
Abstract
Primary Sjögren disease (pSjD) is associated with a wide range of oral manifestations, including mucosal alterations such as oral ulcers, stomatitis, angular cheilitis, papillary atrophy, and tongue fissuration, as well as oral sequelae of sicca symptoms, including dysphagia, dysgeusia, and chewing difficulties. In addition to these oral findings, pSjD also presents with systemic manifestations such as arthritis, cutaneous vasculitis, and involvement of internal organs. This systematic review and meta-analysis aimed to assess the risk of oral disorders and differences in cariological and periodontal indices in pSjD patients compared with controls. The systematic search was conducted in PubMed, EMBASE, and CENTRAL on November 8, 2024 (PROSPERO: CRD42024608240). Studies meeting the eligibility criteria included adult patients with pSjD. Primary outcomes included the odds ratio (OR) and prevalence of oral disorders as well as the mean difference (MD) and single mean values of dental indices. Meta-analyses were performed using random-effects models to calculate pooled outcome measures and corresponding 95% confidence intervals (CIs). Seventy-five studies were included in the systematic review, with 49 eligible for meta-analysis. The following oral disorders showed increased risk: candidiasis (OR: 10.5; CI: 6.99 to 15.79), dysphagia (OR: 26.78; CI: 20.94 to 34.25), dysgeusia (OR: 17; CI: 4.52 to 63.96), stomatitis (OR: 2.65; CI: 2.17 to 3.23), angular cheilitis (OR: 6.31; CI: 1.94 to 20.53), papillary atrophy (OR: 6.68; CI: 1.12 to 42.16), and fissured tongue (OR: 11.72; CI: 3.42 to 40.18). Patients with pSjD were found to have fewer teeth (MD: −2.16; CI: −4.27 to −0.05) and a higher decayed, missing, filled teeth (MD: 4.72; CI: 3.01 to 6.43) and decayed, missing, filled surfaces (MD: 20.45; CI: 10.16 to 30.74) scores. Furthermore, periodontal parameters showed no significant differences. Patients with pSjD have up to a 30-fold higher risk of developing various oral disorders, emphasizing the need for preventive dental care and early recognition.
Introduction
Sjögren disease (SjD) is a chronic systemic autoimmune disease, considered to be the second most prevalent autoimmune rheumatic disease, following rheumatoid arthritis (Helmick et al 2008; Berman et al 2019). The prevalence of SjD ranges from 1 to 72 cases per 10,000 individuals (Ramos-Casals et al 2025), with it occurring more frequently in women typically between 40 and 60 y of age (Ramos-Casals et al 2012; Brito-Zerón et al 2017). Yet, several classification criteria for SjD have been developed over time, and the American-European Consensus Group (AECG) criteria are the most widely used in current clinical practice (Baldini et al 2012).
Although patients are treated by physicians and internal medicine specialists, oral complications are among the earliest and most debilitating manifestations of SjD, which is characterized by lymphocytic infiltration and progressive damage of the exocrine glands (Belkacem Chebil et al 2019; Dézsi et al 2023). Potential xerostomia, rapidly progressing dental caries, oral candidiasis, and periodontal disease not only compromise essential functions such as chewing, swallowing, and speaking but also significantly impair patients’ quality of life. These oral manifestations are often accompanied by systemic symptoms, including thyroiditis, arthritis, primary biliary cirrhosis, and cholangitis, further underscoring the multisystemic impact of the condition (Humphrey and Williamson 2001; Kaplan et al 2008; Stewart et al 2008; Belkacem Chebil et al 2019; Berman et al 2019).
For many individuals, oral manifestations precede systemic symptoms and often prompt their first visit to a dental professional, highlighting the critical role of dentists in early detection. Fox et al (2008) further supported this with their multicenter survey, in which an oral complaint was the initial symptom in more than half of the patients with primary SjD (pSjD). Despite the clinical importance of these oral disorders, the magnitude of their risk in patients with pSjD remains poorly defined. Existing studies focus on isolated manifestations without providing a comprehensive risk profile. One systematic review (Serrano et al 2018) focused on only oral mucosal lesions in SjD patients, whereas 3 meta-analyses (de Goés Soares et al 2018; Maarse et al 2019; Wu et al 2021) investigated the association of periodontal conditions in SjD patients, with de Goés Soares et al and Wu et al reporting greater plaque index (PI) and gingival index (GI), while Maarse et al found no such association.
The lack of synthesized evidence limits the ability of dental practitioners to implement effective preventive strategies, tailor patient education, and involve multidisciplinary teams, including rheumatologists or ophthalmologists. Therefore, this systematic review and meta-analysis aimed to conduct a more comprehensive risk assessment of oral disorders in pSjD, providing evidence to guide both clinical practice and future research in optimizing oral care in individuals with pSjD as well as updating current guidelines to promote early recognition leading to early treatment of pSjD’s manifestations.
Methods
Protocol
This work was carried out as part of the Systems Education Program (Hegyi and Varró 2024) at Semmelweis University and conducted within the Translational Medicine (TM) Cycle Framework by the Academia Europaea (Hegyi et al 2020). We report that our systematic review and meta-analysis followed the recommendations of the PRISMA 2020 guideline and the Cochrane Handbook. The protocol was registered in PROSPERO (CRD42024608240). A minor deviation from the original protocol was made to enhance the scope and clarity of the analysis: in the final analysis, only patients with pSjD were included, while those with secondary Sjögren’s disease (sSjD) were excluded.
Eligibility Criteria
Studies were considered eligible if they met predefined criteria using the Condition, Context, and Population (CoCoPop) framework. We included observational studies (cohort, case-control, and cross-sectional) and interventional studies (randomized, nonrandomized, and pilot) involving adult patients (≥18 y) (Population) diagnosed with pSjD (Context) that reported on oral disorders (Condition). In addition, studies were eligible if they reported oral disorders (Outcome) in adult patients (Population) with pSjD (Exposure) compared to individuals without pSjD (Comparator), according to the Population, Exposure, Comparator, and Outcome (PECO) framework. Case reports, case series, conference abstracts, narrative reviews, systematic reviews, and meta-analyses were excluded. SjD is classified into 2 forms: primary and secondary. PSjD occurs in isolation, whereas sSjD is diagnosed when the condition coexists with another systemic autoimmune disease, such as rheumatoid arthritis, systemic lupus erythematosus, or systemic sclerosis (Negrini et al 2022).
Studies using any accepted diagnostic criteria for SjD were included. Based on the criteria applied, 4 groups were defined: American College of Rheumatology/European League Against Rheumatism classification criteria (ACR/EULAR), European Consensus Group (ECC), American-European Consensus Group (AECG), and non-ACR/EULAR (studies reporting the use of accepted criteria without specifying which).
In general, study populations were considered to represent pSjD unless the authors explicitly reported the inclusion of sSjD. If both pSjD and sSjD patients were included, only data specific to pSjD were extracted.
Information Sources
The systematic search was conducted on November 9, 2024, in 3 electronic databases: MEDLINE (via PubMed), EMBASE, and Cochrane Central Register of Controlled Trials (CENTRAL). All publications were retrieved without any restrictions or filters. Furthermore, the reference lists of the included articles were screened to identify additional relevant articles.
Search Strategy
The search key was constructed with 2 domains. The first domain refers to pSjD, while the second domain contains different oral disorders associated with pSjD. The full search key can be found in Appendix Document 1.
Selection Process
Records downloaded from the systematic search were imported into EndNote 20, where duplicate articles were removed (Á.H.). The selection process was conducted using the Rayyan Intelligent Systematic Review program. Two independent reviewers (Á.H. and M.K.) screened the records by title and abstract, and then by full-text, according to the inclusion criteria. A third reviewer (J.L.) resolved any disagreements. To assess interreviewer reliability, Cohen’s kappa coefficient was calculated after each phase of the screening process.
Data Collection Process
Two reviewers (Á.H. and M.K.) extracted all relevant data independently into separate, standardized Microsoft Excel spreadsheets. Discrepancies were resolved through discussion between reviewers or by consultation with a third reviewer (J.L.).
Data Items
The following data were extracted: study characteristics (first author, year of publication, study design, study period, country, and the number of involved centers), population demographics (total number of participants, age, and percentage of male individuals), characteristics of pSjD and non-SjD individuals (age, percentage of male individuals), outcome measure values (oral parameters [average number of teeth; decayed, missing, filled teeth {DMF-T}; decayed, missing, filled surfaces {DMF-S}], periodontal indices [GI, PI, bleeding on probing {BOP}, probing pocket depth {PPD}, clinical attachment loss {CAL}]), and oral disorders (candidiasis, dysphagia, dysgeusia, stomatitis, oral ulcers, gingivitis, periodontitis, stomatitis, angular cheilitis, papillary atrophy, fissured tongue).
Dysphagia and dysgeusia were patient-reported (self-reported) symptoms. In contrast, oral mucosal and periodontal conditions, including oral ulcers, gingivitis, periodontitis, stomatitis, angular cheilitis, papillary atrophy, fissured tongue, and oral candidiasis were included only when they were clinician diagnosed.
Study Risk-of-Bias Assessment
The risk of bias of included studies was independently assessed by 2 reviewers (Á.H. and M.K.) using the Joanna Briggs Institute (JBI) proportions tool for studies reporting prevalence data and the Quality in Prognostic Studies (QUIPS) tool for prognostic studies. Details of each tool can be found in Appendix Document 2.
Statistical Analysis
As considerable between-study heterogeneity was anticipated, random-effects models were applied in all analyses. For comparative analyses, statistical significance was defined as a 95% confidence interval (CI) not crossing the null value. Results were presented using forest plots.
For comparative dichotomous outcomes, odds ratio (OR) with 95% CIs were calculated using inverse variance weighting and used as the primary effect measure to compare the odds of oral disorders between pSjD and controls. Study-specific ORs and the pooled OR were calculated using extracted event counts and total sample sizes for each group. A Mantel–Haenszel–type treatment arm continuity correction was applied for only the zero-cell counts. The Paule–Mandel estimator was used for τ and τ2, with the corresponding CI derived using the Q-profile method. The prediction interval was based on t distribution. Between-study heterogeneity was assessed using the between-study variance (τ2) and Higgins and Thompson’s I2 statistics.
For continuous outcomes, single mean (SM) and mean differences (MDs) with 95% CIs were calculated using inverse variance weighting. The restricted maximum likelihood estimator was used to estimate between-study variance (τ and τ2), with CI derived using the Q-profile method. Prediction intervals were calculated based on the t-distribution.
For single-arm data dichotomous outcomes, pooled proportions with 95% CIs were estimated using a random-intercept logistic regression model. A maximum-likelihood estimator was used for τ and τ2. The Clopper–Pearson CI was used for individual studies.
Hartung–Knapp adjustment was applied in all models to obtain a more conservative and reliable CI.
Prediction intervals were when at least 8 studies were included in a pooled analysis in accordance with methodological recommendations.
To explore potential sources of heterogeneity, outlier detection was performed by comparing the CI of individual studies with the pooled estimates; studies with nonoverlapping intervals were considered potential outliers. Leave-one-out sensitivity analyses were conducted to assess the influence of individual studies on the heterogeneity (I2) and pooled estimate. Influential studies were identified based on model diagnostics estimates (standardized residuals, DFTs, Cook’s distance, covariance ratio, hat values).
When standard deviations (SDs) were not reported, they were calculated from standard errors of the mean (SEM) using the formula
Publication bias was assessed using funnel plots and statistical tests when appropriate. For analyses including at least 10 studies, visual inspection of funnel plot asymmetry was interpreted alongside Egger’s test (for MDs) and Peters’ test (for ORs). For analyses with fewer than 10 studies, only the visual assessment of the funnel plot asymmetry was performed, recognizing its limited reliability and increased susceptibility to chance; therefore, findings were interpreted with caution, and no definitive conclusions were drawn.
All statistical analyses were conducted using R software, with the meta package for basic meta-analysis calculations and plots, and the dmetar package for influential diagnostics and additional analyses.
Results
Search and Selection
The systematic search and reference chasing identified 13,022 and 1,966 records, respectively. A total of 73 studies were included in the systematic review, of which 49 contained sufficient data for quantitative synthesis. The search and selection process is shown in the PRISMA 2020 flow diagram (Fig 1).
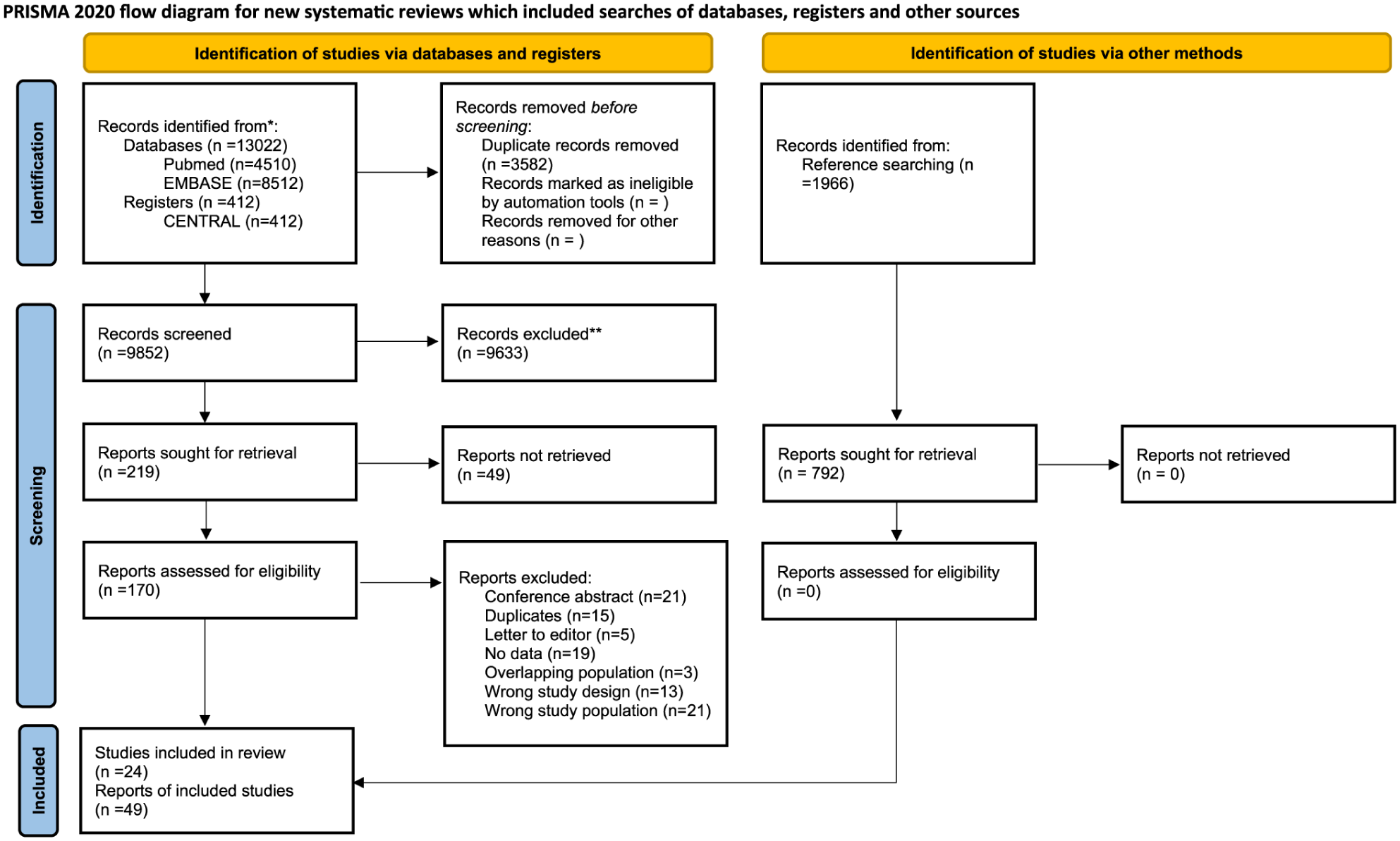
PRISMA flowchart of the article selection process.
Six studies did not clearly state that the study population consisted exclusively of pSjD; however, none reported the inclusion of sSjD patients. Among these, 2 applied AECG criteria, 3 used ECC, 1 used Fox’s criteria, and 1 applied ACR/EULAR criteria. These studies were therefore retained.
Two studies were excluded from the meta-analysis because they included mixed populations of pSjD and sSjD without reporting separate results, precluding the extraction of pSjD-specific data.
Basic Characteristics of Included Studies
Among the 73 studies included in the systematic review, there were 40 case-control studies, 8 cohorts, 19 cross-sectional studies, 4 observational studies, 1 intervention study, and 1 pilot study. All were published between 1980 and 2024 and were conducted across a range of geographic regions: 31 from Europe, 5 from the United States, 4 from South America, and 9 from Asia—ensuring broad population representation. Table 1 provides a detailed summary of their baseline characteristics. Among the included studies, 21 provided data on ORs, 27 on prevalence, 14 on MDs, and 25 on SMs.
Main Characteristics of the Included Studies.
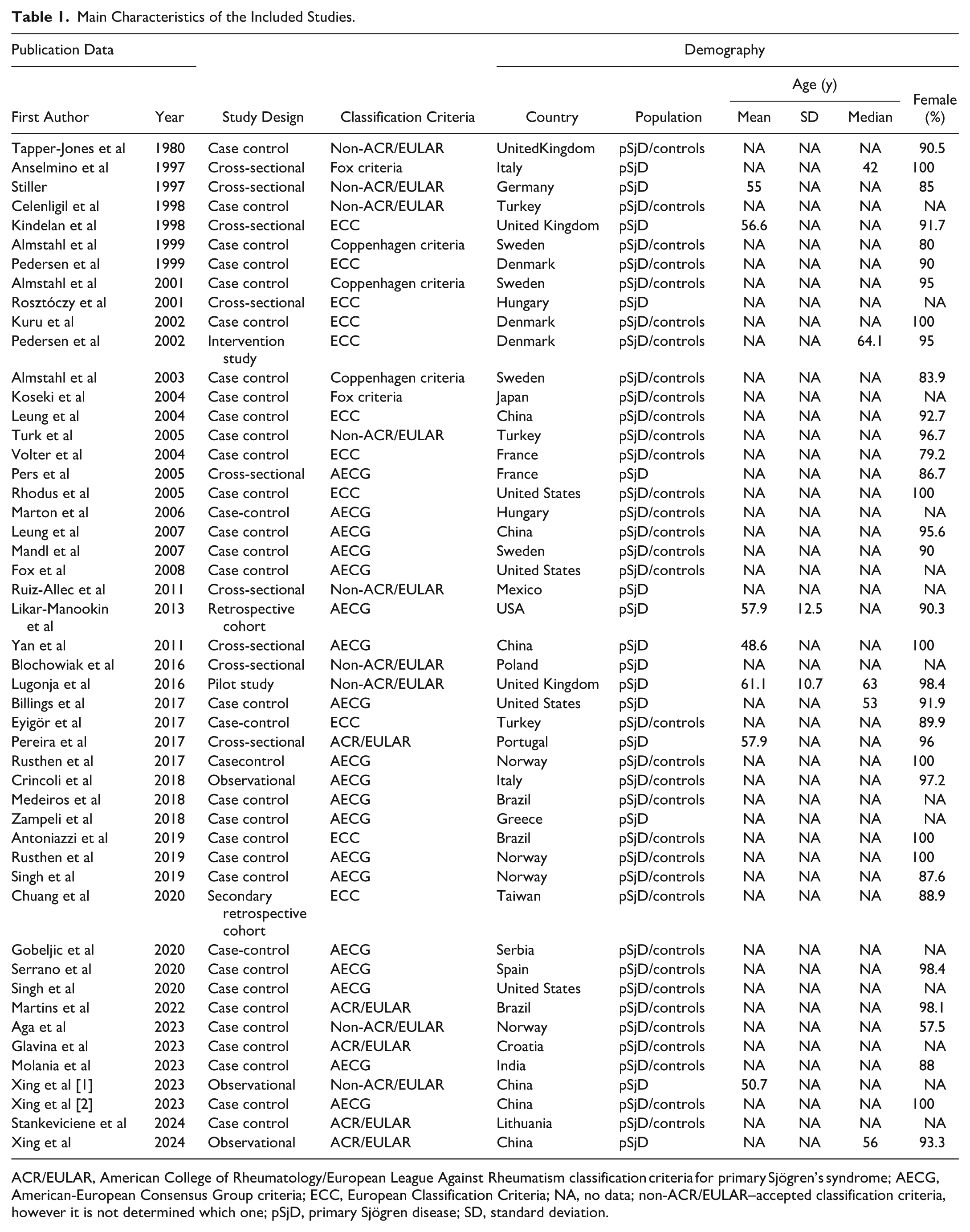
ACR/EULAR, American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren’s syndrome; AECG, American-European Consensus Group criteria; ECC, European Classification Criteria; NA, no data; non-ACR/EULAR–accepted classification criteria, however it is not determined which one; pSjD, primary Sjögren disease; SD, standard deviation.
Oral Disorders in pSjD
Table 2 presents the risk of various oral disorders in patients with pSjD. Dysphagia (OR: 26.78; CI: 20.94 to 34.25; P < 0.001*), dysgeusia (OR: 17; CI: 4.52 to 63.96; P = 0.006*), stomatitis (OR: 2.65; CI: 2.17 to 3.23; P = 0.001*), angular cheilitis (OR: 6.31; CI: 1.94 to 20.53; P = 0.009*), papillary atrophy (OR: 6.86; CI: 1.12 to 42.16; P = 0.042*), and fissured tongue (OR: 11.72; CI: 3.42 to 40.18; P = 0.008*) were associated with a significantly higher odds in patients with pSjD. In contrast, oral ulcers, gingivitis, and periodontitis were not significantly associated with pSjD compared with controls. Detailed prevalence data and the individual OR figures are provided in Appendix Figures 1 to 30.
Odds of Oral Disorders in pSjD.
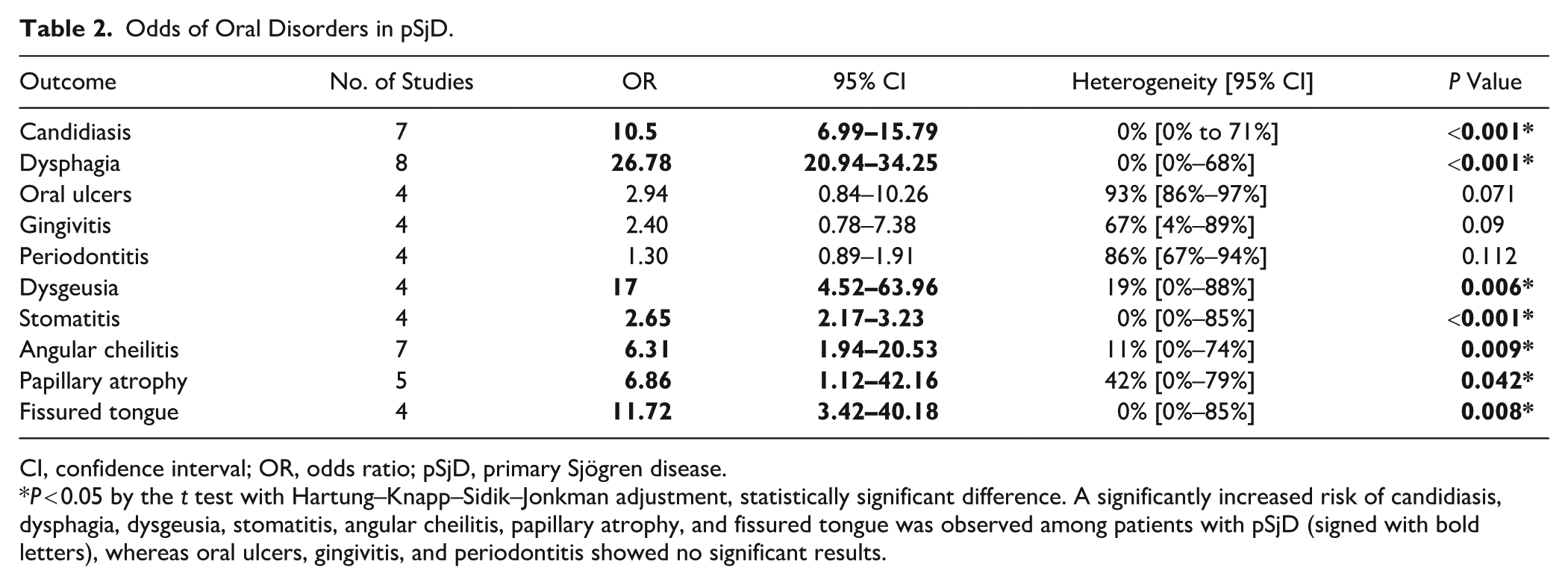
CI, confidence interval; OR, odds ratio; pSjD, primary Sjögren disease.
P < 0.05 by the t test with Hartung–Knapp–Sidik–Jonkman adjustment, statistically significant difference. A significantly increased risk of candidiasis, dysphagia, dysgeusia, stomatitis, angular cheilitis, papillary atrophy, and fissured tongue was observed among patients with pSjD (signed with bold letters), whereas oral ulcers, gingivitis, and periodontitis showed no significant results.
Orofacial Candidiasis in pSjD
Seven studies (Pedersen et al 1999; Leung et al 2004; Fox et al 2008; Crincoli et al 2018; Medeiros et al 2018; Serrano et al 2020; Martins et al 2022) comprising 2,654 patients with pSjD were analyzed (Fig 2). The pooled OR was 10.5 (CI: 6.99 to 15.79; I2 = 0%, CI: 0% to 71%; P < 0.001*), indicating that patients with pSjD had approximately 10-fold higher odds of candidiasis compared with controls. Pooled prevalence estimates of candidiasis are presented in Appendix Figures 31 and 32.
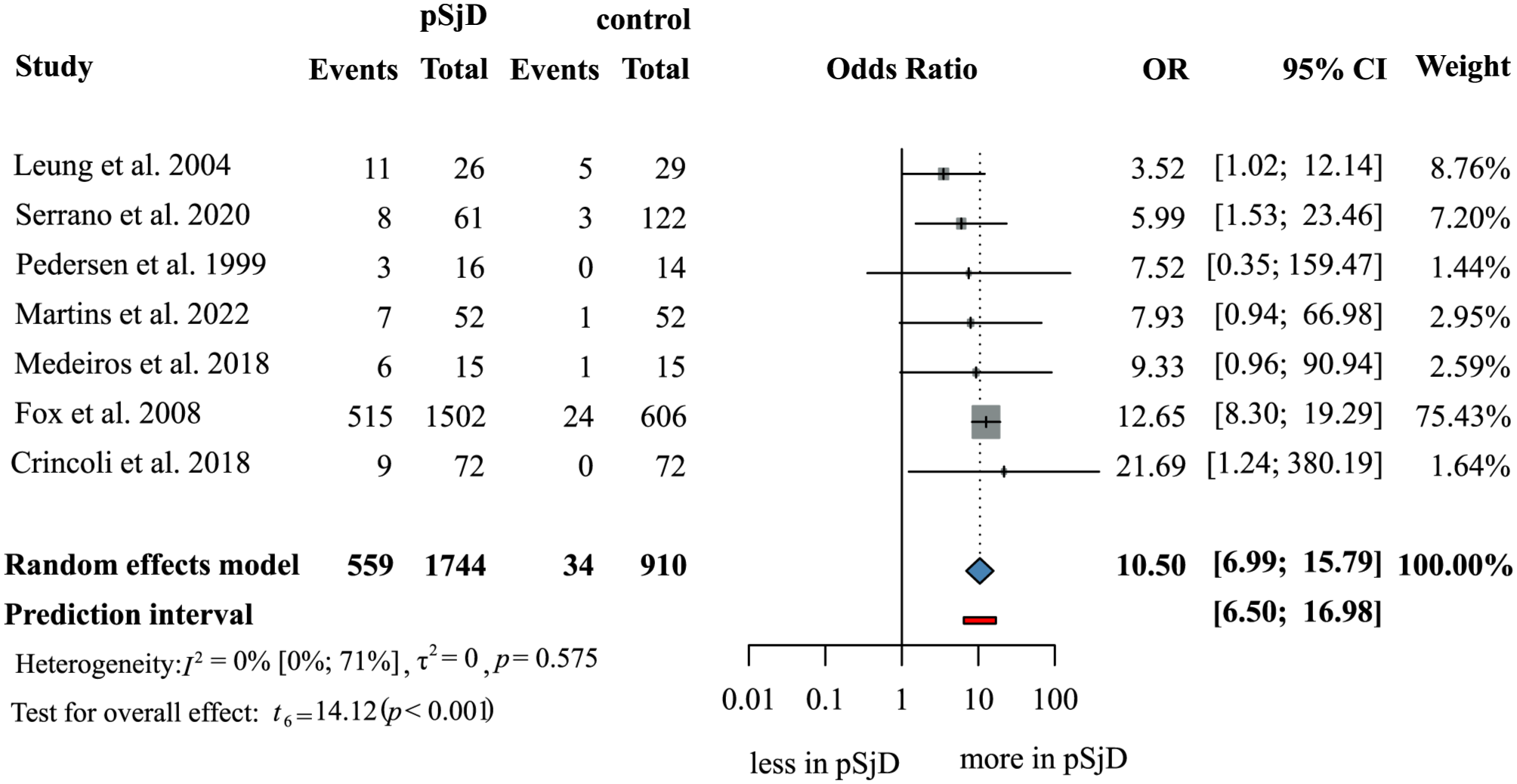
OR of orofacial candidiasis in pSjD versus controls: Forest plot showing the odds ratio for orofacial candidiasis in patients with and without pSjD. A significantly increased risk of orofacial candidiasis was observed among patients with pSjD (OR = 10.50, P < 0.001).
Oral Health Indicators in pSjD
Seven oral health indicators, including structural/caries-related parameters and periodontal parameters, were assessed (Table 3). For structural/caries-related parameters, patients with pSjD had, on average, fewer teeth (MD = −2.16; CI: −4.27 to −0.05; P = 0.046*) and a significantly higher DMF-S index (MD = 20.45; CI: 10.16 to 30.74; P = 0.008*) compared with those without pSjD. In contrast, periodontal indices, such as BOP, PI, GI, PPD, and CAL, did not differ significantly between groups. MD and SM estimates are presented in Appendix Figures 33 to 53.
Mean Difference in Oral Parameters in pSjD Patients versus Controls.
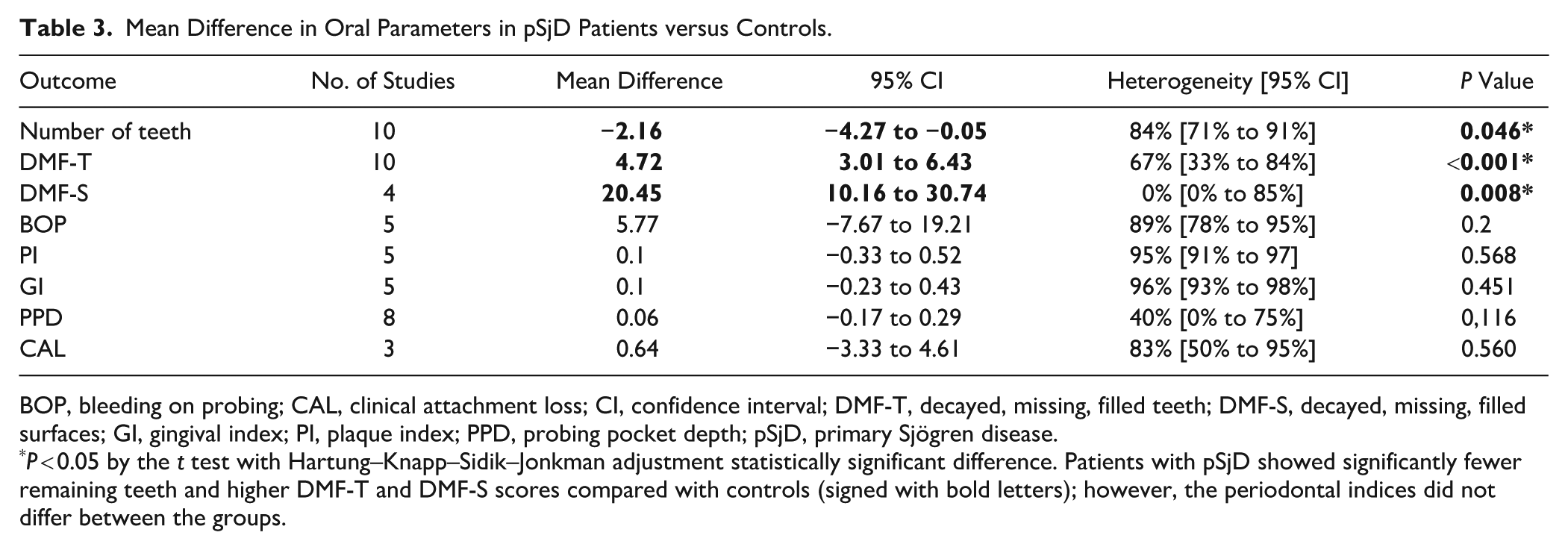
BOP, bleeding on probing; CAL, clinical attachment loss; CI, confidence interval; DMF-T, decayed, missing, filled teeth; DMF-S, decayed, missing, filled surfaces; GI, gingival index; PI, plaque index; PPD, probing pocket depth; pSjD, primary Sjögren disease.
P < 0.05 by the t test with Hartung–Knapp–Sidik–Jonkman adjustment statistically significant difference. Patients with pSjD showed significantly fewer remaining teeth and higher DMF-T and DMF-S scores compared with controls (signed with bold letters); however, the periodontal indices did not differ between the groups.
DMF-T in pSjD
Ten studies (Pedersen et al 1999; Koseki et al 2004; Leung et al 2004; Leung et al 2007; Rusthen et al 2019; Singh et al 2019; Martins et al 2022; Glavina et al 2023; Molania et al 2023; Xing et al 2023) involving 630 individuals were included in the analysis of the DMF-T score (Fig 3). The MD of DMF-T scores between pSjD and controls was 4.72 (CI: 3.01 to 6.43; I2 = 67%, CI: 33% to 84%; P = 0.001*), indicating that patients with pSjD had, on average, 5 more decayed, missing, or filled teeth. The SM values for DMF-T are presented in Appendix Figures 54 and 55.

MD of DMF-T in pSjD versus controls: Forest plot showing the mean difference of DMF-T in patients with and without pSjD. A significantly higher DMF-T score was observed among patients with pSjD compared with the control group (MD = 4.72, P < 0.001).
Quality of the Included Studies
The methodological quality of 49 studies was evaluated using the JBI checklists for proportions. Of these, 11 studies were found to have an overall low risk of bias, 35 studies had a moderate risk, and 3 studies were assessed as having a high risk of bias. With the QUIPS tool, 33 studies were evaluated, where 1 study had low risk and 32 had a moderate risk of bias. The primary sources of potential bias in the studies were a lack of information about confounding factors. The risk-of-bias assessments for each outcome are presented in Appendix Tables 2 to 5.
Heterogeneity
Heterogeneity was moderate to high across most analyses; therefore, additional subgroup and sensitivity analyses were performed to explore potential sources of variability. Subgroup analyses based on geographical region and study design were planned; however, these could not be conducted due to the limited number of available studies per subgroup. When feasible, these analyses did not meaningfully reduce heterogeneity, and in some cases, heterogeneity increased.
Subgroup analyses were conducted based on the diagnostic criteria, region, and study design for several outcomes, including candidiasis, dysphagia, oral ulcers, gingivitis, periodontitis, dysgeusia, halitosis, stomatitis, angular cheilitis, papillary atrophy, tongue fissuration, number of teeth, DMF-T, PI, GI, and PPD. These analyses showed a slight reduction in heterogeneity in some cases; however, no consistent pattern was observed, and firm conclusions could not be drawn.
The results of the sensitivity and subgroup analyses can be found in Appendix Figures 56 to 92 and Appendix Figures 93 to 164, respectively. Additional sources of heterogeneity may include differences in medication use, socioeconomic status, and oral health–related behaviors, which were not consistently reported across studies.
Publication Bias
Visual inspection of the funnel plots revealed varying degrees of asymmetry across outcomes. For the MD in the number of teeth and average number of teeth (SM), smaller studies tended to report more extreme estimates, suggesting potential small-study effects. Similarly, the funnel plot for DMFT demonstrated right-sided asymmetry, with smaller studies indicating higher DMFT values in pSjD patients. For prevalence outcomes, funnel plots of angular cheilitis and candidiasis showed noticeable asymmetry, while the dysphagia plot was difficult to interpret due to the limited number of studies and substantial variability in study sizes, including 1 large outlier. Overall, as these analyses have high heterogeneity and included few studies, the funnel plots may be unreliable and should be interpreted with caution (Appendix Figs 165–171).
Discussion
This systematic review and meta-analysis demonstrated that several oral disorders are significantly associated with pSjD. Patients exhibited fewer remaining teeth and higher DMF-T/DMF-S scores compared with controls. Oral manifestations, especially dysphagia and oral ulcers, may significantly impair quality of life and are negatively associated with patient well-being and overall oral health (McCoy et al 2021).
Oral candidiasis represents a clinically important complication in pSjD. Although Candida species are part of the normal oral microbiota, reduced salivary secretion in pSjD predisposes to fungal overgrowth (MacFarlane and Mason 1974). Our findings demonstrate that pSjD patients have approximately 10 times higher odds of developing oral candidiasis. Recurrent oral candidiasis, which is relatively common among patients with pSjD, may extend into the bloodstream or upper gastrointestinal tract, potentially leading to life-threatening systemic candidiasis (MacFarlane and Mason 1974; Lu 2021).
Reduced salivary production is a known risk factor for candidiasis. Saliva plays a key protective role by facilitating mechanical clearance of yeasts and bacteria from mucosal surfaces and delivering antimicrobial factors such as secretory immunoglobulin A, lysozyme, lactoperoxidase, histatins, calprotectin, and lactoferrin (Challacombe 1994). However, it remains unclear whether elevated candida levels are associated with reduced unstimulated and/or stimulated salivary flow rates. Radfar et al (2003) suggested that stimulated salivary flow may play a key role in influencing candida levels. Guobis et al (2011), however, found no association between low salivary flow rate and elevated candida counts. Interestingly, Chen et al (2022) reported that candida infection may increase the risk for developing SjD in women; however, no significant association was observed in men.
Mucosal alterations, including oral ulcers, stomatitis, angular cheilitis, papillary atrophy, and tongue fissuration, are also frequently observed in SjD. Patinen et al (2004), Likar-Manookin et al (2013), and Serrano et al (2020) have comprehensively described the prevalence of oral lesions in patients with SjD, reporting rates of 80%, 61.2%, and 57.4%, respectively. Our meta-analysis extends these findings by quantifying the increased risk of these conditions in pSjD patients compared with non-pSjD controls. Notably, oral ulcers did not show a statistically significant association, consistent with prior meta-analytic findings by Serrano et al (2018), which may reflect limited sample size and study heterogeneity.
Dysphagia has been frequently reported (Rhodus et al 1995), and our meta-analysis clearly shows a statistically significant increase in the risk of dysphagia in patients with pSjD, with an OR of 26.78. Its pathogenesis is likely multifactorial, involving esophageal dysmotility (Rosztóczy et al 2001), reduced salivary flow (Márton et al 2006; Eyigör et al 2017; Crincoli et al 2018), and immune-mediated damage to glandular and mucosal tissues of laryngopharynx (Eyigör et al 2017).
Dental caries and tooth loss are major concerns in pSjD. Saliva is essential for maintaining oral homeostasis by regulating microbial colonization, clearing biofilm, and neutralizing bacterial by-products (Boutsi et al 2000). Reduced salivary flow promotes bacterial plaque accumulation, especially in crevicular and marginal gingival regions, increasing susceptibility to caries. Consistent with previous findings (Najera et al 1997; Pedersen et al 1999; Koseki et al 2004; Leung et al 2004; Leung et al 2007; Singh et al 2020; Martins et al 2022; Stankeviciene et al 2024), our analysis demonstrated significantly higher DMF-T and DMF-S scores in pSjD patients, reflecting increased caries burden and accelerated tooth loss (Christensen et al 2001).
Periodontal disease, most commonly arising from periodontopathogen bacterial accumulation in dental plaque, is a principal cause of tooth loss in adults (Boutsi et al 2000). Since cariogenic and periodontopathogenic plaques differ, the severe tissue destruction seen in caries in pSjD patients is not observed in periodontal disease (Kuru et al 2002). No significant differences were observed in periodontal indices between pSjD patients and controls. The literature remains inconclusive about periodontitis (Ergun et al 2010), with several studies (Najera et al 1997; Celenligil et al 1998) reporting increased risk, while others (Kuru et al 2002; Pers et al 2005) have found no such association.
There may be several reasons behind the conflicting literature. One possible reason is the difference in how gingivitis and periodontitis are defined. However, the periodontal indices should not differ, because they are objective measures. Subgroup analysis could solve the inconsistencies in periodontal parameters, for example, by grouping the results according to region or oral health–related habits. Nevertheless, it was not feasible in this study due to the lack of articles available for these parameters.
Beyond quantitative salivary reduction, emerging evidence suggests that functional interactions between the oral microbiome and mucosal immunity may contribute to the pathogenesis of SjD. Specific oral bacteria can modulate epithelial immune signaling and maintain T-cell homeostasis, thereby influencing glandular inflammation and microbial composition (Tseng et al 2025). These findings indicate that dysbiosis in pSjD may not only reflect reduced salivary flow but also the altered host–microbe immune interactions at the epithelial interface, potentially contributing to loss of tolerance and chronic mucosal inflammation.
Increasing attention has been directed toward the oral virome and viral contributions to mucosal immune modulation. Viral infections of salivary tissues are recognized as contributors to chronic epithelial activation, cytokine production, and immune dysregulation in pSjD through interactions with toll-like receptors and upregulation of innate immune pathways. Viral components of the oral microbiome may influence immune responses and contribute to autoantibody production. (Otsuka et al 2022).
SARS-CoV-2 has been shown to infect the epithelial cells of the salivary glands and oral mucosa, with the expression of viral entry receptors in these tissues. Viral presence in saliva correlates with oral symptoms such as taste loss and mucosal lesions, highlighting the oral cavity as a site of viral replication and potential mucosal immune dysregulation (Huang et al 2021).
Increasing evidence supports bidirectional inflammatory crosstalk between oral and systemic autoimmune diseases. Periodontal inflammation and associated oral microbiota dysbiosis have been implicated in systemic immune activation in rheumatoid arthritis (RA), while similar microbiome–immune interactions may influence mucosal immunity and systemic autoimmunity in pSjD. Dysbiosis-driven molecular mimicry, epithelial barrier disruption, and aberrant B-cell activation suggest overlapping pathogenic pathways between RA and pSjD (Huang et al 2023).
Strengths and Limitations
Our comprehensive study used a rigorous methodology and included a diverse sample of data. The strengths of our study include the comprehensive assessment of a wide range of oral manifestations and parameters. Most of the studies also include age- and gender-matched controls, which enhances the reliability of our comparisons. However, a key limitation lies in the studies included in our meta-analysis, many of which lacked information on potential confounding factors, including smoking, oral hygiene habits, and the use of medications, and they were limited by small sample sizes.
Clinical and Research Implications
The translation of scientific evidence into practice is vital for patient benefit (Hegyi et al 2021; Hegyi and Garami 2025).
Since we know that patients with SjD have a high risk for oral manifestations, close collaboration between immunologists and dental professionals is important to optimize patient quality of life. Immunologists should involve dentists early to help maintain the oral health of patients with SjD, while dentists who observe findings related to SjD should refer these patients to immunologists.
Future studies should aim to address the key limitations identified in the current literature, particularly by accounting for potential confounding factors, which may influence the relationship between pSjD and oral manifestations. In addition, further research is needed to explore the association between disease activity and the severity or prevalence of oral symptoms. The development of evidence-based guidelines for dental care in patients with pSjD is essential to support clinicians in managing oral health more effectively, and closer dental monitoring is strongly advised and crucial for these patients. Ultimately, future investigations should focus on evaluating the effectiveness of preventive oral health interventions to improve long-term outcomes and quality of life in this patient population.
Conclusion
Patients with pSjD exhibit a substantially higher burden of oral complications, including candidiasis, dysphagia, dysgeusia, and various mucosal alterations, along with greater caries experience and fewer remaining teeth. These complications can significantly impair nutrition, daily comfort, and overall quality of life.
Author Contributions
Á. Heizer, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised manuscript; B. Szabó, Z. Sipos, contributed to conception and design, data acquisition, analysis, and interpretation, critically revised the manuscript; M. Kisgergely, J. Lee, X. Qian, G. Varga, P. Hegyi, K. Márton, contributed to conception and design, critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261450057 – Supplemental material for Oral Burden of SjÖgren Disease: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-jdr-10.1177_00220345261450057 for Oral Burden of SjÖgren Disease: A Systematic Review and Meta-analysis by Á. Heizer, M. Kisgergely, B. Szabó, Z. Sipos, J. Lee, X. Qian, G. Varga, P. Hegyi and K. Márton in Journal of Dental Research
Footnotes
Acknowledgements
We would like to thank Rena Hirose and Mizuki Hirukawa for their contribution to the translation and extraction of Japanese articles and Zsófia Vincze for her helpful comments on the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Centre for Translational Medicine, Semmelweis University, Hungarian Ministry of Innovation and Technology, National Research, Development and Innovation Fund (TKP2021-EGA-23 to Péter Hegyi), NKFIH project grants K131996 and K147265 (to Péter Hegyi). This study was supported by Semmelweis University Research and Innovation Fund.
Ethical Approval
No ethical approval was required for this systematic review with meta-analysis, as all data were already published in peer-reviewed journals. No patients were involved in the design, conducting, or interpretation of our study. The datasets used in this study can be found in the full-text articles included in the systematic review and meta-analysis.
Data Availability
All data analyzed in this study are available in the full text of the studies and supplementary material included.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.