
Abstract
The impact of oral health promotion efforts is hampered by a predominant focus on individual behavior and clinically oriented prevention, which addresses only a narrow part of the complex systems that influence oral disease outcomes. This article applies systems thinking to reorient oral health promotion toward deeper structural and societal determinants. The Action Scales Model (ASM) is introduced as a practical framework that distinguishes 4 interconnected levels at which action can be taken: events (what is happening), structures (how the system is organized), goals (what the system is set up to achieve), and beliefs (the assumptions and values that legitimize those goals and structures). Using the ASM, the oral health care and public health systems are examined to reveal where current efforts are concentrated and where opportunities for transformation lie. Most activity remains at the event level, where behavior change programs and treatment‑oriented care dominate. Structural features, such as financing mechanisms, workforce organization, and weak integration of oral health within public health systems, reinforce this narrow focus. At deeper levels, prevailing goals and beliefs continue to emphasize individual responsibility and market‑driven delivery rather than equity, prevention, and societal well-being. Meaningful system change requires shifting these underlying goals and beliefs, reframing oral health as a socially determined outcome and therefore a collective responsibility. While the ASM cannot fully capture complex realities, it offers a useful methodological framework to support reflection, dialogue, and more coherent system‑level action in oral health promotion.
Limitations of the Current Reductionist Approach in Dentistry
Oral diseases are highly prevalent and impose a substantial burden on individuals, health systems, and societies worldwide (Bernabe et al 2025). Despite decades of research and preventive efforts, socioeconomic inequalities in oral health persist globally, highlighting the limited effectiveness of current approaches in achieving sustainable and equitable improvements. A central critique, raised in the Lancet Oral Health Series, is that oral health promotion remains dominated by a reductionist paradigm, in which oral disease is primarily framed as a clinical and individual problem (Peres et al 2019; Watt et al 2019). Within this paradigm, interventions are largely curative or preventive—but medicalized—and delivered through the oral health care system. Preventive strategies typically focus on downstream risk factors and individual behaviors, such as oral hygiene or dietary choices. While these approaches have somewhat improved oral disease management, they are insufficient to address the complex determinants shaping oral disease outcomes across the life course.
Within the reductionist paradigm, oral health promotion strategies tend to target isolated components of the system. They often assume that behavior change occurs within a stable and predictable context, where individuals can act on information and motivation if adequately supported. In reality, health behaviors and outcomes are embedded in complex, dynamic systems shaped by social and commercial forces (Do et al 2023). For example, the pricing and marketing of sugar-rich products increase exposure to unhealthy foods and limit individuals’ ability to make personal choices (Alvarado et al 2023). Interventions that focus on a single leverage point (usually an individual risk factor) often ignore interactions and contextual influences elsewhere in the system. Therefore, they are unlikely to achieve sustained or equitable reductions in oral disease (Kay and Locker 1996).
These limitations underscore the necessity for a shift toward systems thinking in oral health promotion (Watt 2023). Systems thinking recognizes that health outcomes emerge from complex, interconnected systems rather than isolated risk factors. As Nobles et al (2022) described, these systems are unpredictable and interdependent, responding to political reforms, commercial interests, social norms, and technological changes through feedback loops that can reinforce or stabilize problems. From this perspective, the challenge for oral health promotion is to reconsider where and how action is taken within the system. Building on recent systems-based analyses in dentistry, the Action Scales Model (ASM) adds a much-needed structured methodological framework to support a shift by explicitly linking system understanding to action by identifying leverage points at increasing depths of system change (Nobles et al 2022). (Throughout this article, the term “oral health” is used pragmatically to refer to conditions and processes affecting the mouth and related structures. However, organ-specific conceptualizations of health may reinforce artificial boundaries within health systems. In line with systems thinking, these processes are understood as inseparable from general health and shaped by shared determinants.)
Description and Application of the ASM
The ASM was developed as a practical tool to plan actions in complex health systems, particularly for public health challenges such as obesity (Nobles et al 2022). The ASM can be situated within a broader landscape of systems thinking frameworks that are widely applied in the health and social sciences. Examples include Bronfenbrenner’s ecological systems theory (Bronfenbrenner 1979), the Toulouse–Montreal model (Bedos et al 2020), and frameworks that explicitly focus on leverage and system change, such as the Intervention Level Framework (Meadows 1999). Building on these earlier frameworks, the ASM aligns with approaches that distinguish between deeper and more visible domains of change while providing a unique operationalization.
The ASM identifies 4 interconnected levels of action: events, structures, goals, and beliefs (Nobles et al 2022). “Events” are the visible manifestations of the system, for example, fast food consumption. Actions at this level are often quick fixes with limited impact, such as awareness campaigns, as they do not change underlying system dynamics. “Structures” are the rules, processes, and organizational arrangements that shape these events, for example, regulations around food production. “Goals” reflect what the system is actually trying to achieve. A positive example is a company aiming to increase access to healthy foods, while a negative example is a company prioritizing sales of highly processed foods over nutrition. “Beliefs” are the deeply held norms, values, and attitudes of a system shaping goals and structures. A health-promoting belief might be that nutritious, affordable food should be accessible to everyone, whereas a health-adverse belief could be that profit and market growth are more important than public health. Changing beliefs in a positive direction can fundamentally transform how the entire system functions.
Although developed for obesity, the ASM has also been applied to other public health challenges, such as adolescent sleep schedules and healthy school food environments (Burton et al 2025; Heemskerk et al 2025). In this article, we adopt the ASM as a methodological framework, not as superior to others but as a practical tool for analyzing how systems function and identifying leverage points across multiple levels to address broader determinants and foster system-wide impact.
Analysis of Current Systems for Oral Health Promotion according to the ASM
Generally, oral health is primarily promoted through 2 interrelated systems: the oral health care system, which delivers individualized preventive and curative care, and the public health system, which implements population-level strategies to promote health. We focus on these 2 systems as primary entry points, while recognizing that oral health outcomes also emerge through broader health care, commercial, cultural, and regulatory systems (Marmot et al 2008). In this section, we analyze the oral health care system and public health system using the ASM from the European context (Fig.1).
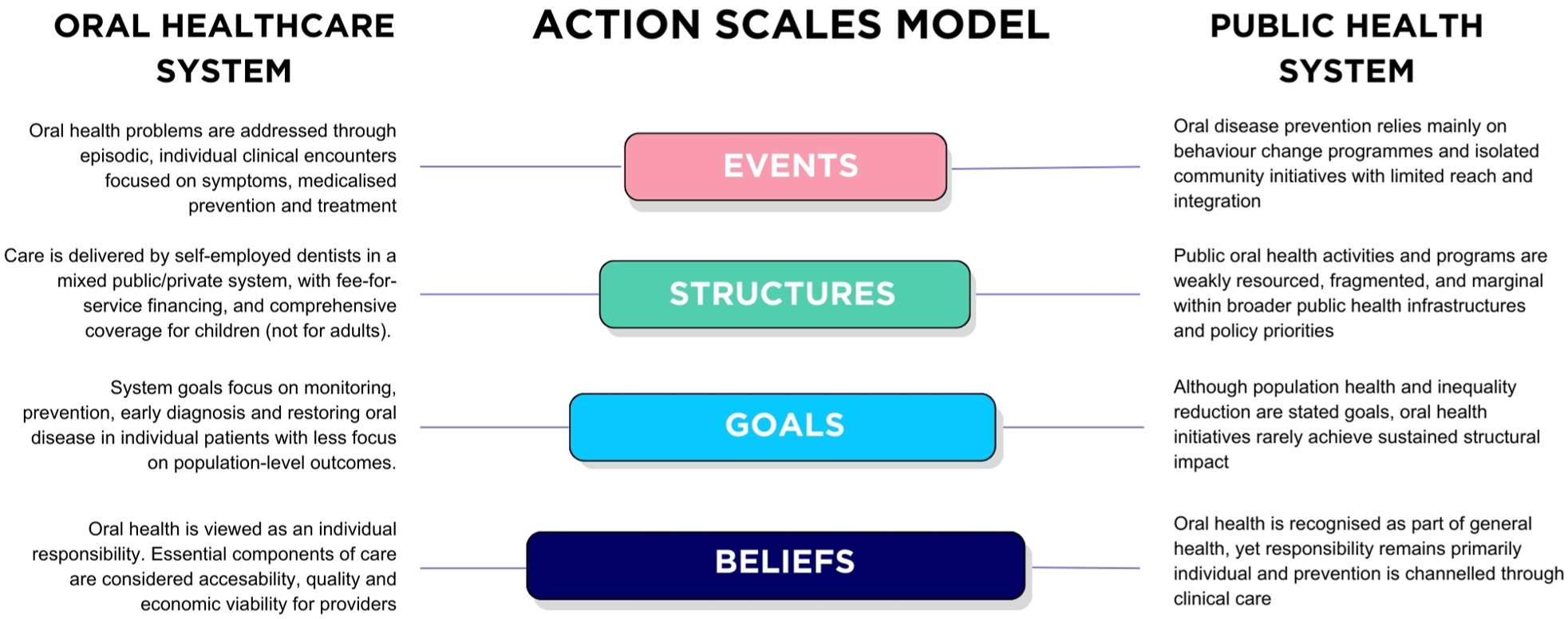
Analysis of the current oral health care and public health systems using the Action Scales Model.
The Current Oral Health Care System
Event Level
The event level reflects the visible manifestations of the European oral health care system, the day-to-day experiences of both patients and care providers. These include checkups, preventive interventions such as fluoride applications and oral health education, restorative treatments, and specialized procedures in secondary or tertiary care. Access and utilization vary: some populations face long waiting times or limited availability of professional care, while others receive rapid, high-quality care. Out-of-pocket costs, fee-for-service billing, and demand for aesthetic treatments further shape patient behavior and utilization patterns. These events illustrate a system’s focus on individual, treatment-oriented, and episodic (short-term) care (Winkelmann et al 2022a).
Structure Level
Across Europe, oral health care is predominantly organized as a mixed public–private system, with considerable variation between countries (Gallagher and Eaton 2015). Primary care is largely delivered by self-employed or privately contracted dentists, while secondary and tertiary services, such as oral surgery, specialized care, and orthodontics, are typically embedded in hospitals or referral practices. In some countries, preventive services are provided by dental hygienists or therapists. Public coverage is generally comprehensive for children and adolescents, whereas adult oral health care is often only partially covered or excluded from statutory health insurance. Financing mechanisms and reimbursement models tend to prioritize treatment-oriented, fee-for-service care. Access therefore remains closely linked to socioeconomic status, insurance coverage, and national policy contexts.
Goal Level
The goals of the European oral health care system largely align with the World Health Organization’s definition of oral health: to prevent diseases, detect pathology early, relieve pain, preserve function, and maintain or restore aesthetics, supporting overall health, well-being, and quality of life (World Health Organization 2022). These goals are particularly emphasized in publicly funded care for children, where prevention, oral health education, and risk-based recall systems are routinely implemented. However, these goals are predominantly oriented toward individual care, focusing on the treatment needs of individual patients rather than population-level outcomes. At the same time, the system is influenced by implicit goals embedded in its financing and delivery models, including maintaining practice viability, revenue generation, and responsiveness to patient demand.
Belief Level
The European oral health care system is underpinned by deeply held beliefs that both enable and constrain its functioning. At its core is the conviction that oral care should be accessible, safe, high quality, and affordable, reflecting professional standards and social responsibility (Winkelmann et al 2022b). Complementing this is a strong belief in individual responsibility for oral health, with prevention, through hygiene, diet, and routine checkups, considered central. While widely valued, prevention is primarily individually targeted and reductionist, and it is structured to ensure providers’ financial viability, making it both health promoting and commercially incentivized.
Critically, conditions affecting the mouth are often treated as distinct from general health within health systems and policy. This reinforces siloed approaches and limits integration with broader public health strategies. Dentistry is generally market driven and libertarian, with treatment prioritized for those able and willing to pay. Elements of utilitarian, egalitarian, and restorative approaches exist, particularly in child prevention programs, subsidized care for low-income adults, and targeted services for socially marginalized groups. This reflects a mixed and sometimes conflicting landscape of priorities and access. Together, these beliefs shape the goals and structures of the system, influencing how care is delivered and who ultimately benefits.
The Current Public Health System
Event Level
Oral disease prevention is primarily delivered through oral health care providers within the oral health care system, rather than through a dedicated public health infrastructure. In most European countries, public oral health promotion remains limited (Durvy et al 2025). Implemented activities typically include behavior change programs and campaigns, often narrowly focused on health education, alongside community- or school-based initiatives such as fluoride programs and diet-related policies (Akera et al 2022). The reach, intensity, and quality of these initiatives vary widely across European countries. Many initiatives remain isolated, lack a robust evidence base, and are rarely integrated into broader public health promotion strategies following the Common Risk Factor Approach (Watt and Sheiham 2012; Durvy et al 2025). Consequently, most programs fail to address the underlying structural determinants of oral health. In the context of systems thinking, prioritizing oral health upstream means acting not only on shared risk factors but also on the structural, commercial, policy, and institutional conditions through which those risks are produced and distributed.
Structure Level
Oral health promotion operates across multiple levels, including national policies, local community programs, schools, workplaces, and public health institutions. In some countries with well-resourced public health services, extensive programs exist (Ross et al 2023). However, in many European countries, funding, attention, and prioritization remain limited, despite statutory mandates. National health promotion policies typically focus on broader issues, such as obesity and lifestyle, with only indirect consideration of oral health.
Goal Level
The goals of the public health system include preventing disease, promoting healthy behaviors, and reducing inequalities, with oral health being integrated into these goals. In contrast to individual oral health care, these goals target population-level impact and aim to address underlying determinants at family, community, and structural or societal levels. In practice, the often isolated, narrowly focused, and underfunded nature of public oral health initiatives limits their long-term effectiveness.
Belief Level
Public oral health promotion is underpinned by the belief that governments have a statutory responsibility for health promotion and that oral health is an integral part of general health (World Health Organization 2024). Implicit in this belief is the notion that individuals are primarily responsible for their own oral health, with the clinical oral health care system serving as the main channel for prevention. Although population-level interventions are conceptually valued, oral health tends to receive less explicit priority within public health agendas compared with other public health issues, and collective responsibility receives limited emphasis (Benzian and Loistl 2022). The focus remains largely on individual-level behavior and interventions delivered via the oral health care system rather than coordinated, society-wide strategies.
Leverage Points for Oral Health Promotion according to the ASM
Table 1 summarizes key leverage points for oral health promotion within the oral health care system and the public health system, structured according to the 4 levels of the ASM. Together, these leverage points illustrate how action can shift from visible, short-term practices toward deeper system goals and beliefs that shape oral health outcomes over time.
Leverage Points for Transformative Oral Health Promotion across Oral Health Care and Public Health Systems, Structured by the 4 Levels of the Action Scales Model.
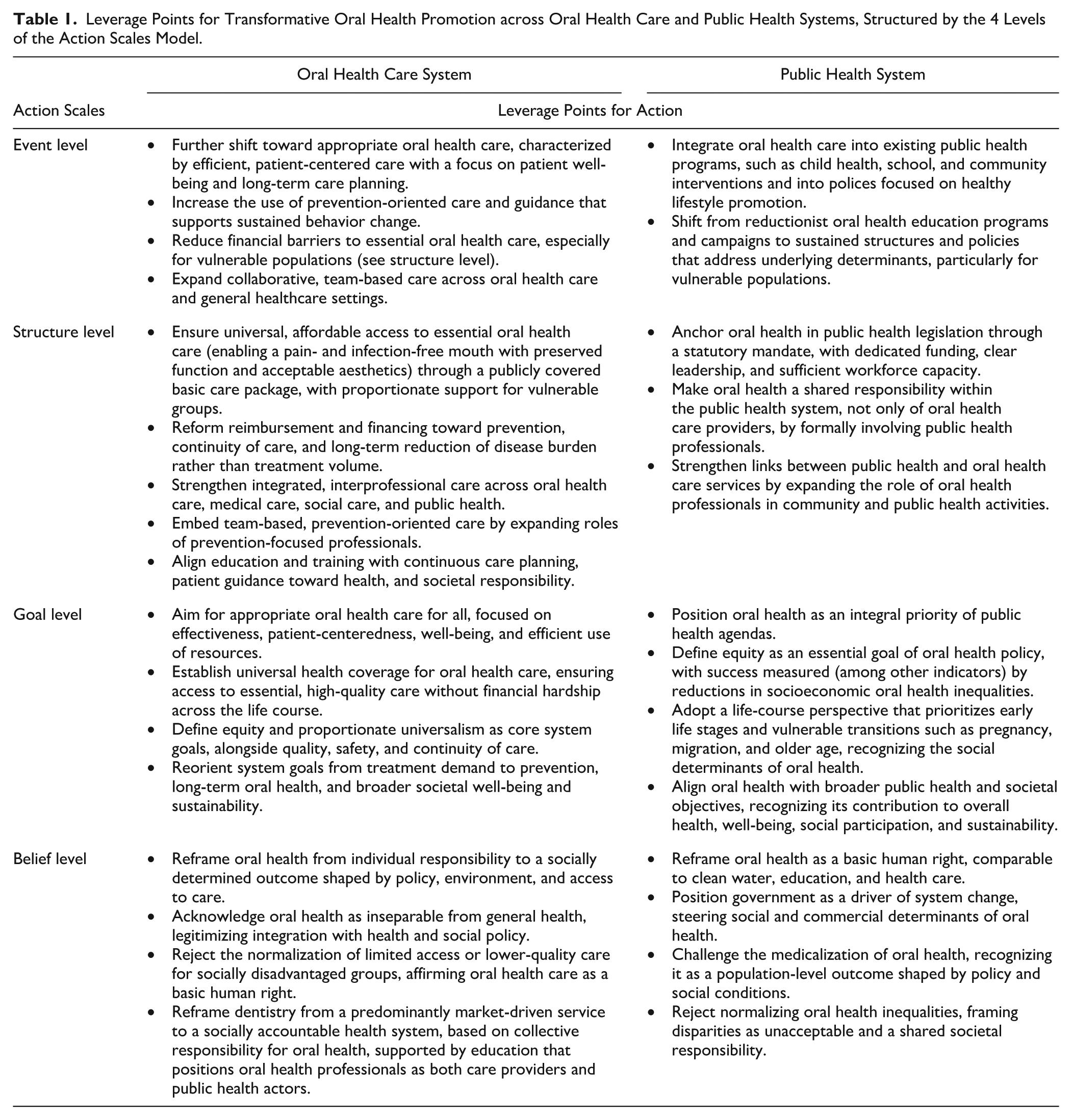
At the event and structure levels, proposed actions focus on reorienting oral health care delivery and public health practice toward prevention, continuity, and integration while reducing financial and organizational barriers to essential oral health care. At the goal level, both systems are aligned around shared objectives, including appropriate care for all, universal coverage, equity, and a life-course perspective that links oral disease to broader societal well-being and sustainability. At the deepest level (belief level), leverage points focus on the shifts required to enable durable system change. This includes reframing oral health as a socially determined outcome, affirming oral health care as a basic right, and redefining the roles of both governments and professionals in promoting population oral health.
An In-Depth Reflection
Generally, models offer useful ways of understanding (oral) health systems, but they cannot fully capture their complexity or offer practical solutions. Any attempt to systematize action inevitably simplifies reality and foregrounds certain perspectives over others. Rather than presenting the ASM as a definitive solution, we position it as a conceptual or methodological framework for reflection and dialogue on how oral health systems function and where opportunities for system-level change can be identified. This responds to needs that are increasingly articulated in global oral health policy agendas (Gallagher et al 2026).
Distinctions such as prevention versus treatment, or dental versus medical domains, are used here pragmatically for clarity. However, from a systems perspective, these categories are not discrete but reflect institutional ways of organizing action, while in reality actions are dynamic and operate across multiple levels within health systems. Applying the ASM reveals a persistent misalignment between the layered complexity of systems influencing oral health and the tendency of most current interventions to operate through simplified representations of these systems. While oral disease outcomes are shaped by interconnected social, commercial, and policy forces, action remains predominantly concentrated at the level of events and, to a lesser extent, structures.
Similar critiques are increasingly recognized across health sciences, where there is growing consensus that persistent inequalities, unsustainable cost trajectories, and limited preventive impact are symptoms of deeper system characteristics rather than isolated policy failures (Rutter et al 2017). This insight underpins a broader shift toward systems thinking and transformative approaches in health care. Within dentistry, this perspective is echoed by increasing attention to social, commercial, and political determinants of oral health, alongside the realization that systems science can provide a basis for repositioning oral health care as a contributor to broader health goals (Peres et al 2019; Dritsch et al 2025).
However, recognizing the need for systems transformation does not make acting on it any easier. System change is inherently challenging, particularly when it confronts established professional norms, institutional arrangements, and economic interests (Best et al 2012). Health care systems are shaped by past decisions, which favor incremental over more fundamental reform. Short-term decision-making, driven by political cycles, budget constraints, and activity-based performance indicators, further reinforces this pattern (Bayat et al 2023). And in oral health care, these dynamics are often stronger because services in many countries are organized around market-based models. In such systems, goals related to population oral health frequently come into tension with fee-for-service incentives and commercial pressures.
Growing attention to environmental sustainability, workforce limitations, and value-based care is placing new demands on how services are organized and delivered (Aftab et al 2020; Van Hoorn et al 2024). From this perspective, system-oriented approaches are desirable in principle, but they are also relevant in practice. They can help orient action toward integrated, prevention-focused, and resource-conscious strategies aligned with broader developments in health policy and management.
A final question, however, is how changes in system goals and underlying beliefs can be achieved in practice. Such shifts are inherently challenging. In practice, they often begin when prevailing assumptions are questioned in public and professional debate, for example, through policy reports, media attention, or professional and civil society advocacy. Periods of political or societal momentum translate these discussions into actions, such as fiscal measures, regulatory changes, or reforms in education and professional practice (Stennett et al 2025). When sustained across sectors, these actions can gradually reshape institutional arrangements and everyday practices, making alternative ways of thinking more feasible and legitimate. Over time, this alignment can support more fundamental shifts in system goals and beliefs.
Conclusion
Advancing oral health promotion requires more than extending existing interventions or fine-tuning delivery mechanisms. It involves a paradigm shift that addresses the deeper goals and beliefs shaping health systems and sustaining current patterns of action. The ASM provides a methodological approach to clarify where action is currently focused and where greater potential for change lies. By positioning oral health within broader debates on transformation, equity, and sustainability, the ASM helps stakeholders orient priorities toward long-term societal well-being.
Author Contributions
D. Duijster, M. de Jong-Lenters, C.M.C. Volgenant, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised manuscript. All authors contributed equally to this manuscript, and all authors gave their final approval and agreed to be accountable for all aspects of the work. All edits were verified by the authors, who take full responsibility for the final content.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to dr.ir. S.C. Dijkstra for bringing the action scales model to our attention. No new data were generated or analyzed in this study, so data sharing is not applicable to this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.