdivision. Our results indicate that a more detailed subdivision of the CL has clinical relevance and that critical factors in the pathogenesis of the CL are also critical for the odontogenesis.
Introduction
Oral clefts are one of the most common congenital anomalies, with a prevalence of 1 in 700 live births (Mossey et al. 2009). Their phenotypes are complex and heterogeneous and involve the lip, the alveolus (i.e., primary palate), and the hard and soft palate, including the uvula (i.e., secondary palate). During embryogenesis, the primary and secondary palates are formed by subsequent outgrowth, fusion, and differentiation (into bone and musculature) of the facial swellings and palatine processes, respectively (Krapels et al. 2006; Luijsterburg et al. 2014). Clefts occur when normal embryological development of the primary and/or secondary palate is disturbed; the incisive foramen forms the demarcation between them. Normal development and thus these complex and heterogeneous defects are related to different cell biological mechanisms, genes, and time frames in embryogenesis. Consequently, they can be classified as fusion defects, differentiation defects, or a combination of both. For example, fusion defects of the primary palate concern complete clefts of the lip (CLs) with complete or incomplete alveolar clefts (CAs). By contrast, incomplete and subcutaneous CLs with or without involvement of the alveolus are differentiation defects that develop after fusion of the primary palate (Luijsterburg et al. 2014; McBride et al. 2016). In addition, accurate phenotyping is of crucial importance for the understanding of both the epidemiology and etiology of oral clefts, because the power to detect effects is weakened when heterogeneous groups are treated as a single entity. Part of accurate phenotyping is the careful attention to (sub)clinical phenotypes that may further our understanding and can include minor structural variants such as dental anomalies (Dixon et al. 2011).
Dental anomalies are common in all phenotypes of oral clefts and may present a further grading of clefts. The most prevalent dental anomalies in cleft lip with or without alveolus (CL ± A) and cleft lip, alveolus and palate (CLAP) cases are located at the position of the lateral incisor on the cleft side. At this position, different dentition patterns are identified (i.e., hypoplastic, missing, or double lateral incisors) (Bøhn 1963; Tsai et al. 1998). These dental anomalies are postulated to be the result of fusion defects of facial swellings (i.e., (in)complete CA) (Hovorakova et al. 2006). But dental anomalies have also been seen in patients with incomplete CLs and normal alveolar processes (Hansen and Mehdinia 2002; Vermeij-Keers et al., in press) as in the healthy population (Haugland et al. 2013). Therefore, it is most likely that initiation and regulation of tooth development occur during the differentiation of the primary palate into the lip and alveolus. That is after the fusion process of the facial swellings (Vermeij-Keers et al., in press) and may present an excellent way for further phenotyping (i.e., subphenotypes).
To identify these subphenotypes of oral clefts, a unique registration system was introduced by the Dutch Association for Cleft Palate and Craniofacial Anomalies (NVSCA) in 1997 (Luijsterburg and Vermeij-Keers 2011; Luijsterburg et al. 2014). This NVSCA registry system is based on craniofacial embryology and records the morphology and laterality of each affected anatomical structure of the primary and secondary palate. This system has been validated and applied successfully but discriminates only between complete, incomplete, and submucous or subcutaneous CLs (Rozendaal et al. 2011; Rozendaal, Luijsterburg, et al. 2012; Rozendaal, Mohangoo, et al. 2012; Rozendaal et al. 2013). However, a recurrent concern is the further morphological grading of incomplete CLs, which has been proposed by several authors (Harkins et al. 1962; Jensen et al. 1988; Smith et al. 1998; Ortiz-Posadas et al. 2001; Koul 2007; Liu et al. 2007; Wang et al. 2014). Vermeij-Keers et al. (in press) suggested after examining dentition patterns in adult unoperated Indonesian patients with (in)complete CL ± A that further morphological grading of incomplete CLs is clinically relevant. Based on this finding, we hypothesized that different deciduous and permanent tooth patterns may be associated with different grades (i.e., subphenotypes of the CL).
Therefore, our study aims at the question of whether distinction of CL subphenotypes is relevant for clinical practice and research by looking at the odontogenic origins of the maxillary lateral incisor in combination with the disturbed embryogenic processes leading to complete and incomplete CLs.
Hypotheses
In this study, 2 hypotheses are tested: 1) no differences exist among different CL subphenotypes in deciduous and permanent dentition patterns, and 2) no differences exist regarding dentition patterns between the NVSCA registry system of the complete and incomplete CL and a more detailed subdivision of CL into 4 subphenotypes according to Jensen et al. (1988).
Materials and Methods
This retrospective cohort study was approved by the medical ethics committee of the Erasmus University Medical Center Rotterdam, the Netherlands (MEC-2015-236).
Study Population
The subjects of the study were retrospectively recruited from the NVSCA registry, an anonymous case registry that is in accordance with the Dutch privacy law. All children with a nonsyndromic unilateral complete and incomplete CL ± A or CLAP, born between January 1, 1997, and December 31, 2005, and registered by the Dutch cleft palate teams of the Erasmus University Medical Center Rotterdam and the Radboud University Medical Center Nijmegen, were included in the study. In both teams, an orthodontist has thoroughly investigated each anatomical structure of the cleft and recorded the data. Because the NVSCA registry did not record information about imaging on the CL ± A and dentition patterns, the medical files of the children were manually assessed. Only children with a complete medical file and complete data on CL ± A morphology and deciduous and permanent dentition patterns were included (Fig. 1).
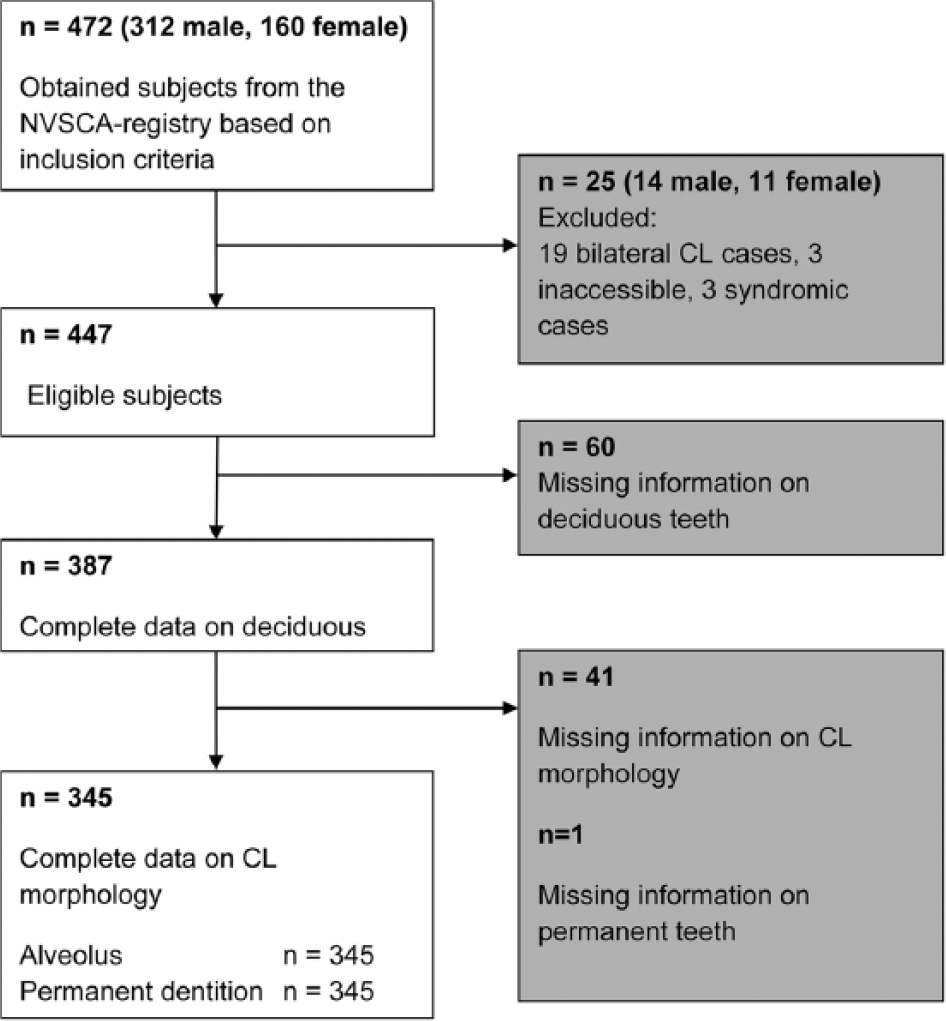
Flowchart of subject selection based on inclusion criteria. CL, cleft lip; NVSCA, Dutch Association for Cleft Palate and Craniofacial Anomalies.
Dentition Pattern and CL ± A Assessments
Preoperative photographs of the cases were used to determine the morphology of the CL. The CL was subdivided into 4 subphenotypes based on the vertical severity of the CL: 1) vermillion notch (including 8 subcutaneous clefts), 2) one-third to two-thirds CL, 3) two-thirds to subtotal CL, and 4) complete CL (Jensen et al. 1988). Preoperative photographs and dental casts of the cases were used to determine the morphology of the alveolar defect. Furthermore, a distinction was made between 4 of the different alveolar defects used in the NVSCA registry: 1) normal alveolus, 2) hypoplastic alveolus, 3) incomplete CA, and 4) complete CA. Due to sample size reasons, we regrouped the alveolar morphology for the statistical analysis into the following subphenotypes: 1) normal alveolus, 2) hypoplastic alveolus and incomplete CA, and 3) complete CA.
Information on dental anomalies in the cleft area was collected from the color photographs, dental casts, and panoramic radiographs of the patients for the deciduous dentition at a mean (SD) age of 5.5 (1.4) y and for the permanent dentition at a mean (SD) age of 9.1 (0.6) y before any alveolar repair (bone graft) was undertaken. Five different patterns of the deciduous lateral incisor were distinguished (i.e., 1 nondeviant and 4 deviant ones as described by Bøhn [1963] and Tsai et al. [1998]): the lateral incisor located in normal position (pattern z), the lateral incisor located in the anterior segment (pattern x) or located in the posterior segment of the cleft (pattern y), 1 lateral incisor in each segment of the cleft (pattern xy), and agenesis of the lateral incisor (pattern ab). These patterns of the permanent dentition are indicated with capital letters (Z, X, Y, XY, and AB; Fig. 2).
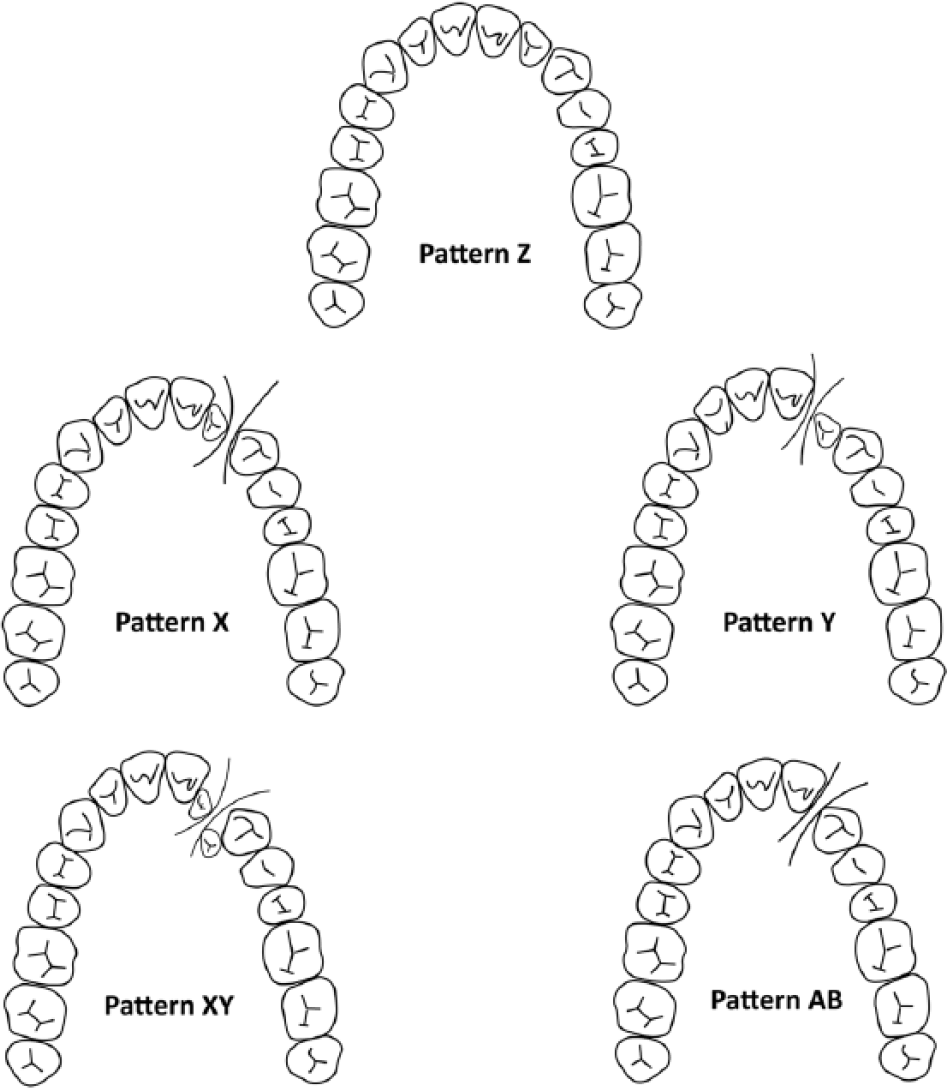
Five dentition patterns sorted by position of the permanent lateral incisor. Pattern Z: in normal position; pattern X: in anterior segment of the cleft; pattern Y: in posterior segment of the cleft; pattern XY: in both segments of the cleft; pattern AB: agenesis of the lateral incisor. Adapted from Tsai et al. (1998).
Primary and Secondary Palate Assessments
Information on the extent of the cleft in the primary and/or secondary palate was obtained from the NVSCA registry. In our analysis, the defects of the primary and secondary palates were grouped into 2 groups: 1) cleft only in the primary palate and 2) cleft in both the primary and secondary palate.
Statistical Analyses
All analyses were performed using Statistical Package of Social Sciences version 21.0 (SPSS, Inc.). Subject characteristics were evaluated among different CL subphenotypes with the χ2 test. Multinomial logistic regression models were used to estimate odds ratios (ORs) with 95% confidence intervals (CIs) for the association between CL morphology and deciduous or permanent dentition patterns. Three different models were built. First, the association between the CL subphenotypes and the occurrence of the different dentition patterns was investigated. Second, this association was adjusted for the alveolar defect, and third, it was also adjusted for a defect in the secondary palate. We adjusted for severity of the alveolar defect and the defect in the secondary palate because of their relation with both the cleft lip and the dentition pattern. Information about sex and the 2 clinics of data collection were included in all models.
In all analyses, the cases with complete CL and their dominant deciduous dentition pattern (pattern y) were used as the reference. To facilitate understanding of our findings in the permanent dentition pattern, the same reference group, pattern Y, was used. Finally, we tested all covariates for interaction with each other to evaluate whether the effect of the cleft lip on the dentition pattern was heterogeneous among sex, the 2 university clinics, alveolar defects, and palatal defects. However, interaction was not present.
Alternative Subdivisions of the CL
Histograms were constructed to inspect the distribution of the permanent dentition patterns and their precursory deciduous dentition patterns across the different CL subphenotypes according to the subdivision by Jensen et al. (1988) (Appendix Fig. 1). Based on the visual inspection of these histograms, 2 new subdivisions of the CL were made. The first alternative subdivision of the CL had 2 groups: 1) vermillion notch and one-third to two-thirds CL and 2) two-thirds to subtotal and complete CL. The second alternative subdivision of the CL had 3 groups: 1) vermillion notch and one-third to two-thirds CL, 2) two-thirds to subtotal CL, and 3) complete CL. The previously mentioned models were built again, using these alternative subdivisions as a determinant one by one, to evaluate their applicability.
Results
Patient Characteristics
In total, 345 subjects were available for the analysis (77.2% of those eligible to participate); 158 patients were from the Erasmus University Medical Center, Rotterdam, and 187 were from the Radboud University Medical Center, Nijmegen. The severity of the registered CL morphologies was different between the hospitals (P = 0.03). Of all subjects, 227 (65.8%) were male and 118 (34.2%) were female, but CL morphology was not statistically significantly different among sex. Of all subjects, 191 (55.4%) had a complete CA, 47 (13.6%) had an incomplete CA, 3 patients (0.9%) had a hypoplastic alveolus, and 104 (30.1%) had a normal alveolus. The alveolar defect was statistically significantly different among the CL morphologies (P < 0.001). Pattern z/Z only occurred in children with a vermillion notch (30.9%/32.3%) and children with a one-third to two-thirds CL (18.2%/23.6%). Therefore, the deciduous and permanent patterns z/Z were excluded from the regression analyses. Sample characteristics of the included patients are presented by the CL morphology in Table 1.
Sample Characteristics of Patients with Unilateral Cleft Lip (CL) with or without an Alveolar Defect.
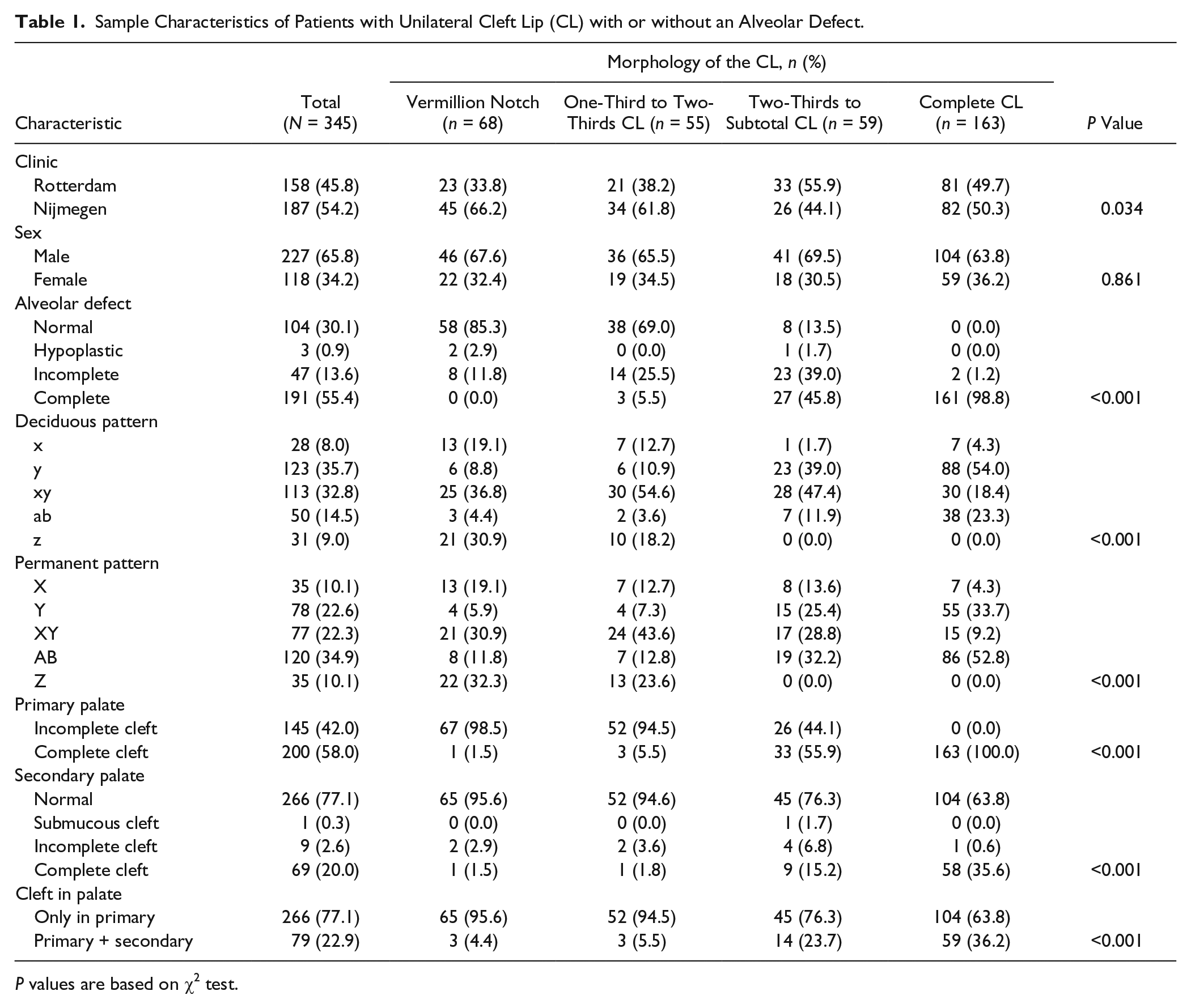
P values are based on χ2 test.
Deciduous Dentition
In Table 2, the results for the association between the CL morphology and the deciduous dentition are presented. Differences were found in the occurrence of deciduous dentition patterns among different CL subphenotypes. In particular, a vermillion notch and a one-third to two-thirds CL were statistically significantly associated with pattern x (OR = 28.91, P = 0.03; OR = 20.54, P = 0.03). A two-thirds to subtotal CL was associated with pattern xy, although without statistical significance, after adjustment for the severity of the alveolar defect and the severity of the defects of the alveolus and secondary palate, respectively (OR = 2.18, P = 0.09). The associations between CL morphology and deciduous dentition patterns was much weaker based on the subdivision used by Jensen et al. (1988) compared to the subdivision used in the NVSCA registry.
Associations of the CL Subphenotypes According to Jensen et al. (1988) and the NVSCA Registry with Different Patterns of the Lateral Incisor in the Deciduous Dentition of Children with Unilateral CL with or without an Alveolar Defect.
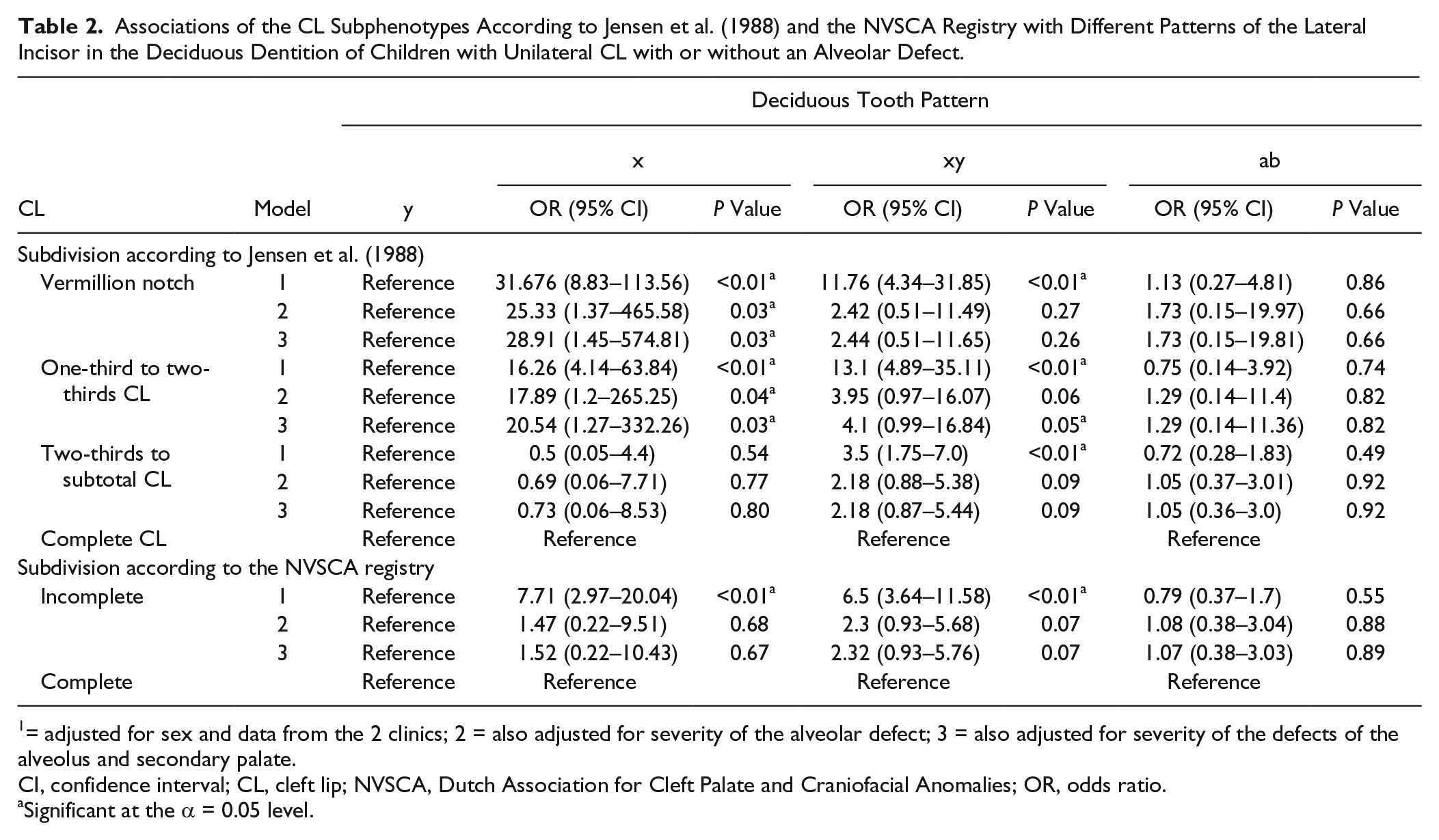
1 = adjusted for sex and data from the 2 clinics; 2 = also adjusted for severity of the alveolar defect; 3 = also adjusted for severity of the defects of the alveolus and secondary palate.
CI, confidence interval; CL, cleft lip; NVSCA, Dutch Association for Cleft Palate and Craniofacial Anomalies; OR, odds ratio.
Significant at the α = 0.05 level.
Permanent Dentition
In Table 3, the results for the association between the CL morphology and the permanent dentition are presented. On the first instance, a vermillion notch was statistically significantly associated with pattern X, and the one-third to two-thirds CL and two-thirds to subtotal CL were statistically significantly associated with pattern XY. However, this association changed after adjusting the analysis for the severity of the alveolar defect and the defects of the alveolus and the secondary palate. All associations after adjusting for the alveolus and secondary palate were not statistically significant, but a vermillion notch, one-third to two-thirds CL, and two-thirds to subtotal CL were all most likely associated with pattern X (OR = 6.72, P = 0.10; OR = 6.85, P = 0.08; OR = 3.99, P = 0.06). Thus, the associations between CL morphology and permanent dentition pattern did not differ between the subdivision used by Jensen et al. (1988) and the subdivision used in the NVSCA registry.
Associations of the CL Subphenotypes According to Jensen et al. (1988) and the NVSCA Registry with Different Patterns of the Lateral Incisor in the Permanent Dentition of Children with Unilateral CL with or without an Alveolar Defect.
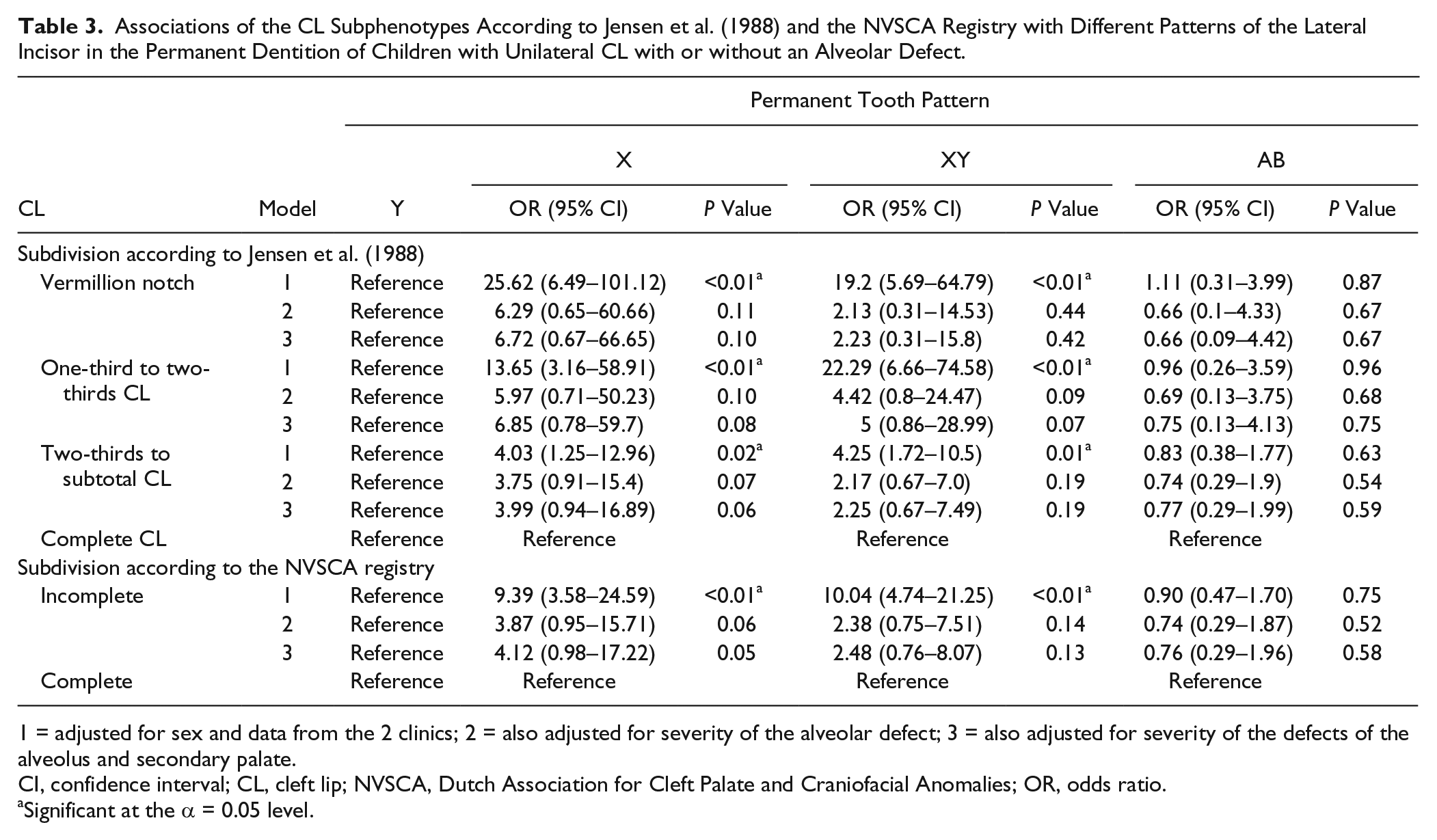
1 = adjusted for sex and data from the 2 clinics; 2 = also adjusted for severity of the alveolar defect; 3 = also adjusted for severity of the defects of the alveolus and secondary palate.
CI, confidence interval; CL, cleft lip; NVSCA, Dutch Association for Cleft Palate and Craniofacial Anomalies; OR, odds ratio.
Significant at the α = 0.05 level.
Alternative Subdivisions of the CL
Based on the histograms (Appendix Fig. 1), the subdivisions were reframed as described in the Materials and Methods section. Using the first alternative subdivision (vermillion notch to two-thirds CL vs. two-thirds CL to complete cleft), the association between certain deciduous dentition patterns related to the CL morphology were much weaker compared to the associations based on the subdivision by Jensen et al. (1988), hereby indicating a substantial loss of information. However, this was not the case when using the second alternative subdivision into 3 groups (vermillion notch to two-thirds CL vs. two-thirds to subtotal CL vs. complete CL). Here, the vermillion notch and one-third to two-thirds CL remained most likely related to deciduous pattern x, the two-thirds to subtotal CL remained most likely related to deciduous pattern xy, and complete CL remained most likely associated with pattern y (Appendix Table 1).
This finding appeared to be different for the permanent dentition. Looking at both alternative subdivisions, there was no change in likelihood to have a certain dentition pattern related to the cleft lip morphology compared to the likelihood based on the subdivision by Jensen et al. (1988) (Appendix Table 2).
Discussion
Interpretation of Main Findings
The present study shows that the different CL morphologies are associated with different deciduous and permanent dentition patterns. Therefore, our results suggest that pathogenesis of the CL and odontogenesis share some critical factors during embryogenesis.
This finding is consistent with literature suggesting that dental anomalies have the same etiological factors as the associated CL ± A (Bøhn 1963; Adams and Niswander 1967; Bhatia 1972; Tsai et al. 1998; Eerens et al. 2001; Letra et al. 2007; Thesleff 2014; Vermeij-Keers et al., in press). Moreover, critical factors can influence the fusion between the facial swellings (i.e., the medial nasal, maxillary, and lateral nasal swellings) that form the primary palate and after the fusion process, thus later during development, the primary palate differentiates into lip and alveolus (Luijsterburg et al. 2014). The medial nasal and maxillary swellings contain the presumptive odontogenic area, including the lateral incisor. In line with this, we found that patterns z/Z occurred only in children with a vermillion notch or one-third to two-thirds CL and normal alveolar morphology (Table 1). Thus, a small alteration in the late development of the lip can be followed by normal development and normal eruption of teeth. However, children born with a vermillion notch or one-third to two-thirds CL most likely had patterns x/XY. Thus, even mild anomalies of lip development are likely related to changes in tooth development. Finally, pattern ab/AB, considered the most severe dental pattern, will most likely coincide with complete clefts, which are also considered the most severe disturbance. This provides evidence that alterations in early development leading to a complete CL (i.e., during the fusion process) cause more severely disturbed odontogenesis, which is in line with earlier studies (Eerens et al. 2001; Lourenço Ribeiro et al. 2003; Aizenbud et al. 2005). Thus, based on our study, abnormal fusion between and differentiation of the medial nasal and maxillary processes causes abnormal formation of the dental lamina and will, depending on the severity, disturb development of the lateral incisor in terms of origin, shape, position, or time of eruption (Vermeij-Keers et al., in press).
We compared associations of different CL subdivisions with the occurrence of deciduous and permanent dentition patterns to see whether a more detailed subdivision of CL might be more informative for clinical and research purposes. We saw that the subdivision by Jensen et al. (1988) distinguished between more deciduous tooth patterns related to the different CL morphology than the subdivision used by the NVSCA registry. However, this effect was not visible in the permanent dentition corrected for the severity of the alveolar defects and for the defects of both the alveolus and secondary palate. Thus, more detailed subdivisions do not provide more information on permanent dentition patterns than the simple subdivision of the NVSCA registry. This finding shows us that the severity of the cleft (i.e., an alveolar defect or an additional defect of the secondary palate) is much more informative for the permanent dentition than for the deciduous dentition. Accordingly, we saw the relation between pattern z/Z and the normal alveolus, which also pointed to the importance of the alveolus in tooth development. Still, the deciduous dentition is strongly linked to the morphology of the CL, and therefore we recommend a more detailed subdivision of the CL than currently used in the NVSCA registry. However, when we tested the alternative subdivisions, we also showed that the very detailed subdivision based on Jensen et al. (1988) is not needed, but it seems rational to divide the CLs into vermillion notch to two-thirds CL, two-thirds to subtotal CL, and complete CL.
Methodological Considerations
In this study, 77.2% of those eligible patients were included in the final analyses. The remaining had to be excluded due to missing preoperative photographs, dental casts, radiographs, or missing patient files. To avoid misclassification, we also excluded patients for whom we could not confirm whether pattern AB was due to early loss or due to agenesis of the lateral incisor. Note that the permanent dentition was measured before the bone graft was performed. Generally, retrospective studies are prone to selection bias, because of exclusion of patients due to missing data. Selection bias occurs when the association of interest in included patients is different compared to excluded patients. However, we consider this unlikely for the present study. In the analysis, we adjusted for the effect of the alveolar and palatal clefts, but residual confounding might have occurred due to unknown factors (e.g., operation methods, pediatric or orthodontic treatment) related to dentition patterns. On the other hand, adjusting for the effect of the alveolar and palatal clefts might have led to an overadjustment of the model and subsequently to an underestimation of the true relationship between CL phenotypes and the different dentition patterns.
The strength of our study is the large sample size. We used clinical records of CL ± A and CLAP patients of 9 registry years from 2 large university hospitals in the Netherlands. Furthermore, our study sample again shows that regional differences exist in the distribution of CL ± A and CLAP patients in the Netherlands (Rozendaal, Mohangoo, et al. 2012). This sample included unilateral nonsyndromic cleft patients only to highlight the role of developmental and molecular mechanisms on facial morphogenesis and odontogenesis.
Finally, to our knowledge, this study is the first that considers statistically the occurrence of the cleft in the alveolus, palate, and both dentition patterns for the evaluation of different subdivisions of the CL morphology.
Relevance and Conclusion
Our study suggests a relation between the CL morphology and the different patterns in the deciduous and permanent dentition, respectively. Possibly, CL morphogenesis and odontogenesis share a genetic and molecular network. By examining the association between CL ± A and dentition patterns among children with unilateral nonsyndromic CL ± A and CLAP, this study provides further insights in the pathways underlying lip morphogenesis and odontogenesis.
In the Netherlands, the NVSCA registry currently distinguishes between complete, incomplete, and submucous CL based on craniofacial embryology (Luijsterburg et al. 2014). However, based on our study, we propose the use of a more detailed subdivision of incomplete CL for research purposes as it covers the phenotypic variability of the CL more comprehensively. This subdivision will improve the understanding and identification of the etiology of CL and alveolar defects. It enables investigating the relation between different CL subphenotypes with specific biological and genetic factors that are evident during specific time points in embryogenesis. For example, a more detailed subdivision of the CL morphology will improve research about the conjunction between CL phenotype and gene mapping highlighted by recent genetic studies (Stanier and Moore 2004; Menezes et al. 2009; Dixon et al. 2011; Leslie and Marazita 2013).
In addition, this subdivision will facilitate 1) the prediction of deciduous dentition patterns based on the morphology of the CL at birth and 2) the prediction of permanent dentition when taking into account the defects of the alveolus and secondary palate. Early identification of high-risk children for one of the dentition patterns is an important requirement for an efficient and informed decision making during the comprehensive treatment of CL patients. Further research is recommended to study the precise mechanisms behind the relationships between CL morphogenesis and odontogenesis.
In conclusion, the present research shows that differences exist among different CL subphenotypes in deciduous and permanent dentition patterns. Therefore, in contrast to conventional CL subdivisions, a more detailed subdivision of the CL is better related to the deciduous and permanent dentition. This indicates that critical factors in CL pathogenesis are similarly relevant in odontogenesis.
Author Contributions
B. Asllanaj, contributed to conception, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; L. Kragt, contributed to design, data analysis, and interpretation, drafted and critically revised the manuscript; I. Voshol, contributed to interpretation, critically revised the manuscript; M. Koudstaal, S.J. Bergé, contributed to data acquisition, critically revised the manuscript; M.A. Kuijpers, contributed to data acquisition and analysis, critically revised the manuscript; T. Xi, contributed to data analysis, critically revised the manuscript; C. Vermeij-Keers, E.M. Ongkosuwito, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors thank the members of the cleft palate teams from the Erasmus University Medical Center, Rotterdam and the Radboud University Medical Center, Nijmegen for the support in data acquisition.
A supplemental appendix to this article is available online.
The Department of Oral and Maxillofacial Surgery, Orthodontics and Special Dental Care, Erasmus Medical Center, Rotterdam, the Netherlands supported the study.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.