
Abstract
The oral cavity is usually the first part of a consumer’s body exposed to the constituents of tobacco products or their emissions. Consequently, the oral cavity is a frequent site for carcinogenic, microbial, immunologic, and clinical effects of tobacco use. This article summarizes 5 presentations on various aspects of oral health affected by combusted or noncombusted tobacco products from a recent conference, “Oral Health Effects of Tobacco Products: Science and Regulatory Policy,” sponsored by the American Association for Dental Research and the Food and Drug Administration.
The oral cavity is usually the first part of a tobacco user’s body exposed to the constituents of tobacco products or their emissions. Consequently, the oral cavity is a frequent site for carcinogenic, microbial, immunologic, and clinical effects of tobacco use. For example, smoking has been established as a major cause of chronic periodontitis (US Department of Health and Human Services 2004), responsible for an estimated one-half of cases in the United States (Tomar and Asma 2000). Tobacco smoke is a major risk factor for cancers of the oral cavity and pharynx (International Agency for Research on Cancer 2004; US Department of Health and Human Services 2014).
Supported by a grant from the US Food and Drug Administration, the American Association for Dental Research convened a 1-d conference in Bethesda, Maryland, on September 14, 2018, entitled “Oral Health Effects of Tobacco Products: Science and Regulatory Policy.” That conference was not intended to provide a comprehensive review on tobacco and oral health but was meant to highlight emerging science on the topic, particularly in areas of potential relevance for tobacco product regulation. This article summarizes 5 presentations on various aspects of oral health affected by combusted or noncombusted tobacco products. The presentations summarized in this article and their presenters are as follows: Chemical Carcinogenesis of Combusted Tobacco Product Ingredients (Stephen S. Hecht); Effect of Combustible Tobacco Products and E-cigarettes on Mucosal Immunity (Ilona Jaspers); Smokeless Tobacco Products: Oral Health Effects, Flavor, and Regulatory Implications (Scott L. Tomar); Effect of Nicotine on Streptococcus mutans (Richard L. Gregory); and Smokeless Tobacco Constituents: Carcinogenicity and Variations across Products (Irina Stepanov).
Chemical Carcinogenesis of Combusted Tobacco Product Ingredients
Epidemiologic studies have conclusively shown that tobacco smoking causes cancers of the lung, oral cavity, nasopharynx, oropharynx, hypopharynx, nasal cavity, accessory sinuses, larynx, esophagus, stomach, pancreas, colorectum, liver, kidney, ureter, urinary bladder, uterine cervix, and ovary (mucinous), as well as myeloid leukemia (International Agency for Research on Cancer 2012). Figure 1 summarizes the accepted overall mechanism by which cigarette smoking causes cancer (US Department of Health and Human Services 2014). People start smoking, usually as teenagers, and become addicted to nicotine. Nicotine is not a carcinogen, but cigarette and other combusted tobacco products are dangerous nicotine delivery devices because each puff also delivers a mixture of >7,000 chemicals, of which at least 70 are established carcinogens (Hecht 2012). This complex mixture also contains tumor promoters, co-carcinogens, and various toxicants that exacerbate the effects of the carcinogens. There may also be carcinogens that have not yet been fully characterized.

Accepted overall mechanism by which cigarette smoking causes cancer.
The human body has drug-metabolizing enzymes, such as cytochromes P450 and glutathione-S-transferases, that catalyze the detoxification of many of these cigarette smoke chemicals. However, some of these catalyzed reactions result in reactive intermediates with electrophilic properties. Epoxides are a good example of this type of intermediate. These electrophilic intermediates can react with DNA to produce DNA addition products, commonly referred to as DNA adducts. DNA adducts are critical in the carcinogenic process because if they persist unrepaired, they can cause miscoding during DNA replication, resulting in a permanent change in the DNA sequence because the wrong base has been inserted opposite the DNA adduct. If this mutation occurs in a critical gene, such as the KRAS oncogene, the TP53 tumor suppressor gene, or other genes, the result can be loss of normal growth control processes, genomic instability, and development of cancer. There are also detoxification mechanisms, DNA repair pathways, and apoptosis that are protective (US Department of Health and Human Services 2014). The balance between the mutagenic and protective pathways can influence the outcome, which is important to consider in view of the fact that most smokers will not get cancer. For example, only 11% to 24% of lifetime cigarette smokers will get lung cancer by age 85 y and not because they die from other smoking-related diseases (International Agency for Research on Cancer 2004).
With respect to oral cavity cancer, the most important carcinogens in cigarette smoke are N′-nitrosonornicotine (NNN) and polycyclic aromatic hydrocarbons (PAHs). NNN is one of the “tobacco-specific nitrosamines,” carcinogens derived from tobacco alkaloids. NNN and the other tobacco-specific nitrosamines are present in all tobacco products. They form during the curing and processing of tobacco and are typically present in parts per million quantities in tobacco, which is far higher than the levels of carcinogenic nitrosamines in any other consumer product designed for human oral consumption (Hecht 1998; International Agency for Research on Cancer 2007). Current levels of NNN in mainstream cigarette smoke average 85 ± 31 ng/cigarette, based on analysis of 50 brands of cigarettes sold in the United States (Edwards et al. 2017). NNN readily induces tumors of the oral cavity and esophagus in rats. Treatment of F-344 rats with 14 ppm of (S)-NNN, the predominant isomer present in tobacco products, in the drinking water for 70 wk caused a 100% incidence of oral cavity tumors. A total of 68 oral cavity tumors were observed upon necropsy of 20 (S)-NNN-treated rats. Tumors were observed in the buccal mucosa, soft palate, pharynx, and tongue of these rats. All of the rats also had esophageal tumors, which have been commonly observed in all studies of NNN carcinogenicity in rats (Balbo et al 2013). NNN also induces tumors of the respiratory tract in mice, hamsters, and mink (International Agency for Research on Cancer 2007). PAHs compose a large group of compounds formed in the incomplete combustion of organic matter, including tobacco. The smoke of all tobacco products contains PAHs, many of which are carcinogenic at the site of contact (International Agency for Research on Cancer 2010). Two PAHs that have received considerable attention with respect to oral cavity cancer are benzo(a)pyrene and dibenzo(a,l)pyrene, although the concentrations of these compounds in tobacco smoke (0.1 to 14 ng/cigarette) are considerably lower than those of NNN (El-Bayoumy et al. 2017).
It is important to be able to monitor human exposure to carcinogens in tobacco smoke because there can be great variation in carcinogen dose depending on not only their concentrations in cigarette smoke but on the ways in which people smoke and the amounts that they smoke. While cigarettes per day and years of smoking have been widely used for this purpose, these measures are somewhat crude and can be nonobjective. Measurement of urinary carcinogen and toxicant metabolites can now be used to assess an individual’s exposure to tobacco smoke constituents (Hecht et al. 2010). One of the most reliable measurements is urinary “total nicotine equivalents,” which comprises at least 85% of the nicotine dose. These nicotine metabolites—such as cotinine and 3′-hydroxycotinine and their glucuronides—can now be reliably quantitated with high-performance liquid chromatography–mass spectrometry techniques. The list of urinary biomarkers that is now available also includes measurements of carcinogen metabolites derived from tobacco-specific nitrosamines and PAHs, as well as volatile tobacco smoke toxicants such as acrolein, butadiene, and benzene (Hecht et al. 2010). Current research focuses on the use of these and related biomarkers, such as DNA adducts, to identify those smokers who are at high risk for cancer so that intensive preventive and early detection measures can be initiated.
Effect of Combustible Tobacco Products and E-cigarettes on Mucosal Immunity
In the oral and respiratory mucosa, the first line of defense is composed of several cell types that all play critical roles in defending against pathogens and toxicants. For example, epithelial cells in the respiratory mucosa not only provide a physical barrier protecting the underlying tissue but also protect mechanically against inhaled particulates and pathogens via the mucociliary escalator, which is designed to trap and remove particles out of the lung. Epithelial cells also secrete cytokines/chemokines and express ligands/receptors, thus orchestrating the overall host defense response. Resident and recruited immune cells, such as neutrophils, lymphocytes, and monocytes/macrophages, patrol the airway mucosa and help phagocytize or neutralize inhaled pathogens or particles. Together, these mucosal cell types mount an integrated and collaborative defense response aimed at protecting us against any perturbation caused by inhaled pathogens or toxicants, which would otherwise cause harm. Inhaled toxicants, such as tobacco smoke, mount a multipronged attack on the respiratory mucosa, thus causing adverse health effects. In epithelial cells, tobacco smoke exposure reduces barrier function, increases mucus production, modifies cytokine/chemokine production, alters receptor/ligand expression, and adversely affects the mucociliary escalator (Jaspers 2014). Similarly, smoking reduces phagocytic activities of neutrophils and macrophages, increases inflammation, and adversely affects lymphocyte function (Jaspers 2014). Together, these effects are the underlying pathophysiology of the many manifestations of smoking-related diseases.
While the effects of conventional cigarette smoking on mucosal immune responses have been examined for many years, less is known about any potential effects of the use of e-cigarettes or vaping on these responses. Considering that >20% of high school students are vaping (Cullen et al. 2018), potential short- and long-term effects on the respiratory mucosa need to be examined. One study demonstrated that the airway epithelium of otherwise healthy vapers showed signs of irritation and markers of inflammation (Ghosh et al. 2018). Similarly, Martin et al. (2016) demonstrated that the nasal mucosa of healthy vapers (i.e., individuals with no signs of respiratory disease) showed markers of an overall suppressed immune status. One recent study demonstrated that the proteomic profile of induced sputum in those individuals showed markers of enhanced inflammation and neutrophil activation (Reidel et al. 2018). Together, these studies strongly suggest that vaping causes proinflammatory yet immune-suppressive changes in the respiratory mucosa and that these effects are different from those seen in smokers.
Similar to cigarette smoke, e-cigarette aerosols contain many chemicals. In addition to nicotine, these include thermal degradation products of the e-liquid base compounds propylene glycol and vegetable glycerin, such as acrolein, formaldehyde, and acetaldehyde (Sleiman et al. 2016; Salamanca et al. 2017), which are known respiratory toxicants. In addition, many flavoring chemicals are added in numerous mixtures to e-cigarettes. Although several of these chemicals are known or suspected respiratory irritants, their toxicity to the respiratory tract is largely unknown. Among these flavoring chemicals is cinnamaldehyde, which is the chemical that gives cinnamon its characteristic flavor. Several in vitro studies have demonstrated that cinnamaldehyde can be cytotoxic in many different cell types (Behar et al. 2014; Behar et al. 2016). Clapp et al. (2017) recently demonstrated that cinnamaldehyde significantly suppresses the function of key respiratory mucosal immune cells. Specifically, cinnamaldehyde suppresses the phagocytic function of neutrophils and macrophages and inhibits the tumor cell–killing ability of natural killer cells. These inhibitory responses were caused by concentrations of cinnamaldehyde that are present in commercially available flavored e-liquids. A separate study showed that cinnamaldehyde or cinnamaldehyde-containing e-liquids also inhibit ciliary beating of airway epithelial cells, a key function of the mucociliary escalator (Clapp et al. 2019). These effects were not affected by the presence or absence of nicotine, indicating that flavoring chemicals exert adverse effects on the respiratory mucosa independent of nicotine. Cinnamaldehyde causes a significant suppression of cellular bioenergetics in epithelial cells and immune cells, thus shutting down the cell’s ability to generate energy (e.g., ATP) to support energy-demanding functions, such as phagocytosis or ciliary beating. Whether the ability to suppress cellular bioenergetics is unique to cinnamaldehyde or also caused by other popular flavoring chemicals contained in e-liquids, such as vanillin or benzaldehyde, or whether these biological effects are further enhanced by reaction of these chemicals with other components of e-cigarette aerosols, such as formation of acetals (Erythropel et al. 2019), needs to be further examined. In summary, these studies demonstrate that flavoring chemicals contained in e-cigarettes can block key functions of various components of the respiratory mucosal cells, likely resulting in impaired respiratory host defense functions.
Smokeless Tobacco Products: Oral Health Effects, Flavor, and Regulatory Implications
Unlike smoked tobacco—which is burned or heated and then inhaled in products such as cigarettes, cigars, pipes, or hookahs—smokeless tobacco (ST) is a broad category of noncombusted tobacco products that are used orally or, much less commonly, inhaled nasally. There is a wide variety of ST products used throughout the world, including commercially manufactured products and handmade cottage industry or individually prepared products (National Cancer Institute and Centers for Disease Control and Prevention 2014). The common feature among these products is the absorption of nicotine and other chemicals across mucous membranes.
The majority of ST products sold and used in the United States are commercially manufactured products that fall into 1 of 5 categories: moist snuff, loose-leaf chewing tobacco, plug or twist chewing tobacco, snus, and Scotch or dry snuff. Moist snuff, an orally used product, is by far the leading ST category in the United States, with 2016 US sales of $3.55 billion and 1.5 billion units, accounting for 89% of total ST sales (Federal Trade Commission 2018). Unit sales of moist snuff increased every year between 2002 and 2016, growing by 69% during that period. In contrast, sales of all other categories—except snus—declined between 2002 and 2016. Snus, which is a Swedish-style oral snuff product, was introduced to the US market in 2006 and saw a gradual increase in sales until 2010, after which sales have been relatively flat. By unit sales, snus accounted for just 3% of the US ST market. Advertising and promotional expenditures by ST manufacturers largely mirrored product sales, with expenditures for moist snuff rising from $209.3 million in 2002 to $678.7 million in 2016, while advertising and promotional spending remained flat or fell for all other ST categories (Federal Trade Commission 2018). As of 2017, nearly the entire US ST market was controlled by 3 manufacturers: Altria (46.3% market share), Reynolds American (34.4%), and Swedish Match (11.9%; Euromonitor International Ltd 2018).
Expert panels have concluded that use of ST products is a cause of cancer in humans, particularly cancers of the oral cavity and pharynx (International Agency for Research on Cancer 2007; US Department of Health and Human Services 1986), although the magnitude of risk appears to vary by product and country (Greer 2011). Other adverse oral health effects include keratosis of oral mucosa and localized gingival recession (Warnakulasuriya et al. 2010; Greer 2011). Chewing tobacco use may increase the risk for root surface caries (Tomar and Winn 1999), and 1 cross-sectional study suggested an association between ST use and severe periodontitis (Fisher et al. 2005). Several cross-sectional studies found a higher prevalence of dental attrition or abrasion among ST users than among nonusers (Ekfeldt 1989; Robertson et al. 1997), perhaps due to the relatively large quantity of abrasive mineral content found in some brands of ST products (Dahl et al. 1989; Bowles et al. 1995).
ST use in the United States has long been most prevalent among adolescent and young adult males (Tomar et al. 2010). The prevalence of past 30-d use of ST among male high schools seniors was declining for more than decade, from a high of 23.6% in 1995 to 11.0% in 2006 (Johnston et al. 2018). The prevalence of ST use then increased for several years, reaching 15.8% in 2009, during the period in which Reynolds American and Altria largely took over the market and invested in new products and promotions (Tomar et al. 2010). The prevalence of past 30-d use has since been gradually declining and was estimated at 9.9% in 2017, not much lower than the prevalence of smoking (10.6%). The emerging pattern of ST use in recent years is one of dual use: nearly 40% of male high school students and 15% of adult males who used ST daily were also current smokers (Tomar et al. 2010).
Flavored products account for nearly 60% of the US ST market (Delnevo et al. 2014). In 2011, wintergreen was the most common flavor, with a 39% market share, followed by spearmint and other mint flavors, at 12%. Flavorings may play a major role in the initiation of moist snuff use by young people, with flavored products representing a majority of first-used products (Oliver et al. 2013; Corey et al. 2015; Villanti et al. 2017). Analysis of internal tobacco industry documents indicates that ST manufacturers have been using flavorings explicitly to attract young consumers for many years (Kostygina and Ling 2016). The tobacco industry has long researched the effects of sugar and flavorings on the sensory properties, nicotine bioavailability, and addiction potential of ST products. In particular, wintergreen flavor is associated with the perceived “strength” of ST products. In addition, wintergreen oil contains methyl salicylate, an organic compound with local anesthetic properties that may help mask the mucosal irritation associated with snuff dipping. Although flavorings appear to play a major role in the marketing, initiation, and addiction potential of smokeless products, the Food and Drug Administration currently has no regulations, including product standards, regarding flavors in moist snuff or other ST products.
Effect of Nicotine on Streptococcus mutans
The relationship between dental caries and Streptococcus mutans is known to involve the formation of oral biofilm (Huang and Gregory 2011). Current and former smokers experience a higher incidence of caries (Johnson and Bain 2000; Aguilar-Zinser et al. 2008; Avsar et al. 2008; Campus et al. 2011; Belstrøm et al. 2014; Hanioka et al. 2014; Edman et al. 2016). S. mutans involvement in oral biofilm requires 2 processes: sucrose-independent and sucrose-dependent attachment, both of which are enhanced in the presence of nicotine (Huang and Gregory 2015). In sucrose-independent attachment, S. mutans uses adhesins, such as cell wall–associated antigen I/II. This antigen is highly conserved among oral viridans streptococci, and to date, reports indicate that only 1 gene (spaP) encoding for antigen I/II is expressed by all strains of S. mutans. Receptors for antigen I/II include glycosylated salivary agglutinin glycoprotein (SAG) electrostatically attached to hydroxyapatite in tooth enamel. Antigen I/II interacts with SAG when it becomes immobile on a surface such as enamel. The solid phase of SAG that is adsorbed onto the dental hard tissue is what allows for initial adhesion of S. mutans. In the sucrose-dependent attachment process, S. mutans converts sucrose into glucan, utilizing glucosyltransferases (GTFs), and further uses glucan to attach to the tooth surface with GTFs and other glucan-binding proteins (Gpbs). S. mutans produces 3 GTFs (GTFB, GTFC, and GTFD) that contain both glucan-binding and catalytic domains and are important for sucrose-dependent attachment. Other than GTFs, Gbps are important in sucrose-dependent attachment. S. mutans produces 4 Gbps: GbpsA, GbpsB, GbpsC, and GbpsD.
The process of dental caries development is multifactorial. Smoking tobacco is one of the factors affecting the spread of dental caries lesions. Smoking 1 cigarette exposes the oral cavity to approximately 1 mg of nicotine (Allam et al. 2011), and recent studies in Dr. Gregory’s laboratory investigated nicotine’s effects on S. mutans. It was found that nicotine increases biofilm formation and metabolic activity of aerobic-grown S. mutans at concentrations of 2 to 8 mg/mL (Huang and Gregory 2012). The viability and metabolic activity of the bacterium also increases and is dependent on the nicotine concentration. That laboratory demonstrated that extracellular polysaccharide, primarily composed of insoluble glucan, increases with increasing nicotine concentration. Antigen I/II, GTF, and GbpsA are all upregulated by as little as 0.25 mg/mL of nicotine (Huang and Gregory 2015). In addition to upregulating virulence-related receptor proteins and extracellular polysaccharide, nicotine at 1 to 4 mg/mL increases glycolytic pathway intermediates, including lactic acid (Li et al. 2016). These increased virulence factors of S. mutans may be responsible for the increased cariogenicity of S. mutans in experimental rats fed 1 mg/mL of nicotine (Liu et al. 2018). Several reports indicate the destructive oral and systemic effects of smoking and nicotine exposure, leading to development or exacerbation of dental caries and heart diseases such as atherosclerosis (Wagenknecht et al. 2018). Additionally, nicotine upregulates collagen, fibronectin, fibrinogen, and laminin-binding proteins on the surface of S. mutans, which may facilitate the attachment of the bacterium to endothelial cell surfaces initiating atherosclerosis (unpublished data). Furthermore, S. mutans isolates from smokers produced significantly more biofilm than isolates from nonsmokers, indicating that an increased tolerance may be acquired by isolates from smokers (unpublished data). Because S. mutans typically grows deep in oral biofilm, the oxygen tension is typically low. Anaerobically grown S. mutans was demonstrated to produce significantly more biofilm than aerobically grown bacteria (Fig. 2). Anaerobic incubation of S. mutans significantly increases biofilm formation with and without nicotine. But nicotine in a range of 1 to 8 mg/mL significantly increases biofilm formation as compared with the 0 nicotine control. Collectively, these results may indicate the importance of nicotine in the virulence of S. mutans in the caries and atherosclerosis processes.
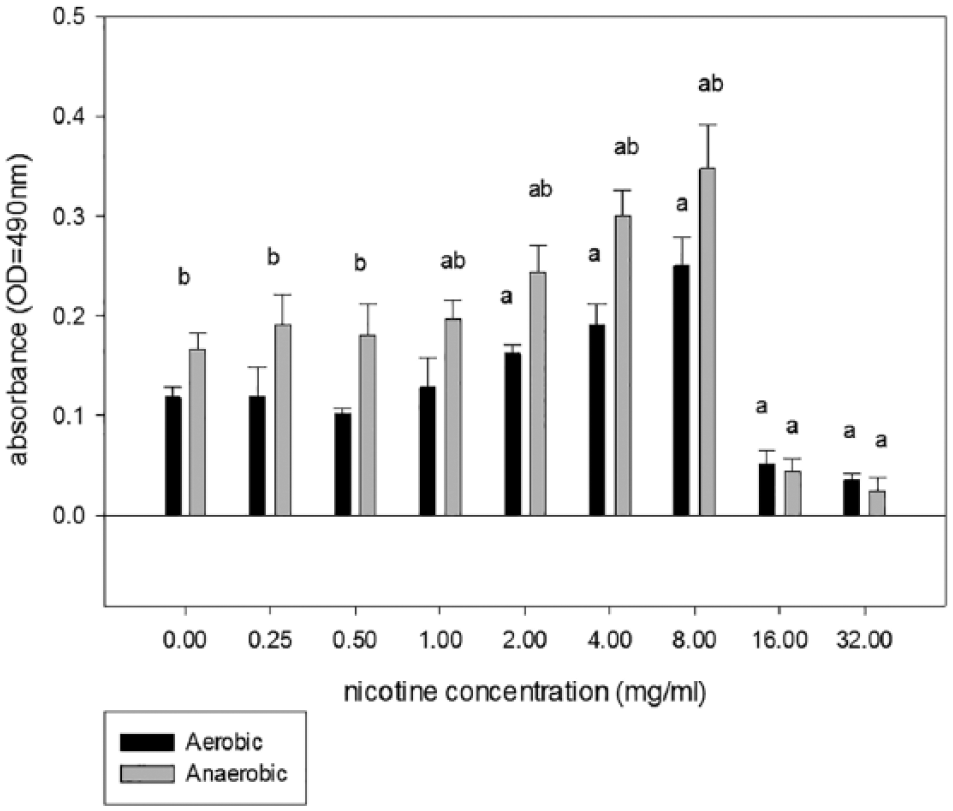
Comparison of aerobic and anaerobic incubation on nicotine-treated Streptococcus mutans biofilm formation. A crystal violet biofilm staining assay (Huang and Gregory 2012) was used to measure the mass of the S. mutans biofilm incubated with different concentrations of nicotine in 96-well microtiter plates. The plates were incubated at 37°C anaerobically or aerobically in 5% CO2. An “a” above the bar indicates a significant difference between the nicotine sample and the 0 nicotine control. A “b” indicates a significant difference between the aerobic and anaerobic samples for that particular nicotine concentration. An “ab” indicates significance for both comparisons. Values are presented as mean absorbance (490 nm) ± SEM
Smokeless Tobacco Constituents: Carcinogenicity and Variations across Products
The chemical composition of ST products is a critical contributing factor in the negative health effects associated with ST use (Stepanov and Hatsukami 2016). Nicotine is the major known addictive agent in tobacco, and its biological availability is defined by how much of its total content is present in the unprotonated form (Tomar and Henningfield 1997). In ST products, the unprotonated nicotine content is highly influenced by even slight variations in the product pH. For example, recent analyses of 79 varieties of US moist snuff products in Dr. Stepanov’s laboratory (unpublished data) showed that while the levels of total nicotine varied only approximately 2-fold, there was >1,000-fold variation in unprotonated nicotine content in the same products (Table). Such a wide range of unprotonated nicotine content may facilitate consumers’ transition to using products with increasingly higher nicotine levels and becoming highly addicted users. Indeed, use of ST products can result in the same degree of nicotine dependence as that observed in cigarette smokers, and >60% of ST users who quit eventually relapse to ST use (Hatsukami et al. 2004). Thus, while nicotine is not carcinogenic or toxic to the oral cavity, its levels in ST products drive users’ continuous exposure to other harmful tobacco chemicals.
Representative Variations of Harmful Constituents in US Smokeless Products.
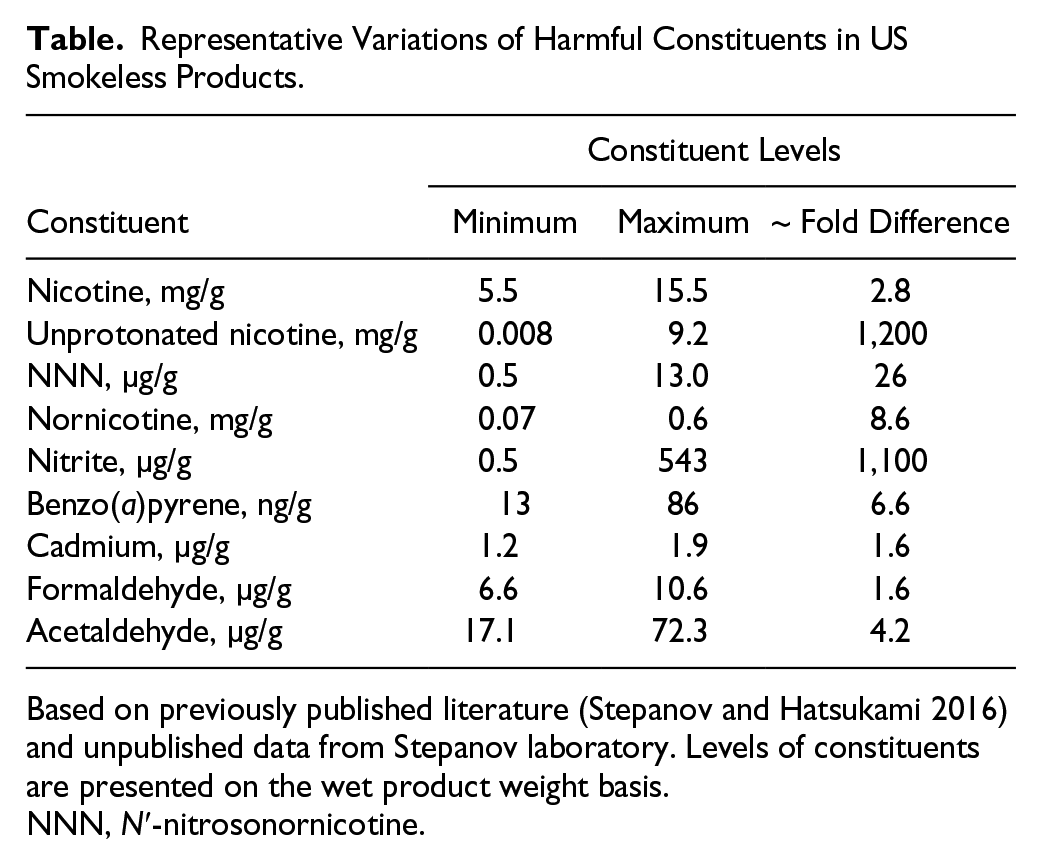
Based on previously published literature (Stepanov and Hatsukami 2016) and unpublished data from Stepanov laboratory. Levels of constituents are presented on the wet product weight basis.
NNN, N′-nitrosonornicotine.
There is a wide range of toxicants and carcinogens in ST products, such as the tobacco-specific nitrosamine NNN and other N-nitroso compounds, PAHs, metals and metalloids, and aldehydes. The levels of these constituents also vary substantially across products depending on a variety of factors, including tobacco type and manufacturing methods (Stepanov and Hatsukami 2016). For example, levels of NNN ranged approximately 25-fold across the 79 moist snuff varieties (Table). Formation of NNN occurs during the processing of tobacco via the nitrosation reaction of the minor tobacco alkaloid nornicotine with nitrite (Stepanov and Hatsukami 2016); however, such a reaction can also occur during the storage of the finished product (Djordjevic et al. 1993) and in the oral cavity of the user (Knezevich et al. 2012). Therefore, levels of these precursors in a ST product also contribute to its carcinogenic potency. In the same varieties of moist snuff, levels of nornicotine and nitrite ranged 9-fold and >1,000-fold, respectively (Table). Such dramatic variations in NNN and its precursors are highly significant because NNN is a potent carcinogen that targets the oral cavity and esophagus—organs most strongly associated with ST carcinogenesis (International Agency for Research on Cancer 2007). Furthermore, a biomarker-based prospective epidemiologic study showed that the level of NNN intake is prospectively and independently associated with the risk of esophageal cancer in humans (Yuan et al. 2011), and this is likely to be true for oral cancer.
The wide variation in the levels of these and other harmful constituents in ST products has direct implications for users’ exposures, as demonstrated in a study that employed urinary biomarkers (Hatsukami et al. 2015). In that study, 359 ST users of brands varying in levels of NNN and the related carcinogenic tobacco-specific nitrosamine NNK were recruited from 3 regions in the United States. Analyses of urine samples collected from these individuals showed that, independent of the pattern of product use and nicotine content, levels of NNN and NNK in ST products were strongly correlated with the corresponding urinary biomarker levels.
Taken together, these data provide strong support for the regulation of toxic and carcinogenic constituents in ST products. Establishing standards for such constituents in ST will eliminate unnecessary variations in their levels across products and reduce exposures in users of these products, which is likely to reduce the risk of oral cancer and other diseases associated with ST use. The US Food and Drug Administration issued an advance notice of proposed rule making in 2017 to limit NNN in finished ST products (Food and Drug Administration 2017).
Summary
Using combusted or ST products exposes consumers to high levels of carcinogens, and they are established causes of human cancer. In addition, tobacco smoke impairs mucosal immunity, which underlies the pathophysiology of many smoking-related diseases. Flavoring appears to play a major role in the initiation and continued use of ST products, particularly moist snuff. Levels of tobacco carcinogens and toxicants are highly variable among the ST products on the US market. Nicotine, the alkaloid primarily responsible for addiction to combusted or ST products, appears to increase the metabolic activity ofS. mutans and the rate of cariogenic biofilm formation. We need further research to better understand the role of various tobacco constituents in the pathogenesis of oral diseases and product usage and to inform the development of evidence-based tobacco product standards and regulations.
Author Contributions
S.L. Tomar, S.S. Hecht, I. Jaspers, R.L. Gregory, I. Stepanov, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
The conference and publication of this issue was supported by a grant from the Food and Drug Administration (1R13FD006142). Views expressed in written materials or publications and by speakers and moderators do not necessarily reflect the official policies of the US Department of Health and Human Services, nor does any mention of trade names, commercial practices, or organizations imply endorsement by the US government.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.