
Abstract
Tooth loss is prevalent in older adults and associated with functional capacity decline. Studies on the susceptibility of some individuals to the effects of tooth loss are lacking. This study aimed to investigate the heterogeneity of the association between tooth loss and higher-level functional capacity in older Japanese individuals employing a machine learning approach. This is a prospective cohort study using the data of adults aged ≥65 y in Japan (N = 16,553). Higher-level functional capacity, comprising instrumental independence, intellectual activity, and social role, was evaluated using the Tokyo Metropolitan Institute of Gerontology Index of Competence (TMIG-IC). The scale ranged from 0 (lowest function) to 13 (highest function). Doubly robust targeted maximum likelihood estimation was used to estimate the population-average association between tooth loss (having <20 natural teeth) and TMIG-IC total score after 6 y. The heterogeneity of the association was evaluated by estimating conditional average treatment effects (CATEs) using the causal forest algorithm. The result showed that tooth loss was statistically significantly associated with lower TMIG-IC total scores (population-average effect: −0.14; 95% confidence interval, −0.18 to −0.09). The causal forest analysis revealed the heterogeneous associations between tooth loss and lower TMIG-IC total score after 6 y (median of estimated CATEs = −0.13; interquartile range = 0.12). The high-impact subgroup (i.e., individuals with estimated CATEs of the bottom 10%) were significantly more likely to be older and male, had a lower socioeconomic status, did not have a partner, and had poor health conditions compared with the low-impact subgroup (i.e., individuals with estimated CATEs of the top 10%). This study found that heterogeneity exists in the association between tooth loss and lower scores on functional capacity. Implementing tooth loss prevention policy and clinical measures, especially among vulnerable subpopulations significantly affected by tooth loss, may reduce its burden more effectively.
Introduction
Over the past few decades, the difference between life expectancy and healthy life expectancy has grown (GBD 2017 DALYs and HALE Collaborators 2018; World Health Organization 2020). The United Nations has declared 2021 to 2030 as the decade of healthy aging and has prioritized optimizing the functional capacity of the older population, including basic needs and other higher-level competence (World Health Organization 2020). A hierarchical model for the functional capacity of older people has been proposed, wherein the higher-level activities, including instrumental self-maintenance and social roles, generally require greater complexity and neuropsychological cooperation than the lower-level activities, such as life maintenance and functional health (Lawton and Brody 1969).
Studies have revealed that tooth loss affects functional capacity (Tsakos et al. 2015; Sato et al. 2016) and mortality (Koka and Gupta 2018), whereas natural teeth retention in older age is associated with a shorter life duration living with disabilities (Matsuyama et al. 2017). The causation is supported by a natural experiment study that reported that retaining natural teeth reduced the probability of having a limitation in higher-level functional capacity (Matsuyama et al. 2021). Tooth loss is a prevalent oral condition among older adults, with 30% of those aged ≥70 y reportedly edentulous in 2019 (Global Burden of Disease Collaborative Network 2020). Therefore, tooth loss contributes substantially to overall population longevity (Nakazawa et al. 2023). Preventing tooth loss could significantly help promote healthy aging as oral diseases are mostly preventable.
Previous studies investigated the association between oral and general health outcomes and mainly estimated the average effect of oral health, adjusting for study participant characteristics with a conventional regression analysis. This method implicitly assumes a consistent magnitude of the effect across levels of adjusted characteristics, which ignores potential heterogeneity in the influence of oral health across individuals. For instance, oral health problems have a greater effect on general self-rated health for adults with health problems (Brennan and Teusner 2015).
Identifying characteristics that modify the impact of oral health can provide valuable insights into which subpopulations benefit most from policy or clinical interventions, which can inspire efficient resource allocations and more targeted interventions that produce better outcomes (Inoue, Athey, and Tsugawa 2023). Traditionally, researchers have prespecified only a few, usually only 1, potential effect modifiers and performed regression modeling using interaction terms between the exposure and each of these potential modifiers separately. This approach makes it difficult to evaluate complex and high-dimensional effect heterogeneity induced by combinations of multiple effect modifiers (e.g., intersections of age, gender, and socioeconomic status). Recent developments in machine learning algorithms allowed us to consider heterogeneity by combinations of various potential effect modifiers (Athey and Wager 2019; Athey et al. 2019; Inoue, Seeman, et al. 2023; Shiba et al. 2023). However, no study has comprehensively assessed heterogeneity between oral condition and older adults’ health using the data-adaptive approach. We hypothesized that the association between tooth loss and functional capacity varies by the characteristics of individuals. The present study aimed to reveal the sources of this heterogeneity among older adults in Japan.
Methods
Study Participants
This prospective cohort study used data from the Japan Gerontological Evaluation Study (JAGES) in 2010, 2013, and 2019. JAGES is an ongoing large-scale cohort study of functionally independent older adults aged ≥65 y in Japan (Kondo et al. 2018). A total of 112,123 individuals in 31 municipalities completed the 2010 survey (response rate = 66.3%). Of the 31 municipalities, 17 participated in the 2013 and 2019 follow-up surveys. Among the respondents to the 2010 survey, 58,369 resided in the 17 municipalities, including 39,810 and 16,553 individuals who followed up in the 2013 and 2019 surveys, respectively; the follow-up rates were 68.2% for 2013 and 28.4% for 2019 from the 2010 survey. The present study used the data of the 16,553 participants. As shown in Appendix Table 1, these participants were younger, met friends more frequently, and had higher education, higher income, partners, better health conditions, and higher functional capacity than the respondents to the 2010 survey. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Functional Capacity
Functional capacity in 2010 and 2019 was assessed using the Tokyo Metropolitan Institute of Gerontology Index of Competence (TMIG-IC) (Koyano et al. 1991), which comprises 13 items on higher-level functional capacity regarding instrumental independence (5 items; e.g., “Can you go out alone by train or bus?”), intellectual activity (4 items; e.g., “Can you complete the paperwork for your pension, etc., by yourself?”), and social role (4 items; e.g., “Do you visit your friends’ homes?”). This study used the total score ranging from 0 (lowest function) to 13 (highest function) as the primary outcome and the 3 subscales as the secondary outcomes.
Tooth Loss
The following question assessed the participants’ number of remaining teeth in 2013: “How many natural teeth do you have?” The respondents answered with 1 of the 5 options: 0, 1 to 4, 5 to 9, 10 to 19, and ≥20 natural teeth. The variable was dichotomized into having <20 natural teeth (coded 1) and having ≥20 natural teeth (coded 0). A clinical dental examination in a previous study has validated the self-reported measurement of the number of teeth in older people (Sekundo et al. 2019).
Covariates
This study used the following variables assessed in 2010 (i.e., prebaseline) as covariates: age, sex, years of education, equivalent household income, marital status, frequency of meeting friends, body mass index (BMI), smoking status, self-rated health, depressive symptoms assessed with the Geriatric Depression Scale (Sheikh and Yesavage 1986), comorbid conditions (heart disease, hypertension, and diabetes), and TMIG-IC total score. Additionally, the following variables on oral functions assessed in 2013 were included: decline in chewing ability in the last 6 mo, choking, oral dryness, and use of dental prosthesis. Table 1 shows the categories for each variable.
Demographic Characteristics of the Participants (N = 16,553).
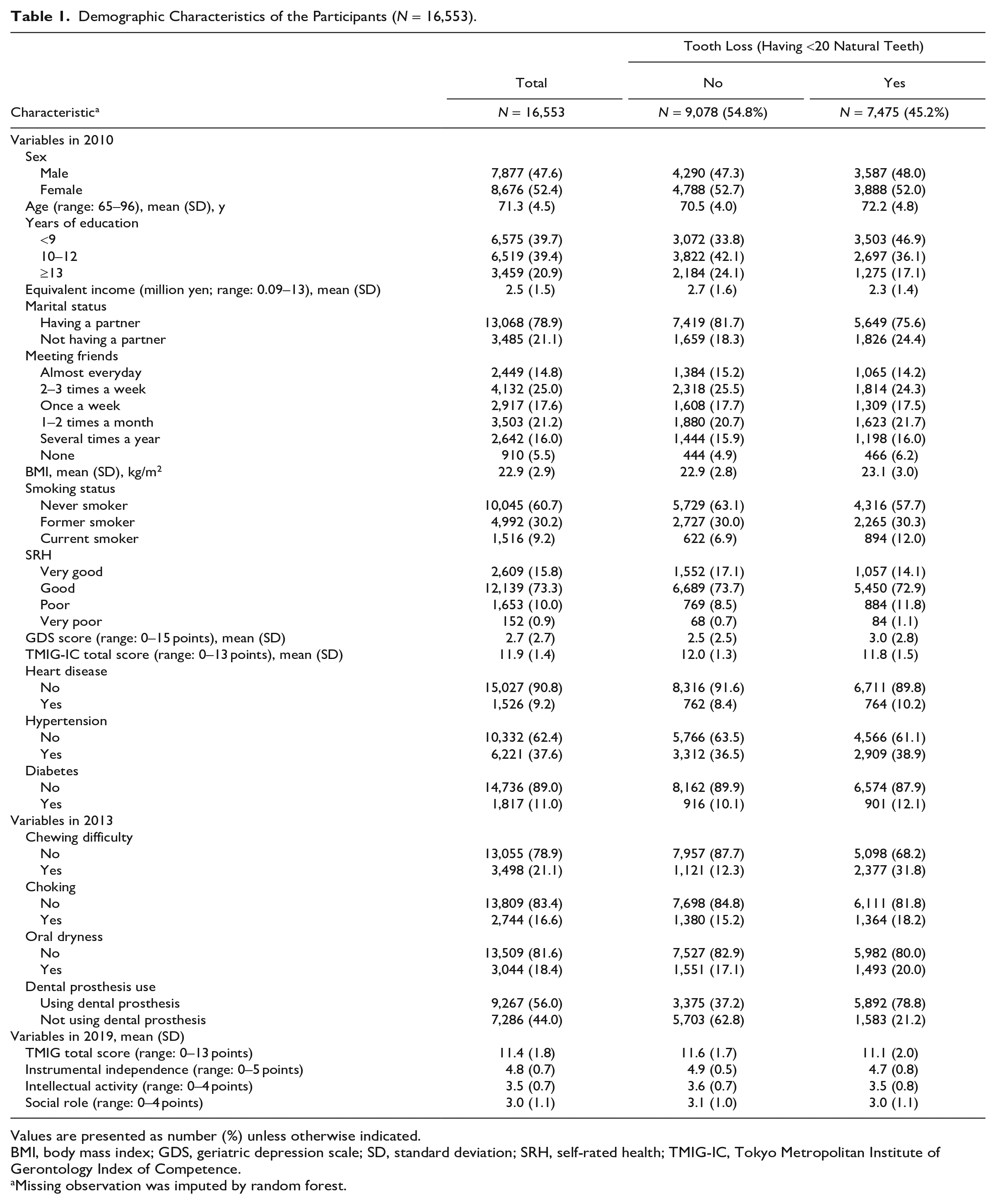
Values are presented as number (%) unless otherwise indicated.
BMI, body mass index; GDS, geriatric depression scale; SD, standard deviation; SRH, self-rated health; TMIG-IC, Tokyo Metropolitan Institute of Gerontology Index of Competence.
Missing observation was imputed by random forest.
Statistical Analysis
A summary of our analytic procedure is presented in the Appendix Method. First, we estimated the average treatment effect (ATE) of tooth loss on functional capacity using targeted maximum likelihood estimation (TMLE), which is a doubly robust estimator that combines outcome regression and inverse-probability weighting methods, thereby reducing the bias due to model misspecification (Schuler and Rose 2017). To further reduce the risk of model misspecification, the models were fitted data-adaptively via the SuperLearner ensemble machine learning algorithm (Polley et al. 2017). We used generalized linear models, gradient boosting models, and neural networks as candidate algorithms. The R packages ltmle and SuperLearner were used for this analysis (Polley et al. 2017; Schwab et al. 2020).
Second, we examined the heterogeneity of the association between tooth loss and functional capacity by estimating conditional average treatment effect (CATE), an average effect of the exposure conditional on the values of a vector of covariates. To estimate CATEs, we used the causal forest approach from the generalized random forest (GRF) algorithm (Athey et al. 2019). The details of the GRF algorithm are reported elsewhere (Athey and Wager 2019; Athey et al. 2019; Inoue, Seeman, et al. 2023; Shiba et al. 2023). In brief, the causal forest approach is built upon the idea of the random forest, but the prediction target is the effect of the exposure on the outcome rather than the outcome itself. It constructs several regression trees by partitioning bootstrapped subsamples into a leaf (i.e., strata defined by the same covariate combinations) and estimates the average exposure effect within the leaf (i.e., CATEs). The present study divided the data into 20 folds and made predictions for each fold from trees trained without using the fold. Parameters were tuned via cross-validation before growing 2,000 regression trees. The R package grf was used for this analysis (Tibshirani et al. 2022).
Third, the model performance of GRF was evaluated by sorted group average treatment effects and best linear predictor analysis (Chernozhukov et al. 2018; Athey and Wager 2019). The Appendix Method describes this procedure.
Fourth, we identified the bottom and top 10 percentile of individuals based on the magnitude of estimated CATEs. The estimated CATEs were mostly negative, and larger absolute values of CATEs indicate more substantial adverse impacts. Therefore, we categorized those in the bottom 10th percentile as the “high-impact subgroup.” Conversely, those in the top 10th percentile were classified as the “low-impact subgroup.” We then compared the distribution of covariates between these 2 groups to investigate potential factors contributing to the heterogeneity of the estimated CATEs. We also summarized the estimated CATEs by subgroups based on those factors.
Missing data in all variables were imputed by random forest imputation with the R package missForest (Stekhoven 2022). Appendix Table 2 shows the frequency of missing information on variables. We performed TMLE and GRF analyses using R version 4.2.2. Other descriptive analyses and plotting were done using Stata MP version 18 software.
Ethical Considerations
The ethics committees at Nihon Fukushi University (Nos. 10-05 and 13-14), Chiba University (No. 3442), National Center for Geriatrics and Gerontology (No. 1274-2), and Japan Agency for Gerontological Evaluation Study (No. 2019-01) approved the procedures for JAGES surveys.
Results
Demographic Characteristics of the Study Participants
Table 1 describes the demographic characteristics of the study population (mean age: 71.3 y; male: 47.6%). Of the study participants, 45% had <20 natural teeth. Participants with <20 natural teeth were older and unmarried, met friends less frequently, and had lower socioeconomic backgrounds, smoking experience, higher depressive symptoms, poor self-rated health, comorbid conditions, poor oral functions, and lower TMIG-IC scores at the prebaseline wave compared to those with ≥20 natural teeth.
Estimation of Population Average Treatment Effects
Figure 1 depicts the estimated ATEs of tooth loss on the functional capacity outcomes. The result revealed that tooth loss was, on average, associated with lower TMIG-IC total scores after 6 y (estimate = −0.14; 95% confidence interval [CI], −0.18 to −0.09). Furthermore, tooth loss was associated with lower scores on the instrumental independence subscale (estimate = −0.05; 95% CI, −0.07 to −0.03) and intellectual activity subscale (estimate = −0.08; 95% CI, −0.10 to −0.06) but not on the social role subscale (estimate: 0.00; 95% CI, −0.03 to 0.03).
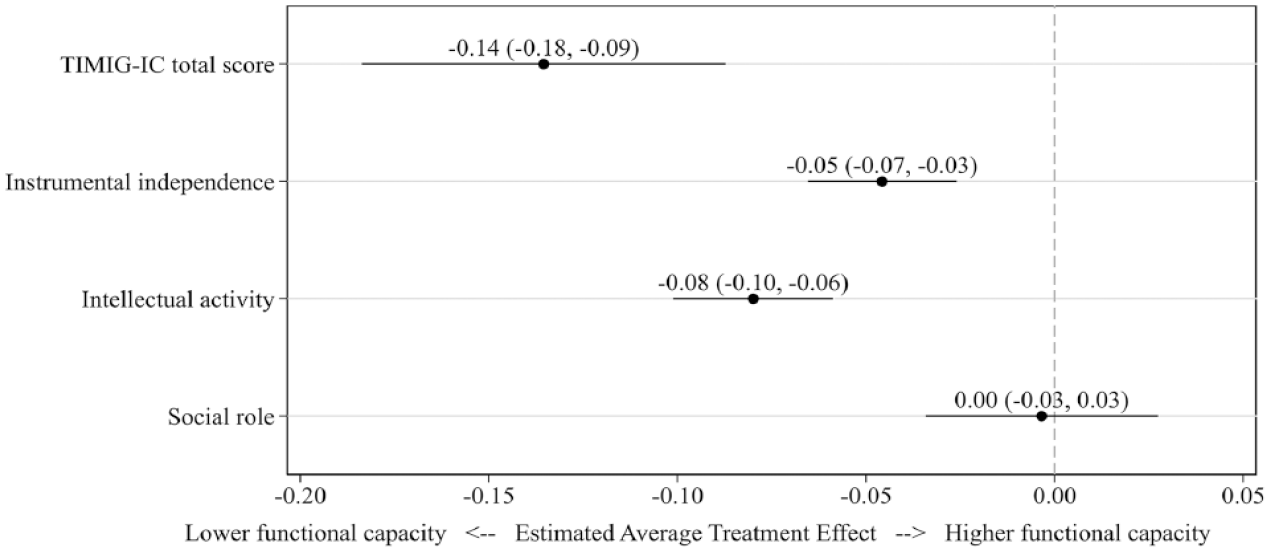
Estimated population-average effect (ATE) of tooth loss on functional capacity. The ATEs and confidence intervals were estimated with the doubly robust targeted maximum likelihood estimation. Models were estimated data-adaptively via the SuperLearner with generalized linear models, gradient boosting machine, and neural net as candidate estimators. All models adjusted for the preexposure demographic and socioeconomic factors and health conditions and oral functions in the survey assessing tooth loss. The functional capacity outcome was measured by the 13-item Tokyo Metropolitan Institute of Gerontology Index of Competence (range: 0–13), and the subscales included instrumental independence (range: 0–5), intellectual activity (range: 0–4), and social role (range: 0–4), wherein a smaller score represents lower functional capacity. Thus, a decrease in these outcomes (left side on the x-axis) indicates lower functional capacity.
Estimation of Conditional Average Treatment Effects
Figure 2A presents the distribution of estimated CATEs for the nonstandardized association between tooth loss and functional capacity after 6 y. The estimated CATEs had widespread distributions for the TMIG-IC total scores (median = −0.13; interquartile range [IQR] = 0.12) and intellectual activity (median = −0.08; IQR = 0.06), whereas the distribution was narrower for instrumental independence (median = −0.05; IQR = 0.01) and social role (median = −0.01; IQR = 0.02). After standardizing CATEs to account for the difference in possible score ranges across the outcomes (Fig. 2B), the distribution of estimated CATEs for total scores became narrower; however, the notable heterogeneity persisted in the total score and intellectual activity subscale.
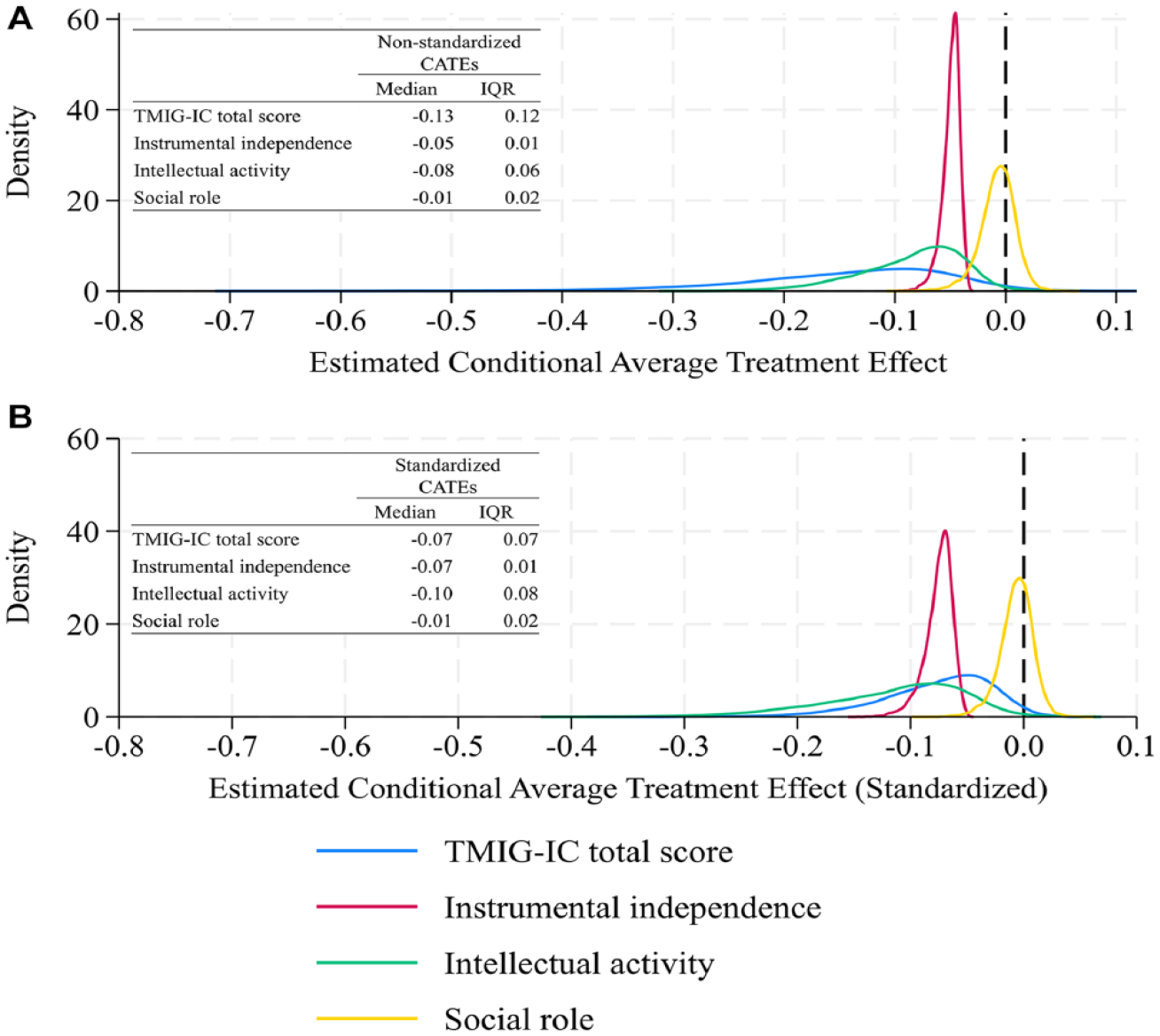
Distributions of estimated conditional average treatment effect (CATEs) of tooth loss on functional capacity. The estimates are shown in raw (
Model Performance Evaluation
Figure 3 shows the sorted group average treatment effects for subgroups categorized based on estimated CATEs below or above the median (i.e., high-impact 50% and low-impact 50%). The estimated ATE of tooth loss on TMIG-IC total score and intellectual activity subscale were significantly greater for the high-impact 50% subgroup than the low-impact 50% subgroup (the estimated difference [95% CI]: −0.15 [−0.26 to −0.04] for total score and −0.07 [−0.13 to −0.01] for intellectual activity). In contrast, the differences in estimated subgroup-specific ATEs were small for the instrumental independence and social role subscales, and the differences were not significant (the estimated difference [95% CI]: 0.01 [−0.04 to 0.06] for instrumental independence and −0.01 [−0.07 to 0.04] for the social role).
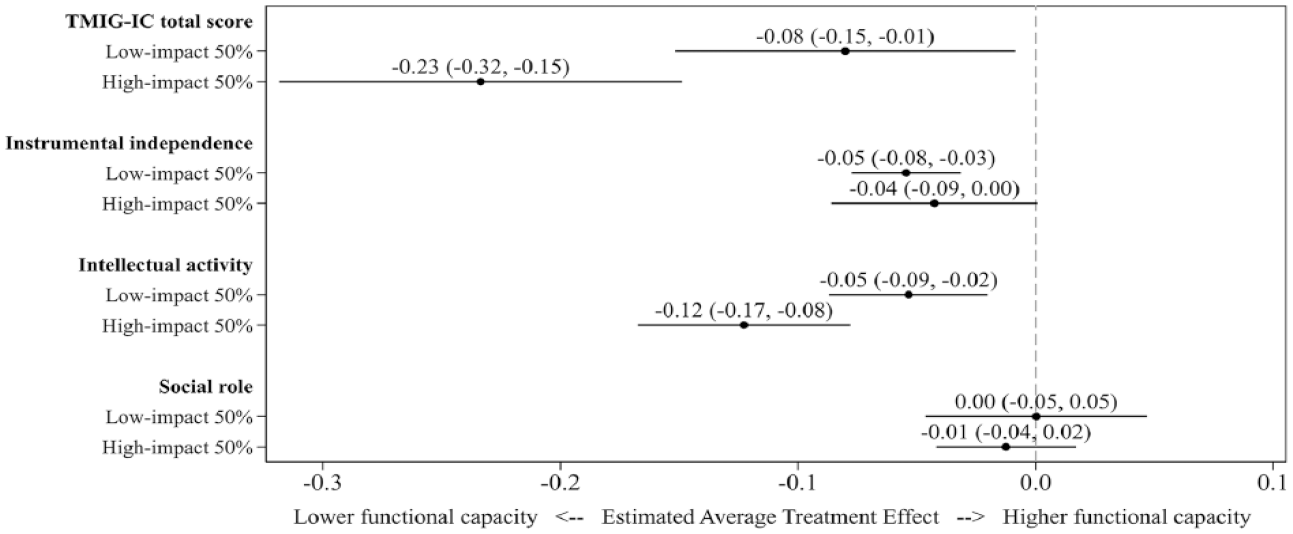
Sorted group average treatment effects (ATE) by 2 groups: The study population was categorized based on their conditional ATEs below or above the median. The ATEs and confidence intervals were estimated via the doubly robust augmented inverse-probability weighting estimation. Models were estimated data-adaptively via the SuperLearner using generalized linear models, gradient boosting machine, and neural net as candidate estimators. All models adjusted for the preexposure demographic and socioeconomic factors and health conditions and oral functions in the survey assessing tooth loss. The functional capacity outcome was measured by the 13-item Tokyo Metropolitan Institute of Gerontology Index of Competence (range: 0–13), and the subscales included instrumental independence (range: 0–5), intellectual activity (range: 0–4), and social role (range: 0–4), wherein a smaller score represents lower functional capacity. Thus, a decrease in these outcomes (left side in the x-axis) indicates lower functional capacity.
The estimated subgroup-specific ATEs monotonically increased as the CATE quintile ranking increased for all outcomes except for the social role subscale (Appendix Fig. 1). The best linear predictor analysis suggested that the models were well calibrated, especially for TMIG-IC total score, instrumental independence, and intellectual activity subscales, and that the model captured the heterogeneity for the total score (P = 0.056) and intellectual activity subscale (P < 0.001) (Appendix Table 3).
Comparison of Characteristics between Low- and High-Impact Subgroups
Table 2 highlights the demographic characteristics of the low- and high-impact subgroups based on the estimated CATE distribution for the TMIG-IC total scores. Participants in the subgroup with a greater magnitude of estimated CATEs (i.e., high-impact subgroup) included more males, were older, did not have a partner, were not diabetic, met friends less frequently, and had lower education, lower income, lower BMI, poor self-rated health, higher depressive symptoms, and lower functional capacity in 2010 and used dental prosthesis and had poor oral functions in 2013.
Demographic Characteristics of Cases with Extreme Conditional Average Treatment Effects (CATEs) on TMIG Total Score.
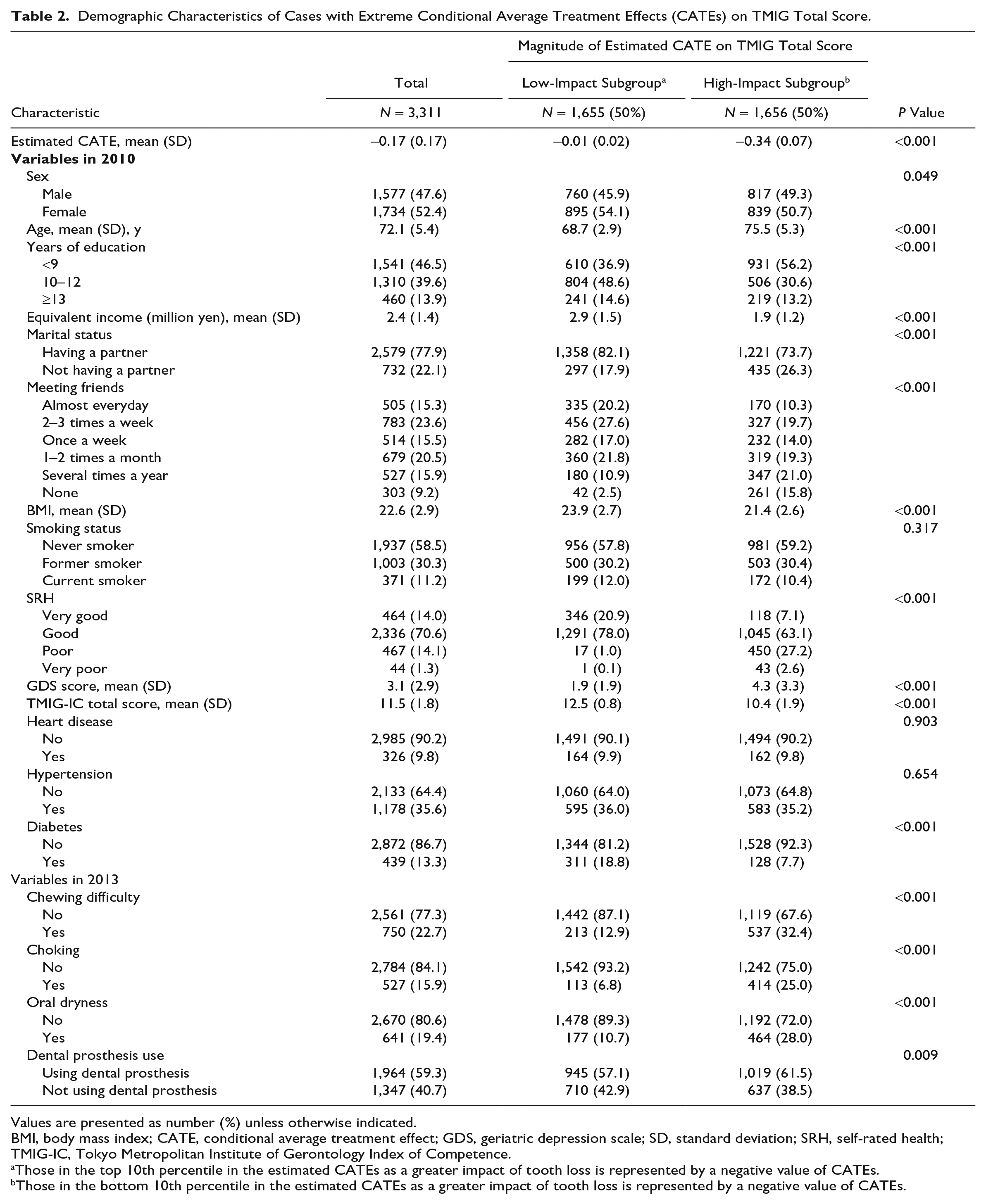
Values are presented as number (%) unless otherwise indicated.
BMI, body mass index; CATE, conditional average treatment effect; GDS, geriatric depression scale; SD, standard deviation; SRH, self-rated health; TMIG-IC, Tokyo Metropolitan Institute of Gerontology Index of Competence.
Those in the top 10th percentile in the estimated CATEs as a greater impact of tooth loss is represented by a negative value of CATEs.
Those in the bottom 10th percentile in the estimated CATEs as a greater impact of tooth loss is represented by a negative value of CATEs.
Participants in the high-impact subgroup based on the estimated CATEs for the intellectual activity subscale, which demonstrated a better model performance than the other 2 subscales, were older, did not have a partner, met friends less frequently, did not use dental prosthesis, and had lower education, lower income, lower BMI, and poor health conditions compared with those in the low-impact subscale (Appendix Table 4). Regarding the instrumental independence and social role subscales, which demonstrated poor model performance, the participants in the high-impact subgroup for instrumental independence were older, males, did not have a partner, met friends less frequently, did not use dental prosthesis, and had lower education, lower income, lower BMI, smoking experience, and poor mental and physical health conditions compared with those in the low-impact subgroup (Appendix Table 5). The difference in characteristics between high- and low-impact subgroups was less remarkable regarding the social role subscale (Appendix Table 6).
As a post hoc analysis, we estimated CATEs by gender, marital status, self-rated health, age group, and household income (Appendix Table 7). The result was consistent with the observed pattern in Table 2; for example, the mean estimated CATEs on the TMIG-IC total scores were greater in magnitude among subgroups characterized by older age, male gender, lower socioeconomic status, not being married, and lower health status.
Discussion
This study revealed that, on average, having <20 natural teeth was associated with a decline in TMIG-IC total score, instrumental independence, and intellectual activity. However, no evidence supported the population-average association with the social role. The TMIG-IC total score demonstrated heterogeneity in the association across individuals. Individuals with greater estimated effects of tooth loss on the outcome were older and male, had lower socioeconomic status, did not have a partner, and had poor health conditions.
Reportedly, 4.1% of the global population is edentulous (Kassebaum et al. 2017), and oral diseases account for a 5.3% loss of quality-adjusted life years due to morbidity (Matsuyama et al. 2019). The present study revealed varying effects of tooth loss by individual characteristics, indicating that policy and clinical measures to prevent tooth loss in the high-impact subpopulation may result in a more effective reduction of the burden associated with tooth loss. The high-impact subpopulation shared risk factors for other health conditions, such as older age and lower socioeconomic status. Therefore, prioritizing them in health policy would also reduce health inequalities.
To our knowledge, this study is the first to explore high-dimensional effect modification in the association between oral and general health outcomes using a data-adaptive approach. This approach addresses limitations in traditional interaction analyses, where researchers typically prespecify a limited number of potential effect modifiers. Meanwhile, this study has limitations. First, the characteristics of high- and low-impact subgroups identified by the GRF analysis do not necessarily represent causal interaction, which requires an additional identification assumption (VanderWeele and Knol 2014). Thus, manipulating the effect modifiers may not necessarily change the impact of tooth loss on the decline in functional capacity. Second, the conditional exchangeability assumption based on the covariates must hold for the causal interpretation. Residual confounding is possible while adjusting for a rich set of prebaseline covariates. Third, the exposure variable was dichotomized to be included in the GRF analysis, resulting in information loss on the number of natural teeth, although having ≥20 natural teeth is crucial for sufficient chewing ability (Steele et al. 1997) and reported to predict all-cause mortality (Koka and Gupta 2018). In the present study, the number of teeth within each category of having ≥20 or <20 natural teeth would vary, which may violate the consistency assumption. Fourth, all variables were self-reported, making them susceptible to information bias. Fifth, the follow-up rate was relatively low, which may induce selection bias in the result. The respondents to the follow-up surveys were younger and had higher socioeconomic status and better health conditions than the 2010 respondents (Appendix Table 1).
The results regarding ATE of tooth loss on functional capacity align with previous studies. Edentulousness is associated with physical and cognitive decline over 10 y in older adults in England (Tsakos et al. 2015) and predicted a faster decline in functional capacity (Iwasaki and Yoshihara 2021). Having ≥20 natural teeth was associated with a 0.156 higher TMIG-IC total score over 3 y compared to being edentulous (Sato et al. 2016). The present study supports these results using a doubly robust estimator, which reduces the bias due to model misspecification. The null effect on the social role domain contradicts the previous study reporting that having ≥20 natural teeth was associated with increased participation in social activities (Cooray et al. 2023). The TMIG social role subscale, a composite score of 4 items assessing activities such as visiting friends’ homes and conversing with younger people, might be less influenced by having <20 natural teeth.
The present study indicated older age, lower socioeconomic backgrounds, not having a partner, and poor mental and physical health conditions were the factors that characterize the high-impact subgroup. A study revealed that older Chinese adults with fewer natural teeth experienced a more rapid decline in cognitive ability (Chen et al. 2022). People with lower socioeconomic backgrounds often lack resources to mitigate the impact of tooth loss as inequalities exist in access to dental care throughout life (Listl 2012). A study in Japan revealed a higher risk of dementia onset in older adults with few teeth who did not use dentures compared to those with ≥20 teeth; however, the risk was similar between those using dentures and those with ≥20 teeth (Yamamoto et al. 2012). This indicates that dental care may help alleviate the impact of tooth loss on functional capacity decline, which is also supported by the results of the present study, in line with the results that the low-impact subgroup on intellectual activity was more likely to use dental prosthesis (Appendix Table 4). Having a partner provides social support, and losing a partner can accelerate frailty among older people (Oberndorfer et al. 2022). The present study identified these potential effect modifiers that can independently or cumulatively increase the effect of tooth loss. Health conditions that characterize high-impact subgroups differ by the outcome; this inconsistency may be associated with other subpopulation characteristics and the relatively poor model performance on the instrumental independence and social role subscales.
In conclusion, the present study revealed the heterogeneous association between tooth loss and functional capacity decline among older adults in Japan. Subpopulations characterized by older age, male, lower socioeconomic backgrounds, no partner, and poor mental and physical health conditions showed a greater impact on the effect of tooth loss. Such subpopulations need to be prioritized for policy or clinical interventions, which may effectively reduce the burden of oral diseases.
Author Contributions
Y. Matsuyama, contributed to conception, design, data analysis and interpretation, drafted the manuscript; J. Aida, K. Kondo, contributed to conception, data acquisition and interpretation, critically revised the manuscript; K. Shiba, contributed to design, data analysis and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-pdf-1-jdr-10.1177_00220345241226957 – Supplemental material for Heterogeneous Association of Tooth Loss with Functional Limitations
Supplemental material, sj-pdf-1-jdr-10.1177_00220345241226957 for Heterogeneous Association of Tooth Loss with Functional Limitations by Y. Matsuyama, J. Aida, K. Kondo and K. Shiba in Journal of Dental Research
Footnotes
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study used data from JAGES (the Japan Gerontological Evaluation Study). This study was supported by Grant-in-Aid for Scientific Research (20H00557, 20K10540, 21H03153, 21H03196, 21K17302, 22H00934, 22H03299, 22K04450, 22K13558, 22K17409, 22K17285, 23H00449, 23H03117) from JSPS (Japan Society for the Promotion of Science), Health Labour Sciences Research Grants (19FA1012, 19FA1018, 19FA2001, 21FA1012, 21FA1013, 22FA2001, 22FA1010, 22FG2001, 23FA1022), Research Institute of Science and Technology for Society (JPMJOP1831) from the Japan Science and Technology (JST), a grant from Japan Health Promotion & Fitness Foundation, TMDU priority research areas grant, and National Research Institute for Earth Science and Disaster Resilience. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the respective funding organizations.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.