
Abstract
Despite their prevalence and burdens, oral diseases are neglected in universal health coverage. In Japan, a 30% copayment (out of pocket) by the user and a 70% contribution by Japan’s universal health insurance (JUHI) are required for dental and medical services. From the age of 70 y, an additional 10% is offered by JUHI (copayment, 20%; JUHI, 80%). This study aimed to investigate the effect of cost on dental service use among older adults under the current JUHI system. A regression discontinuity quasi-experimental method was used to investigate the causal effect of the JUHI discount policy on dental visits based on cross-sectional data. Data were derived from the 2016 Japan Gerontological Evaluation Study. This analysis contained 7,161 participants who used JUHI, were aged 68 to 73 y, and responded to questions regarding past dental visits. Analyses were controlled for age, sex, number of teeth, and equalized household income. Mean ± SD age was 72.1 ± 0.79 y for the discount-eligible group and 68.9 ± 0.78 y for the noneligible group. During the past 12 mo, significantly more discount-eligible participants had visited dental services than noneligible participants (66.0% vs. 62.1% for treatment visits, 57.7% vs. 53.1% for checkups). After controlling for covariates, the effect of discount eligibility was significant on dental treatment visits (odds ratio [OR], 1.36; 95% CI, 1.32 to 1.40) and dental checkups (OR, 1.49; 95% CI, 1.44 to 1.54) in the regression discontinuity analysis. Similar findings were observed in triangular kernel-weighted models (OR, 1.38 [95% CI, 1.34 to 1.44]; OR, 1.52 [95% CI, 1.47 to 1.56], respectively). JUHI copayment discount policy increases oral health service utilization among older Japanese. The price elasticity for dental checkup visits appears to be higher than for dental treatment visits. Hence, reforming the universal health coverage system to improve the affordability of relatively inexpensive preventive care could increase dental service utilization in Japan.
Keywords
Introduction
The Global Burden of Diseases Study 2017 revealed that oral disorders such as dental decay and periodontal diseases remained highly prevalent global disorders since 1990 (James et al. 2018). Oral diseases affect individuals’ quality of life by causing pain, discomfort, and inability to enjoy food (Sheiham and Steele 2001; Griffin et al. 2012). Moreover, the high prevalence of oral diseases causes substantial economic and societal burden due to high treatment costs and disability (Birch and Listl 2015; Bernabé et al. 2017). As with chronic conditions in general, the impact of oral diseases is higher on poorer and less educated populations of society (Watt et al. 2016; Rozier et al. 2017). Universal health coverage (UHC) is put forward as a global policy to enable all individuals and communities, irrespective of their socioeconomic position, to receive health services without suffering financial hardship (World Health Organization [WHO] 2005). However, in many countries, oral health is usually isolated from mainstream primary health care services and neglected in UHC (Watt et al. 2019).
According to the WHO (2013), countries can achieve greater UHC along 3 dimensions—by extending population coverage, by including services not previously covered, and by reducing cost sharing and fees. Treatment of oral diseases is costly and often associated with high out-of-pocket expenditure for service users (Bernabé et al. 2017; Dieleman et al. 2020). Thus, including oral health services in the UHC agenda would be one way of increasing coverage that could minimize cost-related inequalities in service use.
Japan has one of the most generous mandatory universal health insurance schemes in the world. Japan’s universal health insurance (JUHI) policy is unique, as it covers a range of dental treatments at a lower cost for its subscribers, as compared with other countries with “universal oral health care systems” (Zaitsu et al. 2018). Among Organisation for Economic Co-operation and Development (OECD) countries, only Japan (78%), Germany (68%), and the Slovak Republic (53%) cover more than half the dental care cost of adults (OECD 2019). Furthermore, Japan had reported the most frequent dental visits among OECD countries (OECD 2011). In 2013, the prevalence of edentulousness among Japanese adults aged 65 to 74 y was 6.9%, as compared with a mean 13.3% among 15 European countries (Stock et al. 2016). However, inequalities in access to dental services still exist in Japan (Murakami et al. 2014). Therefore, assessing the cost sensitivity of service utilization in a country where oral health is already a part of the UHC system could provide a basis for comparisons with cost effects in the absence of a UHC system for oral health.
In general, the use of dental and medical services in Japan requires a 30% copayment (out of pocket) by the user and a 70% contribution by JUHI. When JUHI subscribers reach the age of 70 y, an additional 10% is offered, starting from the month after their birth month (JUHI, 80%; copayment, 20%), which is a 33% reduction in copayment (Sakamoto et al. 2018). This policy rule provides a unique opportunity to use the regression discontinuity (RD) method to investigate the causal effect of changes in out-of-pocket cost on dental attendance in Japan. The RD method is able to capture an observable discontinuity in a treatment, when the level of treatment changes abruptly at a cutoff value of the treatment assigning variable (Imbens and Lemieux 2008).
Using RD, Shigeoka (2014) and Fukushima et al. (2016) found that the reduction of copayments at the age of 70 y increased the utilization of inpatient and outpatient medical services in Japan. Furthermore, Fukushima et al. (2016) found that the price responsiveness was high for services that are at high demand in an aging society, such as orthopaedic and eye specialties. Although dental treatments are at high demand among older adults, neither of these studies investigated the utilization of dental services. Ando and Takaku (2016) used a similar methodology to show the effect of copayment reduction on denture use and subjective chewing ability. However, the data were prior to the implementation of current copayment rates (2014) and did not examine the impact of copayment on dental attendance.
The aim of this study was to investigate whether the use of oral health care services differed before and after the discount JUHI eligibility and, if a significant difference was observed, to investigate the causal effect of the JUHI discount policy on the observed difference.
Methods
Data Source
Our analyses are based on cross-sectional data from the Japan Gerontological Evaluation Study (JAGES) in 2016 (Kondo et al. 2018). The target population of the JAGES survey was community-dwelling older people aged ≥65 y who were functionally independent. The JAGES survey was conducted from September 2016 to November 2017 and collected information on health, behaviors, and socioeconomic characteristics via a postal survey questionnaire.
The target population for JAGES in 2016 was 279,661 potential participants, of which 180,021 people responded. Around one-eighth of the target population (34,567 people) received the questionnaire containing questions regarding dental visits, and 22,282 people responded. Respondents with missing values for outcome variables were not included in analyses. Characteristics of the participants with missing information for outcomes were compared and are reported in Appendix Table 1. Observations with missing values for other covariates were imputed with multiple imputation (Appendix Table 2). Participants who received social welfare benefits were excluded, as they were eligible for free dental care without a copayment. Figure 1 shows the selection flow of participants in this study.
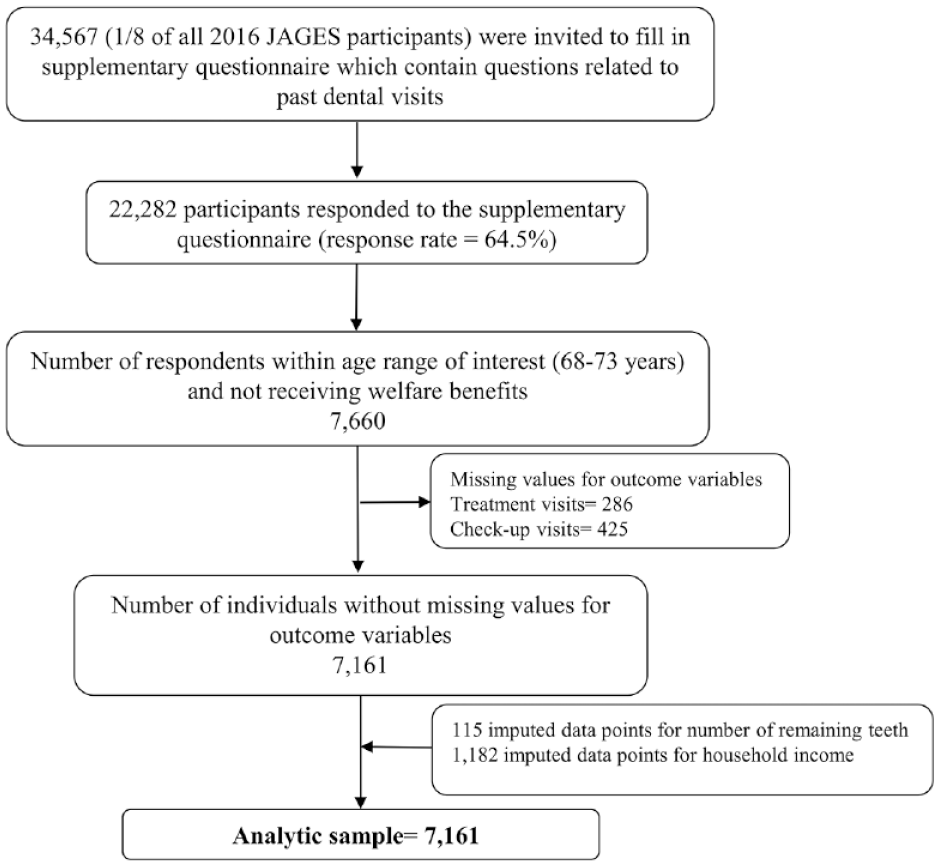
Selection of the participants for the study. JAGES, Japan Gerontological Evaluation Study.
Ethical Approval
The JAGES survey was approved by the ethics committee of the National Center for Geriatrics and Gerontology (No. 992) and the ethics committee of Chiba University (No. 2493).
Outcome Variables
This study used 2 outcome variables (Y) that reflect dental attendance during the past 12 mo. Outcome variables were derived from responses to the questions regarding the time of the latest dental treatment visits and dental checkup visits, with the following response options: 1) during the past 6 mo, 2) 6 mo to 1 y ago, 3) 1 to 3 y ago, 4) >3 y ago, and 5) never seen a dentist. We created dichotomous variables for treatment visits and checkup visits by combining responses 1 and 2 = 1 (during past 12 mo) and 3, 4, and 5 = 0 (>12 mo ago).
Forcing Variable
The forcing variable (Z) was used to assign observations into “treatment” and “control” groups around a cutoff value of the forcing variable (Imbens and Lemieux 2008). The copayment rate for dental care was 30% among those aged ≤69 y and 20% among those aged ≥70 y. We used age as the forcing variable, with age 71 y as the cutoff point. The 71-y cutoff point was chosen as the outcome variables were referring to dental visits during the past 12 mo. Hence, those who were aged 70 y at the time of survey were included in the control group (68, 69, and 70 y as noneligible; 71, 72, and 73 y as discount eligible). People who turned 70 y before 2014 continued to receive a copayment discount under the old copayment scheme (which was 33% more generous than current rate). Therefore, we limited the maximum age as <74 y at the time of the survey to avoid the inclusion of participants falling under the old copayment scheme. A derived age variable centered on the cutoff value (age 71 y = 0) was used in analyses.
Treatment Variable/Discount Eligibility
A dummy treatment assignment variable (T) was created with the age cutoff: T = 0 if Z < cutoff and T = 1 if Z ≥ cutoff. This variable estimated the effect of discount eligibility in RD models.
Covariates
A categorical variable indicating the number of remaining teeth (0, 1 to 9, 10 to 19, ≥20 teeth) and equivalized annual household income in Japanese yen (<2 million, ≥2 to <3 million, ≥3 to <4 million, ≥4 million) were used as covariates (X) in the analyses. Equivalized income was calculated by dividing the annual household income by the square root of the number of family members. Furthermore, all models were adjusted for sex and age (forcing variable).
Statistical Analysis
Descriptive analysis presented the characteristics of the participants against discount eligibility. Then we adopted an RD approach to estimate the effect of JUHI discount eligibility on dental attendance during the past 12 mo. Following the methodology suggested by Jacob et al. (2012), we tested a variety of functional forms of the forcing variable (Z) to identify which fitted our data best based on F statistics and the robustness of estimates (Appendix Tables 3 and 4). We used linear and quadratic interaction forms of the forcing variable. In line with recommendations (Gelman and Imbens 2019), we avoided higher-order polynomials, as they can lead to nonsensical results. The following logistic regression model was used to estimate the effect of discount eligibility on the probability of dental attendance during the past 12 mo.

Y = probability of a dental visit during past 12 mo
T = dummy treatment variable (1 if Z ≥ cutoff, 0 if Z < cutoff)
Z = forcing variable (age-centered variable)
f = polynomial function of Z (quadratic function)
X = matrix of covariates (number of teeth, income, sex)
β1 = measure the impact of discount eligibility (RD estimate)
ε = error term
Logistic regression models were used to predict the likelihood of dental attendance during the past 12 mo for dental treatments and dental checkups. To check the robustness of the RD estimate, a triangular kernel-weighted model was used, which assigns more weight to observations closer to the cutoff. We used 20 multiple-imputed data sets for RD analyses. Then, a single mean estimate and adjusted standard errors were calculated (Rubin 2004). A supplementary complete case-only analysis assessed the robustness of the imputed analysis (Appendix Table 5).
Stata MP 15.1 (StataCorp LLC) was used for analyses. RD plots were constructed with the matplotlib Python library. The reporting of this study conforms to STROBE guidelines.
Results
Table 1 reports descriptive statistics on outcome variables and covariates by discount eligibility. The mean ± SD age was 72.1 ± 0.79 y for the discount-eligible group and 68.9 ± 0.78 y for the noneligible group. Discount-eligible participants reported a higher prevalence of dental treatment and checkup visits than noneligible participants during the past 12 mo (treatment visits: 66.0% vs. 62.1%, P < 0.001; checkup visits: 57.7% vs. 53.1%, P < 0.001). The discount-eligible group had higher proportions of edentulous status and people in the lowest household income as compared with the noneligible group.
Characteristics of the Sample by Discount Eligibility.
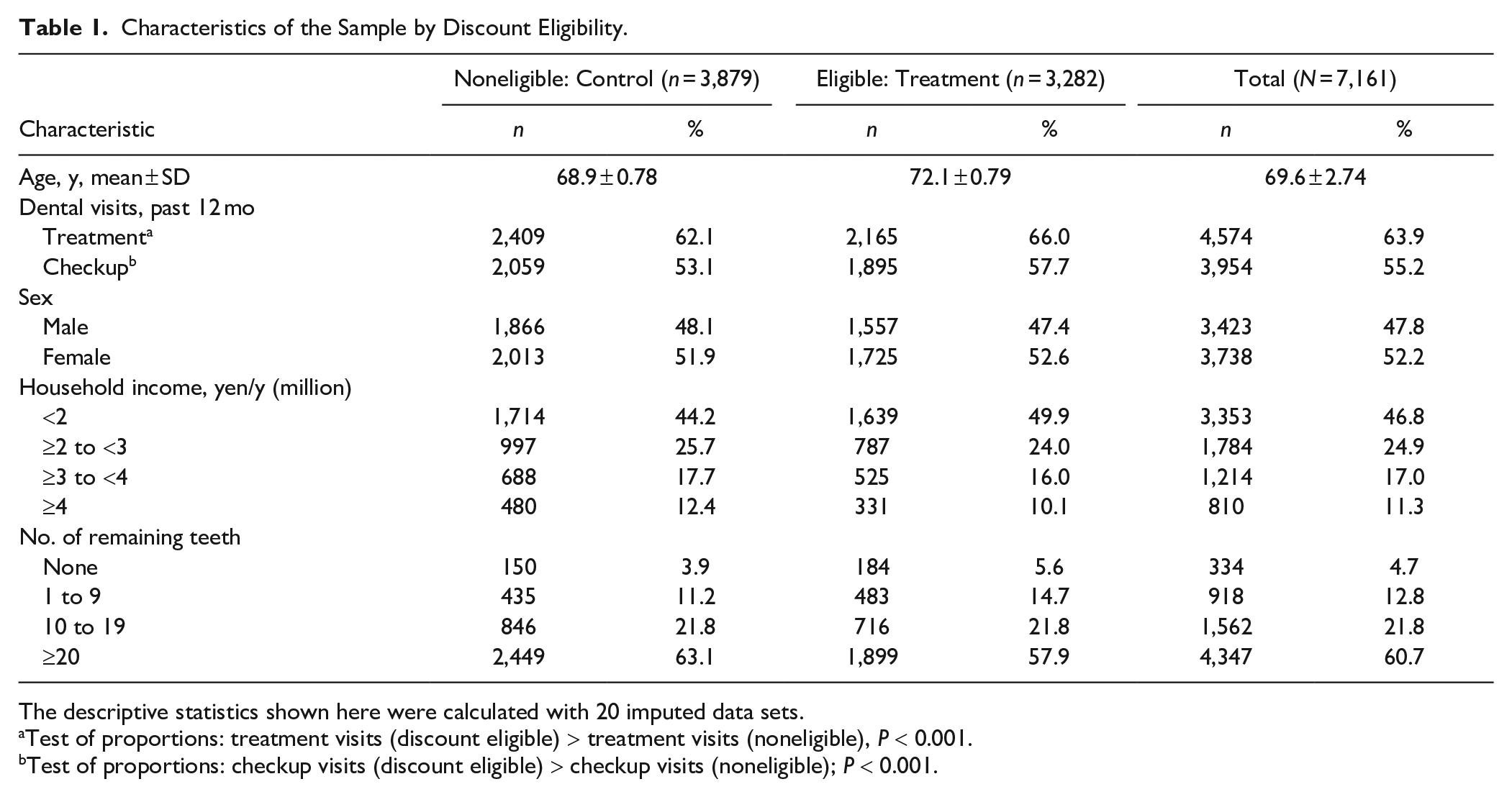
The descriptive statistics shown here were calculated with 20 imputed data sets.
Test of proportions: treatment visits (discount eligible) > treatment visits (noneligible), P < 0.001.
Test of proportions: checkup visits (discount eligible) > checkup visits (noneligible); P < 0.001.
RD estimates and other covariate-related coefficients from unweighted and triangular kernel-weighted logistic models are reported as odds ratios (ORs) in Table 2. Coefficients related to the dummy variable that indicates discount eligibility (T) measured the change in the probability of dental attendance during the past 12 mo between the discount-eligible and noneligible groups, after adjusting for covariates. In unweighted and weighted models, the discount eligibility (RD estimate) was associated with significantly higher prevalence of dental treatment visits and dental checkup visits during the past 12 mo. In the unweighted models, discount eligibility increased the odds of treatment and checkup visits in the past 12 mo, with ORs of 1.36 (95% CI, 1.32 to 1.40) and 1.49 (95% CI, 1.44 to 1.54), respectively. The effect of discount eligibility appeared to be slightly higher in triangular weighted models. Being female and having more teeth were strong predictors of treatment visits and checkup visits, irrespective of the effect of discount eligibility. The highest-income group was more likely to have attended checkup visits during past 12 mo as compared with the lowest-income group (unweighted model: OR, 1.18 [95% CI, 1.03 to 1.34]; weighted model: OR, 1.13 [95% CI, 0.98 to 1.30]).
Results of Logistic Regression Models Predicting Dental Visits during Past 12 mo: Estimated Effect of JUHI Discount Eligibility.
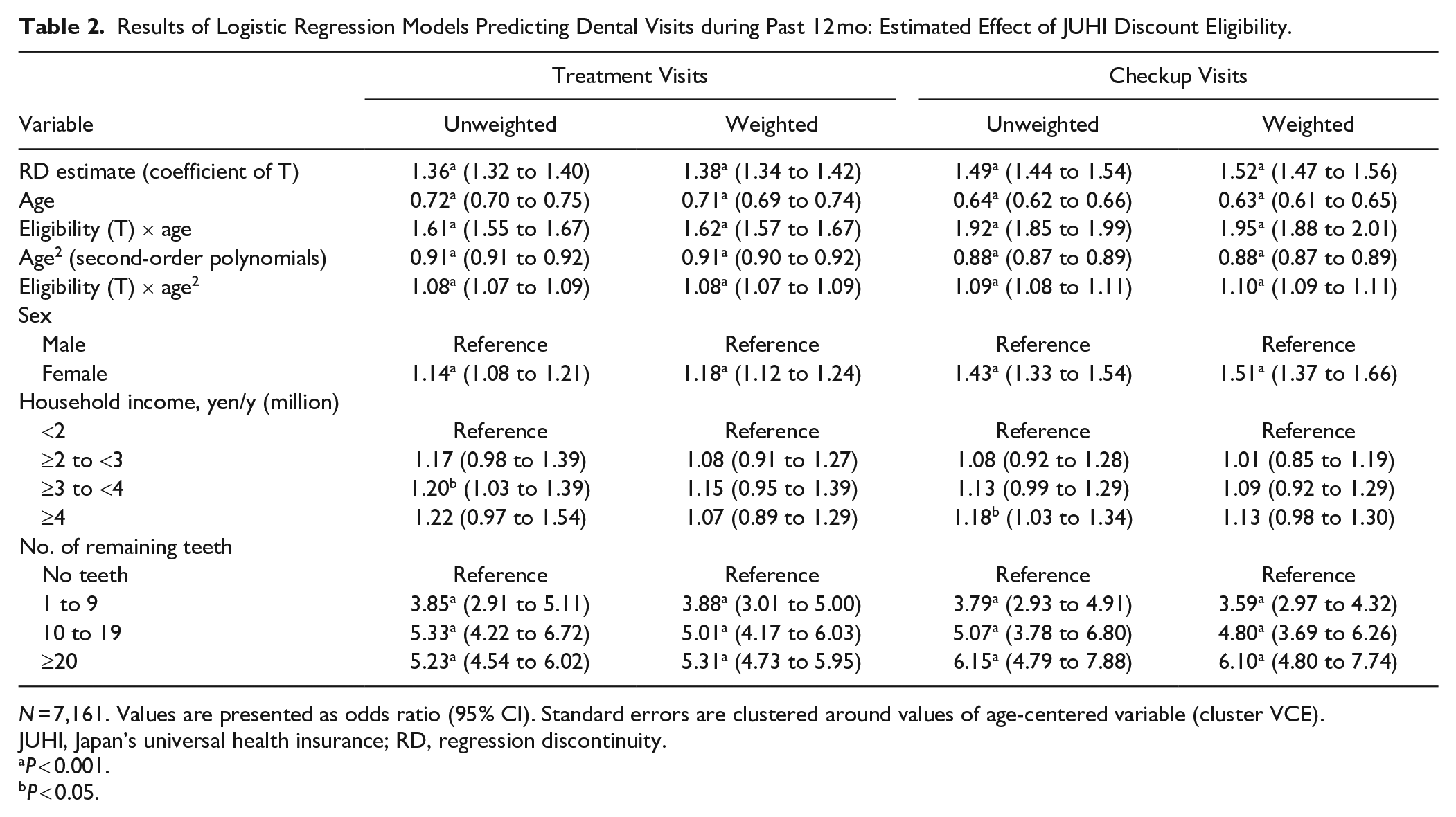
N = 7,161. Values are presented as odds ratio (95% CI). Standard errors are clustered around values of age-centered variable (cluster VCE).
JUHI, Japan’s universal health insurance; RD, regression discontinuity.
P < 0.001.
P < 0.05.
Means of predicted probabilities of dental visits during the past 12 mo for each age were plotted with second-order polynomial fit lines (Fig. 2). Plots related to treatment and checkup visits showed clear discontinuities in the probability of visits during the past 12 mo, before and after the discount-eligible age cutoff.
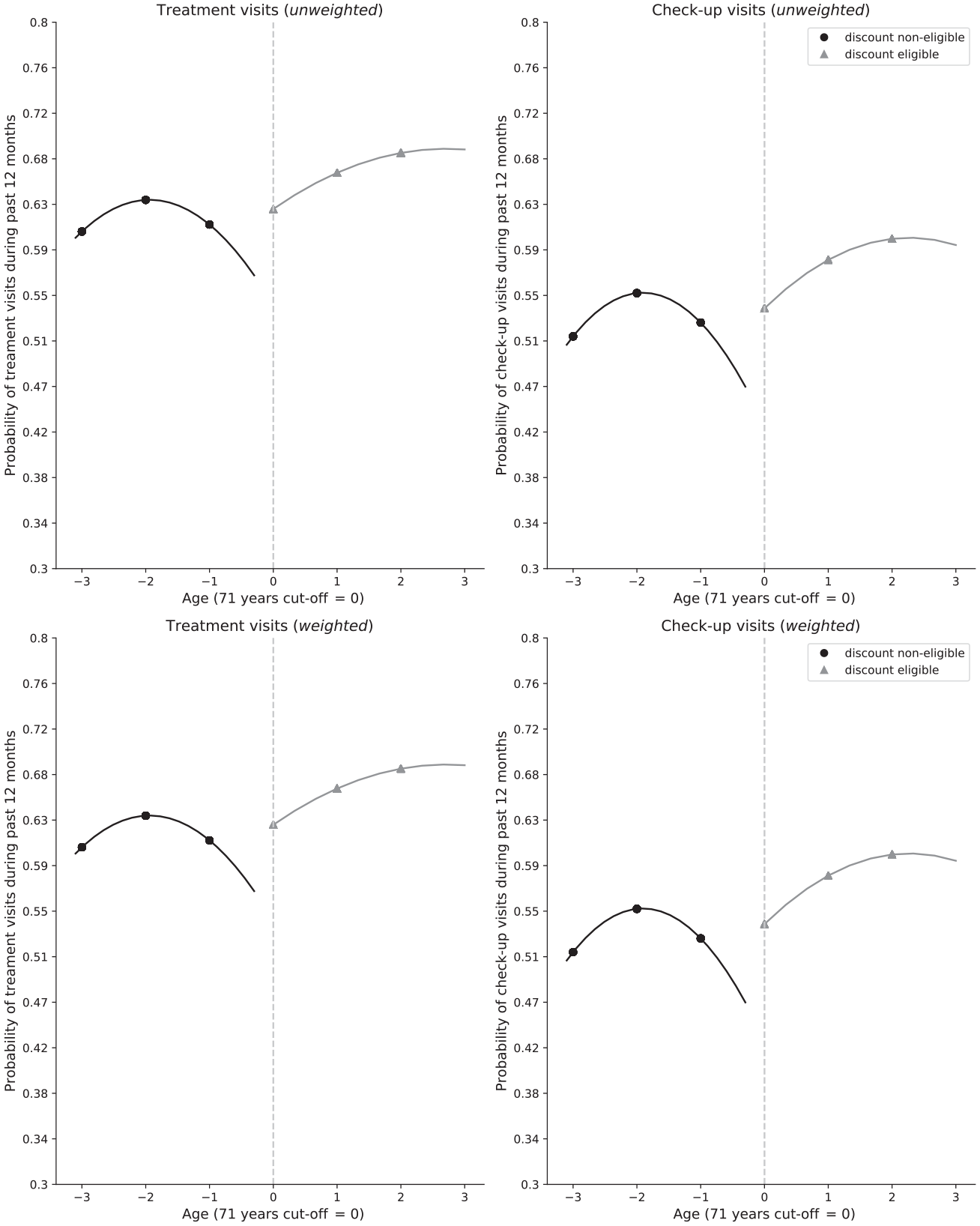
Discontinuity in the probability of dental visits during the past 12 mo before and after the discount eligibility. Means of probability of dental attendance during the past 12 mo for each age are plotted with second-order polynomial fit lines.
Discussion
To the best of our knowledge, this study is the first to determine the effect of cost burden on dental attendance with a quasi-experimental method. We examined the impact of JUHI discount eligibility on dental attendance within a population of Japanese adults to identify how a cost-related policy could influence UHC in oral health. The findings of our study suggest that a higher proportion of Japanese older adults in the 71- to 73-y age group used dental services in the last 12 mo as compared with the 68- to 70-y-old group. RD analysis revealed that the copayment reduction at the age of 70 y significantly contributed toward this higher prevalence of dental service use among older adults aged 71 to 73 y. Furthermore, the effect of the discount appeared to be slightly higher for dental checkup visits than dental treatment visits. Our findings are consistent with the findings of Shigeoka (2014) and Fukushima et al. (2016) regarding the effect of copayment reduction on utilization of inpatient and outpatient medical services in Japan.
There are several strengths and limitations in this study. To determine the relationship between cost burden and dental attendance, the RD method is one of the best approaches for causal inference, as a randomized controlled trial is not feasible (Berk et al. 2010; Leeuwen et al. 2018). The health care setting in Japan is uniquely favorable to the use of the RD method, as most dental treatments are covered by universal health care insurance and the amount of copayments do not vary under this scheme. Hence, we were able to implement the RD method with confidence to isolate the effect of copayment reduction on dental attendance. The RD method could plausibly account for unmeasured confounders between the discount-eligible and noneligible groups, as they are assigned via a deterministic function of age—specifically, within a narrow range (68 to 73 y).
A limitation of the study was that our data did not contain birthdays or age in months; therefore, we were not able to identify the exact point at which participants became eligible for the discount. Thus, we used age of 71 y at the time of the survey as the cutoff for discount eligibility rather than the actual eligible age of 70 y, as we were referring to past dental visits in cross-sectional data. However, this bias possibly attenuates rather than overestimates the impact of discount eligibility on dental attendance. Although current welfare benefit receivers were excluded from the analyses, the history of welfare benefit receipts was not available in the data and thus could not be accounted for. Nevertheless, any bias caused by the inclusion of participants with a history of welfare benefit receipt would have underestimated the effect of the copayment discount, because those who received welfare benefits would not have been expected to change their attendance behavior based on the discount. Another inherent problem of RD designs related to payment policies is the anticipatory behavior of participants. That is, when people anticipate a discount in the near future, they tend to wait until they become eligible (Fig. 2). This anticipatory behavior might lead to an overestimation of the effect of discount eligibility. However, we believe that the 3-y bandwidth that we applied was long enough to reduce potential bias from anticipatory behavior relating to dental attendance. In fact, although the effect of bias from anticipatory behavior could be stronger in the triangular kernel-weighted RD model, the difference between unweighted and weighted estimates was small. Finally, we chose not to undertake sex-stratified analysis due to the limited sample size and instead performed pooled analyses controlling for sex. Previous research reported that denture utilization with respect to the reduction of the copayment in Japan was high for women but close to zero for men (Ando and Takaku 2016). However, our analyses suggested that although women utilized significantly more dental services than men, the effect of copayment reduction was consistent between the sexes, further supporting the aforementioned analytic choice.
Income is one of the most consistent predictors of dental attendance (Listl et al. 2014). In our study, we observed a statistically significant variation in dental checkup visits between the lowest and the highest household income groups. Our findings also suggest that dental checkup visits may be more sensitive to copayment reduction than treatment visits. Dental treatment visits may be associated with emergency care, whereas dental checkups are indicative of a more routine pattern of attendance and a more preventive approach. Therefore, treatment visits may be less affected by cost and may have a lower price elasticity than preventive visits. In fact, a previous study in Japan reported that preventive dental visits were more affected by the income of participants than curative treatment (Murakami et al. 2014). These results suggest that higher copayment could reduce primarily preventive rather than treatment dental visits. These discrete findings might not be generalizable to other countries, as dental attendance behavior would greatly be affected by the country context of the oral health care system. In Japan, 78% of dental care costs were covered by the public insurance (OECD 2019). This percentage was the highest among OECD countries. Therefore, in countries with lower public insurance coverage for dental care, the effect of changes in copayment would be smaller. However, the cost of services has repeatedly been shown to be one of the main barriers to dental attendance in many countries (Donaldson et al. 2008; Thompson et al. 2014; Vujicic et al. 2016).
Our findings have clear policy implications. Globally Japan is considered one of the best countries regarding dental care coverage in UHC, with one of the lowest out-of-pocket dental expenditures (OECD 2011) and the most frequent annual dental visits among all OECD countries (OECD n.d.). This study indicates that dental care access is affected by the level of copayment even in Japan. Regardless of the good coverage, there are social inequalities in access to dental care in Japan (Murakami et al. 2014; Nishide et al. 2017). Therefore, actions to improve universal coverage for dental care should focus on reducing the cost and tackling the underlying inequalities. In addition, the present study shows that copayments disproportionately affect preventive care. Hence, reducing copayments would potentially improve oral health service utilization and help to reorient oral health care from being “treatment oriented” to “prevention oriented.” A prevention-oriented oral health UHC system could benefit more people in terms of access to dental services in Japan. However, our study merely investigated if the copayment reduction was meaningful in terms of dental attendance. While a service-related outcome in its own right, dental attendance is one—but clearly not the only—predictor of good oral health in older adults. It is important to study whether the cost reductions translate into meaningful improvements in oral health. Furthermore, future research could investigate the effect of the cost as compared with other known predictors of dental attendance, such as dental anxiety, attitudes toward oral health, and availability and accessibility of services.
Conclusion
Older adults in Japan attend dental services in higher proportions after the reduction of copayments. After controlling for number of teeth, household income, and sex, the copayment reduction at the age of 70 significantly improved dental attendance. Cost elasticity for preventive dental visits seems to be higher than for treatment visits.
Author Contributions
U. Cooray, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; J. Aida, contributed to conception, design, data acquisition, and interpretation, critically revised the manuscript; R.G. Watt, G. Tsakos, contributed to data interpretation, critically revised the manuscript; A. Heilmann, contributed to design, drafted and critically revised the manuscript; H. Kato, contributed to data analysis, critically revised the manuscript; S. Kiuchi, contributed to conception and design, critically revised the manuscript; K. Kondo, contributed to data acquisition, critically revised the manuscript; K. Osaka, contributed to conception, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_0022034520946022 – Supplemental material for Effect of Copayment on Dental Visits: A Regression Discontinuity Analysis
Supplemental material, DS_10.1177_0022034520946022 for Effect of Copayment on Dental Visits: A Regression Discontinuity Analysis by U. Cooray, J. Aida, R.G. Watt, G. Tsakos, A. Heilmann, H. Kato, S. Kiuchi, K. Kondo and K. Osaka in Journal of Dental Research
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants in the JAGES 2016 survey.
A supplemental appendix to this article is available online.
JAGES 2016 was supported by a JSPS KAKENHI Grant (Japan Society for the Promotion of Science; JP15H01972), a Health Labour Sciences Research Grant (H28-Choju-Ippan-002, H30-Junkankitou-Ippan-004, 19FA2001), the Japan Agency for Medical Research and Development (JP17dk0110017, JP18dk 0110027, JP18ls0110002, JP18le0110009, JP19dk0110034, JP19 dk0110037), the Open Innovation Platform with Enterprises, Research Institute and Academia (JPMJOP1831) from the Japan Science and Technology, and the Research Funding for Longevity Sciences from the National Center for Geriatrics and Gerontology (29-42, 30-22). U. Cooray is supported by a Japanese Government Scholarship (MEXT).
The authors received no financial support and declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Data Accessibility Statement
All data used are from the JAGES 2016 survey. Data requests can be addressed to the JAGES data management committee via email:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.