
Abstract
Much research on children’s oral health has focused on proximal determinants at the expense of distal (upstream) factors. Yet, such upstream factors—the so-called structural determinants of health—play a crucial role. Children’s lives, and in turn their health, are shaped by politics, economic forces, and social and public policies. The aim of this study was to examine the relationship between children’s clinical (number of decayed, missing, and filled teeth) and self-reported oral health (oral health–related quality of life) and 4 key structural determinants (governance, macroeconomic policy, public policy, and social policy) as outlined in the World Health Organization’s Commission for Social Determinants of Health framework. Secondary data analyses were carried out using subnational epidemiological samples of 8- to 15-y-olds in 11 countries (N = 6,648): Australia (372), New Zealand (three samples; 352, 202, 429), Brunei (423), Cambodia (423), Hong Kong (542), Malaysia (439), Thailand (261, 506), United Kingdom (88, 374), Germany (1498), Mexico (335), and Brazil (404). The results indicated that the type of political regime, amount of governance (e.g., rule of law, accountability), gross domestic product per capita, employment ratio, income inequality, type of welfare regime, human development index, government expenditure on health, and out-of-pocket (private) health expenditure by citizens were all associated with children’s oral health. The structural determinants accounted for between 5% and 21% of the variance in children’s oral health quality-of-life scores. These findings bring attention to the upstream or structural determinants as an understudied area but one that could reap huge rewards for public health dentistry research and the oral health inequalities policy agenda.
Introduction
The World Health Organization’s (2010) Commission for Social Determinants of Health (CSDH) posits the structural determinants of health as the social, economic, and political mechanisms that generate and maintain social stratifications that, in turn, determine individual socioeconomic positions according to income, education, occupation, sex, and race/ethnicity. These structural determinants include the labor market, educational system, political institutions, and so on that operate through socioeconomic positions and other intermediary factors (e.g., psychosocial circumstances, behavioral factors) to shape individuals’ exposure and vulnerability to health-compromising conditions. They are sometimes called macro, contextual, global, upstream, or distal factors, or “causes of the causes.”
Despite being viewed as central to explaining health inequalities, the structural determinants of oral health remain understudied. Instead, we have become “prisoners of the proximate” (Baker and Gibson 2014), with individual- or household-based risk factors dominating dental inequalities research. While important, such work ignores the social structure that shapes these risk factors (Link and Phelan 1995; Baker and Gibson 2014). Only attention on upstream political and economic priorities such as tax regulations, distribution mechanisms, social policies, and political ideologies will begin to address the question of “What puts people at risk of risks?” Such research could advance our policy making for addressing oral health inequalities (Watt et al. 2016).
While the wealth of a nation strongly determines its population health (Evans 2004), the distribution of this wealth also appears to play a role (Sen 1999; Wilkinson and Pickett 2009). This may be because governments invest less in key public policies or infrastructures that affect education, health, and social services that pattern health and well-being (Bambra et al. 2005; Raphael 2006). For instance, welfare state regimes reflect political systems and policies and determine health through the allocation and distribution of resources (Bambra 2011). Countries also differ in the liberties and civil and political rights, which determine population health (Beckfield and Krieger 2009; Muntaner 2013).
In the field of oral health, the methods and analytic tools to examine upstream determinants are still nascent (e.g., Do 2012). The one area in which some research has been carried out is on welfare state regimes (Sanders et al. 2009; Guarnizo-Herreno et al. 2013, 2014; Listl et al. 2014). Recently, Guarnizo-Herreno et al. (2017) found that a large proportion of differences in oral health between 31 European countries was attributable to the welfare state regime. More redistributive and universal welfare policy regimes (Scandinavian/social democratic) had better self-reported oral health than Eastern European regimes in particular.
However, the limitations of the welfare regime approach have been highlighted in the comparative social policy literature (Bambra 2011). Given this and the absence of research on other structural determinants in relation to oral health, the aim of the present study was to identify the association between all of the structural determinants outlined within the CSDH framework (governance, macroeconomic, public and social policy) and both clinical and subjective oral health outcomes. We studied children’s oral health for 2 reasons. First, structural determinants (e.g., country affluence, welfare regime, income inequality) have been shown to influence young people’s health (Holstein et al. 2009). Second, life course studies suggest that social inequalities in childhood and adolescence predict adult general and oral health (Power et al. 2007; Broadbent et al. 2016).
Method
Secondary analyses were conducted on data from 6,648 children using samples of 8- to 15-y-olds in Australia, New Zealand (3 samples), Brunei, Cambodia, Hong Kong, Malaysia, Thailand (2 samples), United Kingdom (2 samples), Germany, Mexico, and Brazil. Data sets were chosen pragmatically, based on availability. All but the Cambodian and 2 UK samples were representative at the national or regional level. The clinical outcome was the number of decayed, missing, and filled teeth (DMFT). Oral health–related quality of life was assessed with either the 37-item (Jokovic et al. 2002) or 16-item (Jokovic et al. 2006) Child Perceptions Questionnaire (CPQ). Methodological details of individual studies are in Appendix 1. Table 1 summarizes the national sociodemographic and oral health data.
Overview of Sociodemographic Characteristics and Oral Health across the 11 Countries.
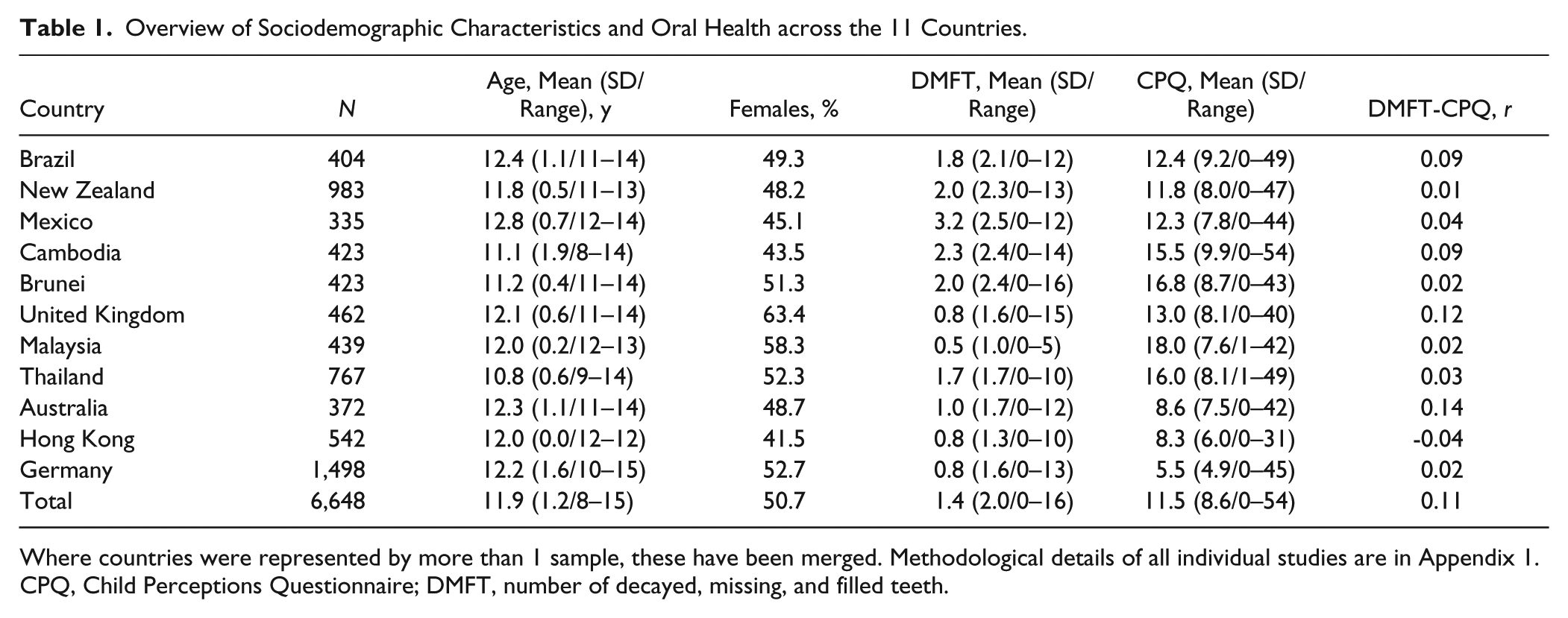
Where countries were represented by more than 1 sample, these have been merged. Methodological details of all individual studies are in Appendix 1.
CPQ, Child Perceptions Questionnaire; DMFT, number of decayed, missing, and filled teeth.
Structural Determinants
Full details of the determinants (governance, macroeconomic, public and social policy), including definitions, indicators, measurement, sources, and year of collection, are in Appendix 2. All indicators were chosen based on their extensive use in comparative social policy research. The fifth determinant in the CSDH—cultural and social values—was excluded, as it could not be operationalized with available data. As the first data collection occurred in 2002 (Appendix 1), all structural indicator data were obtained for 2000 to ensure temporal precedence between country-level determinants and outcomes (Table 2).
Overview of Structural Determinants and Their Indicators across Countries.
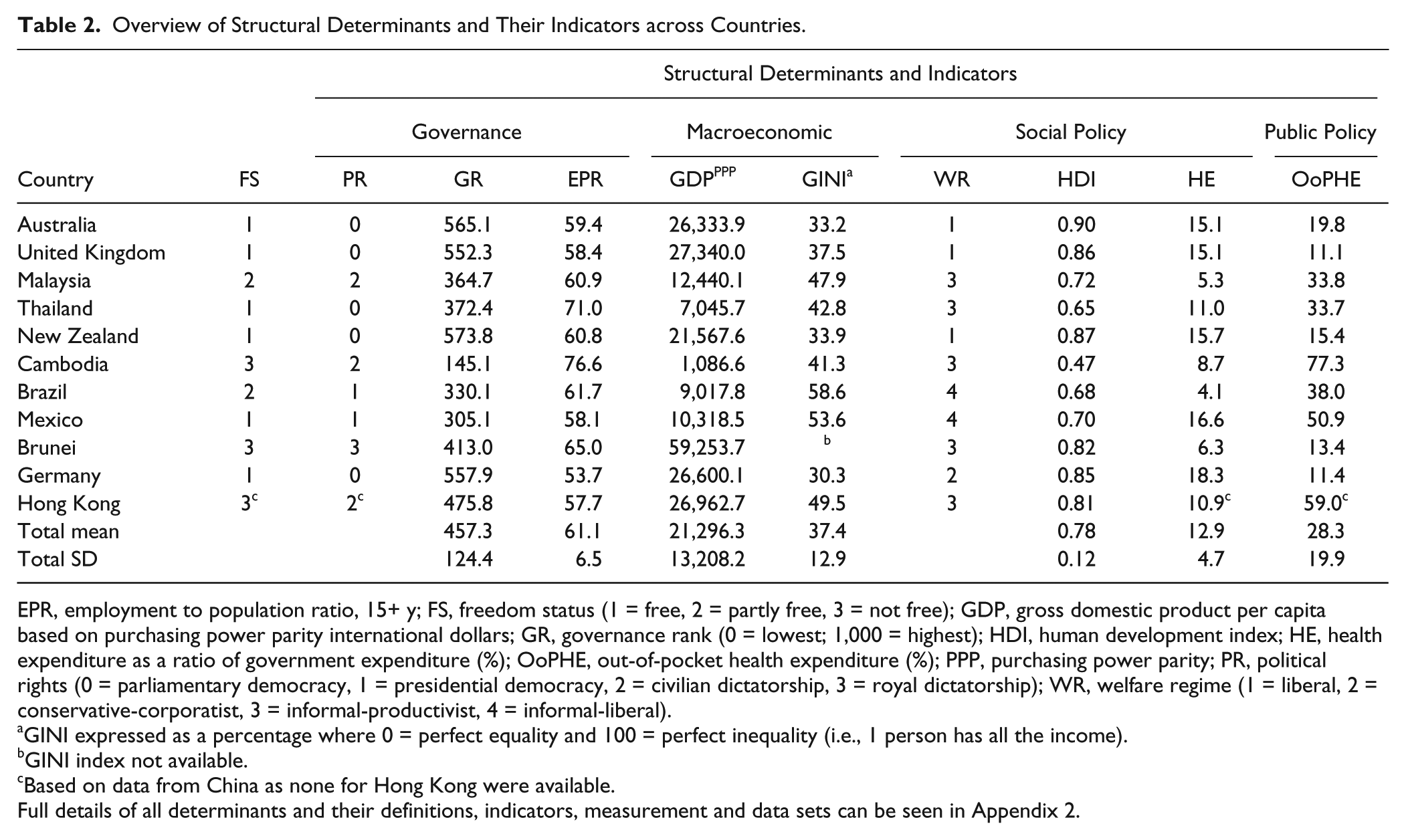
EPR, employment to population ratio, 15+ y; FS, freedom status (1 = free, 2 = partly free, 3 = not free); GDP, gross domestic product per capita based on purchasing power parity international dollars; GR, governance rank (0 = lowest; 1,000 = highest); HDI, human development index; HE, health expenditure as a ratio of government expenditure (%); OoPHE, out-of-pocket health expenditure (%); PPP, purchasing power parity; PR, political rights (0 = parliamentary democracy, 1 = presidential democracy, 2 = civilian dictatorship, 3 = royal dictatorship); WR, welfare regime (1 = liberal, 2 = conservative-corporatist, 3 = informal-productivist, 4 = informal-liberal).
GINI expressed as a percentage where 0 = perfect equality and 100 = perfect inequality (i.e., 1 person has all the income).
GINI index not available.
Based on data from China as none for Hong Kong were available.
Full details of all determinants and their definitions, indicators, measurement and data sets can be seen in Appendix 2.
Governance
These are traditions and institutions of authority within a country, including how governments are selected, monitored, and replaced and how effectively they formulate and implement policies. Three indicators were chosen: 1) freedom status, based on Freedom House (2000) ratings. Each country’s “freedom status” is determined from free (<1.0 to 2.5), partly free (3.0 to 5.0), to not free (5.5 to 7.0). 2) Political regime, based on Cheibub and colleagues’ (2010) typology of democracy and dictatorship (0 = parliamentary democracy, 1 = presidential democracy, 2 = civilian dictatorship, 3 = royal dictatorship). 3) Governance, based on the Worldwide Governance Indicators Project (2000). Each country is ranked on 6 dimensions (e.g., Voice and Accountability, Political Stability, Rule of Law) from 0 (lowest) to 1,000 (highest) (Kaufman et al. 2010).
Macroeconomic Policy
Macroeconomic policy involves government regulations around fiscal, monetary, balance of payments, and trade policies. Three indicators were chosen from the World Bank (2000): 1) employment to population ratio for those 15+ y, expressed as a total percentage based on International Labour Organisation estimates. 2) Gross domestic product per capita based on purchasing power parity (PPP) measured in international dollars. This reflects the average standard of living per household, controlling for differences in cost of living across countries. 3) GINI index measures the degree of inequality in distribution of family income within a country as a percentage and ranges from 0 (no inequality—all have the same income) to 100 (maximum inequality).
Social Policy
Social policy involves the role of the state in the protection and promotion of the economic and social well-being of citizens through education, health, housing, welfare, and taxation. Two indicators were used: (1) welfare state, measured using an expanded version of Esping-Andersen’s typology to include low-income and non–Organisation for Economic Co-operation and Development (OECD) countries (Wood and Gough 2006). Each country was classified on 4 welfare types: 1 = welfare state regime—liberal, 2 = welfare state regime—conservative-corporatist, 3 = informal-security regime—productivist, and 4 = informal-security regime—liberal informal. 2) Human development index (HDI), the geometric mean of normalized indices on 3 dimensions: health (life expectancy at birth), education (mean years of schooling for adults, 25+ y), and standard of living (gross national income per capita) transformed to a scale from 0 (lowest) to 1 (highest).
Public Policy
This is the spending on systems (rather than system’s performance) in areas such as health and education. Two indicators were used from the World Bank (2000): 1) health expenditure as a ratio of government expenditure and 2) out-of-pocket health expenditure (percentage of total expenditure on health). This is any direct outlay by households, including gratuities and in-kind payments relating to health. It is part of private health expenditure.
Data Analysis
The data set combined both individual child-level outcomes (DMFT, CPQ) and country-level indicators. We used a fixed-effects analytic approach rather than conventional multilevel models for 3 reasons (Mohring, 2012): 1) country selection was not random as would be required for multilevel (random-effects) models, 2) its applicability for a small number of countries (level 2 units), and 3) its control of country-level heterogeneity (i.e., influential outliers) through the use of dummy variables. Negative binomial count models were employed for DMFT as the data were skewed. For CPQ, ordinary least squares regression models were used. Cluster robust standard errors corrected for the clustered data (by country). Given that linearity could not be assumed, continuous country-level indicators (gross domestic product [GDP], health expenditure, etc.) were categorized into 3 groups (low, medium, high) based on a tertile split (see Table 2 for variable categorizations). All analyses were carried out using R (R Core Development Team, Version 3.4.2).
Results
As seen in Table 1, the mean DMFT was 1.4, ranging from 0.4 (Malaysia) to 3.2 (Mexico) (range, 0 to 16; median = 1). The self-reported mean CPQ score was 11.5, ranging from 5.5 (Germany) to 17.9 (Malaysia). While there was a weak positive correlation between CPQ and DMFT scores overall (r = 0.12), the association varied considerably across countries.
Governance
Freedom status was not associated with either outcome measure (see Table 3). Political regime and governance were associated with CPQ scores. Children in countries with a royal dictatorship (Brunei) had more oral health–related quality of life (OHRQoL) impacts (greater by 6.6 CPQ points, P < .001) than those with parliamentary democracies (e.g., Australia, Table 3). Children in both civilian dictatorships (CPQ + 3.4) and presidential democracies (CPQ + 2.2) also had more OHRQoL impacts than parliamentary democracies, but these differences were not significant. Children living in countries with royal dictatorships (+0.4) or presidential democracies (+0.6) had greater DMFT scores than those in parliamentary democracies, (P = 0.06). Children in countries with the highest governance (e.g., accountability, rule of law) (e.g., Germany) had fewer OHRQoL impacts (by 6.6 CPQ points, P < .05) than those with the lowest governance (e.g., Cambodia). A similar pattern was seen for DMFT, but this was not significant. Political regime and governance accounted for 5% and 12% of the variance in CPQ scores, respectively.
Fixed-Effects Model Estimates and 95% CIs for the Association Between Each Structural Determinant Indicator and Clinical (DMFT) and Oral Health Quality of Life (CPQ) Outcomes.
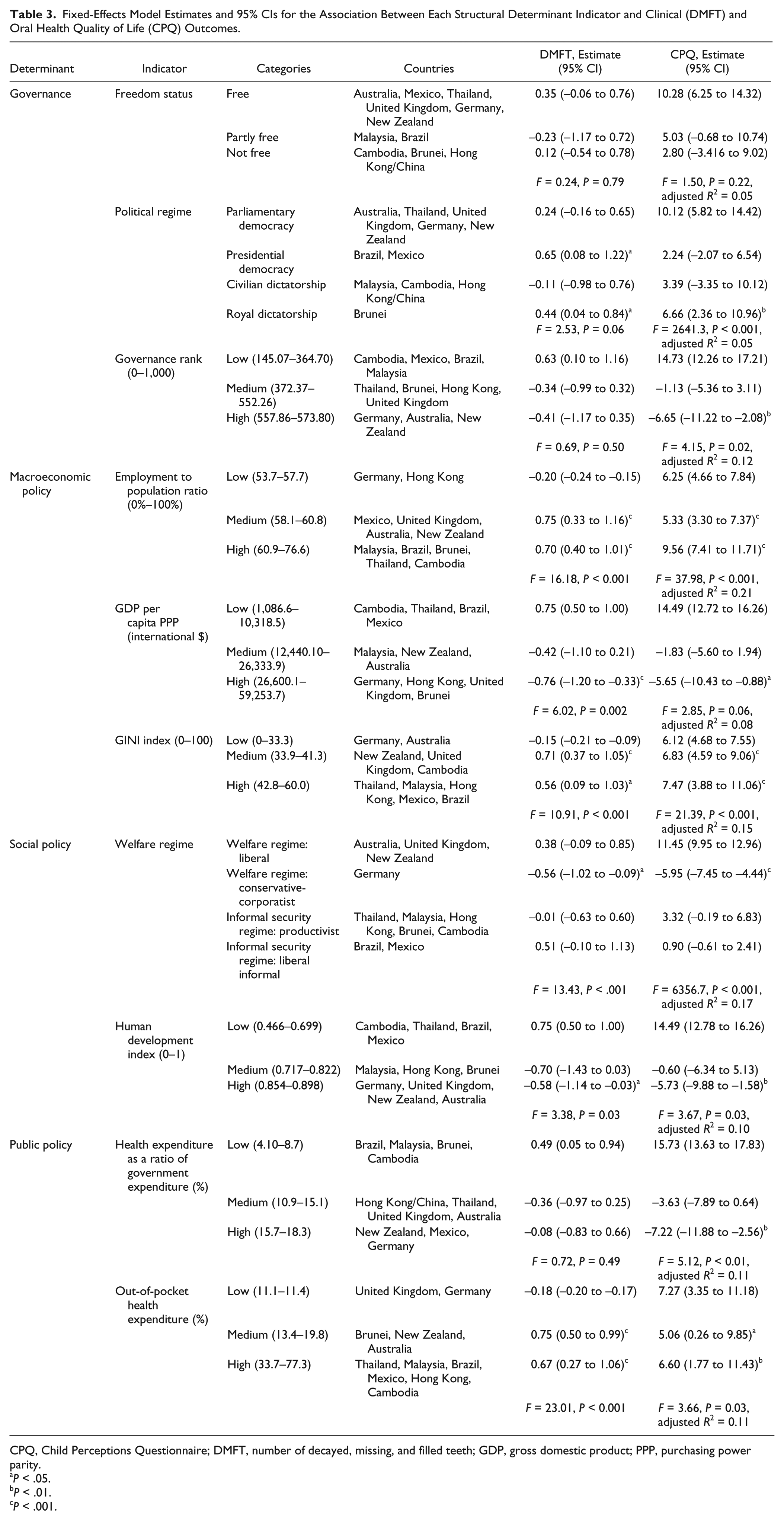
CPQ, Child Perceptions Questionnaire; DMFT, number of decayed, missing, and filled teeth; GDP, gross domestic product; PPP, purchasing power parity.
P < .05.
P < .01.
P < .001.
Macroeconomic Policy
Children in countries with high GDP per capita (e.g., Germany) had significantly lower DMFT (by 0.7) and CPQ scores (by 5.6) than in low GDP countries (e.g., Cambodia, Thailand) (P = 0.06). Countries with medium and higher employment ratios had greater DMFT (by 0.7, 0.7) and CPQ (by 5.3, 9.5) than low ratio countries (Germany). For the third indicator—GINI index—both DMFT and CPQ models were significant (P < .001). In those countries with medium (≥33.9) and high GINI scores (≥42.8), children had greater DMFT (0.7, 0.5) and CPQ (6.8, 7.4) compared to those with a low GINI index (≤33.2) (Germany, Australia). Employment, GDP, and the GINI index accounted for 21%, 8%, and 15% of the variance in CPQ scores, respectively.
Social Policy
Welfare regime and the HDI were related to both outcomes (Table 3). DMFT and CPQ scores were significantly lower (by 0.5, 5.9) in a conservative-corporatist (Germany) than a liberal welfare system (e.g., United Kingdom, New Zealand). The 2 informal security regimes did not differ significantly from the liberal welfare regime. Children in countries with a high HDI score (e.g., Germany) had lower DMFT and CPQ scores (by 0.5, 5.7) than those with a low HDI (e.g., Cambodia, Thailand). Welfare regime and HDI accounted for 17% and 10% of the variance in CPQ scores, respectively.
Public Policy
Countries with a higher health expenditure as a ratio of government expenditure (e.g., New Zealand) had significantly lower CPQ scores (by 7.2 points) (i.e., better OHRQoL) than those with lower health expenditure (e.g., Brazil). Government health expenditure was not significant for DMFT (Table 3). Children in countries with high (e.g., Thailand, Mexico) and medium out-of-pocket expenditure (e.g., Brunei) had greater CPQ scores (by 6.5, 5.0 points) and DMFT (by 0.6, 0.7) than countries with low expenditure (United Kingdom, Germany). Health and out-of-pocket expenditure both accounted for 11% of the variance in CPQ scores.
Discussion
Summary of Findings
Measures of democracy and quality of governance were strongly associated with children’s oral health impacts, with less consistent associations for the clinical measure, DMFT. Macroeconomic measures of employment, per capita GDP and income inequality, and social policy measures (welfare regime, human development) had strong and consistent associations with both children’s caries experience and self-reported impacts. Both outcome measures were strongly associated with private, out-of-pocket health expenditure, while public health expenditure was associated with subjective impacts only. These structural determinants accounted for between 5% (political regime) and 21% (employment ratio) of the variance in children’s OHRQoL scores.
Interpretation
Our findings are in line with previous comparative research on structural (upstream) determinants in health. Much of this research centers on welfare regimes where those with more generous, universal and redistributive policies (i.e., social democratic/Scandinavian) have better population health than less redistributive regimes with means-tested services (i.e., Anglo-Saxon). Studies of oral health support these findings (e.g., Guarnizo-Herreno et al. 2017). The present study did not include any countries with social democratic welfare regimes, but we found that a conservative-corporatist regime (Germany), which is less committed to redistributive policies than a social democratic regime but still has generous social payments, had a better caries experience and self-reported oral health than liberal regimes (e.g., United Kingdom). These findings are consistent with infant mortality data (e.g., Conley and Springer 2001).
One explanation may be that the impact of welfare regime on young people’s health is mediated by income inequalities; countries with higher redistributive characteristics have smaller inequalities in health (Bambra 2011). Indeed, welfare state regimes are strongly linked to health inequalities, accounting for up to 50% of the variation (Muntaner et al. 2011). While we examined only the direct effect of structural determinants, countries with greater income inequality had greater children’s caries experience and oral health impacts. This pattern was also seen for the other measure of social policy, the HDI.
Oral health was associated not just with social policy indicators and income equality but also with measures of economic resources, such as per capita GDP. Such resources are key to improved population health at a national level (e.g., Patterson and Veenstra 2016) through better welfare, higher standard of living via better wages (Firebaugh and Beck 1994), or “trickling down” through intermediary factors such as education (Jenkins and Scanlan 2001). In addition, the national distribution of economic resources is important. With high income inequality, economic growth may be less effective in improving health (Clark 2011). We found that greater per capita GDP, welfare generosity, education and income (through the HDI), and lower income inequality were independently associated with better oral health.
Linked to a country’s welfare regime are its public policies—namely, spending on education and health. Greater government spending on health care and less private, out-of-pocket health expenditure were strongly associated with better oral health. Both of these findings support studies on infant mortality (Conley and Springer 2001). Others have linked greater out-of-pocket health costs to lower service use and greater health inequalities (e.g., Van Doorslaer and Koolman 2004). Mackenbach and McKee (2015), in their study of 30 European countries between 1990 and 2010, found national health policy was strongly associated with its democracy and quality of governance. Similarly, we found that in countries where quality of governance was higher, children had better self-reported oral health.
Like Mackenbach and McKee (2015), we found that the democratic regime within a country was important. Children in countries with the least democratic processes (i.e., royal dictatorships) had worse OHRQoL and greater caries experience than in parliamentary democracies. Although there has been far less research into the role of democratic governance in health, electoral democracies experience 62.5% lower infant mortality (Patterson and Veenstra 2016) and more public investment in health care (Liang and Mirelman 2014). Democracies may be better at encouraging income growth or more equal distribution of income, both of which were positively associated with children’s oral health. However, we examined only direct effects. While we have begun to address the first question (does politics matter?), what is needed is to address the next 2 questions: what specific political conditions matter and under what circumstances? For example, is it economic resources (e.g., GDP per capita), welfare generosity, governance quality (e.g., participation), or income inequality that account for better oral health in more democratic countries than in less democratic countries or dictatorships?
Strengths and Limitations
This is the first attempt at understanding the influence of multiple structural determinants on oral health, rather than focusing on just one indicator (e.g., welfare regime type) for one key determinant (i.e., social policy). We grounded our study on a theoretical framework (World Health Organization 2010) and we used both clinical and self-reported oral health measures. Many comparative studies include only self-reports (e.g., tooth loss, OHRQoL) because they are dependent on secondary analysis of existing data sets (e.g., Eurobarometer). The problem with such measures in comparative studies is the risk of cultural differences in reporting of health. Participants in different countries may have different reference levels for reporting health or perceptions of response categories (Jurges 2007). In our study, children in Germany reported lower OHRQoL (CPQ = 5.5) than other countries. Is this because German children have better oral health or are more likely to report better oral health than in, for example, Malaysia (18.0)? The former would not be supported by our data; Malaysian children had slightly lower mean DMFT (0.5) than German children (0.8). Thus, future oral health comparative research needs to include clinical measures, alongside self-reports. This is particularly important when, as seen here, there are not strong associations between person-reported (e.g., child rated) and clinical measures. Finally, unlike most comparative health research, our study did not only rely on secondary data from European countries. Instead, we built a data platform, collating primary data sets from an international community across 11 European, Australasian, and East and South East Asian countries comprising over 6,000 children.
Despite these strengths, our study is incomplete. Only aggregated DMFT scores were available, rather than the disaggregated “D” component, which may have had an effect on estimates of caries experience. While indicators of the structural determinants were collected as near as possible to the date of primary data collection, there was variation in when primary studies occurred. Such variation may have influenced the findings given that a country’s governance structures and public and social policies are not static over time. For some structural determinant indicators, categories were represented by only 1 or 2 countries but compared to categories represented by many countries (e.g., freedom status). Finally, structural determinants were examined for their direct effects on child oral health and thus treated essentially as an independent factor. We must now examine how these factors are interrelated and the role of intermediary determinants (e.g., psychosocial characteristics) in a way more in line with complex systems approaches (e.g., Baker and Gibson 2014). This will develop our understanding of how structural determinants become embodied (Beckfield and Krieger 2009) to identify how social structures “get into the mouth” and generate oral health (Baker and Gibson 2014).
Conclusion
This is the first study to consider politics and social and public policy in relation to oral health, and it offers a promising heuristic for future work. The findings suggest that strategies to reduce risk by changing downstream factors—such as toothbrushing—will be ineffective on their own at a population level because such personal policy changes, based on the study of risk factors at the level of the individual, are too narrow. While oral health problems are experienced individually, they are public and political in nature. Mainstream oral epidemiology needs to move from viewing the social context as a problem of confounding to be disentangled in order to achieve objectivity. As we move further upstream, the more uncertain we are in making causal inferences, yet this cannot be a reason for not examining these “fundamental causes.” This will entail a transdisciplinary approach incorporating the theories from sociology, economics, and politics into oral epidemiology using mechanism-centered methods that can identify context-mechanism-outcome patterns and establish causal links for meaningful oral health improvement.
Author Contributions
S.R. Baker, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; L. Foster-Page, contributed to conception, design, data acquisition and interpretation, critically revised the manuscript; W.M. Thomson, contributed to conception, design, and data interpretation, critically revised the manuscript; T. Broomhead, contributed to data analysis and interpretation, critically revised the manuscript; K. Bekes, P.E. Benson, F. Aguilar-Diaz, L. Do, C. Hirsch, Z. Marshman, C. McGrath, R. Mohamed, P.G. Robinson, J. Traebert, B. Turton, contributed to data acquisition, critically revised the manuscript; B.J. Gibson, contributed to conception and design, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_0022034518767401 – Supplemental material for Structural Determinants and Children’s Oral Health: A Cross-National Study
Supplemental material, DS_10.1177_0022034518767401 for Structural Determinants and Children’s Oral Health: A Cross-National Study by S.R. Baker, L. Foster Page, W.M. Thomson, T. Broomhead, K. Bekes, P.E. Benson, F. Aguilar-Diaz, L. Do, C. Hirsch, Z. Marshman, C. McGrath, A. Mohamed, P.G. Robinson, J. Traebert, B. Turton, and B.J. Gibson in Journal of Dental Research
Footnotes
Acknowledgements
We thank the participants and the various funding bodies for their support for the primary data collection.
A supplemental appendix to this article is available online.
Full details of funding for individual studies are contained in Appendix 1.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.