
Abstract
Fluoride is widely regarded within dentistry and public health as a safe and effective measure for preventing dental caries. Public ambivalence toward fluoride has intensified in recent years, reflected in ongoing disputes over water fluoridation. This scoping review synthesizes qualitative evidence on how fluoride hesitancy is constructed and expressed across social and clinical contexts. Qualitative studies examining perceptions, beliefs, and decision-making related to fluoride use were identified through searches of PubMed, Scopus, Embase, and CINAHL to April 2025. Twelve studies met the inclusion criteria. Data were extracted using a standardized charting approach and synthesized through an inductive, grounded theory–informed thematic analysis supported by constant comparison and reflexive memoing. Five interconnected domains of hesitancy were identified: (1) perceptions of fluoride as harmful or toxic; (2) uncertainty about benefits or necessity; (3) mistrust of scientific, professional, or governmental institutions; (4) ethical concerns regarding autonomy, consent, and environmental integrity; and (5) discomfort with specific delivery modalities paired with preferences for alternatives. Hesitancy was shaped not only by information but also by emotional responses, lived experience, parenting norms, online discourse, and interpretations of institutional credibility. Across studies, decisions about fluoride reflected broader efforts to navigate uncertainty, protect children, and maintain control over health choices. Fluoride hesitancy is a multifaceted interpretive process rather than a simple knowledge deficit. Addressing it requires approaches that pair clear scientific communication with attention to trust, autonomy, and the social contexts in which preventive recommendations are received. Strategies that acknowledge experiential perspectives and increase transparency around policy decisions may enhance the credibility and uptake of fluoride guidance, but some degree of hesitancy is likely to persist given wider environments of uneven trust and contested information.
Keywords
Introduction
Fluoride is widely presented as an effective measure for preventing dental caries, with global policy frameworks endorsing its safety and efficacy (Petersen and Lennon 2004; Whelton et al 2019). Despite this long-standing scientific consensus, public unease regarding fluoride has intensified in recent years. Communities across multiple countries have engaged in recurrent debates over water fluoridation (Chikte 1997; Griffin et al 2008; Quiñonez and Locker 2009; Knox et al 2017), and dental professionals increasingly report encounters with caregivers who hesitate or decline professionally applied fluoride treatments (Chi et al 2023; Cruz et al 2024b). Fluoride hesitancy is defined as a delay in acceptance, thoughts of refusal, or refusal of fluoride despite availability (Ko and Chi 2023). This emerging ambivalence corresponds to a broader family of behaviors known as health hesitancies, driven by a broader shift in how individuals engage with health information, interpret risk, and place trust in scientific, professional, and governmental institutions (Bowen et al 2025).
Fluoride hesitancy shares features with other forms of contemporary health hesitancies in terms of the broader structural and cultural factors but remains distinct (Carpiano and Chi 2018). Unlike vaccine hesitancy that arises during discrete clinical encounters, fluoride-related choices permeate daily routines: brushing a child’s teeth, attending dental checkups, or drinking tap water (Ko and Chi 2023). These repeated exposures shape attitudes before clinical encounters (Burgette et al 2022), drawing on personal experience, parenting expectations, notions of “naturalness,” online discourse, and broader beliefs about autonomy and institutional trust. Understanding how these influences come together requires approaches attentive to lived experience and meaning, rather than solely to behaviors or outcomes.
Despite its growing relevance, qualitative evidence on fluoride hesitancy remains dispersed across settings, populations, and treatment modalities. Studies have examined parental refusal of topical fluoride in clinical settings (Hendaus et al 2016; Koh et al 2024), community resistance to water fluoridation (Quiñonez and Locker 2009), online promotion of fluoride-free lifestyles (Milne et al 2017), and culturally-specific narratives among minority groups (Scherzer et al 2010; Barker et al 2016). However, these perspectives have not been synthesized to explain how individuals construct meaning around fluoride such as how they interpret risk, weigh competing information, or justify refusal. Without such synthesis, the field lacks a coherent and empirically grounded understanding of fluoride hesitancy.
This scoping review addresses the gap by mapping the perspectives, motivations, and social processes that underpin fluoride hesitancy. Through a grounded, inductive analysis of qualitative studies across diverse contexts, this review develops a conceptual framework that illustrates how fluoride hesitancy emerges and is sustained.
Methods
Protocol and Registration
This review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology (Peters et al 2020). The reporting of the methodology and results was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (Tricco et al 2018). The review protocol was prospectively registered on the Open Science Framework (10.17605/OSF.IO/VNCPD).
Eligibility Criteria
The inclusion criteria followed the JBI Population–Concept–Context framework:
Population: Studies involving members of the public, dental patients, parents or caregivers, dental professionals, or other stakeholders whose perceptions, beliefs, or behaviors regarding fluoride use were explored.
Concept: Studies examining fluoride hesitancy or factors contributing to hesitancy, including beliefs, perceptions, risk interpretations, or decision-making related to fluoride or fluoridation, including fluoride toothpaste, varnish, supplements, and community water fluoridation.
Context: Studies conducted in any setting (community, clinical, educational, or public health) and in any geographical location.
Only qualitative studies using methods such as interviews, focus groups, or qualitative surveys were included. Qualitative components embedded within broader study designs (eg, mixed–methods or trial-based process evaluations) were also eligible. Quantitative studies, reviews, commentaries, conference abstracts, and non–peer-reviewed publications were excluded. Only studies published in English were considered, with no restriction on publication year.
Literature Search, Screening, and Selection
The search strategy was developed in accordance with the JBI methodology for scoping reviews. An initial search of PubMed and Scopus informed the final search terms, which were then applied to PubMed, Scopus, Embase, and CINAHL (Appendix Table 1). Reference lists of included studies were also screened. Searches were conducted up to April 10, 2025. Records were de-duplicated in EndNote and screened in ASReview Lab v2.0, with potentially relevant reports retrieved for full-text assessment against eligibility criteria by 2 reviewers; disagreements were resolved by consensus with a third reviewer when needed. Reasons for full-text exclusions were documented (Appendix Table 2). Additional details on ASReview screening, calibration, and interrater reliability are provided in the Appendix Methods.
Data Extraction
Data extraction used a standardized charting form capturing key study characteristics and findings relevant to fluoride hesitancy. The reviewers piloted the charting form on 3 studies to ensure clarity, consistency, and completeness. Minor revisions were made following this pilot phase. Two reviewers (S.M.S.C. and Y.J.O.) independently extracted data from each included study and compared the results for consistency. Discrepancies were resolved through consensus, with a third reviewer (J.R.H.T.) consulted when necessary. Extracted data included bibliographic details (author, year, country, journal), study aims, participant characteristics and recruitment context, qualitative methodology and data collection approaches, funding sources, conflict-of-interest statements, key themes and subthemes, and illustrative quotations reported in each study.
Quality Assessment
Following guidance for qualitative evidence synthesis, the methodological quality of included studies was appraised using the JBI Critical Appraisal Tool (Lockwood et al 2015). Two reviewers (A.H.C.T. and Y.J.O.) independently assessed each study, with any disagreements resolved through discussion. Where necessary, a third reviewer (J.R.H.T.) was consulted.
Data Synthesis
Qualitative findings from the included studies were synthesized using an inductive, grounded theory–informed thematic analysis, guided by the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) framework (Tong et al 2012). Consistent with grounded theory, the synthesis drew on the constant comparative method, allowing patterns and theoretical insights to emerge from the data.
Open coding was first conducted independently, concurrent with data extraction, examining data line by line to generate initial concepts and preliminary codes. These codes directed further data extraction and sampling and were iteratively compared, refined, and regrouped into higher-order categories capturing relationships among concepts across studies. Throughout this process, memo writing was used to document emerging ideas, conceptual links, and evolving interpretations. The study team also considered how their positions as dental clinicians and researchers within fluoride-endorsing health care systems might shape interpretation. Reflexive memoing and regular team discussions supported the identification of underlying assumptions, helping to ensure that interpretations remained anchored in the perspectives reported in the primary studies.
Themes were developed through continuous comparison of data within and between studies, with team discussions used to achieve interpretive coherence and consensus. Coding and thematic refinement continued until no further conceptual insights emerged. The resulting themes offer a conceptually grounded account of the factors shaping fluoride hesitancy, supported by illustrative quotes and interpretations from the included qualitative studies.
Results
Study Characteristics
A total of 1,036 records were identified. After screening and full-text assessment of 109 records, 12 studies met the inclusion criteria (Fig 1). Three studies examined water fluoridation as a municipal public health intervention. None focused on perceptions of naturally occurring fluoride in groundwater. One study assessed salt fluoridation, and the remaining studies focused on topical fluoride in clinical contexts or broader fluoride-related beliefs. Studies were conducted across North America, Europe, Australia, and the Caribbean. There was only 1 study in an upper-middle-income country (Tayhan and Çetinkaya 2024), and all other studies were in high-income contexts. When disclosed, reported funding sources were public or governmental (Appendix Table 3).
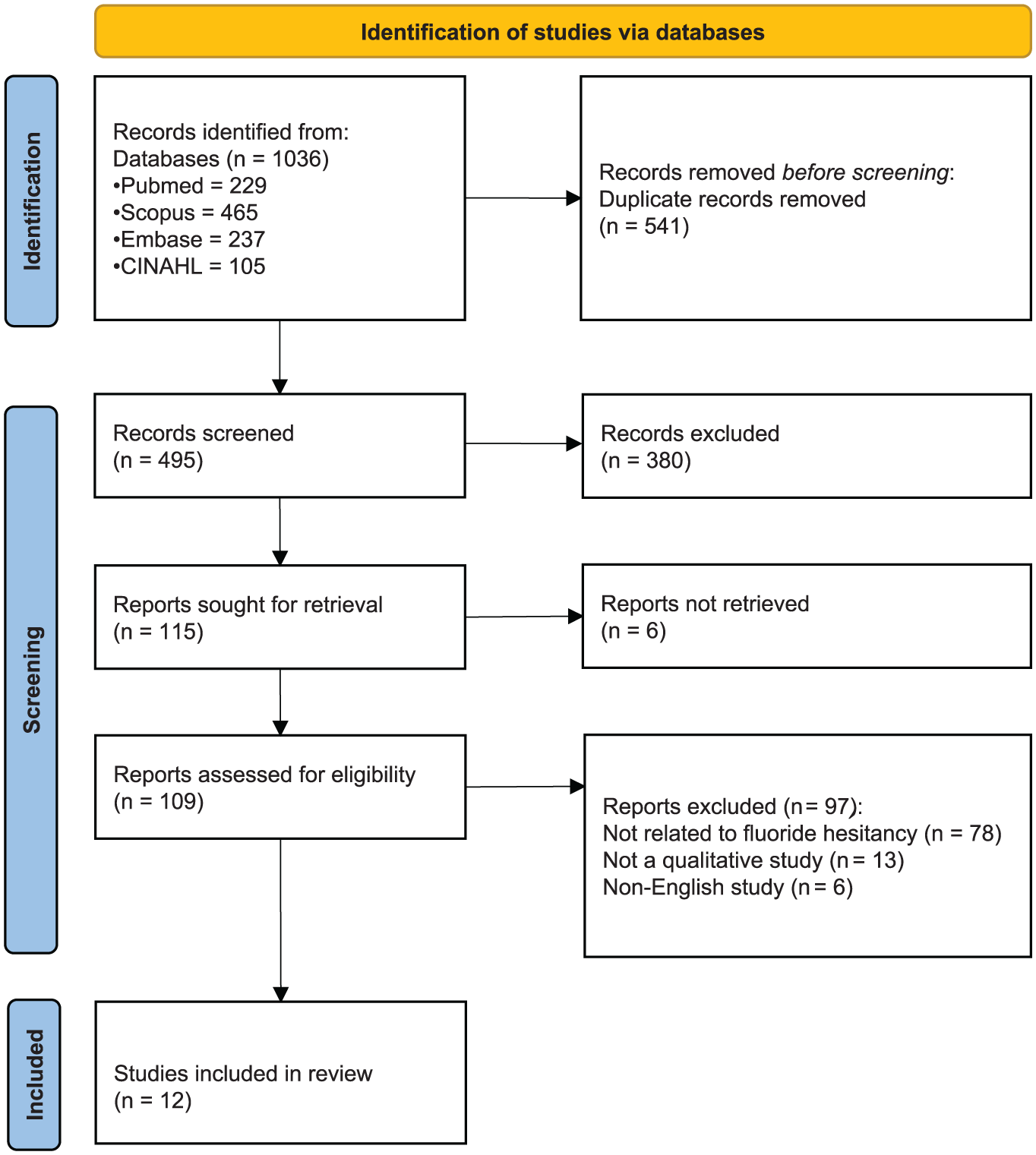
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Study aims centered on public perceptions of fluoride, drivers of hesitancy, and decision-making surrounding fluoridated products or programs. Participants included parents, community members, dental patients, and online forum users recruited through clinical settings, community outreach, household surveys, and digital platforms. Across 9 studies reporting individual qualitative interview participants, 394 participants contributed to the evidence base (range 10–66 per study). One study used focus group discussions and 2 analyzed nonparticipant online data. Included studies were published between 2008 and 2024, with 7 published from 2022 onward. Data collection methods comprised interviews, focus groups, ethnography, online discourse analysis, and mixed-methods surveys (Table 1).
Study Characteristics of Included Studies.
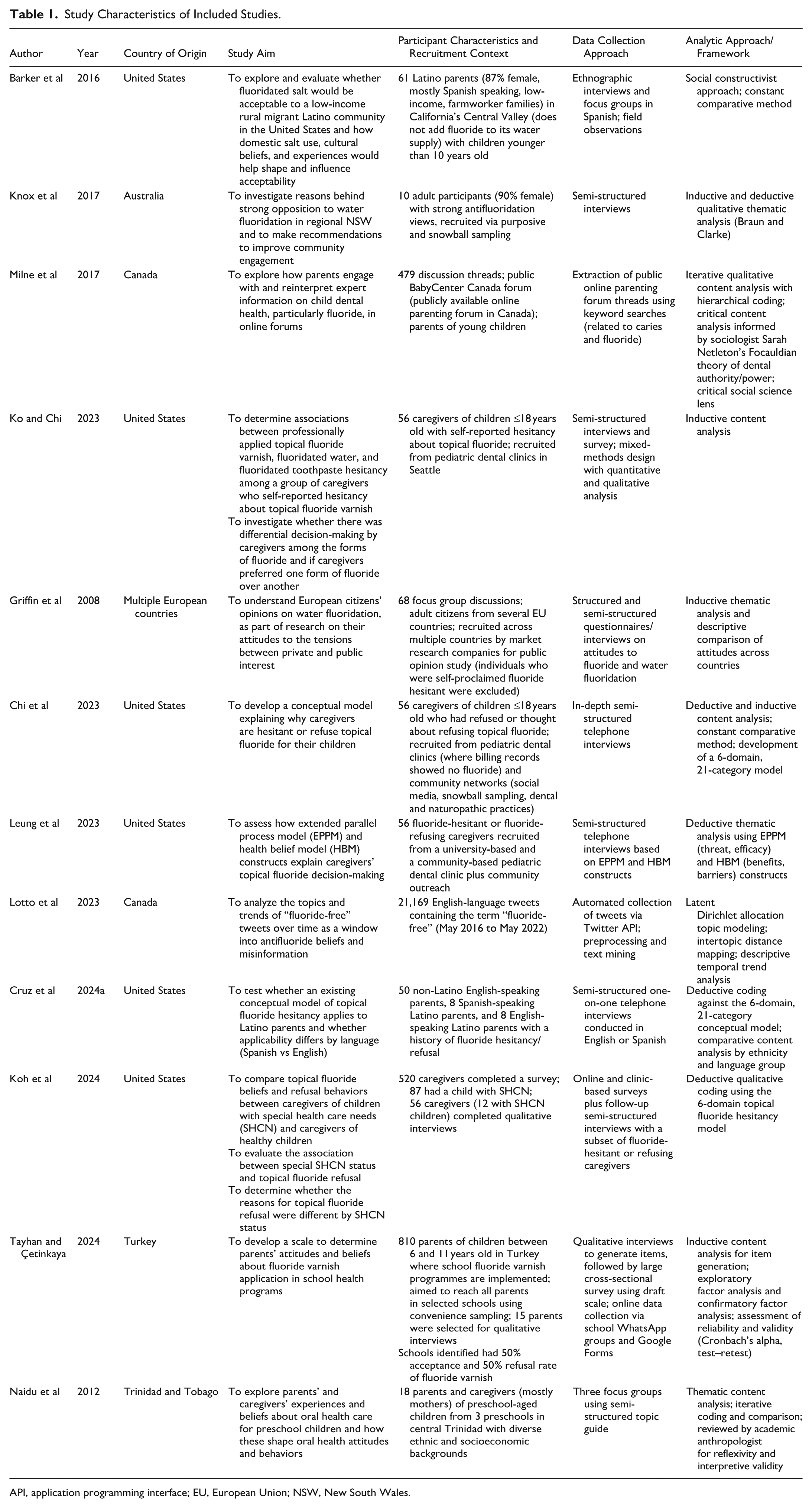
API, application programming interface; EU, European Union; NSW, New South Wales.
Quality Appraisal
Overall, the studies demonstrated coherence between philosophical perspectives, methodologies, and methods, with most providing ethical approval and data-aligned conclusions. A consistent limitation across the evidence base was the lack of reporting on researcher positioning and reflexivity, with nearly all studies providing insufficient or unclear detail (Appendix Table 4).
Thematic Analysis
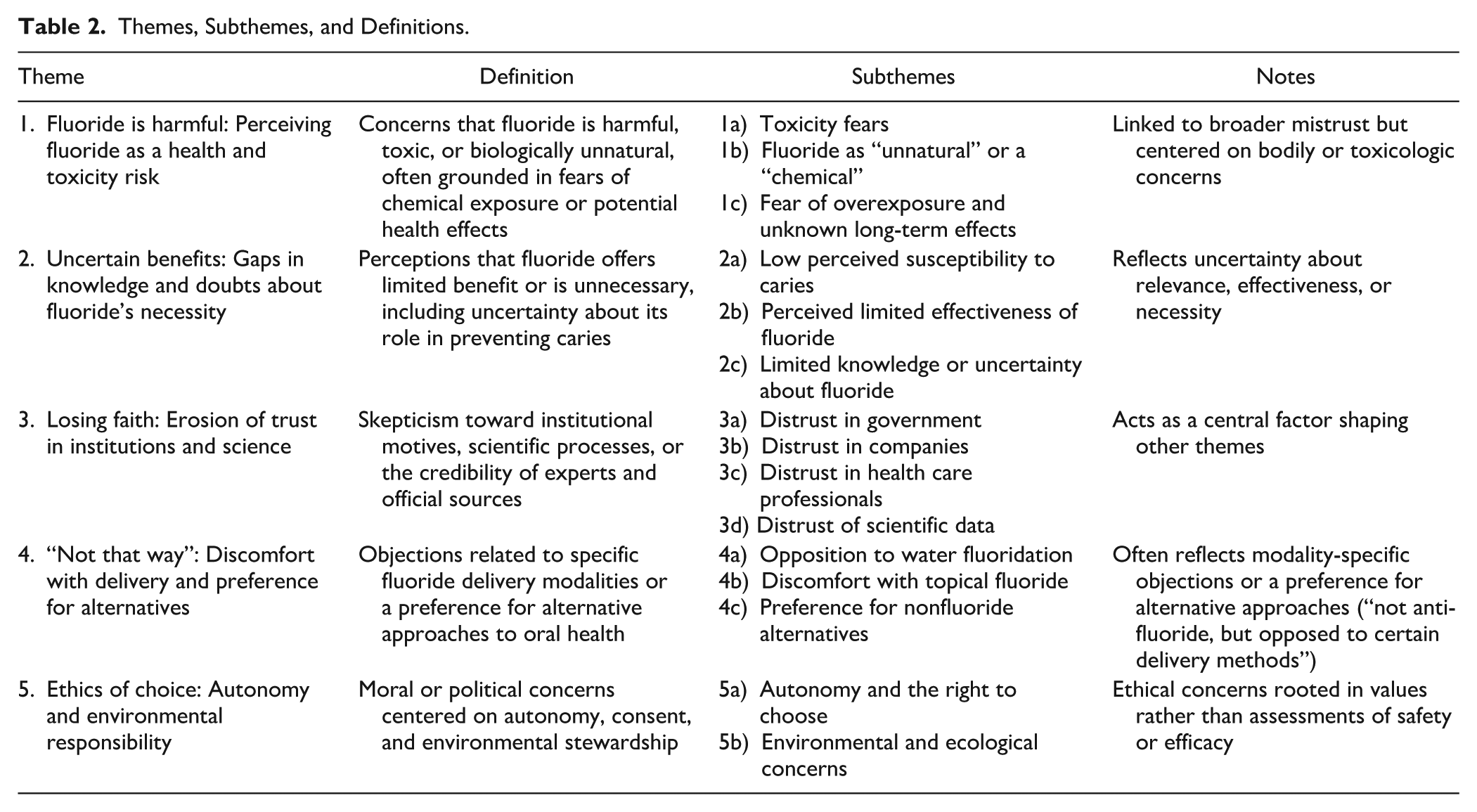
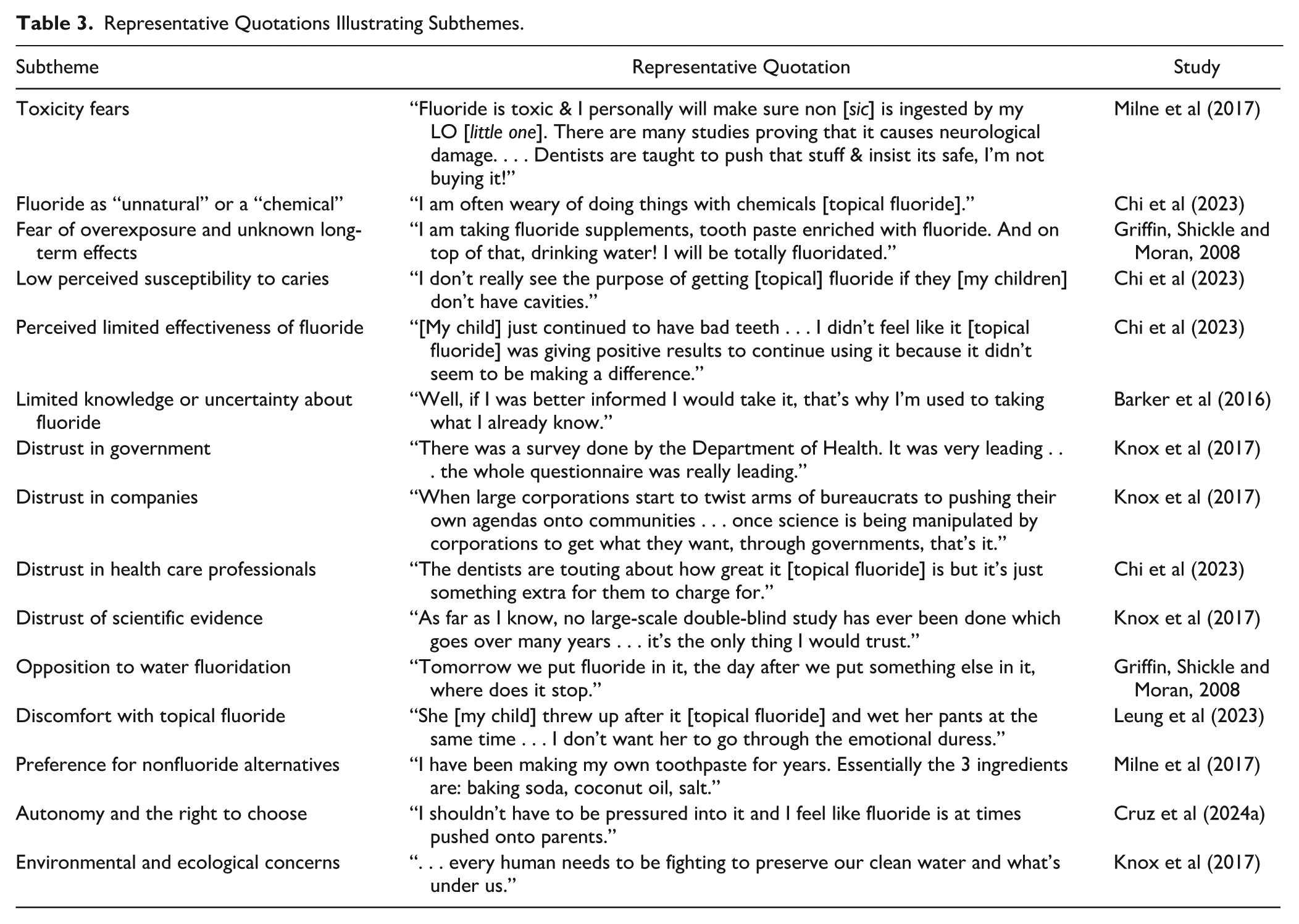
Across the included studies, a coherent picture of fluoride hesitancy emerged, spanning reluctance or refusal toward fluoride in community water supplies, professionally applied interventions, and home-use dental products (Appendix Table 5). Five overarching domains were identified (Table 2) and illustrated by representative quotes (Table 3).
1.
Themes, Subthemes, and Definitions.
Representative Quotations Illustrating Subthemes.
Across settings, participants frequently characterized fluoride added to water or dental products as an unnatural chemical additive, contrasting with the growing preference for “chemical-free” lifestyles and natural products (Griffin et al 2008; Chi et al 2023; Ko and Chi 2023; Leung et al 2023; Lotto et al 2023; Cruz et al 2024a; Koh et al 2024; Tayhan and Çetinkaya 2024). Fluoride was often described as artificial and potentially toxic, and these interpretations contributed to expressions of hesitancy (Griffin et al 2008; Naidu et al 2012; Barker et al 2016; Milne et al 2017; Chi et al 2023; Ko and Chi 2023; Leung et al 2023; Lotto et al 2023; Cruz et al 2024a; Koh et al 2024; Tayhan and Çetinkaya 2024). Fluoride was commonly regarded as a chemical contaminant and less as a preventive measure. Emotional reactions to the term “fluoride,” such as fear, anxiety, aversion, or disgust, further reinforced these views.
These risk perceptions persisted regardless of the information provided during these encounters, suggesting that concerns were grounded equally in emotional and experiential factors as in informational ones. Among caregivers, particularly parents of young children or those with special health care needs, avoidance was often described as a precautionary measure to protect the child (Chi et al 2023; Leung et al 2023; Cruz et al 2024a; Koh et al 2024). Biological or toxicological worries were frequently cited, but these accounts also intersected with wider concerns, including varying levels of trust in institutions and differing views on whether fluoride is necessary.
2.
Many participants also questioned whether fluoride was necessary, expressing uncertainty and skepticism about its effectiveness. For some, this uncertainty stemmed from limited knowledge or awareness rather than deliberate opposition (Barker et al 2016; Milne et al 2017; Chi et al 2023; Ko and Chi 2023; Cruz et al 2024a; Koh et al 2024; Tayhan and Çetinkaya 2024). Several caregivers of children and adolescents reported not knowing whether professionally applied fluoride or community water fluoridation provided additional benefits beyond routine oral hygiene. In situations in which explanations from health professionals were perceived as unclear or inconsistent, uncertainty tended to lead to hesitation rather than outright refusal. Other participants believed that good oral hygiene and regular toothbrushing were sufficient, reducing their perceived need for fluoride exposure (Griffin et al 2008; Milne et al 2017; Chi et al 2023; Ko and Chi 2023; Leung et al 2023; Cruz et al 2024a; Tayhan and Çetinkaya 2024). Some also expressed low confidence in fluoride’s effectiveness, questioning whether water fluoridation or topical applications provided the level of protection presented in public health messaging (Knox et al 2017; Chi et al 2023; Leung et al 2023; Cruz et al 2024a; Koh et al 2024; Tayhan and Çetinkaya 2024). These doubts extended to the credibility and relevance of scientific evidence, with fluoridation viewed by some as outdated or overstated. Overall, low perceived benefit often intersected with varying levels of trust in institutions. When the purpose of fluoride was unclear or uncertain, concerns about perceived risks became more prominent in decision-making.
3.
Mistrust was a recurring influence on hesitancy. Participants frequently expressed skepticism toward government agencies, health authorities, dental professionals, and scientific institutions (Griffin et al 2008; Knox et al 2017; Milne et al 2017; Chi et al 2023; Ko and Chi 2023; Cruz et al 2024a; Tayhan and Çetinkaya 2024). In several studies, fluoridation initiatives were interpreted as politically or commercially motivated, rather than oriented toward public health. Perceived inconsistencies or a lack of clarity in public health messaging sometimes led participants to seek information from alternative sources, such as online communities and personal networks, which were viewed as more relatable or trustworthy.
4.
Participants generally did not oppose fluoride itself; rather, their concerns centered on how it was delivered. Community water fluoridation was perceived by some as a broad, population-level intervention that might be suitable for large groups but not tailored to individual needs (Griffin et al 2008; Knox et al 2017; Ko and Chi 2023; Lotto et al 2023; Cruz et al 2024a). Individual modalities, such as fluoridated toothpastes, dietary measures, or professionally applied products, were often preferred (Griffin et al 2008; Cruz et al 2024a). Among parents and caregivers, especially those caring for children with special health care needs, practical and sensory considerations further shaped these choices. Topically applied fluoride was frequently described as uncomfortable or distressing for children due to taste and texture sensitivity (Chi et al 2023; Leung et al 2023; Cruz et al 2024a; Koh et al 2024). Avoidance in these instances was often framed as a rejection of the mode of delivery to protect the child’s comfort and well-being, despite recognition by caregivers of the potential preventive benefits of fluoride.
5.
Ethical and rights-based concerns featured across studies, particularly in relation to community water fluoridation (Griffin et al 2008; Knox et al 2017; Ko and Chi 2023; Lotto et al 2023; Cruz et al 2024a). Participants frequently described fluoridation as limiting personal autonomy, with some characterizing it as a form of “forced medication,” or as a public health measure implemented without individual consent (Griffin et al 2008; Knox et al 2017; Chi et al 2023; Ko and Chi 2023; Cruz et al 2024a; Koh et al 2024). Informed consent was viewed as a moral principle that should apply not only in clinical settings but also to population-level interventions. Beyond individual autonomy, some participants raised broader ethical and environmental concerns (Knox et al 2017). These included questions about the collective right to alter natural water systems and potential ecological consequences, such as the effects on aquatic ecosystems or water purity. In these accounts, hesitancy extended beyond bodily considerations to ideas about environmental integrity and resistance to perceived human-made modification of natural resources.
Ethical considerations therefore centered on issues of consent, choice, and the role of government in influencing health-related behavior. These concerns often intersected with broader patterns of trust and mistrust, with participants who doubted governmental motives being more likely to express reservations about the legitimacy of fluoridation policies. Social context added further complexity. Some individuals felt encouraged by professionals or peers to accept fluoride, while others found their doubts reinforced within personal networks or online communities that promoted “natural” or fluoride-free lifestyles (Ko and Chi 2023; Tayhan and Çetinkaya 2024). Thus, autonomy concerns interacted with social identity, moral values, and environmental perspectives.
Discussion
This review indicates that fluoride hesitancy is a multidimensional process shaped by emotional responses, interpretations of risk and benefit, trust in institutions, ethical commitments, and the practicalities of everyday care. Rather than a simple matter of “for” or “against” fluoride, the findings suggest a continuum of positions in which people negotiate uncertainty, responsibility, and control across different social and clinical contexts.
Across the themes, concerns about harm and toxicity were often expressed in vividly emotional terms. This pattern is consistent with broader work in risk psychology showing that affective reactions often precede and shape risk judgments. The “affect heuristic” and “risk-as-feelings” models propose that intuitive, emotion-based appraisals can dominate over more deliberative assessments when individuals evaluate hazards in health and environmental domains (Loewenstein et al 2001; Slovic et al 2007). Research on vaccine decision-making similarly demonstrates that people rely on heuristic cues such as the behavior of trusted persons, perceived experts, or the majority when navigating uncertainty, with social signals serving as practical means of resolving ambiguity (Xu et al 2024). Within this perspective, hesitancy is not simply a knowledge deficit but a response to uncertainty. Persistent concerns about fluoride safety, even in the presence of additional information, can therefore be understood as part of a broader process of making sense of risk, responsibility, and protection in everyday life.
In several studies, fluoride concerns related as much to the institutions promoting it as to fluoride itself. Healthcare operates as a social institution sustained by trust, cooperation, and perceptions of fairness (Gilson 2003). When communication from authorities was experienced as opaque, one sided, or inattentive to individual concerns, people often sought information from sources that felt more responsive to their own experiences. Similar patterns have been observed in the vaccine confidence literature, where declining trust in governments, industry, and scientific institutions has created space for competing explanations (Larson et al 2018). Social media can amplify this shift by strengthening trust in peer communities, elevating lay expertise, and making personal stories appear more credible than institutional messages (Nicholls et al 2024). A clear dichotomy emerged when comparing studies on water fluoridation, where the underlying institution was the government and utility infrastructure against studies on topical fluoridation, where the underlying institution was the healthcare system mediated by the specific healthcare providers. In water fluoridation, in which decisions were made by government and utility infrastructure rather than face to face, participants framed their concerns in terms of coercion, lack of choice, and suspicion of political or corporate agendas. For professionally applied topical fluoride, hesitancy was more often centered on children’s vulnerability, previous negative experiences, and perceived pressure or inadequate explanation from dental teams. Only 1 study examined fluoride toothpaste hesitancy, with the qualitative literature instead emphasizing community water fluoridation, likely because it is a collective, nonoptional intervention. Caregivers in several studies expressed uncertainty about its evidence and wanted more clarity about how safety and effectiveness were established. Across both contexts, institutional advice was interpreted alongside information drawn from peers, social media, and alternative health networks. The resulting doubts typically related to wider questions of trust and credibility rather than to specific disputes about toxicology or caries-prevention data (Griffin et al 2008; Knox et al 2017).
Conceptual Framework: Anthropological Model on Fluoride Hesitancy
Medical anthropology offers a useful lens for understanding fluoride hesitancy because it positions health decisions within wider cultural and political contexts rather than treating them solely as responses to clinical risk information (Singer and Clair 2003; Janes and Corbett 2009). As reflected in the conceptual framework (Fig 2), fluoride hesitancy emerges through the interaction of macro-level political and informational environments, meso-level social and cultural systems, and micro-level embodied experiences. Concerns about fluoride or preferences for “fluoride-free” products can be understood as part of broader patterns of self-care and identity, resonating with the idea of the “mindful body,” in which health practices reflect personal values and social expectations (Lock and Scheper-Hughes 1987).
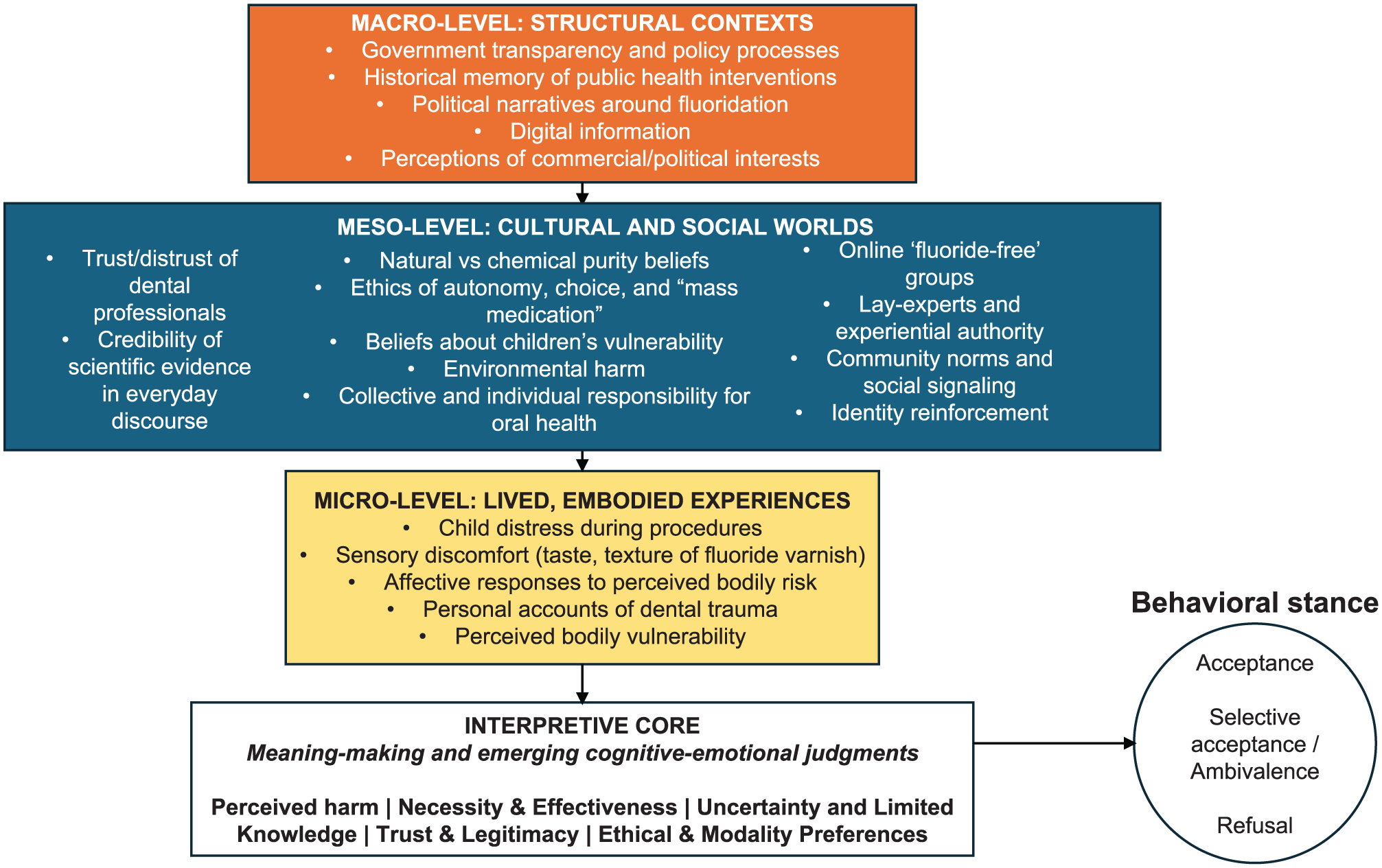
Conceptual framework of fluoride hesitancy.
Research on parenting and health behaviour shows that refusals of preventive interventions often stem from perceived efforts to be vigilant and protective, rather than from disagreement with clinical recommendations. These decisions are also shaped by parents’ social environments, including peer networks and moral expectations about responsible caregiving (Reich 2020): caregivers frequently grounded decisions in children’s sensory experiences, previous distress, or a desire to retain control over what enters the child’s body. These are shaped and reinforced by meso-level social environments such as peer networks and online communities.
Fluoride hesitancy also reflects interpretations of the legitimacy of institutions. Concerns about water fluoridation often centered on the role of government, perceived transparency of decision-making, and whether population-level measures respected community values. In contrast, hesitancy around topical fluoride tended to arise within everyday clinical encounters, shaped by communication style, perceived pressure, or how well parents felt their concerns were acknowledged. Attending to these social and institutional dimensions does not detract from the strength of the evidence for fluoride’s effectiveness; rather, it highlights where communication and engagement efforts can be strengthened so that preventive guidance feels credible, relevant, and responsive to the communities it aims to serve.
The findings also suggest that participants often approach fluoride from social, ethical, and experiential perspectives that differ from professional framing of fluoride as a routine preventive measure. While professional discourse tends to frame fluoride as a well-established preventive measure, members of the public may interpret it through alternative understandings of safety, autonomy, or past experiences with institutions. Recognizing these differing ways of making sense of fluoride can facilitate more productive dialogue and improve the credibility of preventive recommendations within the lived contexts in which individuals and families make decisions.
Strengths and Limitations of the Study
This review adhered to methodological and reporting standards, including JBI guidance, PRISMA-ScR, and ENTREQ. A quality assessment of the included studies was conducted, strengthening the transparency of the synthesis. Inductive and grounded analysis, drawing on constant comparison, allowed findings to be synthesized into a coherent, conceptually informed account of how fluoride hesitancy is constructed. However, the study is not without limitations. Studies were mostly from high-income settings, which may reflect varying cultural perceptions of risk, autonomy, and health responsibility that may not generalise to contexts in which dental caries burden, water infrastructure, or trust in public institutions differ. In such settings, fluoride hesitancy may also be shaped by affluence, as the ability to opt out of fluoride exposure (eg, through bottled water, filtration, or specialty products) may also be unevenly distributed by socioeconomic resources. None of the included studies explicitly examined the role of fluoridated bottled water or how commercial alternatives may mediate fluoride exposure and decision-making. As an interpretive synthesis, it offers a map of documented perspectives and underlying patterns not accessible through quantitative approaches. Formal patient and public involvement consultation was not undertaken in this scoping review. This may have limited the incorporation of lived experience, and future reviews would benefit from integrating patient and public involvement to enhance relevance and interpretation of findings.
Implications for Practice and Policy
Future research should use anthropological, ethnographic, and participatory approaches to examine how fluoride hesitancy develops in everyday life. Such approaches can inform communication strategies that prioritise dialogue rather than downstream messaging, while experiments testing informational cues and adapted trust-framework measures can clarify when hesitancy increases and what predicts it (Schwarzinger et al 2021; Bowen et al 2025).
The findings also highlight a broader misalignment between how clinicians and policymakers frame prevention and how members of the public make sense of fluoride. Professional guidance is often presented through epidemiological and risk–benefit logics, whereas patients draw on experiential, moral, and relational frameworks shaped by daily life (Dein 2003; Buus et al 2012). The evidence base was also dominated by public, caregiver, and community perspectives, with minimal representation of dental professional, policymaker, or implementer viewpoints. Future qualitative research incorporating these perspectives may support more comprehensive and context-sensitive engagement strategies. Addressing fluoride hesitancy requires strategies that extend beyond information provision. Clinically, this involves making space for questions, acknowledging uncertainty where appropriate, and explaining decisions clearly. At the policy level, clearer communication about how fluoridation decisions are made, why specific concentrations are used, and how safety is monitored may help strengthen trust. Treating experiential and scientific knowledge as complementary can help ensure that fluoride guidance is both trusted and used. However, in environments characterised by uneven trust and conflicting information, some hesitancy will be expected to remain.
Conclusion
Fluoride hesitancy reflects a combination of emotional, ethical, social, and experiential influences rather than a single concern. These dynamics influence how individuals interpret risk, benefit, and the trustworthiness of recommendations in relation to water fluoridation, professionally applied topical fluoride, and fluoride use at home. Recognising hesitancy as an interpretive process rather than a knowledge deficit provides a foundation for clinical and policy approaches that are more responsive to lived experience, more attentive to autonomy and trust, and ultimately more effective in supporting preventive oral health.
Author Contributions
S.M.S. Chen, Y.J. Ong, contributed to design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; L.Y. Soh, contributed to design, data acquisition, analysis, and interpretation, critically revised manuscript; A.H.C. Tay, D.Y. Chow, contributed to design, data analysis and interpretation, critically revised the manuscript; J.R.H. Tay, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261428043 – Supplemental material for Understanding Fluoride Hesitancy: A Qualitative Scoping Review
Supplemental material, sj-docx-1-jdr-10.1177_00220345261428043 for Understanding Fluoride Hesitancy: A Qualitative Scoping Review by S.M.S. Chen, Y.J. Ong, L.Y. Soh, A.H.C. Tay, D.Y. Chow and J.R.H. Tay in Journal of Dental Research
Footnotes
Acknowledgements
None.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data supporting the findings of this study are provided in the Appendix. Detailed descriptions of the literature-screening process, calibration procedures, and interrater reliability are provided in the Appendix Methods. The complete search strategies and database counts are in Appendix Table 1, the list of full‑text exclusions with reasons is in Appendix Table 2, the reported funding sources and conflict of interest statements from included studies are in Appendix Table 3, the qualitative critical appraisal outcomes for included studies are in Appendix Table 4, and the thematic synthesis mapping of studies to themes and subthemes is in Appendix Table 5. As this review synthesized published qualitative studies, no original interview transcripts were generated; illustrative quotes were drawn from the included publications and cited in the text.
Registration Number
10.17605/OSF.IO/VNCPD
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.