
Abstract
This study examined the role played by aftercare following (mainly) inpatient community-based treatment in the outcomes of criminal ex-offenders with substance use disorders. Two hundred seventy individuals who had been released from the criminal justice system were randomly assigned to either a therapeutic community (TC), recovery homes called Oxford Houses (OHs), or usual care settings (UA). The OHs and TCs are residential settings that emphasized socialization and abstinence from drugs and alcohol, but OHs do not include the formal therapeutic change interventions common to TCs, nor do they include any on-site access to drug abuse or health care professionals. UA involved what occurred naturally after completing treatment, which included staying with friends or family members, their own house or apartment, homeless shelters, or other settings. Longer lengths of stay in either the TCs or OHs were associated with increased employment, and reduced alcohol and drug use. Those assigned to the OH condition received more money from employment, worked more days, achieved higher continuous alcohol sobriety rates, and had more favorable cost–benefit ratios.
About 1.6 million individuals are incarcerated in state and federal prisons (West & Sabol, 2008), and more than 650,000 offenders will return from prison to their families, communities, and society each year (Hughes & Wilson, 2003). Many of these ex-offenders are released from prison with ongoing drug addictions. While many factors contribute to criminal recidivism, such as lack of employment or housing, the strongest predictor of criminal recidivism is substance use (Jason, Olson, & Foli, 2008). Regrettably, the process of integrating ex-offenders into society after release is often poorly implemented (Jason et al., 2008).
One of the most effective ways of reducing criminal recidivism is through substance abuse treatment and intensive prison-based drug treatment programs (Pelissier et al., 2001). Reductions in recidivism rates have been documented when in-prison therapeutic communities (TCs) have been combined with community transition programs, many of which have been based on the TC model (Hiller, Knight, & Simpson, 1999). For example, Inciardi, Martin, and Butzin (2003) found that at a 5-year follow-up, those who participated in a TC aftercare program had significantly less drug use and were significantly less likely to be reincarcerated compared with those in a regular work release aftercare program. TCs are among the most common types of professional, staff-run residential settings for substance abuse treatment (De Leon et al., 1985). TCs vary widely in overall capacity, staffing and training, program philosophies, and services for residents’ personal or professional growth, and they often incorporate mutual self-help principles in their treatment milieu (De Leon et al., 2008). TC aftercare programs are well respected and researched (Melnick et al., 2001; Pelissier et al., 2001). In TCs, staff and residents share work responsibilities and residential stays range from 6 to more than 15 months (De Leon, 1985). TCs provide residents with a supportive abstinent social support system, which is likely to increase self-efficacy, and has a phased structure with an emphasis on various therapies including behavioral, cognitive, and relapse prevention.
Halfway houses and TCs offer professionally led environmental support following substance use treatment and involvement in the criminal justice system. Halfway house is a common terminology for transitional living, especially for ex-offenders, but it may not always provide a treatment atmosphere. In addition, increasingly, substance abuse treatment programs are providing briefer formal programs, often followed by a referral to Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) and an expectation to refrain from substance use. Many professional-led treatment settings also have restrictions on length of stay and high cost (Polcin & Henderson, 2008). This is unfortunate particularly in light of Vaillant’s (1983) findings that environmental factors (amount and type of support) may be key contributors to whether or not individuals maintain abstinence after treatment and criminal involvement.
Recovery homes are another type of community-based residential program for people with substance use disorders (Polcin & Henderson, 2008). Typically, residents can stay for as long as they want, but they are required both to abstain from substance use and to pay a modest rent to the recovery home owner. Often, the residents are provided some opportunities for self-governance, but typically, the staff and/or owner determine who can enter the recovery homes, how long residents can stay in these settings, and how rules are enforced. Although staff live in some of these traditional recovery homes, it is more common for staff to regularly visit and monitor these settings. Researchers have long maintained that recovery homes are an essential component of the solution for a wide range of offenders (Steadman, Morris, & Dennis, 1995). In the recently released National Drug Control Strategy (2013), the Obama Administration has prioritized the further development of recovery support services and recovery-oriented service systems, and a number of studies were cited as evidencing the effectiveness of this approach, including those involving abstinent recovery homes (e.g., Jason, Olson, et al., 2007).
Oxford Houses (OHs) are one type of self-run, abstinent recovery homes for individuals dealing with substance abuse problems. Since its inception in the 1970s, the number of OHs has grown to more than 1,700 nationally. Furthermore, many of these homes contain individuals who have been released from jail. No professional staff are involved with these OHs; residents live together in a democratic, moderately sized, single-sex, single-family home and provide each other with a supportive abstinent social support network. The OH network of substance abuse recovery homes has been placed on SAMHSA’s National Registry of Evidence-Based Programs and Practices (2011).
A key question is whether community-based recovery supports can have an effect on the high costs of substance abuse to our society. Olson et al. (2006) found that costs associated with the OH program were relatively low, whereas costs associated with inpatient and incarceration history prior to entering OHs were high. This study, however, did not compare the costs and benefits of those in OHs with those in a comparison condition. In another study, individuals who completed treatment at alcohol and drug abuse facilities were randomly assigned to live in an OH or usual community-based aftercare services (Jason, Olson, Ferrari, & Lo Sasso, 2006). A 24-month follow-up found that only 31% of participants assigned to the OH condition reported substance use compared with 65% of usual aftercare (UA) participants. OH participants earned roughly US$550 more per month than participants in the UA group. When using the public payer perspective, which does not include the rent and expenses associated with the OH treatment modality as the residents paid these expenses out of their own pocket, the net benefit for OH was US$31,043 per person (Lo Sasso, Byro, Jason, Ferrari, & Olson, 2012). This study did not compare OH with a staff-administered treatment program such as a TC.
Several important questions relevant to public health issues remain unclear in the scientific literature regarding TC aftercare. For example, it is unclear whether the main therapeutic effect of TC aftercare is TC substance abuse treatment or alternative aftercare that provides a similar living environment but offering little or no therapeutic intervention. Typically, TC aftercare outcomes are compared with aftercare-as-usual, which can range across a wide variety of interventions. Few, if any, comparison groups have included a residential setting that emphasizes socialization and abstinence from drugs and alcohol—a hallmark of TC aftercare settings. In other words, it is important to compare the relative effectiveness of TC aftercare with an aftercare alternative that provides a supportive living environment without the professional treatment of TC aftercare. OHs provide, like TCs, a residential setting that emphasizes socialization and abstinence from drugs and alcohol, but they do not include the formal therapeutic change interventions common to TCs, nor do they include any on-site access to drug abuse or health care professionals. A comparison of TCs with OHs would possibly clarify the value added to TC aftercare intervention processes not present in OHs, particularly if both conditions could be also compared with a UA condition. Knowledge of the various environments that directly and possibly additively contribute to long-term abstinence could guide public health and criminal justice resource allocation decisions.
The present study compared TCs, OHs, and UA. The TCs and OHs are aftercare treatment modalities that hold promise in providing ex-offenders protective factors from high-risk environments. In addition, our study examined the economic costs and evaluated the dollar value of benefits that accrue. TCs with professional staff were hypothesized to be more effective in creating a stable abstinence support system, and helping residents find maintain abstinence and employment as well as reduce recidivism than OH recovery homes or UA. However, it was hypothesized that OH recovery homes would have cost–benefit advantages compared with more traditional TC modalities and UA.
Method
Participants
A total of 270 adults (224 men, 46 women) agreed to participate in the Chicago metropolitan area. All participants were recruited through inpatient substance abuse treatment facilities or reentry/case management programs. Ninety-three percent of the participants (n = 251) were recruited from inpatient treatment facilities where they were receiving inpatient services. Five percent of the participants (n = 13) were referred to the project through inpatient treatment facilities, although the participants themselves were not receiving inpatient services at the time of recruitment. Two percent of the participants (n = 6) were referred through reentry/case management services.
Recruitment began in March 2008 and continued through May 2011. Participants eligible for inclusion were above the age of 18, recovering from alcohol and drug dependence, and had been released from prison or jail within the past 24 months. Participants were excluded from the study if they refused random condition assignment or had been convicted of violent crimes or sex offenses. This latter exclusion was due to the TC not accepting these types of high-risk clients, so we had to impose similar recruitment restrictions on all conditions. Of the participants approached, 26 were excluded for eligibility violations (no substance use, no criminal history, convicted of violent crimes, etc.), 13 were not interested in the study, and 15 refused their random condition assignment.
Procedures
After providing informed consent, participants were randomly assigned to UA, OH, or TC via a random number table. A random number generator was used to produce a numerical set of 270 digits between 1 and 3. This set was subdivided into 90 three-digit sets with numerical values ranging between 1 and 3. This randomized block approach to the condition assignment procedure was utilized to ensure that the sample size across the three conditions would be equal, with 90 participants assigned to each condition. When the interviewer met with the participant for the first time, the interviewer was provided with a sealed envelope. The sealed envelope contained the participant number and the condition that the participant was assigned to.
UA involved what occurred naturally after completing treatment. Those in the UA condition were discharged and went to a variety of places, including staying with friends or family members, their own house or apartment, homeless shelters, or other settings.
The OH condition involved an OH recovery home. OHs are self-run, abstinent settings for individuals dealing with substance abuse problems. There are about 65 OH recovery homes in Illinois, and for this study, we focused on 23 of them that are in the Chicago metropolitan area. Residents can remain in these settings as long as they pay their rent, which is about US$100 a week, abstain from any alcohol or drug use, and comply with assigned weekly chores. In other words, each of the OHs is self-governing without any professional staff, and each of the OHs follow these basic rules. Some OHs are for females and others are for males, but none include both sexes.
For comparison purposes, we selected a TC that is a licensed, private organization in Chicago providing a structured sober living residential program with staff for persons in recovery. Approximately 70% of residents in this TC are men and 30% are women, which matches the gender ratios for OHs in Illinois. As in most TCs, residents in the TC we selected occupy a two- or three-person unit that is fully furnished by the organization and residents must follow a regimented program of recovery supervised by trained staff and site managers. Some units are for males and others are for females. Residents are required to have random urine testing for substance abuse. For the first few months, all residents must attend five self-help meetings per week, make a minimum of four “recovery-related” phone calls per week (through which they receive a sponsor’s support), and obtain full- or part-time employment. During later months, residents can serve as role models and help orient newer residents, attend four 12-step meetings a week, continue making four phone calls to their sponsors, and move toward financial stability. After 12 months, residents can move to independent living arrangements that are owned by the TC, continue random drug screening tests, and follow a regimented plan of recovery.
To assess the fidelity of the TC as a setting consistent with a TC, two high-level administrators at the TC were interviewed on the TC Scale of Essential Elements Questionnaire (SEEQ; De Leon & Melnick, 1993). The SEEQ measures a variety of characteristics of a TC. This includes the TC perspective, treatment approach and structure. It also assesses the “community as therapeutic agent,” education and work activities, and therapeutic elements and process. Each item is rated on a 5-point scale, with higher scores indicating more fidelity to the TC model. In every category, this setting was determined to be a TC setting (the overall average of the scores was M = 4.62, SD = 0.72). Of a possible total score of 755, the TC scored a 697. In summary, across multiple items under each TC perspective, the agency’s treatment approach and structure, the community as a therapeutic agent, educational and work activities, and formal therapeutic elements and process, the TC was determined to be a “therapeutic community.”
Participants assigned to OHs or TCs were given rides to placements after completing baseline measures, whereas participants assigned to UA made their own post-treatment arrangements. Participants received US$40 for completing their baseline interviews and US$40 for each of the subsequent waves. Follow-up interviews were conducted every 6 months over a 2-year period, yielding five assessments in total. Interviewers used data from tracking sheets provided by participants to facilitate contact for 6 (Wave 2), 12 (Wave 3), 18 (Wave 4), and 24 (Wave 5) month follow-up interviews. Interviewers had bachelor’s degrees and prior experience interviewing.
Follow-up interviews were conducted on-site whenever possible, and participants received 24-h Chicago Transit Authority (CTA) passes (which allow access to the public transportation system) in addition to US$40 for on-site interviews. In cases where on-site interviews were not possible, participants completed phone interviews or were met by interviewers at off-site locations. Off-site interviews were conducted in private when possible, but on occasion it was necessary to conduct interviews in restaurants, libraries, or other public locations. Those assigned to the OH condition stayed in these settings a mean of 91.61 days (SD = 141.99), whereas those assigned to the TC resided in this facility for a mean of 60.61 days (SD = 79.29). Dose was defined at the number of days in the OH or TC. By the 24-month follow-up, we were able to interview the majority of the participants in each condition: OH (74/90 = 82%), TC (73/90 = 81%), and UA (70/90 = 78%). Over the course of the study, two individuals in the OH and UA conditions, and one individual in the TC condition died. Most attrition was due to our interviewers not being able to find a way of contacting the participants.
Measures
Demographic survey
A set of demographic questions were used to elicit information regarding race/ethnicity, gender, age, and date of birth. Additional questions focused on participants’ current treatment setting and incarceration history.
Psychiatric problem severity
The Addiction Severity Index-Lite (ASI-Lite; McLellan, Cacciola, & Zanis, 1997), a briefer version of the Addiction Severity Index (ASI; McLellan et al., 1992), was used to assess problems in areas commonly affected by substance dependence. The ASI-Lite assesses potential problems for the respondents, and includes items assessing alcohol and drug use over the past 30 days. For the legal composite domain, higher scores indicate greater problem severity. The ASI was used to assess employment income, number of days of paid work, income from illegal sources, days incarcerated, and times treated for psychiatric problems in a hospital. The ASI has good internal consistency, excellent predictive and concurrent validity (McLellan et al., 1992), and the ASI-Lite has been demonstrated as being quite comparable with the ASI with good validity and reliability (Cacciola, Alterman, McLellan, Lin, & Lynch, 2007).
Timeline followback
Six months alcohol and drug use outcomes were measured using Miller and Del Boca’s (1994) Form 90 Timeline Followback. This instrument was used to measure alcohol and drug use. This instrument provides a linear measure of substance consumption over 90 days; however, as we collected data every 6 months we expanded this time to 180 days. Respondents were asked to construct a 180-day calendar marking important days and events (e.g., employment, health care utilization, incarceration, drug use). A retrospective substance use interview provides a reliable time frame for abstinence assessment (Miller & Del Boca, 1994). Test–retest reliability is excellent for core substance abuse variables.
Urinalysis
During Wave 5, if participants reported that they have been abstaining from illegal and alcohol use, a urinalysis test was used to confirm their self-report. We used ACCU, a full-service laboratory familiar with large-scale research protocols. If self-report data indicated that the person was abstinent, but urine data indicated that the person was using, the person was counted as using.
Drug Abuse Treatment Cost Analysis Program (DATCAP)
The DATCAP (French, 2003) was administered at the beginning of data collection. The DATCAP is a cost evaluation instrument that assesses the full range of economic costs of various types of addiction treatment modalities (French, 2002; French, Salomé, & Carney, 2002).
Statistical Analyses
We used a Generalized Linear Mixed Model (GLMM) to assess our major outcomes in the areas of substance use and employment. The GLMM predicts a continuous or categorical target based on one or more predictors. GLMM is a particular type of mixed model, and the linear predictor may contain random effects in addition to the fixed effects. The random effects are assumed to have a normal distribution, although sometimes the random effect may be excluded. As this is a multilevel model, if the data are missing at Level 2, the person is deleted. However, if the data are missing at Level 1, it uses the available data and still estimates the model using that person’s data. This model allows for nested data structures, including longitudinal designs. The main hypotheses used the intent-to-treat approach, including all participants. We report all p values, but we a prior considered levels of <.05 as significant, and all tests were two-tailed.
Results
Table 1 summarizes socioeconomic data for the three conditions. Age was significantly different across the conditions, F(2, 267) = 6.30, p < .01, with those in the TC being older than those in either the OH or UA conditions. Therefore, age was controlled for in all subsequent analyses. The sample had an average 10.9-grade education, and had been treated in the past for alcohol and substance abuse problems three to four times. The sample had been previously incarcerated an average of 9.9 times, with their most recent incarceration averaging 15.4 months, and they had been most recently released from prison for an average of 144.3 days. Regarding race, 74.1% of the sample were African American, 21.1% were White, 3.3% were Hispanic, and 1.5% other. Regarding marital status, 74.9% had never been married, 18.3% were divorced/separated/widowed, and 6.9% were married or remarried. In terms of occupations, the largest category was unskilled and this represented from 37 to 43% of the sample. Heroin had been the main substance of choice for 43.2% of the sample, and this was followed by 28.9% for crack/cocaine, 14.7% for alcohol, 7.1% for marijuana, 5.6% for polysubstance use, and 0.4% for amphetamine/crystal methamphetamine.
Socio-Demographic Variables of Participants at Baseline.
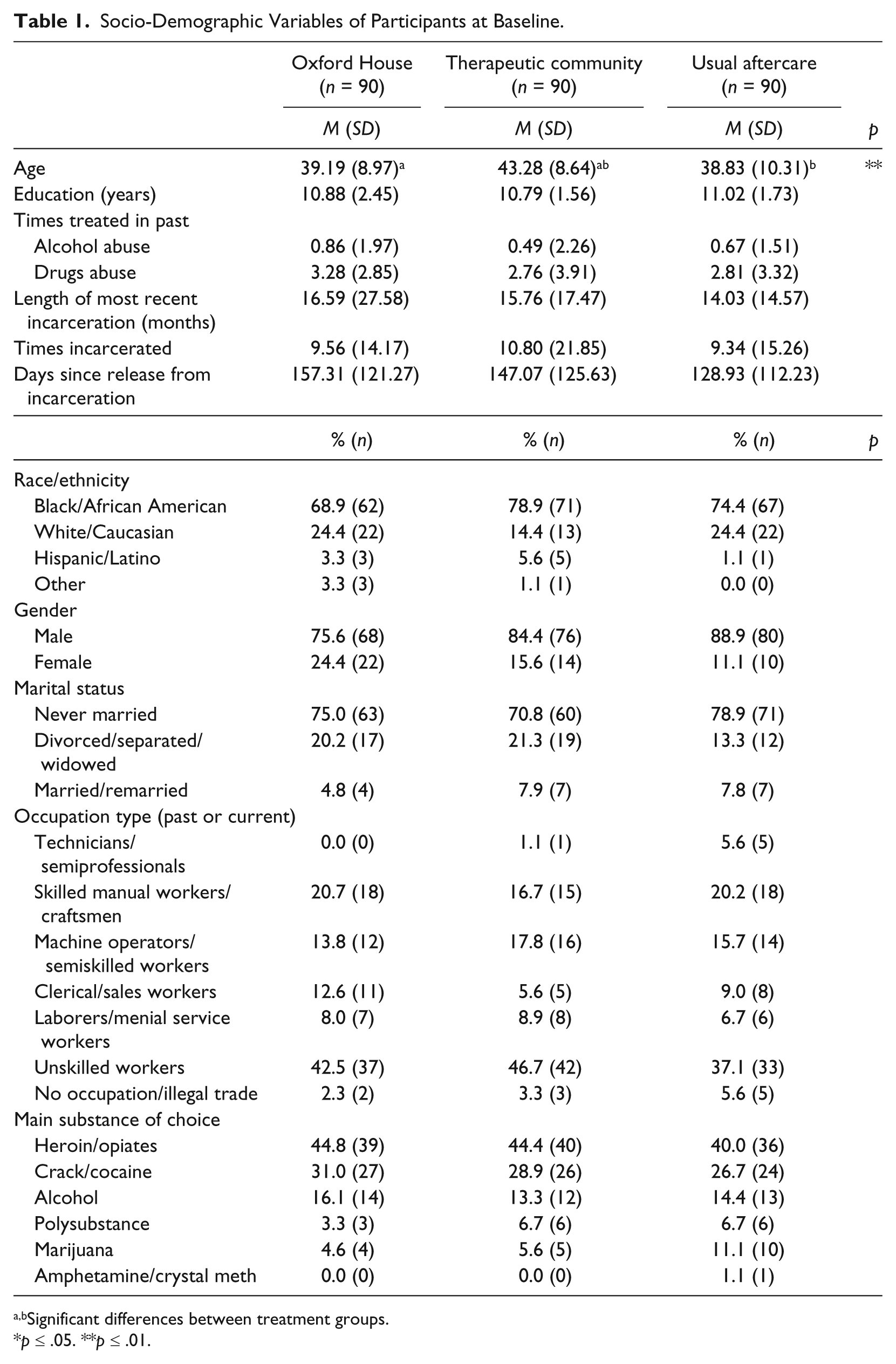
Significant differences between treatment groups.
p ≤ .05. **p ≤ .01.
Substance Use Outcomes
Table 2 presents data on the major outcome variables over time. Table 3 contains the findings from the GLMM. Group refers to the three conditions (OH, TC, or UA), time refers to the five waves of data collection, and dose was defined as the number of days in the OH or TC. For the number of days using alcohol over the past 6 months, there was no significant effect for condition, time, time by condition interaction, or the covariate age. There was a significant dose effect for alcohol, indicating that a higher dose led to lower days using alcohol.
Outcome Data Over Time.
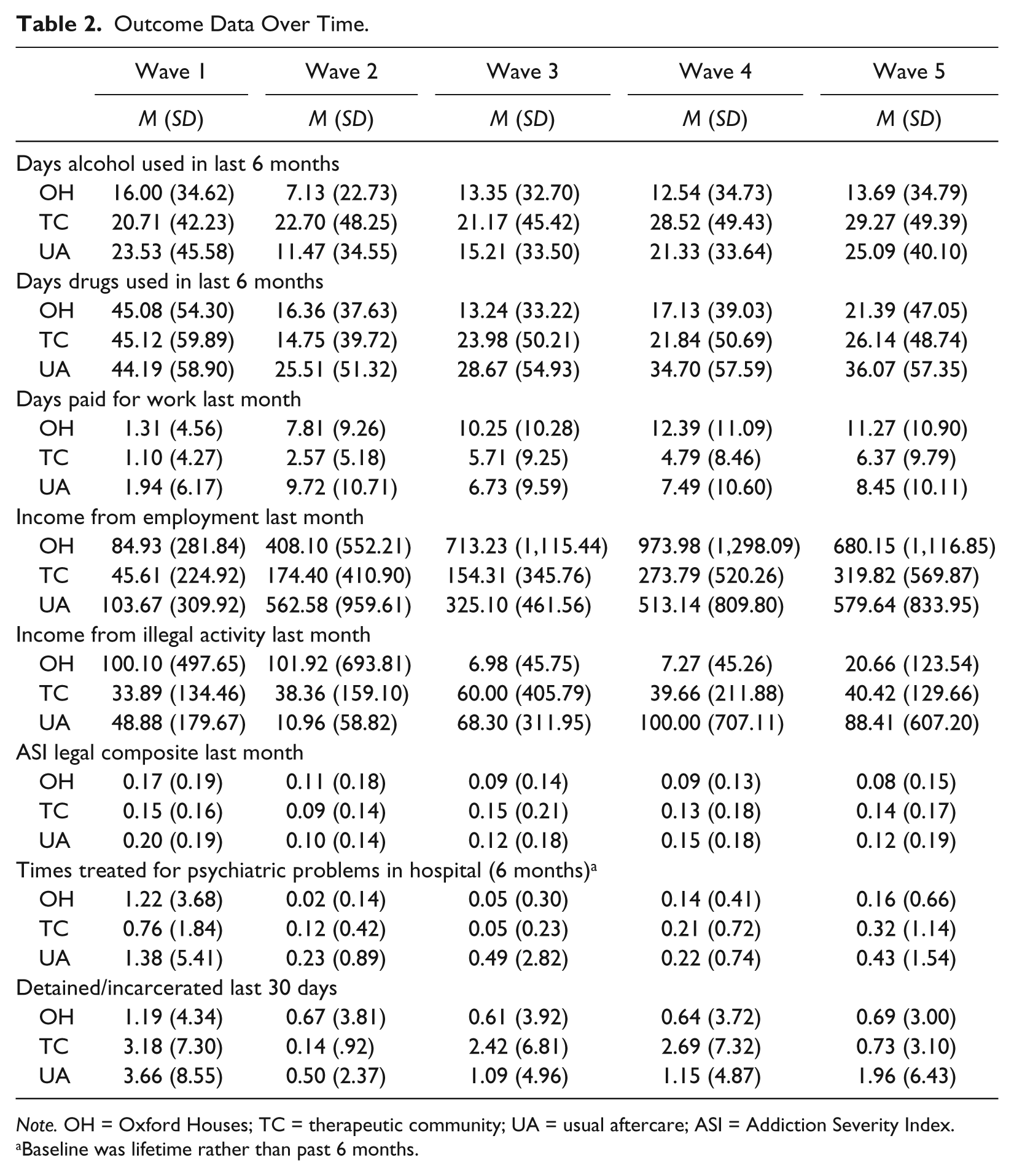
Note. OH = Oxford Houses; TC = therapeutic community; UA = usual aftercare; ASI = Addiction Severity Index.
Baseline was lifetime rather than past 6 months.
GLMM for Major Outcomes.

Note. GLMM = generalized linear mixed model; ASI = Addiction Severity Index.
For the number of days using alcohol over the past 6 months, there was significant variability around the intercept due to person, σ2 = 21,584.12, Z = 22.03, p < .001.
For the number of days using drugs over the past 6 months, there was significant variability around the intercept due to person, σ2 = 2,642.61, Z = 22.03, p < .001.
For the number of paid days worked in the last 30 days, there was significant variability around the intercept due to person, σ2 = 75.71, Z = 21.65, p < .001.
For money received from employment over the past 30 days, there was significant variability around the intercept due to person, σ2 = 476,577.81, Z = 21.69, p < .001.
For illegal income earned during the last 30 days, there was significant variability around the intercept due to person, σ2 = 127,724.56, Z = 21.70, p < .001.
For the ASI legal composite score over the last 30 days, there was significant variability around the intercept due to person, σ2 =.03, Z = 21.39, p < .001.
For times treated in a psychiatric hospital over the past 6 months, there was significant variability around the intercept due to person, σ2 = 5.28, Z = 21.74, p < .001.
For days detained/incarcerated, there was significant variability around the intercept due to person, σ2 = 29.48, Z = 21.71, p < .001.
p ≤ .05. **p ≤ .01.
For the number of days using drugs over the past 6 months, there were no significant effects for condition, time by condition interaction, or the covariate age. There was a significant time and dose effect for drugs, indicating that a higher dose led to fewer days using drugs.
We also examined continuous abstinence from the baseline to the 24-month follow-up, with data from the Timeline Followback at each wave indicating whether the person had been abstinent. For alcohol use, there was a significant overall effect among conditions, χ2(2, N = 270) = 12.12, p < .01, with the OH condition achieving significantly higher continuous rates (66%) than the TC (40%), χ2(1, N = 180) = 11.79, p < .01, and the UA (49%) conditions, χ2(1, N = 180) = 5.01, p = .02. There were no significant differences for continuous drug abstinence rates, OH (47%), TC (44%), UA (42%); χ2(2, N = 270) = .36, p = .84.
Employment Outcomes
Table 2 also describes economic variables. For the number of paid days worked in the last 30 days, there were significant effects for condition, time, and time by condition interaction. The impact of time differed significantly between OH and UA, b = 1.16, t(937) = 1.16, p = .01, indicating that time has a greater positive impact for OH than UA. There was no significant difference in the impact of time for TC and UA, b = −0.02, t(937) = −0.43, p = .97. Based on the signs of the coefficients, one can infer that impact of time differed between TC and OH, with OH receiving a more positive impact of time. The covariate, age, on which groups differed, significantly affected earned money, with lower age related to better outcomes. In addition, there was a significant dose effect, indicating that higher dose led to more days worked.
For money received from employment over the past 30 days, the effect of condition was not significant, but the time, and the time by condition interaction effects were significant. The impact of time neither differed between OH and UA, b = 64.27, t(941) = −1.06, p = .07, nor between TC and UA, b = −37.21, t(941) = −1.04, p = .30; but based on the direction of the coefficients, one may infer that the impact of time differed significantly between OH and TC, with time having a greater positive impact for OH. The covariate age, on which groups differed, significantly affected earned money, with those younger earning more money. There was a significant dose effect, indicating more dose led to better outcomes.
Finally, for illegal income earned during the last 30 days, there were no significant effects for condition, time, time by condition interaction, age, or dose.
Other Outcomes
The final variables involving legal issues, incarcerations, and psychiatric hospitalizations are also presented in Tables 2 and 3. Regarding the legal ASI composite score over the last month, there was no significant condition, condition by time interaction, or dose effect. There were significant time and age effects, and the latter finding indicated that younger participants had less legal problems.
For times treated in a psychiatric hospital over the past 6 months, there was a significant time effect, but not a significant condition, time by condition interaction, age, or dose effect.
For days incarcerated, there was a significant time effect, but not a significant condition, condition by time interaction, age, or dose effect.
Economic Analysis
Lo Sasso and Jason (2012) collected data in 2010 using the DATCAP (French, 2003) on three OHs used in this study. Data were collected on the number of clients and their mean length of stay. As there are no professionally employed staff and OHs have no equipment generally, miscellaneous expenditures was the largest cost component (80%-90% of the total), and among the categories rent was the greatest expense. The sum of all of the expenditure categories was computed to arrive at the total annualized cost. The sum was divided by the average daily census to derive the average annual cost per client. Dividing this value by 52 produces the average weekly cost per client of OH. As all expenses were paid by residents, the net public payer (Lo Sasso & Jason, 2012) costs (where the opportunity and program costs such as rent are paid by the residents) are $0 for the OH condition (see Table 4). We thought that this public payer perspective was appropriate in tabulating costs as residents pay for their housing and food expenses rather than relying on local, state, or federal resources. However, economists often calculate costs using what is called a societal perspective. Using this approach, rent and other miscellaneous items for those in the OH condition are counted as costs, as this provides a perspective for analyzing all costs regardless of who has to pay them. Using this more conservative societal perspective, the costs for all program expenditures would be US$93 per week or a total of US$1,116 over the average of 3 months each OH resident resided in this setting.
Summary of Mean Per-Person Benefits and Costs.
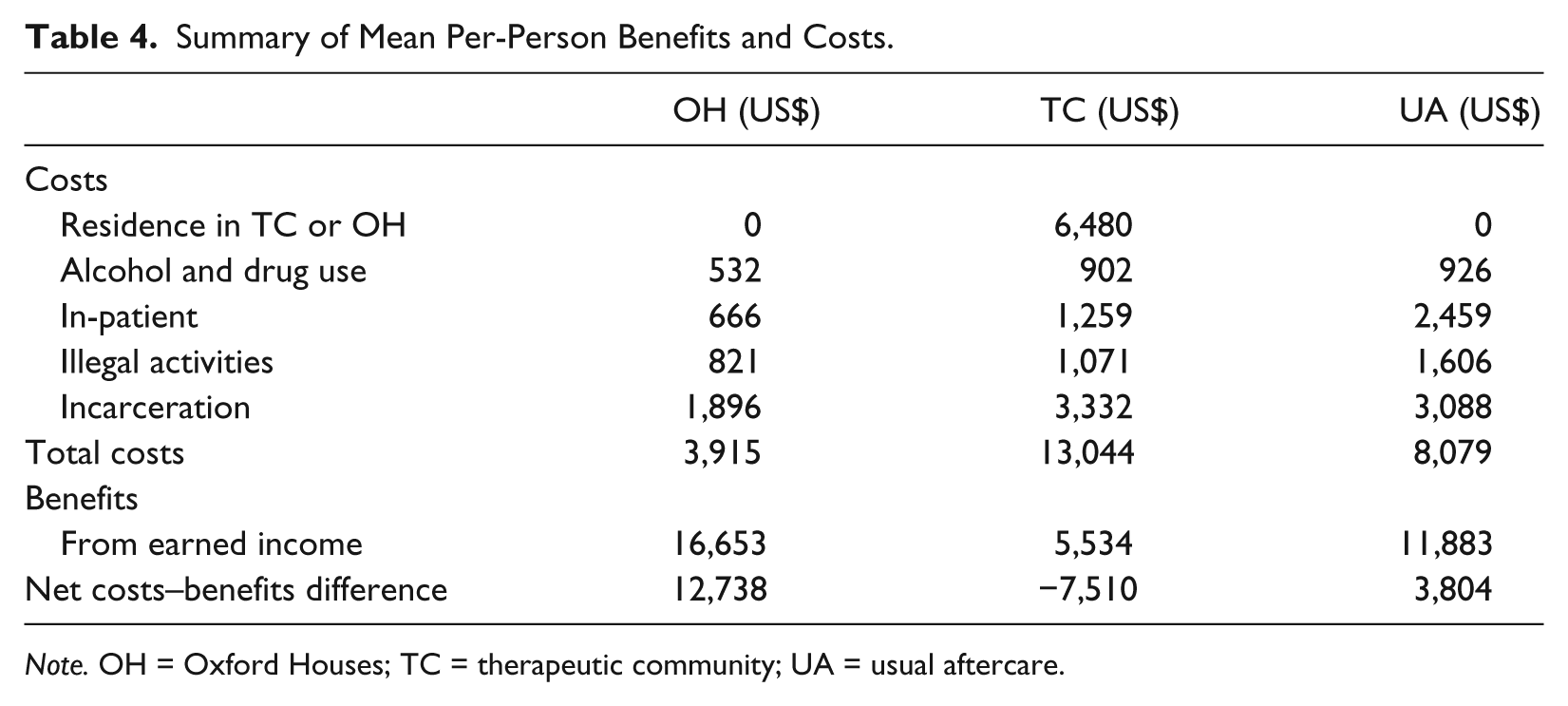
Note. OH = Oxford Houses; TC = therapeutic community; UA = usual aftercare.
As we only used one TC, we decided to use costs associated with a range of TCs. The average weekly cost per client reported for TCs was US$554 in 1994 dollars. To compare this value with the range of estimates calculated in the OH surveys, they must be converted to 2010 dollars. To do this, we determined how much general prices have risen between 1994 and 2010 using the consumer price index (see www.bls.gov/cpi). As the consumer price index increased 46.2% from 1994 to 2010, scaling the TC cost estimate up to 2010 dollars yielded an estimate of US$810 for the average weekly cost per client. As the average TC person was in treatment for 8 weeks, the costs per person in the TC condition were US$6,480.
Other costs include reported drug and alcohol use. To impute values of monthly alcohol and drug expenditures among users in our sample, we borrowed average monthly expenditures from Sindelar et al.’s (2004) data on the Philadelphia Target Cities project. Sindelar et al. found average monthly alcohol expenditures of US$21.36 and average monthly drug expenditures of US$112.07. The 6-month expenditure was estimated to be US$185.74 [(US$21.36/0.69) × 6] per alcohol user and US$738.92 (US$112.07/0.91) per drug user. For the alcohol outcome, the 43 OH alcohol users (individuals who used during one of the 6-month waves) cost US$7,987; the 103 TC users cost US$19,131; and the 85 UA users cost US$15,788. For drug outcome, the 54 OH drug users cost US$39,901; the 84 TC drug users cost US$62,069; and the 91 UA drug users cost US$67,242. Total alcohol and drug cost per person for the OH condition was US$532 (US$47,888 divided by 90 participants); for the TC condition, the average cost was US$902 (US$81,200/90); and for the UA condition, the average cost was US$926 (US$83,030/90). We did not count baseline data in these economic analyses, as this is a time period before the intervention began.
Other costs included income from illegal activities, which was summed over the 2-year period. It amounted to US$817 for the OH (the sum of income over the last month for Waves 2, 3, and 4 = US$136.83 × 6 months), US$1,071 (US$178.44 × 6) for the TC, and US$1,606 for the UA (US$267.67 × 6).
The cost of incarceration for individuals was estimated to be US$23,384 per year based on the average cost to treat recovering abusers in Illinois jails (LoSasso et al., 2012), or US$64.07 per day. From Waves 2 to 5, the OH, TC, and UA conditions self-reported having spent an average of 2.6, 6.0, and 4.7 days incarcerated, respectively, within 30-day periods. Extrapolating for the 6 months, we would expect that there would be 15.6, 36, and 28.2 incarcerated for the entire period for the OH, TC, and UA conditions. In addition, at Wave 5, we were not able to interview 7 OHs, 8 TCs, and 10 UAs who were incarcerated, so we conservatively estimated that these OH members had an average incarceration of 14 days [(7 incarcerated × 180 days)/90 participants], 16 days for TCs, and 20 days for UAs. Adding the two sums, we derive an average of 29.6 days incarcerated for the OHs (15.6 + 14), 52.0 days for the TCs (36 + 16), and 48.2 days for the UAs (28.2 + 20). Therefore, the average cost per person in the OH condition was US$1,896 (29.6 days × US$64.07 per day), US$3,332 for the TC condition, and US$3,088 for the UA condition.
Each respondent reported whether they had any inpatient treatment for psychiatric problems. We used the average total cost of treatment in Illinois for each program. For inpatient treatments, we used the average daily medical expense for an inpatient stay in Illinois community hospitals, US$1,799 (Fiscal Year 2008). The 33.3 people in the OH condition who indicated being hospitalized for any wave are estimated to have cost US$59,907 or US$666 per person (US$59,907/90 participants); the 63 TC participants cost US$113,337 or US$1,259 per person; and the 123 UA participants cost US$221,277 or US$2,459 per person.
Benefits included earnings from work were self-reported by enrollees. The monthly earnings in Table 4 were multiplied by 6 to provide estimates over the 6 months (not counting Wave 1 as it was prior to the start of the study). Over the 2-year study, those in the OH condition earned US$16,653; those in the TC earned US$5,534; and those in the UA earned US$11,883.
Subtracting the benefits above from the costs indicated that the net benefits per person for the OH, TC, and UA conditions were US$12,738, −US$7,510, and US$3,804, respectively (where the opportunity and program costs such as rent are paid by the residents). Using a societal perspective (where rent and other miscellaneous items were counted as a cost), the OH costs would be US$93 per week or US$1,116 over the average of 3 months for each OH resident, so the net benefits of the OH would be reduced to US$11,622.
Discussion
A major finding in this study was that dose appears to be critical for positive substance use and income outcome variables, although not for legal issues, incarcerations, and psychiatric hospitalizations. We did not find support for our main hypothesis, which was that TCs would be more effective in creating a stable abstinence support system and helping residents find and maintain abstinence and employment as well as reduce recidivism compared with OHs or UA. Although days using alcohol and days using drugs were not significant for the three conditions over the different waves, those in the OH condition achieved significantly higher continuous sobriety rates. For money received from employment and number of paid days worked, those in the OH condition did better than those in TC. No significant differences were found for illegal income obtained. We also found that costs were lower and benefits in terms of earned income were higher for the OH condition. These findings suggest that the OH condition had the best cost–benefit outcomes.
Our study found that higher doses of OH and TC treatment led to better outcomes on substance use and employment variables. These findings are consistent with studies that have found that recovery most likely occurs when one has social support networks that support substance abstinence (Beattie & Longabaugh, 1997; Longabaugh, Wirtz, Beattie, Noel, & Stout, 1995; Zywiak, Longabaugh, & Wirtz, 2002). These types of “safe” social environments could contribute to ongoing abstinence in many ways (e.g., by reducing opportunities to use). This is of particular importance as the medical costs associated with drug and alcohol addictions are exorbitant, totaling approximately US$428 billion annually (National Drug Intelligence Center, 2011). Research suggests that individuals who participate in aftercare services sustain abstinence for a longer period of time (Laudet, Becker, & White, 2009; Sannibale et al., 2003). In fact, one study found that each additional month spent in aftercare led to a 20% increase in the odds of maintained abstinence from substance use (Schaefer, Cronkite, & Hu, 2011). In a previous study, Jason, Olson, et al. (2007) found that individuals who stayed at least 6 months in an OH had lower relapse rates and significantly better indicators of personal change such as employment, abstinence self-efficacy, and proportion of abstinent others in the personal “significant persons” network, compared with those staying less than 6 months (Jason, Olson, et al., 2007). DiClemente, Fairhurst, and Piotrowski (1995) also found that efficacy expectations stabilize after 6 months of abstinence. If longer stays in both types of programs lead to better outcomes, then a critical issue involves how to keep individuals committed to such settings for long-enough periods of time.
It is important to note that only 50% of those assigned to the OH condition maintained residency for 3 months or greater. Resident stays in OHs were appreciably shorter than national averages in these types of recovery homes, which tend to be about 6 months (Jason et al., 2006). The reason for these shorter stays was probably due to the fact that the current study occurred during a recession, and it was even more difficult for individuals with a criminal history to find employment during this period of time. If these individuals were not able to find employment, then it was more difficult for them to pay their weekly rent and stay in the OHs. The same difficult financial situations also occurred for the other two conditions during this 2-year study. In a sense, with significant reductions in employment during the worst recession since the depression of the 1930s, our outcomes are probably at the lower limit of what might be expected. An additional factor limiting the effectiveness of the OHs was that many of the houses were relatively newly opened and within Chicago, and these houses provided residents both limited economic opportunities as well as houses that were less stable than those with a longer history of existence. In fact, over the course of the study, many of the OHs in Chicago had to close due to these economic difficulties.
Because ex-offenders with substance abuse problems are more likely to be unemployed (Needels, 1996; “Treatment Improvement Protocol 38,” 2000), they miss the benefits of employment which provides a source of income, requires managing the use of time, and improves self-esteem. Given these types of benefits of employment for ex-offenders, an important finding in our study was the significant time by condition interaction effects for earned income and days worked, suggesting that the OH condition had better outcomes on these variables than the TC condition. OHs provide abstinent support networks, but without professional staff involvement, and perhaps better outcomes occurred with the OHs because self-help-based approaches might be more effective in influencing residents to find employment as that is a requirement for remaining within the OHs. The better OH employment outcomes might also have been due to OHs providing support for employment in less-structured ways than TCs (i.e., peers might have encouraged residents to find work and provide job leads).
Regarding the cost–benefit analyses, our hypothesis that the OH condition would have the best ratio was confirmed. It was surprising to see that the TC had a worse ratio than the UA condition. Much of this difference was due to the expense of being in a staffed setting and less earned income. Settings such as TCs and halfway houses represent important recovery resources for those who need structured environments, so we would not conclude by this one study that TCs are not of importance to the health care system. It is still unclear why those in the TCs had lower earned income over time, and it is at least possible that the recession that all participants were exposed to had more negative consequences for those exiting a staffed TC, but of course, more research is needed to better understand this unexpected finding.
There were a number of limitations of this study, which go beyond the dire economic circumstances involving a difficult job market that affected our participants. Certainly, the length of stay in treatment settings was below initial expectations, so the results might be limited by the economic conditions that were present during our study. In addition, our investigation only followed up individuals for 2 years, and clearly it would be beneficial to continue monitoring this cohort for longer periods of time. Also, our reported cost–benefit analysis only involved a limited number of variables. Finally, we recruited individuals who had been released up to 24 months from prison, and future studies might focus on individuals who are more recently released from prison.
Future research needs to be directed to the OH, TC, and UA social ecology itself, which might be the active ingredient in a successful residence experience for the recovering person with a substance use disorder. How do new residents fit into this ecology—or fail to? What do they need to take away from it to put their lives back together? Are there more systematic ways prospective residents could prepare for a successful stay? How do residents’ relationships within the OH and TC, as well as within their own (non-house) personal networks, interact to fulfill recovery requirements? The answers to such questions would help us understand the way OH and TC cultures develop, are maintained, and are extended to new residents, and how this process interacts with residents’ attempts to refashion their personal networks to support their recoveries.
In conclusion, OHs comprise a large network that provides inexpensive housing and support for abstinence. They represent alternative housing environments and are of particular importance, given the cost to house a prison inmate (California Legislative Analyst Office, 2012) or costs of temporary shelter (HUD, 2006). The present study compared associated economic costs and benefits of staffed TC versus these OH community-based housing, and findings suggest that OH recovery homes were more successful in providing help for those needing treatment aftercare, but much work remains to determine the process by which clients are helped with these types of aftercare settings.
Footnotes
Acknowledgements
We appreciate the support of Paul Molloy and Leon Venable from the Oxford House organization. We also thank David Mueller and Ray Legler for their logistic help, as well as Steven Miller for his statistical consultation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors appreciate the financial support from the National Institute on Drug Abuse (Grants DA13231 and DA19935).