
Abstract
This study aimed to determine if sampling of oropharyngeal secretions (OSs) helps improves detection of SARS-CoV-2 RNA by nucleic acid amplification testing of potential patients with COVID-19. The first prospective study consisted of 75 patients with COVID-19 who were ready for discharge and who had 2 consecutive negative results per nucleic acid amplification testing (NAAT) of viral samples retrieved with nasopharyngeal swabs (NPSs). Because of detection of potential false negatives in that cohort, the NAAT results of paired OS and NPS samples from 50 additional recruits with COVID-19 during their recovery stage were used in a second prospective study to compare the diagnostic values of the 2 viral RNA sampling methods. For identification of the frequency of inconsistency between the sampling methods, the McNemar’s test was used for difference analysis and the kappa statistic for consistency analysis. OSs obtained from 2 of the 75 participants in the first study yielded positive results for SARS-CoV-2 nucleic acid. Both were male and aged >60 y. Subsequent chemiluminescence enzyme immunoassays indicated that they were positive for the SARS-CoV-2 IgM and IgG antibodies. For parallel NAAT of OS and NPS samples in the second study, McNemar’s test indicated that the difference between the frequencies of inconsistent parts of OS and NPS was statistically significant (P = 0.021). Cohen’s kappa coefficient for OS and NPS was 0.244, which is indicative of fair consistency. The NPS test has a risk of sending home more patients (59%) who still have the infection, while the OS test will make such an error in fewer patients (14%). Although OS sampling improves the accuracy of SARS-CoV-2 nucleic acid testing, it has to be emphasized that this conclusion is based on a very small sample size. Detection of viral RNA from a patient’s secretions is not confirmative of viral infectivity.
Keywords
Introduction
An epidemic of coronavirus-induced pneumonia (COVID-19), triggered by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), scourged China in November to December 2019 (Huang et al. 2020). Commencing from the epicenter in Wuhan, Hubei province (Chan et al. 2020), the infection rapidly became a pandemic that currently affects >211 countries and territories. Close to 9.5 million people were diagnosed with COVID-19 globally and >480,000 have died (Google News, 2020) through cytokine storm, acute respiratory distress syndrome, multiorgan failure, and sepsis (Vincent and Taccone 2020; Ye et al. 2020). The positive-sense single-stranded RNA virus spreads from person to person through respiration, aerosol, and contact transmission (Deng and Peng 2020). Respiratory infections caused by the Middle East respiratory syndrome coronavirus (Chan et al. 2015) and severe acute respiratory syndrome coronavirus (Cheng et al. 2007) have higher mortality rates. However, SARS-CoV-2 spreads much more rapidly than the other 2 Coronaviridae members, probably because it is also transmitted through asymptomatic carriers, which renders containment a challenge (Yu and Yang 2020). As vaccines against SARS-CoV-2 are unavailable (Amanat and Krammer 2020), COVID-19 pneumonia has become a public health emergency of international magnitude.
For COVID-19, most countries mandate that recovered patients be quarantined for at least 14 d prior to discharge; if subsequent tests become positive, the patient has to return to the hospital for further treatment. This “recurrent positivity” poses a grave challenge to the management of COVID-19 (Chen et al. 2020). Recurrence may be partially attributed to the relatively high rate of false-negative results obtained from nucleic acid amplification testing (NAAT) via reverse transcriptase polymerase chain reaction (RT-PCR), with sensitivity being only 66% to 80% (Ai et al. 2020). The recommended discharge criteria include 2 negative results obtained from NAAT taken 24 h apart (Jin et al. 2020). Thus, the accuracy of NAAT is crucial for determining whether an individual should be discharged.
Specimens for NAAT of SARS-CoV-2 may be collected from the upper respiratory tract (nasopharynx, oropharynx), lower respiratory tract (deep expectoration fluid, bronchoalveolar lavage fluid), serum, or stool (Wang et al. 2020). The accuracy of NAAT is the highest for specimens obtained by bronchoalveolar lavage. This is followed by specimens obtained from deep expectoration, nasopharyngeal swab (NPS), and oropharyngeal swab. Because many hospitals and isolation settings are not equipped with armamentaria for bronchoalveolar lavage (Warriner and Lewis 2019), the procedure is not extensively used in clinical practice. Sputum derived from deep expectoration can avoid false-negative results and misdiagnosis. However, the viral load within alveolar cells varies over the course of the disease (To, Tsang, Leung, et al. 2020; Yu et al. 2020). Chest computed tomography (CT) indicates that SARS-CoV-2 pneumonia lesions are predominantly subpleural and remote from the airway (Shi et al. 2020). Of the 67.8% of patients with COVID-19 who experience a cough, 34.1% produce a dry cough, in which no mucus or phlegm is available for sampling (Guan et al. 2020). Hence, NPSs are most often used for viral sampling (Wölfel et al. 2020).
Recent studies reported that there is more SARS-CoV-2 in oropharyngeal secretions (OSs) than in NPS (Cheng et al. 2020; To, Tsang, Chik-Yan, et al. 2020). Saliva collection is a SARS-CoV-2 sampling method approved by the US Food and Drug Administration under emergency use authorization. This method enables self-sampling by those in quarantine or self-isolation. OSs contain fluids derived from different salivary glands with pulmonary and nasopharyngeal discharges (Sole et al. 2011). A previous study reported that the accuracy of NAAT of respiratory viruses via saliva was equivalent to NPS (Kim et al. 2017).
In the present work, OS was used initially to confirm the negative NAAT results derived from NPS, prior to discharge of a cohort of patients with COVID-19 who had presumably recovered. Detection of potential false negatives in that cohort prompted us to perform NAAT of paired OS and NPS samples collected from additional COVID-19 recruits during their recovery stage. The paired samples were used to compare the diagnostic values of the 2 viral RNA sampling methods. The null hypothesis was that there is no difference between NAAT results derived from OS and NPS sampling.
Methods
OS Sampling for Validation of NPS-Negative Results
The first prospective observational study was approved by the Institutional Review Board of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China (TJ-IRB20200218), compliant with STROBE guidelines (Appendix 1), and registered with the Chinese Clinical Trial Registry (ChiCTR2000030005). Sample size estimation is included in Appendix 2. All recruited participants provided informed consent for participation. OSs were collected for NAAT from patients with COVID-19 who had undergone treatment at Tongji Hospital between March 9 and 14, 2020, and were scheduled for discharge. Procedures for OS sampling are included in Appendix 3.
The inclusion criteria were as follows: 1) posttreated patients with COVID-19 with ready-for-discharge status who had 2 negative results from NAAT of NPS specimens conducted at least 24 h apart; 2) body temperature that had returned to normal for >3 d (<38 °C); 3) chest CT showing obvious absorption of pulmonary inflammation; and 4) improved respiratory systems with peripheral capillary oxygen saturation (SpO2 >93%).
Patients were excluded if they 1) were unable to understand/follow instructions due to severe mental illness; 2) underwent invasive ventilation, such as invasive mechanical ventilation, extracorporeal membrane oxygenation, or both; 3) experienced frequent vomiting; and 4) had consumed breakfast prior to OS sampling.
Two trained researchers (C.Y. and L.L.) worked separately to retrieve samples from all patients to reduce information bias. All recruits meeting the inclusion and exclusion criteria were tested to avoid selection bias. Details of NAAT are included in Appendix 4. The outcome of the study was positive NAAT result based on OS. No predictors, potential confounders, and effective modifiers were anticipated.
Data extracted from the medical records included onset time, cough symptoms during the course of the disease, body temperature, chest CT findings, and NAAT results from NPS during hospital stay. If a medical record was incomplete, the patient or the nurse in charge was contacted by telephone to complete the medical record.
Time-to-event data associated with inclusion criteria 1 to 3 (from the time when a recruit was admitted to the time when the respective end point was reached) were expressed as cumulative incidence of clinical improvement and expressed as Kaplan-Meier plots. The results were reported as average estimates and 95% CIs via Prism 8 (GraphPad). Statistical comparisons of survival curves were not performed because data for body temperature, NAAT, and chest CT were all derived from the same cohort.
The recruits’ oxygen support mechanism (ambient air or low-flow oxygen) was recorded during secretion sampling. Because a patient considered eligible for discharge was no longer critically ill, advanced noninvasive ventilation strategies, such as noninvasive positive-pressure ventilation, nasal high-flow oxygen, or high-frequency oscillatory ventilation, were not administered.
Apart from NAAT, serologic testing of the body’s immune response (IgM and IgG antibody production) against the infected virus was performed on all recruits who were diagnosed as COVID-19 positive based on NAAT derived from NPS or OS (Appendix 5).
Calibration of NAAT Detection Methods: Parallel NPS and OS Sampling
The second STROBE guidelines–compliant (Appendix 1) prospective observational study was approved by the Institutional Review Board of Tongji Hospital (registration TJ-IRB202 00383). All newly recruited participants provided informed consent for participation. Sample size estimation is included in Appendix 2.
OSs and NPS were collected from 50 new patients diagnosed with COVID-19. Sampling procedures are included in Appendix 3. The recruited patients had been receiving treatment at Tongji Hospital and Huoshenshan (Mount Fire God) Hospital between March 16 and April 7, 2020. Samples were transferred to the Medical Laboratory of Tongji Hospital or Huoshenshan Hospital for NAAT of SARS-CoV-2. Data collected from medical records included age, sex, comorbidities, onset time, body temperature, and NAAT results from OS and NPS during hospital stay. If the information of a medical record was incomplete, the recruited patient was contacted by telephone by the nurse in charge to complete the medical record.
Patients were included if 1) they had confirmed COVID-19 and 2) both OS and NPS were used for NAAT and the interval between OS and NP swab sampling was <24 h. Patients were excluded if 1) they had endotracheal intubation and 2) they had consumed breakfast prior to OS sampling.
OS and NPS samples were obtained from each recruit to avoid selection bias. The outcomes of the study were sensitivity, Youden’s index, agreement rate, negative predictive value, and negative likelihood ratio. Outcomes were based on analysis of data obtained from positive NAAT results derived from NPS and OS sampling. No effective modifiers, potential confounders, and predictors were anticipated.
Analyses were performed with SPSS 19.0 (IBM). Continuous variables were presented with mean and standard deviation if the data satisfied normality and homoscedasticity assumptions. Otherwise, data were presented as median and interquartile range. Categorical variables were reported as frequencies (percentages).
Because there is no currently accepted gold standard for nucleic acid detection of SARS-CoV-2, the NAAT results obtained from combining OS and NPS samples of an individual into a parallel experiment were taken as “the ground truth,” which was approximated as follows:
True positive: patients tested positive by either of the 2 diagnostic tests (OS and NPS)
True negative: patients tested negative by both tests
For identification of the frequency of inconsistency between the sampling methods, the McNemar’s chi-square test was performed for difference analysis and the kappa statistic for consistency analysis.
Results
OS Sampling for Validation of NPS-Negative Results
Seventy-five patients who fulfilled the inclusive and exclusive criteria were included in the study (Table 1). Of the 75 recruits, 12 took <30 d to yield 2 consecutively negative results from NAAT for SARS-CoV-2, with samples retrieved from the respiratory tract; 57 took 31 to 60 d; and 1 recruit took >60 d to fulfil this criterion.
Demographics and Clinical Characteristics of the COVID-19 Cohort in the First Study.
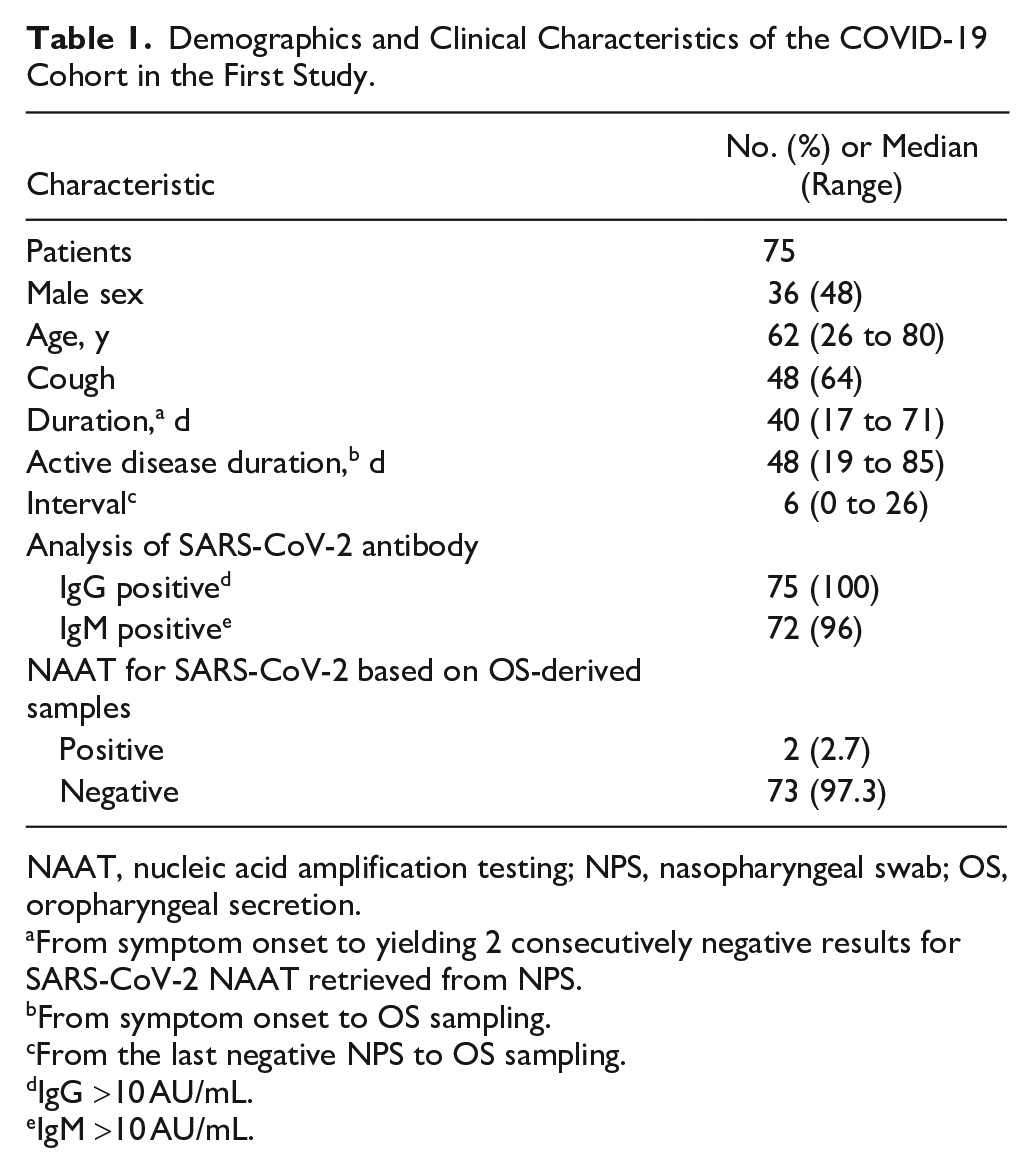
NAAT, nucleic acid amplification testing; NPS, nasopharyngeal swab; OS, oropharyngeal secretion.
From symptom onset to yielding 2 consecutively negative results for SARS-CoV-2 NAAT retrieved from NPS.
From symptom onset to OS sampling.
From the last negative NPS to OS sampling.
IgG >10 AU/mL.
IgM >10 AU/mL.
Over the course of their illness, the patients’ fever (body temperature), pulmonary condition (chest CT), and viral status (NAAT) gradually improved (Fig. 1). The patients’ body temperature returned to normal first (mean, 5.91 d; 95% CI, 3.27 to 8.55). This was followed by the NAAT results becoming negative (mean, 27.15 d; 95% CI, 24.72 to 29.58) and, finally, improvement in the pulmonary status (mean, 36.05 d; 95% CI, 36.60 to 38.50).
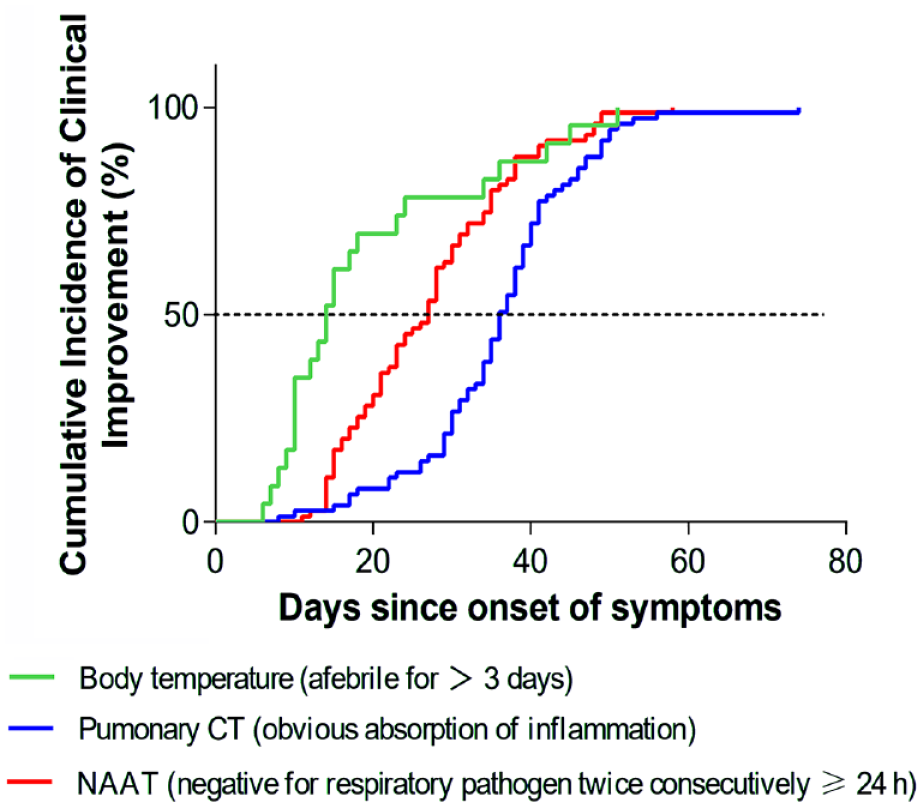
Cumulative incidence of clinical improvement for the entire cohort from symptom onset (day 0) to day 80. CT, computed tomography; NAAT, nucleic acid amplification testing.
Prior to their official discharge from Tongji Hospital, all members of the cohort were retested for SARS-CoV-2 with OS samples. These participants were predominantly breathing ambient air (73.3%), while the rest were taking low-flow oxygen when their secretions were collected. Surprisingly, 2 male participants who had a dry cough and no obvious sputum were SARS-CoV-2 positive (Fig. 2). Their demographic and clinical characteristics are summarized in Appendix 6. Their oxygen support requirements during the hospitalization period are depicted in Appendix 7. Because the 2 participants had already satisfied the hospital discharge criteria, they would have been discharged and staying in quarantine hotels if not for the additional NAAT based on OSs. The 2 patients were readmitted to the hospital.
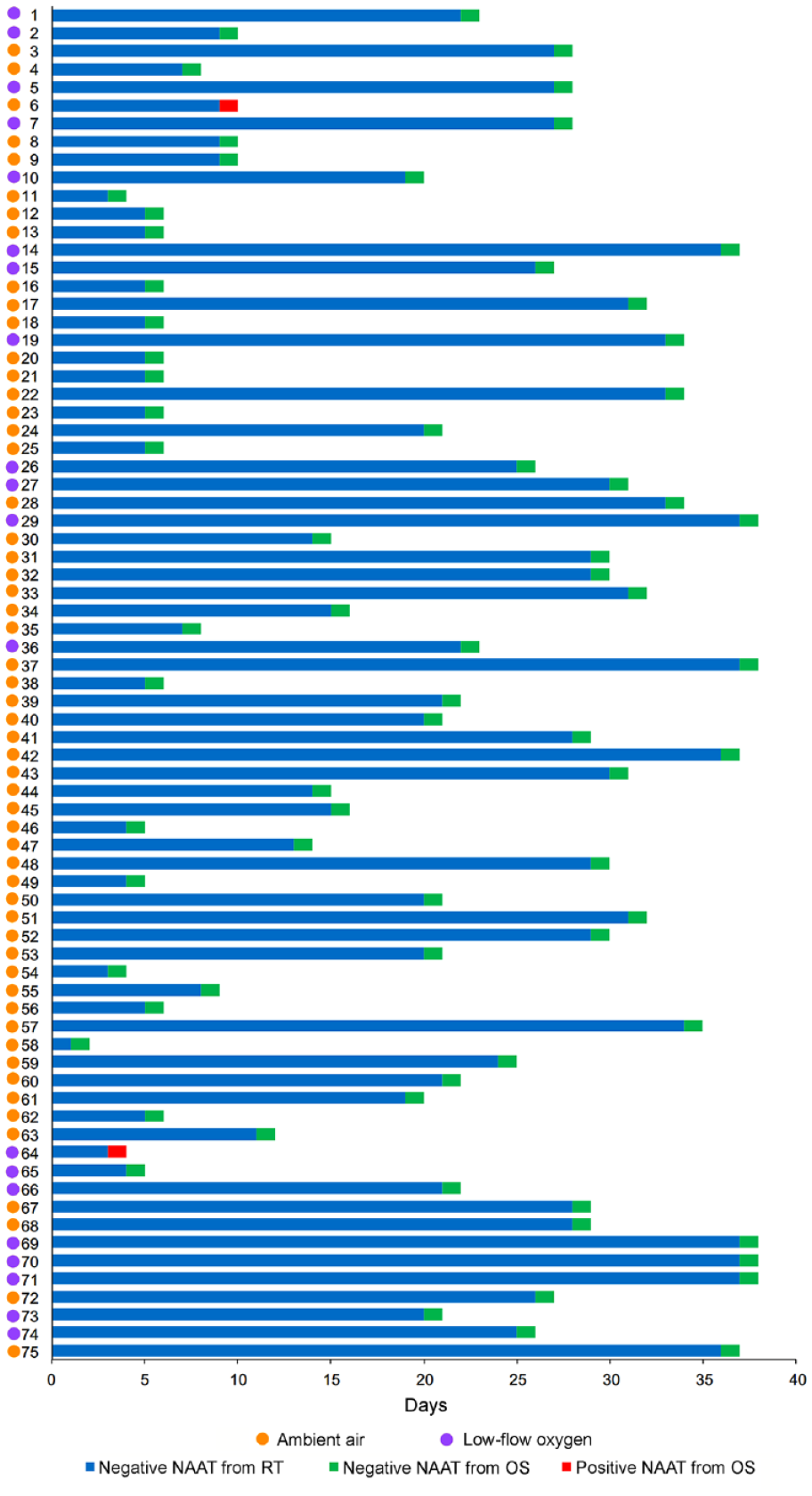
Data derived from a cohort of 75 posttreated patients with COVID-19 who were ready to discharge, based on 2 negative nucleic acid amplification testing (NAAT) results for SARS-CoV-2 obtained from the respiratory tract (RT). For each patient in this first study, the number days from first negative NAAT results from RT to the acquisition of oropharyngeal secretions (OSs) for additional NAAT is indicated as a blue box of variable length. Green box: negative NAAT result based on sample derived from OS. Red box: positive NAAT result based on sample derived from OS. The patients’ oxygen support mechanisms during the time of OS retrieval are represented by the line of circles on the left of the chart. Orange circle: ambient air. Purple circle: low-flow oxygen.
Serologic testing for SARS-CoV-2-specific antibodies indicated that they were IgM and IgG positive (note that IgM becomes detectable prior to IgG and disappears during the convalescence phase of an infectious disease; Table 1). For the 2 patients who were retested for antibodies after OS sampling, the IgM titer of patient 2 was >166 times that of IgG. Combined with a positive NAAT result, the data suggest that patient 2 was still in the active, declining phase of infection (Lauer et al. 2020; To, Tsang, Leung, et al. 2020; Appendix 8). Although the IgM titer was in the normal range for patient 1, his IgG titer exceeded the threshold for normality. Combined with a positive NAAT result from OSs, the data suggest that patient 1 could be in the late or recurrent stage of infection (Appendix 3).
Calibration of NAAT Detection Methods: Parallel NPS and OS Sampling
Demographics of the 50 recruits with COVID-19 are presented in Appendix 9. The NAAT results derived from OS and NPS are listed in Table 2. Based on these results, the ground truth assumption was as follows: truly positive cases = 19 + 9 – 6 = 22; truly negative cases = 28 (total 50). Comparison of each test with the ground truth is listed in Table 3. The ability of OS to detect SARS-CoV-2 was stronger than that of NPS (sensitivity: 86% vs. 41%). The diagnostic capability of OS was stronger (Youden’s index: 86% vs. 41%). The OS results were in better agreement with “the ground truth” (agreement rate: 94% vs. 74%). For patients with negative diagnosis, the probability of recruits who were true disease-free was higher for OS (negative predictive value: 90% vs. 68%). As a consequence of the ground truth definition, specificity and positive predictive value were maximum by design (i.e., there are no false positives).
NAAT Results for SARS-CoV-2 from Paired OS and NPS Samplings Performed in the Second Study.
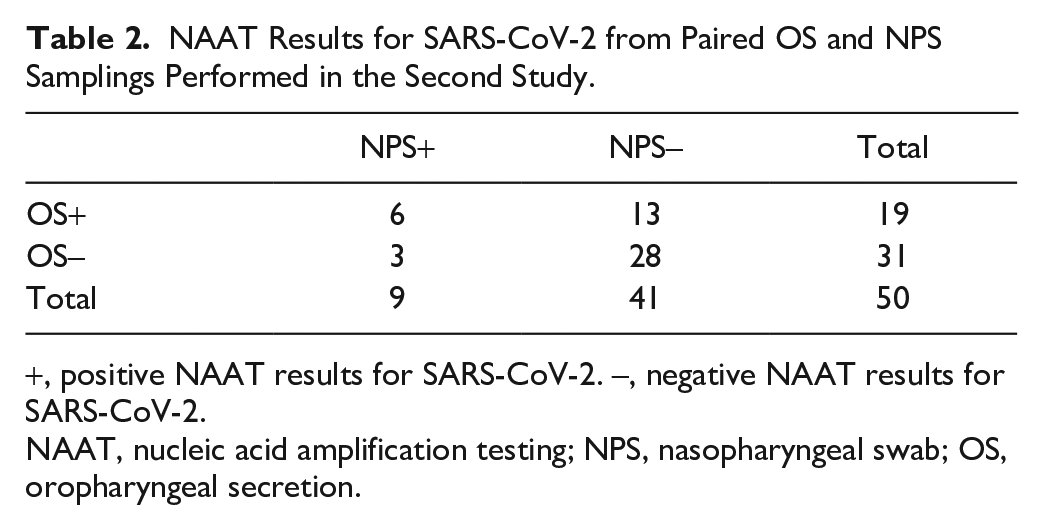
, positive NAAT results for SARS-CoV-2. –, negative NAAT results for SARS-CoV-2.
NAAT, nucleic acid amplification testing; NPS, nasopharyngeal swab; OS, oropharyngeal secretion.
Comparison of Each Test with “the Ground Truth.”
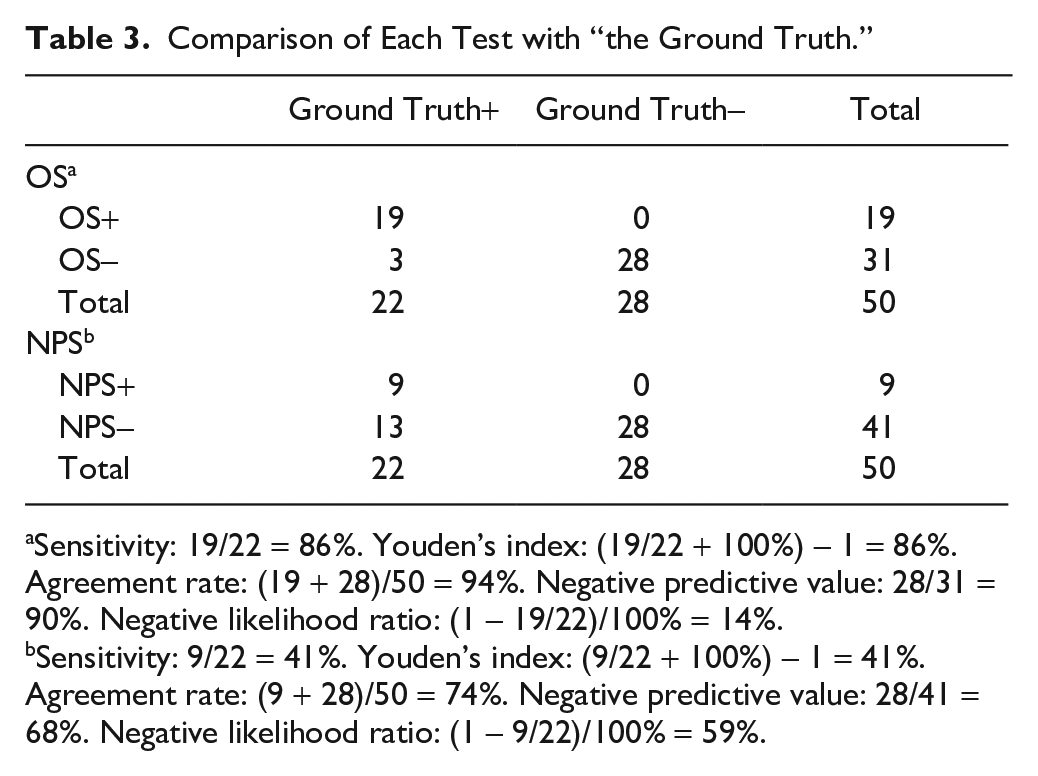
Sensitivity: 19/22 = 86%. Youden’s index: (19/22 + 100%) – 1 = 86%. Agreement rate: (19 + 28)/50 = 94%. Negative predictive value: 28/31 = 90%. Negative likelihood ratio: (1 – 19/22)/100% = 14%.
Sensitivity: 9/22 = 41%. Youden’s index: (9/22 + 100%) – 1 = 41%. Agreement rate: (9 + 28)/50 = 74%. Negative predictive value: 28/41 = 68%. Negative likelihood ratio: (1 – 9/22)/100% = 59%.
McNemar’s test indicated that the difference between the frequencies of inconsistent parts of OS and NPS was statistically significant (P = 0.021). The Cohen’s kappa coefficient for OS and NPS was 0.244, which is indicative of fair consistency.
Discussion
The present study confirms recent reports that a small percentage of convalescent patients retested positive after 2 negative consecutive results from NAAT of NPS samples and remained carriers of viral SARS-CoV-2 RNA (Yuan et al. 2020; Zhang et al. 2020). Rather than being a manifestation of a recurrent disease, the phenomenon has been attributed to false-negative RT-PCR results or delayed viral clearance from the upper respiratory tract (Xiao et al. 2020).
Viral pneumonia usually does not produce purulent sputum (Shah and Wunderink 2017). Thus, NPS is the preferred method for retrieving viral RNA for COVID-19 diagnosis and chaperoning the duration of patient isolation or hospital discharge. With respect to false-negative results, although the kits employed for NAAT have been approved by the corresponding disease-monitoring organizations and possess high specificity, false negatives may occur if a sample contains inadequate amount of viral RNA to be amplified (Cheng et al. 2020; Lippi et al. 2020). The quantity of viruses present in the upper respiratory tract depends on how soon the samples were retrieved after onset of clinical symptoms (Loeffelholz and Tang 2020). This is due to the difference in extent of nasopharyngeal virus shedding during the course of the infection (Wölfel et al. 2020). The retrieved viruses are highly pathogenic, and thermal inactivation at 56 °C is used by some clinical microbiology laboratories prior to RNA extraction. This may also result in increased Ct values in RT-PCR detection, particularly for samples with low viral loads (Pan et al. 2020). In this regard, guanidinium-based inactivation agents appear to be less destructive to viral genetic materials (Tang et al. 2020).
Results of the present study showed that the NPS test has a risk of sending home more patients (59%) who still have the infection, while the OS test will make such an error in fewer patients (14%); this is a direct consequence of the difference in sensitivity. This requires rejection of the null hypothesis that there is no difference between NAAT results derived from OS and NPS sampling. OSs do not only contain saliva secreted by major and minor salivary glands but also include secretions descending from the nasopharynx or arising from the lung via the cilia lining of the respiratory tract. Collection of OS has several advantages. Sampling of OS is a simple procedure that can be performed in any quarantine setting. This sampling method minimizes contact between health care workers and patients, thereby reducing the risk of virus transmission. Collection of nasopharyngeal specimens tends to be uncomfortable and may cause bleeding in patients with reduced platelet counts who are more susceptible to bleeding. Conversely, OS sampling is noninvasive and does not create discomfort for patients. Moreover, the sudden increased demand for NPS created by the pandemic has created immense pressure on supply chain capacities for these products. The use of an alternative NAAT sampling method would be an immense relief for countries that are short of these sampling items. As a form of liquid biopsy (Aro et al. 2017), oropharyngeal discharges are also valuable for point-of-care detection of the novel coronavirus (Sri Santosh et al. 2020).
In terms of accuracy, saliva specimens have a consistency rate >90% in the detection of respiratory viruses by molecular assay when compared with nasopharyngeal aspirates (To et al. 2019). Consistent detection of SARS-CoV-2 has been reported in the saliva of 11 patients with COVID-19 from the first day of hospitalization in a Hong Kong hospital (To, Tsang, Chik-Yan, et al. 2020). These positive results were confirmed in a more recently published Italian study (Azzi et al. 2020). Similar to the findings of the present study, the authors of the Italian study reported positive salivary results on the same day when NPS sampling indicated conversion.
In the first part of the present study, the 2 participants who retested positive for SARS-CoV-2 after OS sampling were subjected to serologic validation. Production of IgM is the body’s first line of defense against infections. The IgM titer rises for a short time when the body senses an invader, and it begins to drop as the IgG level kicks in to protect the body in the long term. Studies have reported that the IgM and IgG antibodies of SARS-CoV-2 were detected as early as the fourth day after onset of symptoms (Xiang et al. 2020). This suggests that serologic detection may play an important complementary role in the validation of tests that are based on detection of viral genetic material.
A limitation of the present work is the inevitable presence of a certain degree of selection bias because of the single/double-center study design. The initial conditions of patients with COVID-19 admitted to 2 hospitals were severe. Hence, the virus-shedding time in these patients may be different from the COVID-19 infected by the general population at large. Another limitation is that specificity was not reported for NAAT with OS or NPS sampling in the second part of the study. Specificity, also known as the true-negative rate, measures the proportion of actual negatives who are correctly identified as such. Accurate expression of specificity requires the use of a gold standard for nucleic acid detection of SARS-CoV-2, which, unfortunately, is not available to date. Hence, expressions of specificity for NAAT based on OS or NPS testing are not meaningful.
In conclusion, results of the present study are supportive of the notion that OS sampling improves the accuracy of SARS-CoV-2 nucleic acid testing. Nevertheless, it has to be emphasized that this conclusion is based on a very small sample size. It must be mentioned that detection of viral RNA from a patient’s secretion or excretory products is not confirmative of viral infectivity (Joynt and Wu 2020). Viral RNA has been shown to be detectable after disappearance of the infectious virus. For SARS-CoV-1, viral RNA was identified in the respiratory secretions and feces of some patients for >30 d after the onset of symptoms, although live viruses could no longer be detected by viral culture after the third week (Chan et al. 2004). This is the limitation of RT-PCR-based assays for clinical diagnosis. Because cultures of aerosol-transmissible disease-causing viruses can be conducted only in a biosafety level 3 microbiology laboratory, the use of OS for NAAT has to be accepted as a proxy for potential transmissibility. Accordingly, the 2 participants in the first part of the study were reisolated in the hospital for observations.
Author Contributions
C. Yu, L. Li, contributed to data acquisition, analysis, and interpretation, drafted the manuscript; Y. Tuersun, Q. Feng, contributed to data analysis and interpretation, drafted the manuscript; X. Zhao, contributed to data acquisition and interpretation, drafted the manuscript; T. Zhang, contributed to conception, critically revised the manuscript; F.R. Tay, J. Ma, contributed to conception and design, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_0022034520940292 – Supplemental material for Oropharyngeal Secretion as Alternative for SARS-CoV-2 Detection
Supplemental material, DS_10.1177_0022034520940292 for Oropharyngeal Secretion as Alternative for SARS-CoV-2 Detection by C. Yu, L. Li, Y. Tuersun, X. Zhao, Q. Feng, T. Zhang, F.R. Tay and J. Ma in Journal of Dental Research
Footnotes
A supplemental appendix to this article is available online.
This work was supported by the National Natural Science Foundation of China (grants 81873714 and 81802710).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.