
Abstract
The purpose of this study was to develop a diagnostic tool to automatically detect temporomandibular joint osteoarthritis (TMJOA) from cone beam computed tomography (CBCT) images with artificial intelligence. CBCT images of patients diagnosed with temporomandibular disorder were included for image preparation. Single-shot detection, an object detection model, was trained with 3,514 sagittal CBCT images of the temporomandibular joint that showed signs of osseous changes in the mandibular condyle. The region of interest (condylar head) was defined and classified into 2 categories—indeterminate for TMJOA and TMJOA—according to image analysis criteria for the diagnosis of temporomandibular disorder. The model was tested with 2 sets of 300 images in total. The average accuracy, precision, recall, and F1 score over the 2 test sets were 0.86, 0.85, 0.84, and 0.84, respectively. Automated detection of TMJOA from sagittal CBCT images is possible by using a deep neural networks model. It may be used to support clinicians with diagnosis and decision making for treatments of TMJOA.
Keywords
Introduction
Temporomandibular joint osteoarthritis (TMJOA) is a subtype of temporomandibular joint disorder (TMD) and is characterized by pain, crepitus, masticatory dysfunction, and dentofacial deformity (Mercuri 2008; Krisjane et al. 2012; Wang et al. 2015). The prevalence of TMJOA is reported as 5% to 12% worldwide (National Institute of Dental and Craniofacial Research 2018), and it increases to 43% among patients with skeletal malocclusion (Krisjane et al. 2012). In South Korea, the number of outpatients diagnosed with TMD has increased by 25.7% over the last 5 y, and the national health insurance costs for TMD treatment has grown 60.6%, thus increasing the economic burden (National Health Insurance Service 2018).
TMJOA can be associated with other arthritic conditions, such as hand osteoarthritis (Abrahamsson et al. 2017), generalized osteoarthritis (Gynther et al. 1996), rheumatoid arthritis (Koh et al. 1999), and juvenile idiopathic arthritis (Arvidsson et al. 2009; Keller et al. 2015). Thus, accurate TMJOA diagnosis can be challenging during the early stages of the disease. As signs and symptoms have weak correlations to TMJOA, clinical examinations do not often provide accurate diagnosis (Keller et al. 2015).
Medical imaging modalities are crucial to accurate TMJOA diagnosis. Computed tomography (CT) has been the gold standard for diagnosing osseous changes of the temporomandibular joint (TMJ) because the integrity of the cortical bone lining and the underlying bony structure of the condyle can be observed (Ahmad et al. 2009; Schiffman et al. 2010). Additionally, cone beam CT (CBCT) has a lower radiation dose but has diagnostic accuracy similar to conventional CT (Honda et al. 2006; Hintze et al. 2007).
Applications of artificial intelligence (AI; e.g., deep neural networks) in medical and dental image analysis have rapidly grown. Computer-aided detection systems have also been developed, such as automatic polyp detection in colonoscopy videos (Tajbakhsh et al. 2015), detection of tumors in CT images (Koley et al. 2016), and dental caries detection on radiographs (Choi et al. 2018). However, there is a paucity of studies on TMD imaging diagnosis with AI, even though automatic classification of 3-dimensional (3D) condylar shapes and their associations with biomarkers in patients with TMJOA have been reported (de Dumast et al. 2018). There has been no study on the automatic detection of TMJOA. Therefore, the purpose of this study was to develop a diagnostic tool to detect condylar resorption from CBCT images with AI.
Materials and Methods
This study was approved by the institutional review board of Korea University Anam Hospital (2019AN0213). The CBCT images of 314 patients who were diagnosed with TMD and showed signs of TMJOA on CBCT were included (84 males, 230 females; mean ± SD age, 39.5 ± 18.2 y; range, 16 to 84 y). The CBCT images of right and left TMJs that showed osseous changes were included. For patients who had >1 CBCT scan, only the initial scan was included for training the AI model. CBCT was obtained with 3D eXam (KaVo Dental GmbH) with the following parameters: field of view, 17 × 23 cm; 120 kV and 5 mAs; voxel size, 0.3 mm; pulsed scan time, 17.8 s.
The AI model for disease detection used in this study requires training of the images of target lesions; thus, only CBCT images of patients showing signs of TMJOA were included for training. As a result, for the images of normal TMJ, the AI model would not detect any irregularities, thereby concluding the final diagnosis as normal. Three dentists (H.J.K., N.J., Y.J.K.) prepared the images of TMJOA. The sagittal images of the TMJ were inspected, and all that showed signs of TMJOA (Hatcher 2013), such as irregular contour, osseous defects, loss of cortication, and flattening of the condylar head, were captured and saved as JPG files via ITK-SNAP software (v. 3.6.0; Yushkevich et al. 2006); images showing a smooth and rounded outline of the condyle with no subchondral defects were considered normal and were excluded. Four to 10 images per TMJ were selected, and a total of 3,749 images showing signs of osseous changes in the condyles were obtained. After the images were resized to 300 × 300 pixels, the region of interest—the condylar head—was identified inside a rectangle and converted to XY coordinates with ImageJ software (v. 1.52k; National Institutes of Health). Then, an orthodontist with 10 y of clinical experience (Y.J.K.) reviewed and classified the TMJ images into 3 categories, according to image analysis criteria for the diagnosis of temporomandibular disorder (research diagnostic criteria for TMD [Ahmad et al. 2009]; diagnostic criteria for TMD [Schiffman et al. 2014]): no TMJOA, indeterminate for TMJOA, and TMJOA. TMJOA is diagnosed when condylar deformation is present due to subcortical cysts, surface erosions, generalized sclerosis, or osteophytes; condylar flattening and sclerosis are considered indeterminate finding for TMJOA (Schiffman et al. 2014). From the prepared 3,749 images, 235 that had mild morphologic variations but showed well-corticated articular surfaces with no signs of flattening or sclerosis were diagnosed as normal. Therefore, they were excluded from the training data, as the detection model only requires training of images with signs of osseous changes. Among the 3,514 images, 1,700 were diagnosed as indeterminate for TMJOA (class 1), and 1,814 were diagnosed as TMJOA (class 2).
A single-shot detector (SSD)—a deep learning framework designed for object detection (Liu et al. 2016)—was trained with the 3,514 images and tested with 2 sets of 300 images. Each test set included 150 images: 50 cases of normal TMJ and 50 cases of class 1 (control group, n = 100) and 50 cases of class 2 (TMJOA group, n = 50). Half of the 3,514 images were used for building the model, and the other half were used for validating the model. We considered this process of model building and validation to be a “training process,” and we repeated the training process 10,700 times (10,700 epochs) to improve the model. The 2 test sets with 300 images total were completely separate from the training process and were used for testing the model. Also, images from the same patient were allocated to only 1 of the 3 data sets: training, validation, or test set. Two orthodontists (U.B.B., Y.J.K.) with 28 and 10 y of clinical experience, respectively, and a TMJ specialist (W.K.) with 25 y of clinical experience diagnosed the TMJ images in the test data sets. The learning rate of the model was 1.0 × 10−5 during the first 450 epochs and 1.0 × 10−4 during the last 10,250. SSD discretizes the output space of predicted boxes into a set of default boxes over different ratios and scales per featured map location. SSD does not require the stages of proposal generation and feature resampling (Faster R-CNN, another detection model, requires this). For this reason, SSD is considered to be faster than Faster R-CNN and to show comparable performance at the same time (Liu et al. 2016).
Accuracy, precision, recall, and F1 score are the performance measures of the model. Accuracy is defined as the ratio of correct predictions among the 150 cases. Precision is the ratio of true positives to true positives and false positives. Recall is the ratio of true positives to true positives and false negatives. For example, precision represents the ratio of true TMJ disorders among predicted ones, whereas recall represents the ratio of predicted TMJ disorders among true ones. Finally, the F1 score is a harmonic mean of precision and recall: (2 × precision × recall) / (precision + recall). These measures were calculated for the intersection-over-union (IOU) threshold of 0.50. The IOU is defined as the ratio of the intersection (overlap) over the union of predicted and true boxes in an image (Everingham et al. 2010). For instance, if the IOU threshold is set to 0.50, only predicted boxes with IOUs ≥0.50 will be presented. A value of 0.50 was adopted as the IOU threshold in the 2010 PASCAL Visual Object Classes Challenge, a prominent international competition of object classification, detection, and segmentation (Everingham et al. 2010). We followed this convention, setting the IOU threshold at 0.50. The Python programming language (v. 3.52) and a graphics card (GeForce GTX 1080 Ti D5X 11 GB) were used for the analysis.
Results
After 10,700 training epochs, the validation loss of the model decreased from 114.87 to 0.83 (Fig. 1). Table 1 shows the confusion matrix of the model, which compares the predicted classes against the true classes for 150 images in each of test sets 1 and 2. The accuracy, precision, recall, and F1 score of the model are shown in Table 2. These values were derived from Table 1, which represents the confusion matrix of the model. The average accuracy over the 2 test sets was 0.86. The average precision over the 2 test sets was 0.80 for TMJOA, 0.89 for the control, and 0.85 for the average of the 2 groups. The average recall over the 2 test sets was 0.77 for TMJOA, 0.90 for the control, and 0.84 for the average of the 2 groups. Similarly, the average F1 score over the 2 test sets was 0.78 for TMJOA, 0.89 for the control, and 0.84 for the average of the 2 groups. Examples of correctly classified cases of classes 1 and 2 are presented in Figures 2 and 3, respectively.
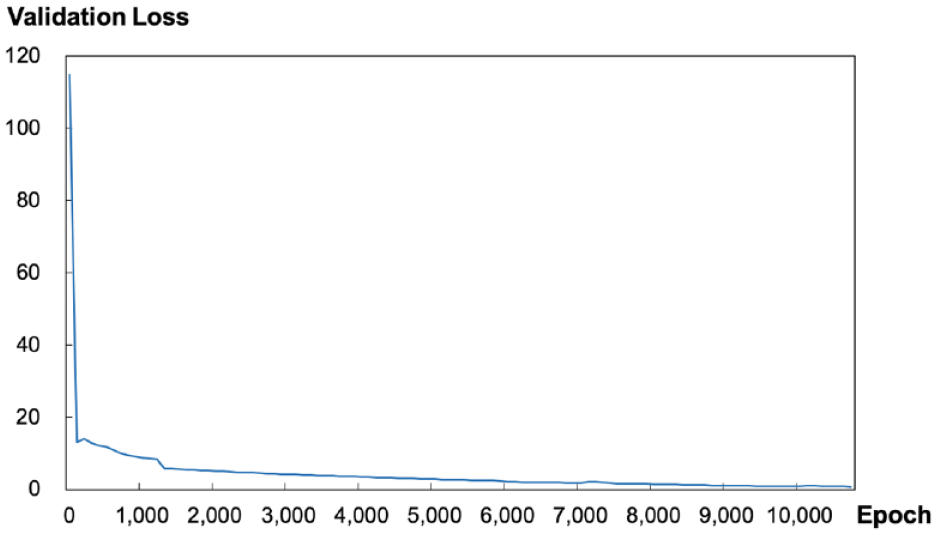
Change in validation loss as a result of model training: validation loss decreased as the epochs increased.
Confusion Matrix of Single-Shot Detection Model for Diagnosis of TMJOA.
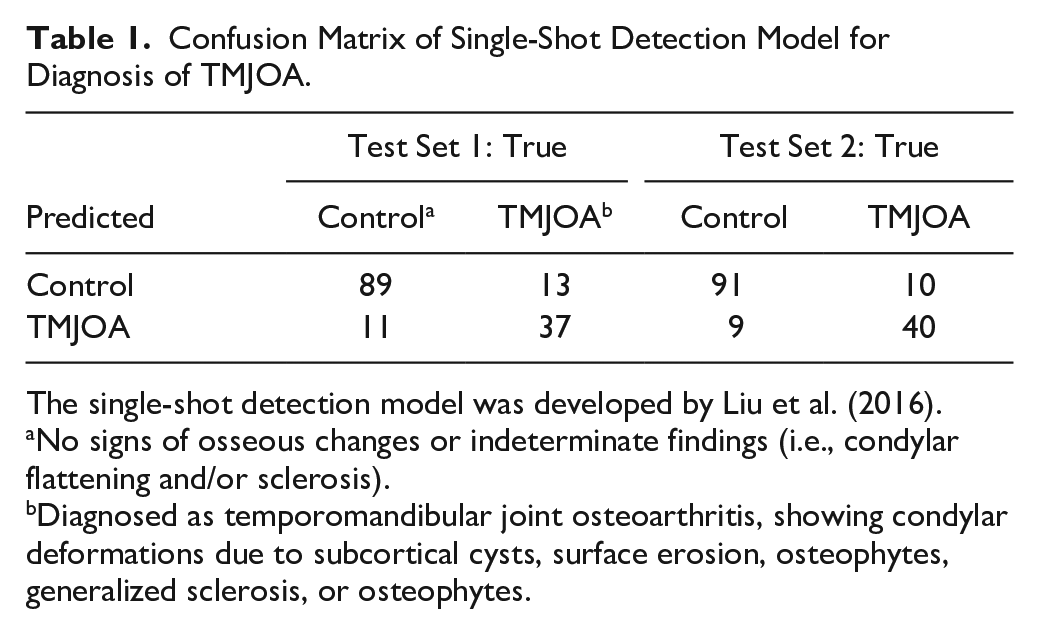
The single-shot detection model was developed by Liu et al. (2016).
No signs of osseous changes or indeterminate findings (i.e., condylar flattening and/or sclerosis).
Diagnosed as temporomandibular joint osteoarthritis, showing condylar deformations due to subcortical cysts, surface erosion, osteophytes, generalized sclerosis, or osteophytes.
Single-Shot Detection Model Performance.
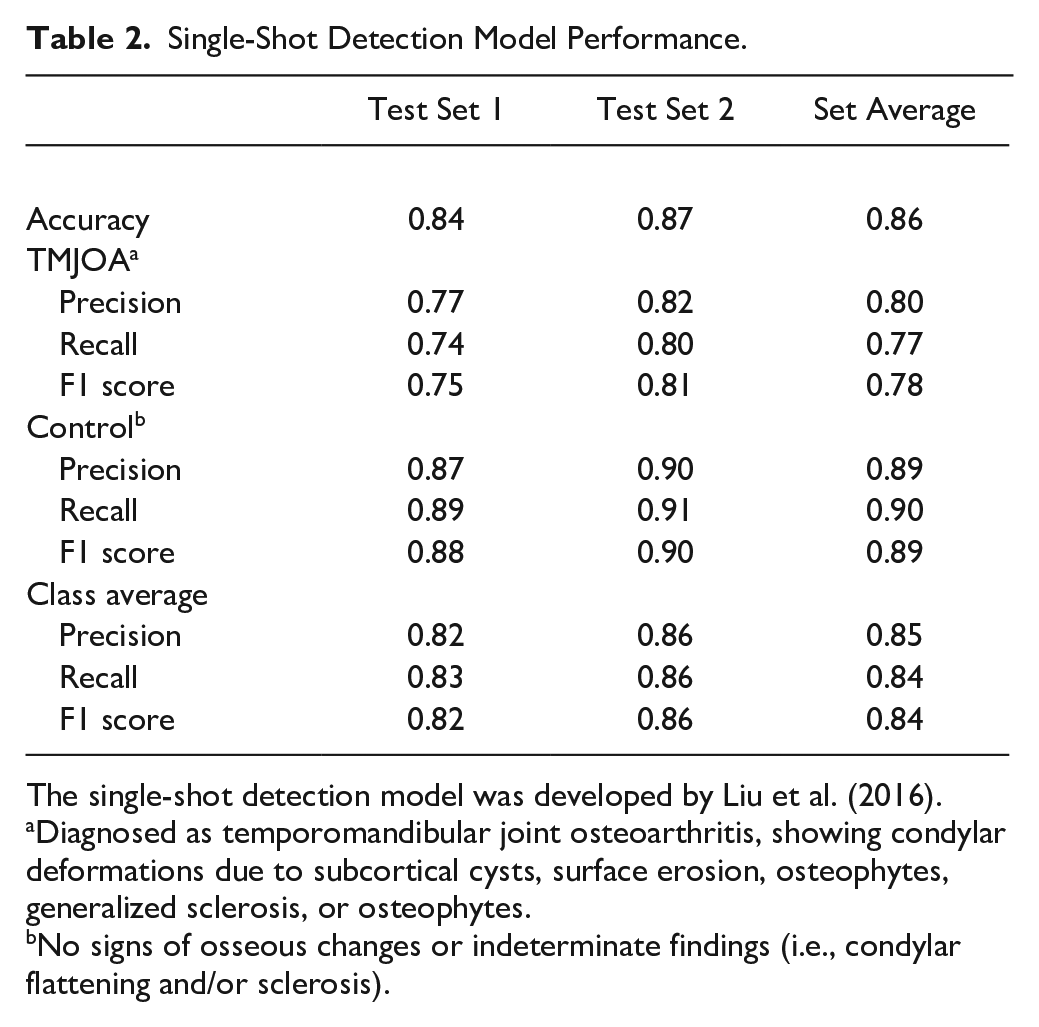
The single-shot detection model was developed by Liu et al. (2016).
Diagnosed as temporomandibular joint osteoarthritis, showing condylar deformations due to subcortical cysts, surface erosion, osteophytes, generalized sclerosis, or osteophytes.
No signs of osseous changes or indeterminate findings (i.e., condylar flattening and/or sclerosis).
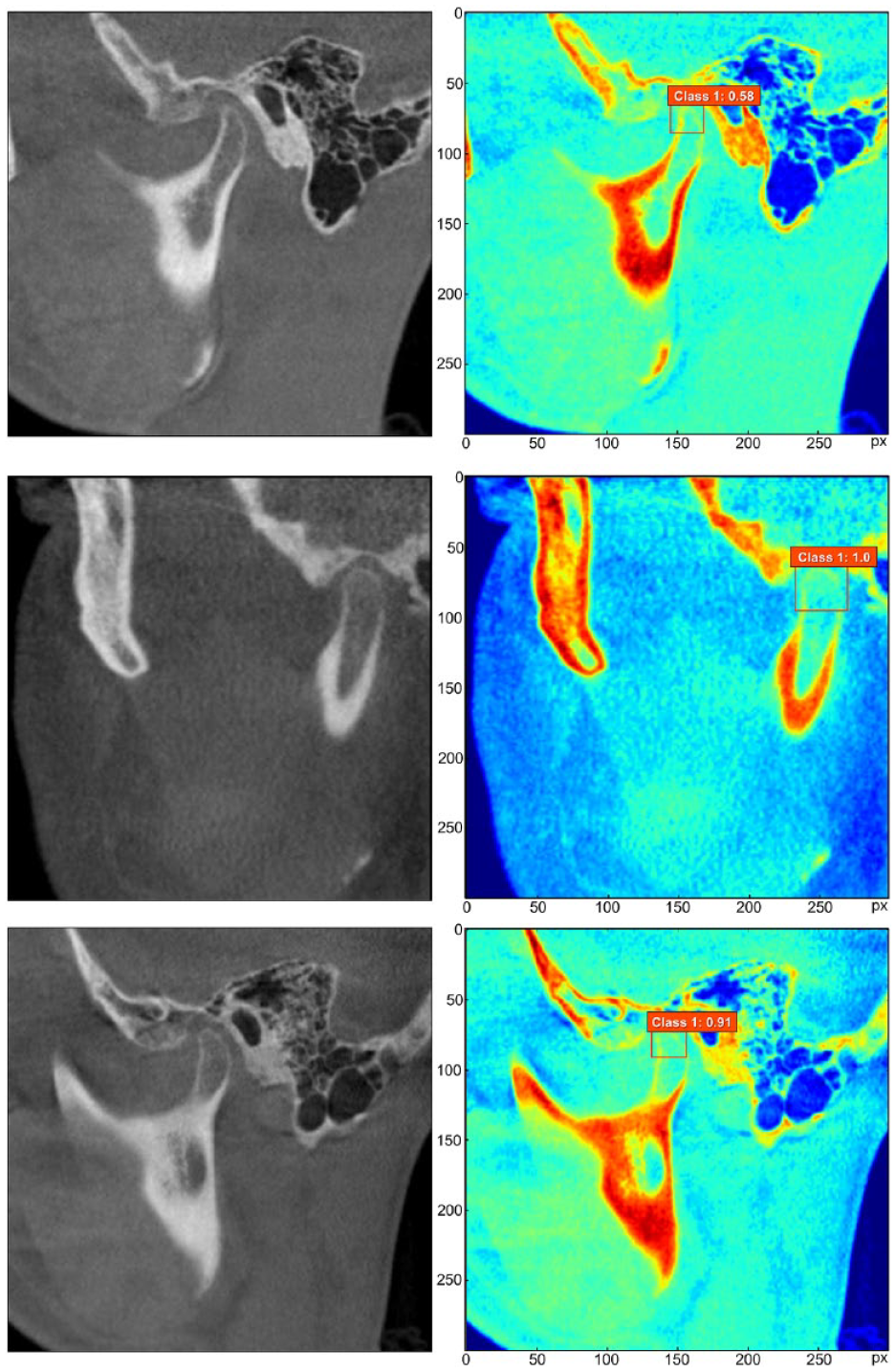
Images correctly classified as indeterminate for TMJOA (class 1). The region of interest, the condylar head, was detected (red box) and classified as indeterminate for TMJOA. Also, a confidence level ranging from 0 to 1 is provided for the indicated class. TMJOA, temporomandibular joint osteoarthritis.
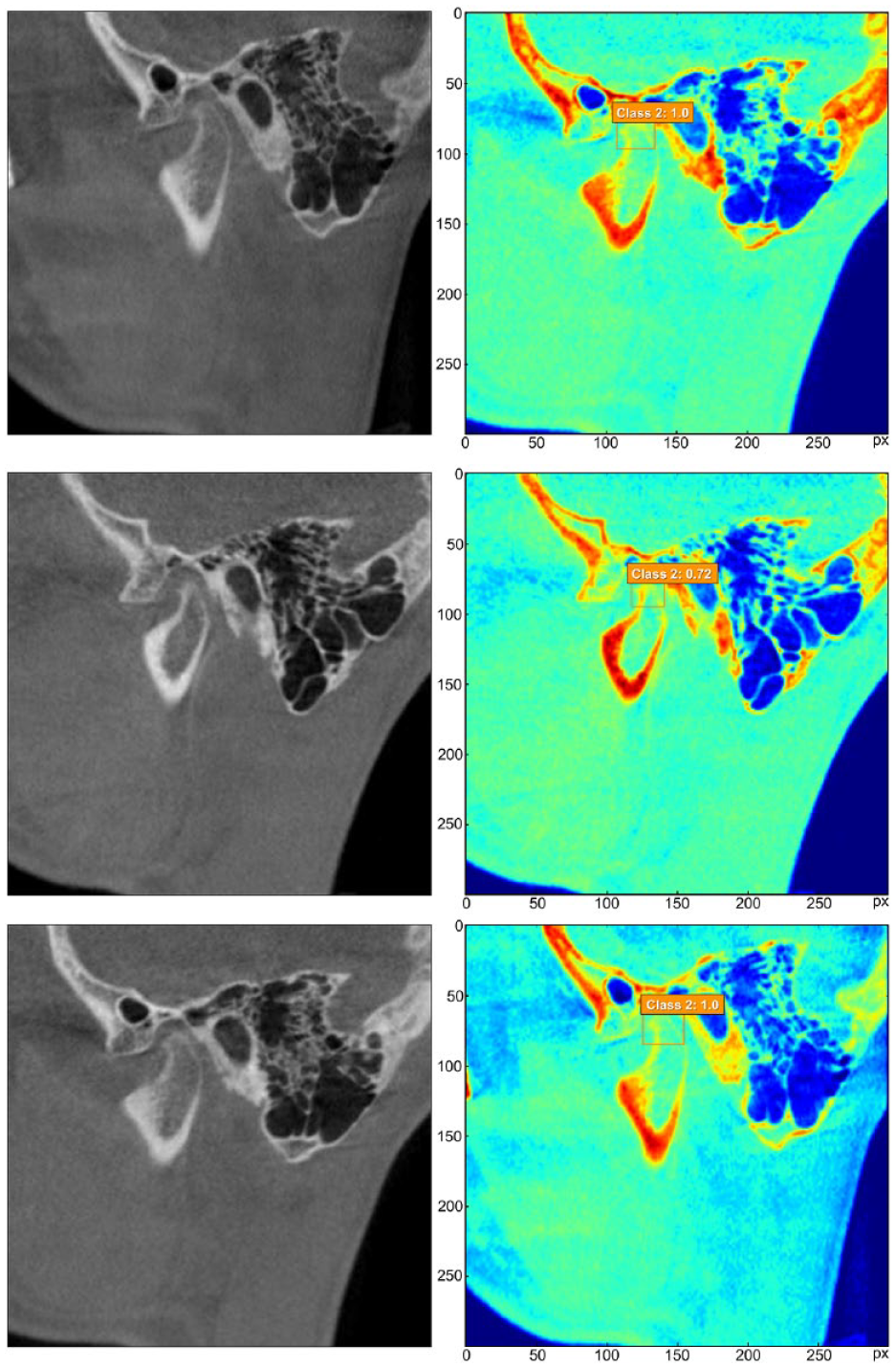
Images correctly classified as TMJOA (class 2). The region of interest, the condylar head, was detected (orange box) and classified as TMJOA. Also, a confidence level ranging from 0 to 1 is provided for the indicated class. TMJOA, temporomandibular joint osteoarthritis.
Discussion
From the sagittal CBCT images of the condyle, the SSD model developed in this study automatically detected the area of the condylar head that showed signs of osseous changes; in addition, the SSD model classified the images into 3 categories: class 1, indeterminate for TMJOA; class 2, TMJOA; class 3, normal with no detection. We trained the model only with condylar images of patients having TMD symptoms and showing signs of osseous changes in the TMJ CBCT; images showing a round condylar head morphology with no signs of bony changes were excluded. In general, the AI model for detecting lesions is trained with images that have lesions, such as TMJOA. Thus, in CBCT images with signs of TMJOA, the trained model would identify and classify the lesions as trained (indeterminate for TMJOA or TMJOA). In normal images, nothing would be detected with a final diagnosis of normal. The average accuracy, precision, recall, and F1 score over the 2 test sets were 0.86, 0.85, 0.84, and 0.84, respectively. These results indicate the stability of the model as well.
A previous study on the diagnosis of TMJOA with deep learning was reported by de Dumast et al. (2018); they constructed 3D condylar models and analyzed biomarkers that were associated with 3D morphologic deviations by using a shape correspondence algorithm. Although the 2-dimensional sagittal images used in this study do not provide visualization of the overall condylar morphology, we observed the integrity of the cortical bone lining and subcondylar sclerosis, which may be associated with the early stage of TMJOA. However, some sagittal sections may not contain osseous changes. Thus, observing all image sections, such as the coronal and axial sections, for a condyle may be needed for accurate diagnosis. Further training of additional views of the condyle should support the understanding of the 3D position on the condyle having arthritic changes.
The images diagnosed as class 1 (indeterminate) may be considered normal variation, aging, physiologic remodeling, or a precursor to TMJOA (Schiffman et al. 2014). Therefore, 50 class 1 images and 50 normal images of TMJs were regarded as the control group in the test process. Similarly, in the accuracy analysis per the image analysis criteria of the research diagnostic criteria for TMD (Ahmad et al. 2009), the authors combined the diagnoses of normal and indeterminate for TMJOA as no osteoarthritis, which was then compared with TMJOA. In other CNN models developed for lesion detection (e.g., brain tumors), models are generally trained with tumor images that are relatively easy to detect because tumors have specific round or ellipsoidal shapes that are easily distinguishable. It is challenging to diagnose TMJOA because a condylar head in a sagittal image is relatively small and the osseous changes in the early stages of TMJOA may be too subtle to distinguish, even for clinicians.
Images that were misclassified by the AI model were observed. Among some class 1 cases that were misclassified as class 2, the cortical bone lining showed discontinuity accompanied by sclerosis in the underlying bone (Appendix Fig. 1). Although the cortical outline of the condylar head was the main feature, the AI model recognized the subcondylar sclerotic area as the outline of the condyle. Consequently, the detected region of interest missed the superior border of the condyle and recognized that the condylar shape was deformed. Additional categories based on the continuity of the cortical bone lining and the presence of subcondylar sclerosis may be defined in training for future studies. Most class 2 cases misclassified as class 1 were borderline cases (Appendix Fig. 2). In some images, the “bird beak” feature indicating proliferative changes was present. However, it was not clearly visible because of the low image contrast with the thin cortical border.
A limitation of this study is that only 1 observer classified the TMJ images in the training data set. However, the diagnosis of TMJOA was strictly based on the image analysis criteria for the research diagnostic criteria for TMD, which is an internationally accepted standard for the diagnosis of TMD (Ahmad et al. 2009). According to Ahmad et al. interexaminer reliability for the diagnosis of TMJOA was reported as a kappa statistic of 0.71 for CT, which is close to the threshold for excellent. In contrast, reliability was poor for panoramic radiography (k = 0.16) and fair for magnetic resonance imaging (MRI; k = 0.46). In addition, positive percentage agreement for diagnosing TMJOA among radiologists was 84% for CT and 19% and 59% for panoramic radiography and MRI, respectively (Ahmad et al. 2009). For testing the SSD model, however, 3 dentists independently diagnosed the 300 images of TMJ in the 2 test data sets. The results showed high accuracy, as demonstrated in the results.
CBCT images are optimized for observations of the bony changes of the TMJ. In cases where differential diagnoses of the active inflammation are required, such as juvenile idiopathic arthritis, additional imaging modalities, including contrast-enhanced MRI and bone scintigraphy, may provide more accurate information on the presence of active inflammation in the TMJ (Küseler et al. 1998; Peacock et al. 2016).
Conclusions
Automated detection of TMJOA from sagittal CBCT images was possible by using a deep neural networks model. It may be used to support clinicians in diagnosis and decision making for treatment of TMJOA. In the future, a model that incorporates data other than images, such as signs, symptoms, patient demographic data, and medical records, would increase diagnostic accuracy. Additionally, training images with more classifications should provide insight into the clinical phenotypes of TMJOA and their possible associations with etiologic factors, such as biomarkers, genetic variations, and immunologic responses.
Author Contributions
K.S. Lee, contributed to conception, design, and data analysis, drafted and critically revised the manuscript; H.J. Kwak, contributed to design and data acquisition, critically revised the manuscript; J.M. Oh, N. Jha, contributed to data acquisition, drafted the manuscript; Y.J. Kim, contributed to conception, design, and data interpretation, drafted and critically revised the manuscript; W. Kim, U.B. Baik, contributed to data analysis and interpretation, critically revised the manuscript; J.J. Ryu, contributed to conception, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_0022034520936950 – Supplemental material for Automated Detection of TMJ Osteoarthritis Based on Artificial Intelligence
Supplemental material, DS_10.1177_0022034520936950 for Automated Detection of TMJ Osteoarthritis Based on Artificial Intelligence by K.S. Lee, H.J. Kwak, J.M. Oh, N. Jha, Y.J. Kim, W. Kim, U.B. Baik and J.J. Ryu in Journal of Dental Research
Footnotes
A supplemental appendix to this article is available online.
This study was supported by the National Research Foundation of Korea funded by the Ministry of Science and ICT of South Korea (grant 2019R1C1C1009881).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.