
Abstract
Secondhand smoke (SHS) is a pervasive health concern increasingly associated with tooth loss, yet studies assessing its population-level associations and potential heterogeneity are limited. This study aimed at estimating the average and subgroup-specific effects of SHS exposure on tooth loss among US adults using modern causal inference–based methods. This study analyzed cross-sectional data from 6,019 nonsmokers aged ≥20 y, representing 48.2 million individuals, in the National Health and Nutrition Examination Survey (2009 to 2018). SHS was defined by serum cotinine. This study quantified the association between SHS exposure and tooth loss using targeted minimum loss estimation, a doubly robust estimator that enhances confounding adjustment in observational data. Confidence intervals were obtained via bootstrap resampling. Heterogeneity of the association was evaluated by a data-adaptive causal forest method that identifies subgroup-specific variation. SHS exposure was associated with having 0.74 fewer teeth (average association, −0.739; 95% CI, −1.053 to −0.426) and with a 4.6-percentage higher probability of having <20 teeth (average association, 0.046; 95% CI, 0.027 to 0.065). Larger associations were observed among adults aged ≥45 y, those with lower socioeconomic position, individuals with higher sugar intake or medical comorbidities, and participants at the extremes of flossing frequency. This study found that SHS exposure was associated with greater tooth loss, with disproportionate burdens observed among adults facing socioeconomic disadvantages or chronic health conditions. These findings underscore the potential value of integrating oral health outcomes into tobacco control initiatives and guiding targeted prevention for groups at elevated risk.
Keywords
Introduction
Smoking remains a major global health concern, with well-established detrimental effects on multiple organ systems (Dai et al 2022). Importantly, the harm of tobacco use extends beyond smokers themselves: secondhand smoke (SHS) exposure contributes substantially to the global disease burden (Flor et al 2024). While public health initiatives have made progress in reducing active smoking, SHS continues to pose risks for nonsmokers, particularly vulnerable populations (GBD 2017 Risk Factor Collaborators 2018). Oral health is increasingly recognized as an essential component of overall health and quality of life (Aida 2021), as tooth loss has been linked to malnutrition, weight loss, functional limitations, cardiovascular diseases, and higher mortality (Zelig et al 2022; Kusama et al 2023; Matsuyama et al 2023; Matsuyama et al 2024; Wang et al 2026). The burden of tooth loss also mirrors broader socioeconomic disparities (Mbulo et al 2016).
Accumulating evidence has linked SHS exposure to adverse oral health outcomes, including periodontal disease and dental caries (Sanders and Slade 2013; González-Valero et al 2018), raising concerns that SHS could influence tooth loss (Umemori et al 2020). Yet, despite well-established evidence supporting a causal link between active smoking and tooth loss (Baumeister et al 2025), analogous evidence for SHS remains limited. Most existing studies rely on self-reported measures of SHS and have not examined heterogeneity in the observed associations, thereby limiting their relevance for policy formulation and preventive interventions (Oliveira et al 2022; Luo et al 2025). These limitations are particularly concerning because reliance on self-reported exposure without objective biomarkers and the absence of heterogeneity assessment may lead to exposure misclassification and obscure population subgroups with stronger associations. The World Health Organization’s Oral Health Action Plan 2023–2030 calls for the integration of oral health within national tobacco control efforts, highlighting the importance of clarifying how tobacco exposure, including SHS, affects oral health. Because experimental studies on SHS exposure are ethically infeasible, observational data play a crucial role in advancing understanding of its impact. Recent developments in causal inference methodology provide opportunities to strengthen inference from such data by improving adjustment for confounding and enabling data-adaptive exploration of heterogeneity (Nugent et al 2024). These tools allow researchers to approximate aspects of experimental designs and to identify subgroups who may be disproportionately affected.
To bridge the gap, the present study aimed to evaluate the association between SHS exposure and tooth loss in a nationally representative sample of US adults, using modern causal inference approaches. To our knowledge, this is the first study that leveraged causal inference methods, including targeted minimum loss estimation and causal forest, within the Neyman-Rubin potential outcomes framework to estimate average and heterogeneous treatment effects of SHS on tooth loss. The findings may underscore the value of incorporating oral health into tobacco control efforts and inform public health policies and clinical supports that prioritize high-risk populations.
Materials and Methods
Study Population
The National Health and Nutrition Examination Survey (NHANES) is an ongoing cross-sectional survey that employs complex multistage sampling weights to reflect the national condition. NHANES 2009 to 2018 are the latest consecutive waves that incorporated dentition examination data, from which 8,063 nonsmokers who participated in the survey on household smoking were included. Participants without available data on serum cotinine level and complete dentition examination (n = 2,044) were excluded. Eventually, 6,019 nonsmokers were incorporated for the analytic procedure. The flowchart in Figure 1 illustrates the inclusion strategy.
Workflow of the inclusion criteria. NHANES, National Health and Nutrition Examination Survey.
Measurements of Tooth Loss
A full-mouth dentition examination was performed by calibrated examiners. The third molar was excluded from the tooth count. A permanent tooth present (excluding a permanent root fragment) was considered a “tooth present.” Our primary outcome was total tooth count, which was analyzed as a continuous variable to maximize statistical power (Lopez-Ayala et al 2025). As the secondary analyses, the continuous tooth count was dichotomized into having <20 natural teeth and having at least 20 natural teeth.
Identification of Exposure to SHS and Smoking Status
Participants who were currently smoking or had quit, with histories of smoking >100 cigarettes in their lives, were identified as either current or former smokers, while their counterparts were identified as nonsmokers. Serum cotinine is the primary metabolite of nicotine and is widely accepted as an optimal biomarker for tobacco smoke exposure due to its half-life of approximately 16 to 20 h, which may reflect recent exposure over 1 to 3 d (Benowitz 1996). Thus, the present study identified nonsmokers as being exposed to SHS if their serum cotinine levels were ≥0.05 ng/mL per a previous study (Tsai et al 2021). The alternative definition considered the presence of household smokers based on serum cotinine levels.
Ascertainment of the Confounders
According to existing evidence (Bashir et al 2026), we included the following as potential confounders: sex, age, race, poverty-to-income ratio, educational attainment, weekly dental floss by frequency, daily sugar consumption, body mass index, diabetes, hypertension, and hyperlipidemia. Detailed definitions can be found in Appendix Table 1.
Statistical Analysis
All statistical analyses were performed in R software (version 4.3.0). The modeling assumption was visualized by the directed acyclic graph in Appendix Figure 1. First, a descriptive analysis was performed on all participants. According to the potential outcome framework, the “What if” scenarios hypothesized in this study were as follows: “What if all nonsmokers were exposed to SHS?” and “What if all nonsmokers were not exposed to SHS?” The average treatment effect (ATE) was calculated by the difference in the mean outcome (ie, tooth count) values under the 2 scenarios (Hernan and Robins 2025).
Targeted minimum loss estimator (TMLE) is a doubly robust estimator that combines the outcome model of g-computation and the exposure model of inverse probability weighting and therefore may provide valid estimates where either model holds (Schuler and Rose 2017). We applied the Super Learner ensemble within the TMLE framework, stacking regularized linear regression, extreme gradient boosting (XGBoost), and neural networks. To estimate the nuisance functions, we employed a stratified 10 × 10 cross-validation (Brown et al 2025): for each outer 10-fold used to obtain cross-fitted Q estimates, the Super Learner was tuned on a prespecified hyperparameter grid (Appendix Table 3) in the remaining outer folds via an inner 10-fold cross-validation, in which candidate learners with suboptimal hyperparameters were effectively downweighted (Bodnar et al 2022; Polley et al 2024). This ensemble strategy enhances robustness and mitigates bias from misspecification by leveraging the complementary strengths of diverse algorithms (Moccia et al 2024). ATE was estimated by TMLE in the tmle3 R package (Gruber and Laan 2012; van der Laan 2023); the conditional ATE (CATE) was derived by a causal forest from a generalized random forest algorithm in the grf R package (Athey et al 2019); and hyperparameter was tuned prior to growing 2,000 trees. To avoid overfitting, the data were divided into 5 folds; for each fold, prediction was derived from trees trained by the other 4 folds. Model performance of the generalized random forest was assessed by the group ATE and the best linear predictor analysis (Athey et al 2017; Athey and Wager 2019).
To explore heterogeneity, we employed 2 strategies. First, participants were stratified into different groups based on the interquartile range (IQR) of CATEs. For the tooth count outcome, individuals of a lower percentile of the IQR were those experiencing greater tooth loss from SHS. In contrast, for the dentition status outcome (probability of having <20 teeth), individuals of a lower percentile of the IQR were those who retained more teeth, per the outcome coding (Matsuyama et al 2024). Second, participants were classified into different groups by employing causal distillation tree in the causalDT package, which distills complex heterogeneity from CATEs derived from a generalized random forest and summarizes the subgroups with various treatment effects into a tree structure, offering additional clinical interpretability (Rehill 2024; Huang et al 2025). The optimal maximum tree depth for the student model was based on a Jaccard similarity index. For ATE, the 95% confidence interval (95% CI) was calculated by a bootstrapping method with 1,000 iterations (Tibbe and Montoya 2022), and E value was applied to estimate the residual confounding (VanderWeele and Ding 2017). Specifically, E values were calculated by the formula for linear regression coefficients for the continuous tooth count outcome and the formula for risk differences for dentition status, implemented via a publicly available online calculator (https://www.evalue-calculator.com/evalue/; accessed December 25, 2025). A random forest algorithm was used to complete the missing data in the missForest R package (Tang and Ishwaran 2017). The missing rates and distribution of the missing data are illustrated in Appendix Table 2 and Appendix Figure 2. P < 0.05 was considered statistically significant. The NHANES weight was applied to all analyses per the NHANES guideline. R code used in the study can be found at https://github.com/Jackieyueqi/SHS_tooth. The results were reported following STROBE (Strengthening the Reporting of Observational Studies in Epidemiology).
Sensitivity Analysis
Sensitivity analyses were conducted to evaluate the robustness of the findings by 1) applying alternative serum cotinine thresholds to define SHS; 2) defining SHS by urinary 4-methylnitrosamino-1-3-pyridyl-1-butanol (NNAL), a biomarker of tobacco exposure with a half-life of 10 to 18 d, allowing it to reflect SHS exposure over 4 to 8 wk (Goniewicz et al 2009); 3) completing missing values in the exposure and outcome; and 4) reestimating models without survey weights. More details are provided in the Appendix 2.
Results
Characteristics of Participants
In total, 6,019 nonsmokers, representing 48.2 million US adults, were included. Among them, 36% were identified as being exposed to SHS based on their serum cotinine levels, corresponding to 16.0 million adults. When compared with unexposed participants, those exposed to SHS more frequently reported living with household smokers and had a higher prevalence of having <20 natural teeth. SHS-exposed individuals also tended to be younger, female, of lower socioeconomic position, and non-Hispanic Black; they had higher sugar intake and more comorbid conditions; and they flossed less often (Table 1). Of the included NHANES cycles, only 2009 to 2014 contained laboratory data of urinary NNAL, resulting in a subsample of 4,512 participants for this sensitivity analysis.
Baseline Characteristics of Participants Stratified by Exposure to Secondhand Smoking.
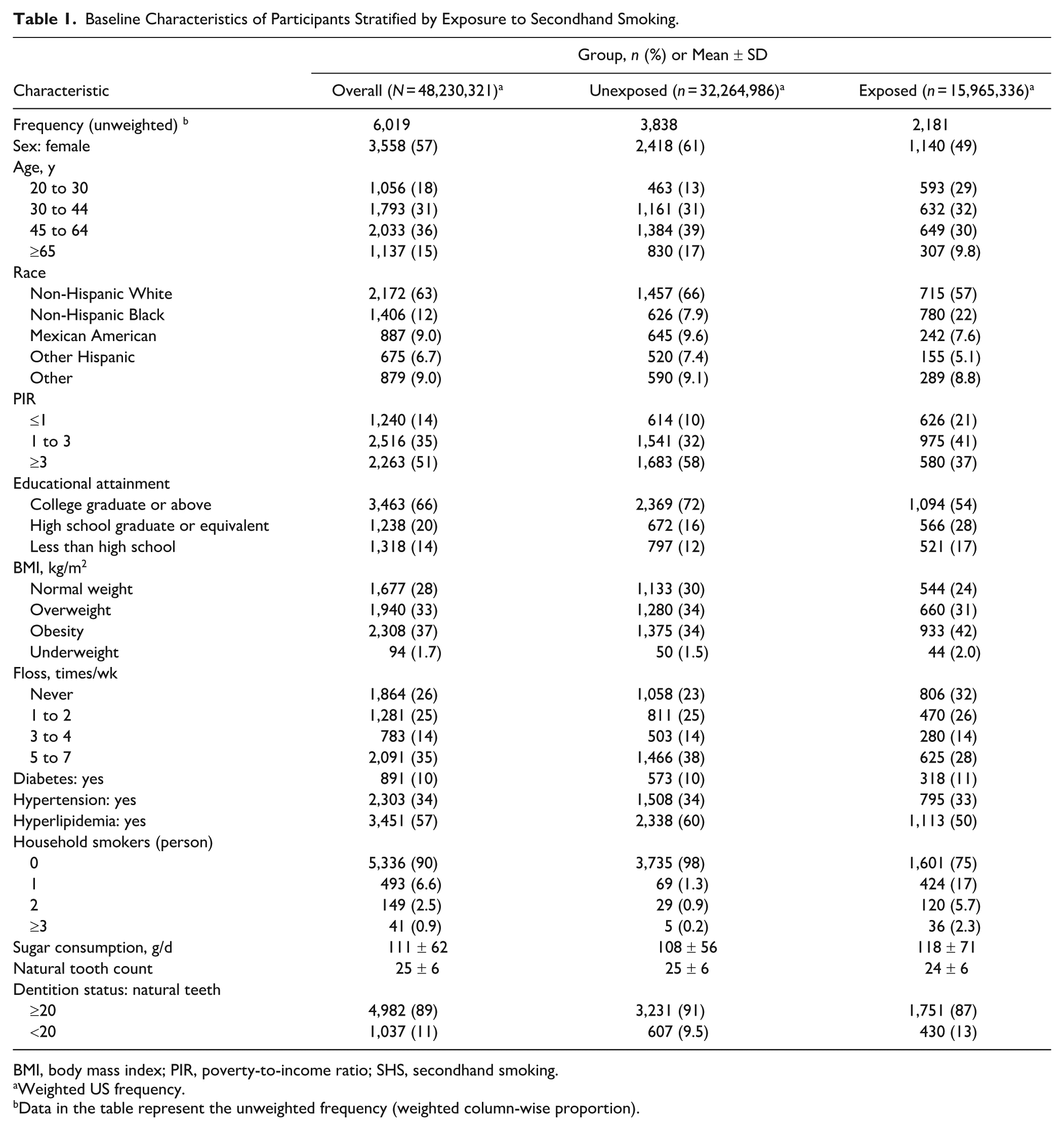
BMI, body mass index; PIR, poverty-to-income ratio; SHS, secondhand smoking.
Weighted US frequency.
Data in the table represent the unweighted frequency (weighted column-wise proportion).
Average Associations between SHS Exposure and Tooth Loss
When serum cotinine was the primary SHS definition, exposure was associated with 0.74 fewer teeth (95% CI, −1.053 to −0.426) and a 4.6-percentage higher prevalence of having <20 teeth (95% CI, 0.027 to 0.065). Estimates obtained per the alternative definition requiring elevated serum cotinine and a household smoker were similar in magnitude and direction (Table 2).
Average Associations Between Secondhand Smoking and Tooth Loss.
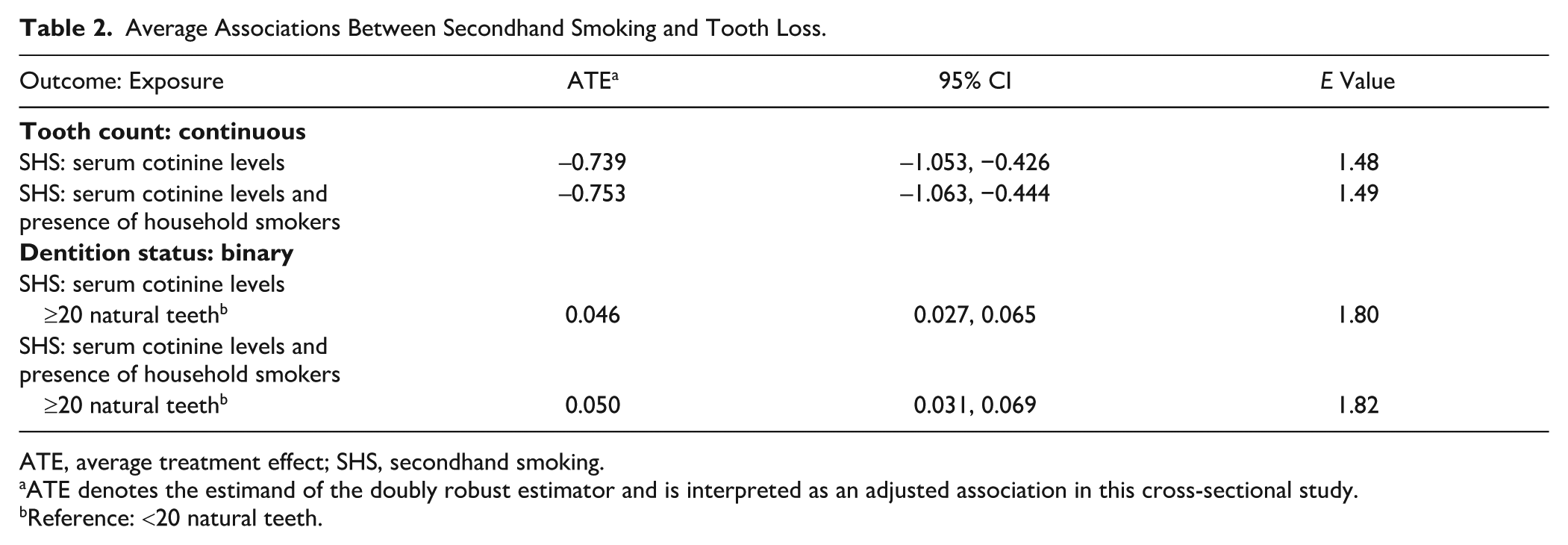
ATE, average treatment effect; SHS, secondhand smoking.
ATE denotes the estimand of the doubly robust estimator and is interpreted as an adjusted association in this cross-sectional study.
Reference: <20 natural teeth.
Performance of Causal Forest Model
Figure 2 depicts the distribution of CATEs. CATEs for the primary SHS definition centered on a median reduction of 0.653 teeth (IQR, −1.036 to −0.335) and a 3.5–percentage point increase in the probability of having <20 teeth (IQR, 0.018 to 0.058).
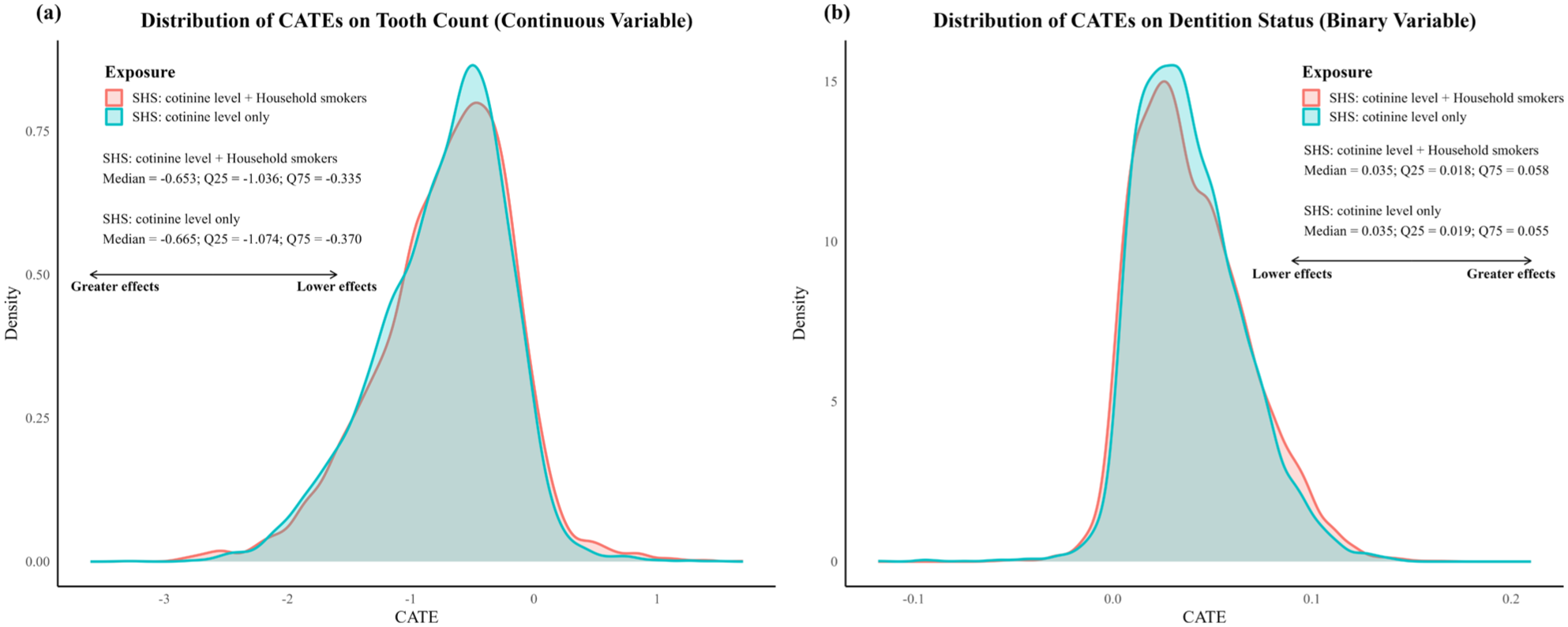
Distribution of the conditional average treatment effects of secondhand smoking on tooth loss. (
Higher- and lower-effect subgroups stratified by CATEs showed clear separation for the continuous tooth count outcome (difference, ~0.7 teeth), with more limited separation for the binary dentition outcome under the primary SHS definition (difference, ~0.005). Best linear predictor analyses indicated that the causal forests for tooth count were well calibrated and captured treatment effect heterogeneity, whereas forests for dentition status, although well calibrated, did not successfully capture the heterogeneity (Appendix Tables 7 and 8).
Appendix Figure 3 depicts the models’ stability. The student decision tree distilled from the causal forest achieved optimal performance at a depth of 2 and was constructed only for models in which the best linear predictor analysis indicated detectable treatment effect heterogeneity, providing a stable and interpretable summary of the heterogeneity structure.
Heterogeneous Association with Tooth Count
Descriptive analyses based on the CATEs indicated that adults aged ≥45 y, those with higher sugar intake, and those with metabolic conditions exhibited larger associations between SHS exposure and tooth loss. A U-shaped pattern was observed for flossing frequency, with greater vulnerability among participants who never flossed and those who flossed nearly daily (Table 3, Appendix Tables 4–6).
Characteristics across Subgroups Stratified by Conditional Average Treatment Effects.
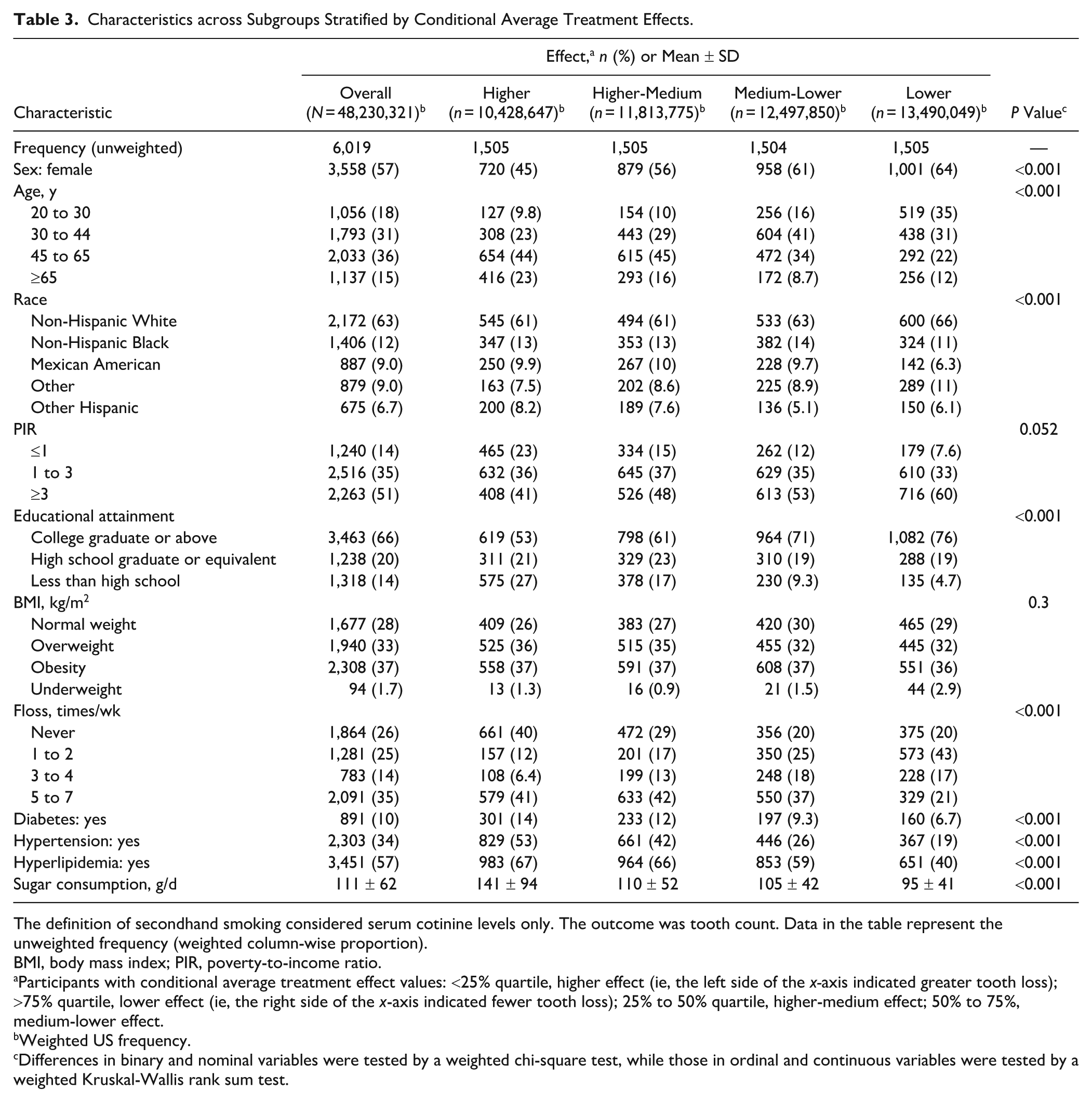
The definition of secondhand smoking considered serum cotinine levels only. The outcome was tooth count. Data in the table represent the unweighted frequency (weighted column-wise proportion).
BMI, body mass index; PIR, poverty-to-income ratio.
Participants with conditional average treatment effect values: <25% quartile, higher effect (ie, the left side of the x-axis indicated greater tooth loss); >75% quartile, lower effect (ie, the right side of the x-axis indicated fewer tooth loss); 25% to 50% quartile, higher-medium effect; 50% to 75%, medium-lower effect.
Weighted US frequency.
Differences in binary and nominal variables were tested by a weighted chi-square test, while those in ordinal and continuous variables were tested by a weighted Kruskal-Wallis rank sum test.
CDT-derived decision trees consistently identified lower educational attainment and higher sugar consumption as key factors delineating higher-risk subgroups (Appendix Fig. 3).
Results of Sensitivity Analyses
When serum cotinine thresholds varied from 0.05 to 3 ng/mL, the associations with tooth count grew increasingly negative at higher cutoffs—for example, with ATEs of −0.836 at >1.5 ng/mL and −0.884 at >2 ng/mL, reaching −1.164 at >3.0 ng/mL. However, the associations with dentition status remained statistically significant across most cutoffs but did not show a consistent monotonic trend. The associations with tooth count were consistently significant across thresholds when SHS was defined by NNAL, with ATEs ranging from −0.677 to −0.692. For dentition status, the estimate was 0.054 (95% CI, 0.025 to 0.083) and statistically significant at the 3-pg/mL threshold but attenuated and became nonsignificant at higher cutoffs (0.033 at 6 pg/mL, 0.021 at 9 pg/mL; Appendix 2: Tables 1–3).
Sensitivity analyses based on complete case data for serum cotinine and tooth count and models fitted without survey weights yielded smaller but directionally consistent estimates: ATEs on tooth count ranged from −0.449 to −0.653 and ATEs on dentition status from 0.032 to 0.043, supporting the robustness of the primary findings. For the heterogeneous associations, both sensitivity analyses identified broadly similar profiles of vulnerable subgroups. However, in the unweighted analysis, the causal forests were well calibrated but did not capture meaningful heterogeneity, whereas in the complete case analysis, the forests were well calibrated and detected statistically significant heterogeneity, albeit with evidence of underdispersion in the predicted effects (Appendix 2: Tables 4–16).
Overall, SHS exposure was consistently associated with modest reductions in tooth count and higher prevalence of having <20 teeth, with larger associations observed in several socioeconomically and medically vulnerable subgroups.
Discussion
To our knowledge, this is the first study to apply advanced causal inference methods to evaluate the association between SHS exposure and tooth loss. SHS exposure, as assessed by a biomarker, was associated with fewer natural teeth and a higher probability of having <20 teeth. Analyses of heterogeneous associations indicated that several demographic, socioeconomic, behavioral, and metabolic characteristics were linked to greater susceptibility, and these patterns were broadly supported across sensitivity analyses.
Average Associations
Our results align with previous observational studies that linked SHS to oral health outcomes. Previous work has shown elevated risks of edentulism and periodontal disease among nonsmokers exposed to environmental tobacco smoke, although most studies relied on self-reported exposure and conventional regression approaches (Umemori et al 2020). By incorporating an objective biomarker of exposure and a doubly robust estimator, the present study extends this evidence base and provides more robust population-level estimates. Our results also agree with studies documenting the benefits of tobacco control measures for oral health (Baumeister et al 2025), underscoring the importance of minimizing involuntary exposure among nonsmokers. Additionally, evaluations of smoke-free legislation have shown that public smoking bans do not compromise economic growth and may confer broad population benefits (Fu et al 2024). Importantly, there remains a lack of studies that directly quantify the impact of smoking control policies on dental outcomes via causal inference methods, highlighting an important gap for future research.
Heterogeneous Associations
Heterogeneity in the associations was observed. The causal distillation tree and descriptive analysis suggested that individuals with lower educational levels and higher sugar consumption appeared to be more susceptible to the adverse association between SHS exposure and tooth loss. A possible explanation is that those with higher education tend to possess greater health literacy, preventive behaviors, and access to professional dental care (Ghanbari-Jahromi et al 2023), which may attenuate the SHS-related harm and tooth loss and thereby support tooth retention (Baumeister et al 2025). These findings emphasize that public interventions for oral health should be tailored to socioeconomic backgrounds to reduce inequalities in oral health (Thomson et al 2018). This notion was supported by a study revealing that public intervention such as water fluoridation may yield larger benefits on caries reduction in people from lower educational backgrounds (Matsuyama et al 2025). Additionally, SHS has been linked to shifts toward cariogenic oral microbiota and to impaired oral immune defenses, creating conditions conducive to dental caries (Golpasand Hagh et al 2013; Al-Marzooq et al 2022). In the presence of high sugar consumption, caries risk and progression may increase. Our finding provides additional rationale for taxing sugar-sweetened products, with potential revenue allocated to oral health promotion in vulnerable subgroups (Andreyeva et al 2022).
Individuals who never used dental floss and those who reported flossing >5 d per week appeared to be more susceptible to SHS-related tooth loss. This seemingly paradoxical pattern may reflect, at least in part, that frequent flossing is more commonly reported among those who are already engaged with dental care due to existing oral health problems, rather than indicating a protective behavior per se (Chapple et al 2015). While this paradox was found in another study in a similar population (Cepeda et al 2017), it should be interpreted prudently without robust validation. Similarly, common comorbidities, including diabetes, hypertension, and hyperlipidemia, were identified as features of the vulnerable group, suggesting that SHS may exacerbate the oral health burden in persons already at elevated systemic risk (Kocher et al 2018; Bitencourt et al 2023). This observation is biologically plausible, given that these conditions are characterized by chronic inflammation and metabolic dysregulation, which are implicated in periodontitis (Hajishengallis and Chavakis 2021). On the grounds that these comorbidities are particularly prevalent among elderly adults (Cao et al 2023) and that our results indicate that the elderly are more susceptible to SHS, clinicians should systematically assess not only personal but also household smoking exposure when managing patients with these conditions. At a broader level, these findings reinforce the need for public health strategies that integrate smoking control with chronic disease management, thereby improving oral health and overall resource allocation (Neophytou et al 2024).
Strengths and Limitations
This study has several strengths. We used a nationally representative dataset, applied biomarker-based exposure assessment, and employed advanced causal inference methods under the potential outcomes framework. The incorporation of a generalized random forest and causal distillation tree allowed us to estimate heterogeneous treatment effects and offer clinically interpretable insights into population subgroups most affected (Matsuyama et al 2024; Rehill 2024; Huang et al 2025). With application of NHANES weights, our estimates are generalizable to the US adult population, providing policy-relevant information (Burgos-Ochoa and Clouth 2025).
Several limitations warrant consideration. First, tooth loss is cumulative and biologically plausible as an outcome influenced by SHS; however, the cross-sectional design precludes establishing temporality, and reverse causation cannot be excluded. Second, despite the use of E values to evaluate robustness, residual confounding from unmeasured factors may persist. Third, dichotomizing serum cotinine may not capture cumulative exposure patterns relevant to tooth loss. Future studies employing panel data or longitudinal modified treatment policy strategies offer a more appropriate framework to characterize dose-response relationships and account for within-individual variation in exposure over time. Beyond the methodological limitations, the results of the present study were derived from the US population, which limits the generalizability to populations with distinctive smoking behaviors or from different oral health systems. Future studies are warranted to examine the external validity in other populations or combine results from various datasets with meta-analytic approaches.
Conclusion
This study provides evidence from causal inference methods that SHS exposure was associated with tooth loss among nonsmokers, and it highlights that individuals with disadvantaged socioeconomic status, higher sugar consumption, and comorbidities are particularly vulnerable. These findings reinforce the need for integrating dental outcomes into tobacco control policy making and prioritizing the susceptible subpopulations in public health interventions. Clinicians may consider assessing SHS exposure, particularly for vulnerable subgroups, in dental settings and mitigating such exposure as a supporting measure within oral health management.
Author Contributions
Y.Q. Chen, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised manuscript; J.M. Zheng, contributed to design, data analysis and interpretation, critically revised the manuscript; Y.Z. Chen, H.Y. Zhang, contributed to design, data acquisition and interpretation, drafted the manuscript; J.Y. Li, H. Deng, contributed to data interpretation, drafted the manuscript; Y.Y. Kong, contributed to conception and design, data interpretation, critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261419027 – Supplemental material for Average and Heterogeneous Associations between Secondhand Smoking and Tooth Loss
Supplemental material, sj-docx-1-jdr-10.1177_00220345261419027 for Average and Heterogeneous Associations between Secondhand Smoking and Tooth Loss by Y.Q. Chen, J.M. Zheng, Y.Z. Chen, H.Y. Zhang, J.Y. Li, H. Deng and Y.Y. Kong in Journal of Dental Research
Supplemental Material
sj-docx-2-jdr-10.1177_00220345261419027 – Supplemental material for Average and Heterogeneous Associations between Secondhand Smoking and Tooth Loss
Supplemental material, sj-docx-2-jdr-10.1177_00220345261419027 for Average and Heterogeneous Associations between Secondhand Smoking and Tooth Loss by Y.Q. Chen, J.M. Zheng, Y.Z. Chen, H.Y. Zhang, J.Y. Li, H. Deng and Y.Y. Kong in Journal of Dental Research
Footnotes
Acknowledgements
The authors acknowledge the endeavor of all participants in NHANES project. The authors thank Professor Aida Jun at the Institute of Science Tokyo for providing suggestions on the results interpretation. The authors thank Professor Jiang Hongbo at Guangdong Pharmaceutical University for his assistance in the implementation of statistical approaches.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Guangdong Basic and Applied Basic Research Foundation Project (2022A1515110601).
Ethical Considerations
The NHANES project was approved by the Ethics Review Committee of the National Center for Health Statistics of the United States. All participants provided their informed consent.
A supplemental appendix to this article is available online.