
Abstract
Low-income adults with substance use disorders (SUDs) have a high prevalence of tobacco use and often limited access to tobacco cessation treatment. This study examines the relationship between low-income SUD patient census (i.e., percentage of patients whose treatment costs are covered by Medicaid and Federal block grants) and SUD programs’ availability of three evidence-based tobacco cessation services (TCS): behavioral treatments, system-level support, and pharmacotherapy. Data were collected from a random sample of 1,006 program administrators in 2010. Mixed-effects models results show that the percentage of low-income patients is significantly positively associated with the availability of behavioral treatments and system-level support but not pharmacotherapy. Thus, low-income patients may have similar access to tobacco cessation pharmacotherapy but greater access to behavioral treatments and system-level support. However, the availability of TCS is not widespread overall, which may hamper access to extensive services to address low-income SUD patients’ high smoking rates.
Introduction
The pervasiveness of smoking among U.S. adults has decreased by more than 50% over the past five decades. In 1965, 42.4% of adults smoked compared with 19% in 2011 (American Lung Association, 2011; Centers for Disease Control and Prevention [CDC], 2012; Moreno & Houston, 2012). Despite these significant reductions, the prevalence of smoking remains high among certain subpopulations. Among individuals seeking treatment for substance use disorders (SUDs) the smoking rate is between 65% and 87% (Fiore et al., 2008; Guydish et al., 2011), among low-income adults receiving Medicaid benefits it is 36% (American Legacy, 2010), and among those who are uninsured it is 33% (American Legacy, 2010).
Unfortunately, adults suffering from SUDs not only have a higher prevalence of tobacco use than adults in the general population but they also often have low incomes and limited access to tobacco cessation treatment (American Legacy, 2010). As a result, they are at a greater risk of negative but preventable health-related outcomes than other populations. The current study examines the relationship between low-income SUD patient census and SUD treatment programs’ availability of tobacco cessation services (TCS) that are recommended by the Public Health Service (PHS; Fiore et al., 2008) to gain a better understanding of the factors that support access to TCS.
Evidence-Based TCS
The clinical practice guidelines on TC published by the PHS encourage clinicians and other professionals to adopt and implement a variety of evidence-based treatments (EBTs), including behavioral treatments, system-level support, and pharmacotherapy (Fiore et al., 2008). Behavioral treatments generally include using the 5 As (ask about tobacco use, advise to quit, assess willingness to quit, assist in quitting, and arrange for follow-up care), increasing patients’ problem solving skills, offering counseling services, and providing ongoing TC support and encouragement (Fiore et al., 2008; Kalman, Morissette, & George, 2005; Richter & Arnsten, 2006). System-level support includes treatment programs providing counselor training on TC, counselor resources for TC, and clinical supervision on TC (Fiore et al., 2008). Furthermore, the U.S. Food and Drug Administration (FDA) approved seven first-line pharmacotherapies including five nicotine replacement therapies (nicotine gum, inhaler, lozenge, nasal spray, patch), bupropion, and varenicline. Second-line TC therapies include clonidine and nortriptyline that have proven efficacy but are not approved by the FDA as TC aids (Fiore et al., 2008). Because patients’ needs vary and there is no one best TC treatment service, patients should be offered as many services as possible (Fiore et al., 2008).
Demand for TCS Among Low-Income SUD Patients
Tobacco use among low-income adults continues to be higher than among other adults (CDC, 2012; Moreno & Houston, 2012) and is likely to increase over time (Franks et al., 2010; Moreno & Houston, 2012). Research finds that lower compared with higher socioeconomic status (SES) is related to greater TC obstacles including psychological and behavioral (Yong et al., 2013), less intent to quit tobacco use, and less abstinence from tobacco at both 1 and 6 months follow-up (Reid et al., 2010). Concurrently, low-income individuals have less access to health care in general, and TCS in particular (American Legacy, 2010). This puts them at increased risk of well-known tobacco-related diseases (U.S. Department of Health and Human Services [USDHHS], 2004).
Considering the high smoking rates among low-income adults and the fact that individuals with SUDs start smoking earlier than the general population, are more likely to be heavy smokers, and often have more difficulty quitting (Breslau, Peterson, Schultz, Andreski, & Chilcoat, 1996; Hayford et al., 1999; Hays et al., 1999; Novy, Hughes, & Callas, 2001), providing TCS to low-income patients in SUD treatment should be a public health priority. SUD treatment is a context where TC EBTs might also have the best chance of reaching low-income smokers considering that between 44% and 80% of patients overall express an interest in quitting their tobacco use when seeking SUD treatment (Clarke, Stein, McGarry, & Gogineni, 2001; Richter, Gibson, Ahluwalia, & Schmelzle, 2001; Rohsendow et al., 2003).
Importantly, clinical trials have shown no undesirable effects on treatment outcomes when TC treatment is integrated into SUD treatment (Cooney, Litt, Cooney, Steinberg, & Oncken, 2007; Grant et al., 2007; M. S. Reid et al., 2008). In fact, TC treatment is positively associated with greater abstinence from alcohol and other drugs, decreased risk of alcohol and drug relapse, and decreased alcohol consumption (Baca & Yahne, 2009; Barrett, Tichauer, Leyton, & Pihl, 2006; Prochaska, Delucchi, & Hall, 2004; Satre, Kohn, & Weisner, 2007; Weinberger & Sofuoglu, 2009). However, TCS are not extensively adopted in treatment programs (Eby & Laschober, 2013; Friedmann, Jian, & Richter, 2008; Guydish et al., 2012; Knudsen & Studts, 2010; Knudsen, Studts, & Studts, 2012; Rothrauff & Eby, 2010), which may hamper access to EBTs among low-income smokers.
Current Study
The purpose of the present study is to examine the relationship between low-income SUD patient census (i.e., percentage of patients whose SUD treatment costs are covered by Medicaid and Federal block grants) and SUD treatment programs’ availability of three recommended evidence-based TCS. Specifically, the following three research questions are addressed:
This study adds to the SUD literature in two main ways: First, not enough is known about the quality of TC programs that are offered alongside SUD treatment and the extent to which evidence-based TCS are made available in SUD treatment programs. Thus, we examine the availability of a wide range of recommended TCS (behavioral treatments, system-level support, and pharmacotherapy) in a random sample of SUD treatment programs located across the United States. Second, research is greatly lacking on low-income patients’ access to TCS in SUD treatment programs. Yet, by understanding the availability of TCS for low-income patients, recommendations can be made about how to better reach low-income smokers, intervene on their smoking behavior, and how to make services more accessible.
Method
Study Design and Sample
The Managing Effective Relationships in Treatment Services (MERITS III)project provided data for this study. MERITS III is a National Institute on Drug Abuse (NIDA) funded longitudinal project that started in 2010 and is carried out by researchers affiliated with the University of Georgia. The purpose of MERITS III is to assess the impact that treatment program processes and management practices have on the adoption, implementation, and sustainability of TCS in a random sample of SUD treatment programs in the United States. All procedures were approved by the University of Georgia Institutional Review Board. A detailed description of the study design and sample has been published previously (Muilenburg, Laschober, & Eby, 2014a, 2014b).
Briefly, the sampling frame for MERITS III was based on 11,153 treatment programs that were included in the Substance Abuse and Mental Health Services Administration (SAMHSA) 2010 National Directory of Federal, State, local government, and private facilities that offer substance abuse treatment services. To screen for eligibility, programs were assigned a random number and research assistants called programs starting at the lowest number. Treatment programs had to provide SUD counseling services in a community setting to qualify for participation. Programs that offered only methadone maintenance, Veterans administration programs, driving-under-the-influence (DUI) educational programs, or those listed as Halfway Houses and only offered detoxification were ineligible. In-depth structured phone interviews were conducted with program administrators. Once the target sample size was reached, the screening, qualifying, and interviewing process stopped. A total of 1,599 programs were eligible for participation of which 1,006 program administrators completed a survey (62.91% basic response rate).
Measures
TCS
The availability of the three TCS was examined regarding behavioral treatments, system-level support, and pharmacotherapy (Fiore et al., 2008). Response options for each service were 0 = no and 1 = yes. Each TCS index was created by summing the number of yes responses to the respective questions. First, program administrators noted which of the 11 behavioral treatments for TC are available at their treatment program (Fiore et al., 2008). Example items include the use of the 5 As (ask about tobacco use, advise to quit, assess willingness to quit, assist in quitting, and arrange for follow-up care), provision of self-help materials, and availability of individual counseling that focuses on social support. Second, program administrators specified which of the nine items measuring system-level support for TC characterize their treatment program (Fiore et al., 2008). Example items are whether their treatment program provides counselor training on TC treatments, counselor resources for TC treatments, and clinical supervision on TC treatments. Third, program administrators indicated which of the nine TC pharmacotherapies (nicotine patch, nicotine gum, nicotine lozenge, nicotine nasal spray, nicotine inhaler, bupropion, varenicline, clonidine, nortriptyline) are available in their treatment program (Fiore et al., 2008).
Low-income patients
Low-income patient census was measured with two items. Program administrators indicated the percentage of patients whose treatment costs are covered by (a) Medicaid and (b) Federal block grants. Medicaid is a free or low-cost health insurance provided to low-income people (SAMHSA, 2012). Federal block grants are awarded to States for the prevention and treatment of behavioral health issues and made available to SUD treatment programs to provide services to patients who lack private insurance, Medicaid, or Medicare coverage (SAMHSA, 2012). Response options ranged from 0% to 100%. The measure was created by calculating the mean of the two items.
Control variables
The percentage of SUD patients who smoke seeking treatment in the program and an organization’s hospital affiliation were used as control variables. Previous research has shown a positive association between the availability of TCS and the percentage of patients who smoke (e.g., Friedmann et al., 2008) and hospital affiliation (e.g., Friedmann et al., 2008; Knudsen, Studts, Boyd, & Roman, 2010). The percentage of patients who smoked ranged from 0% to 100%. An organization’s hospital affiliation was recorded as 0 = no and 1 = yes.
Data Analytic Plan
All analyses were conducted using SAS 9.3. Descriptive statistics were used to provide background information on program administrators (see Table 1) and assess the extent of TCS availability (see Table 2). Correlation analyses were run to examine the correlations among all study variables (see Table 2). Prior to answering the research questions, we first examined whether the nested structure of the data (i.e., treatment programs are nested within states) needed to be statistically taken into consideration. This is important because states tend to differ in their Medicaid coverage of TCS (Kaiser Family Foundation, 2011). An examination of the intraclass correlation coefficients (ICCs) showed that 9% of the variance of behavioral treatments availability, 11% of the variance of system-level support availability, 6% of the variance of pharmacotherapy availability, was explained by within state nesting. The generally accepted rule is that ICCs around 10% indicate the need to account for the nested structure of the data (Kreft & de Leeuw, 1998).
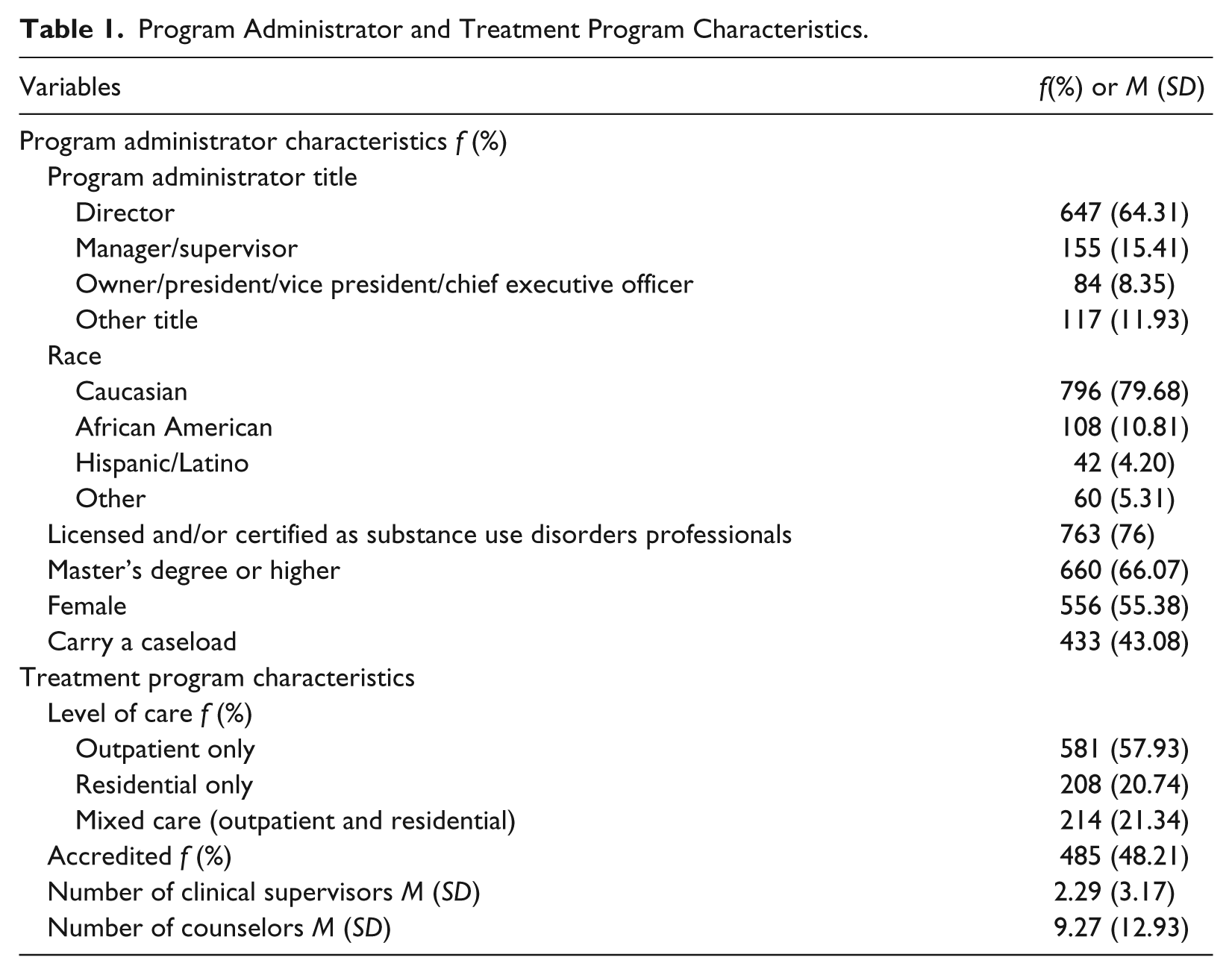
Program Administrator and Treatment Program Characteristics.
Descriptive Statistics of and Correlations Among All Study Variables.
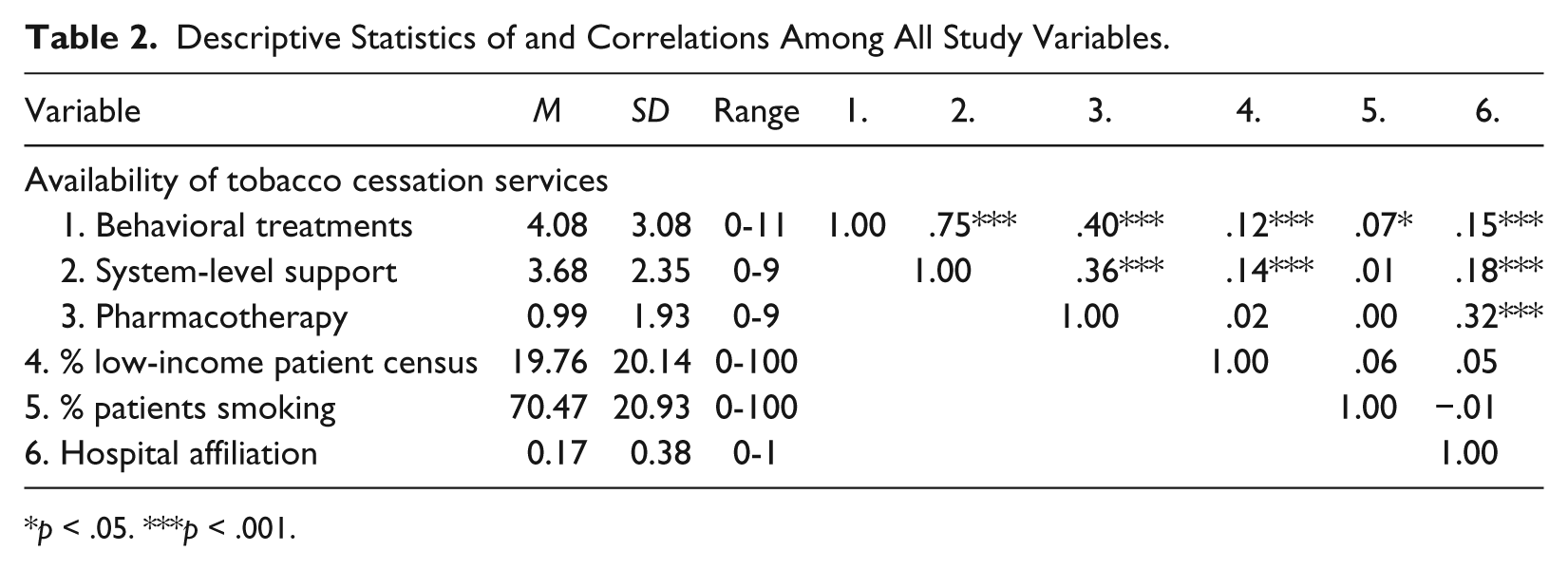
p < .05. ***p < .001.
Thus, the first research question (What is the relationship between low-income SUD patient census and the availability of TC behavioral treatments?) and second research question (What is the relationship between low-income SUD patient census and the availability of TC system-level support?) were answered using mixed-effects models rather than ordinary least squares (OLS) regression models that do not account for the nesting of the data to avoid misleading inferences (see Table 3). For the third research question (What is the relationship between low-income SUD patient census and the availability of TC pharmacotherapy?), we ran the analyses with both an OLS and a mixed-effects model given that the ICC was 6% for TC pharmacotherapy, which is below the 10% threshold. The statistical significance of the results was unchanged so we decided to also use a mixed-effects model for nested data similar to the other two research questions (see Table 3). Specifically, for all three research questions, the model-based analysis using PROC MIXED for continuous, correlated data and the “identity” link function were used (see Ying & Liu, 2006, for more detailed information). The random statement included the intercept and the “state” variable. These are standard selections with continuous dependent variables and nested data.
Mixed-Effects Models Results: Relationship Between Percentage of Low-Income Patients and Availability of TC Services.
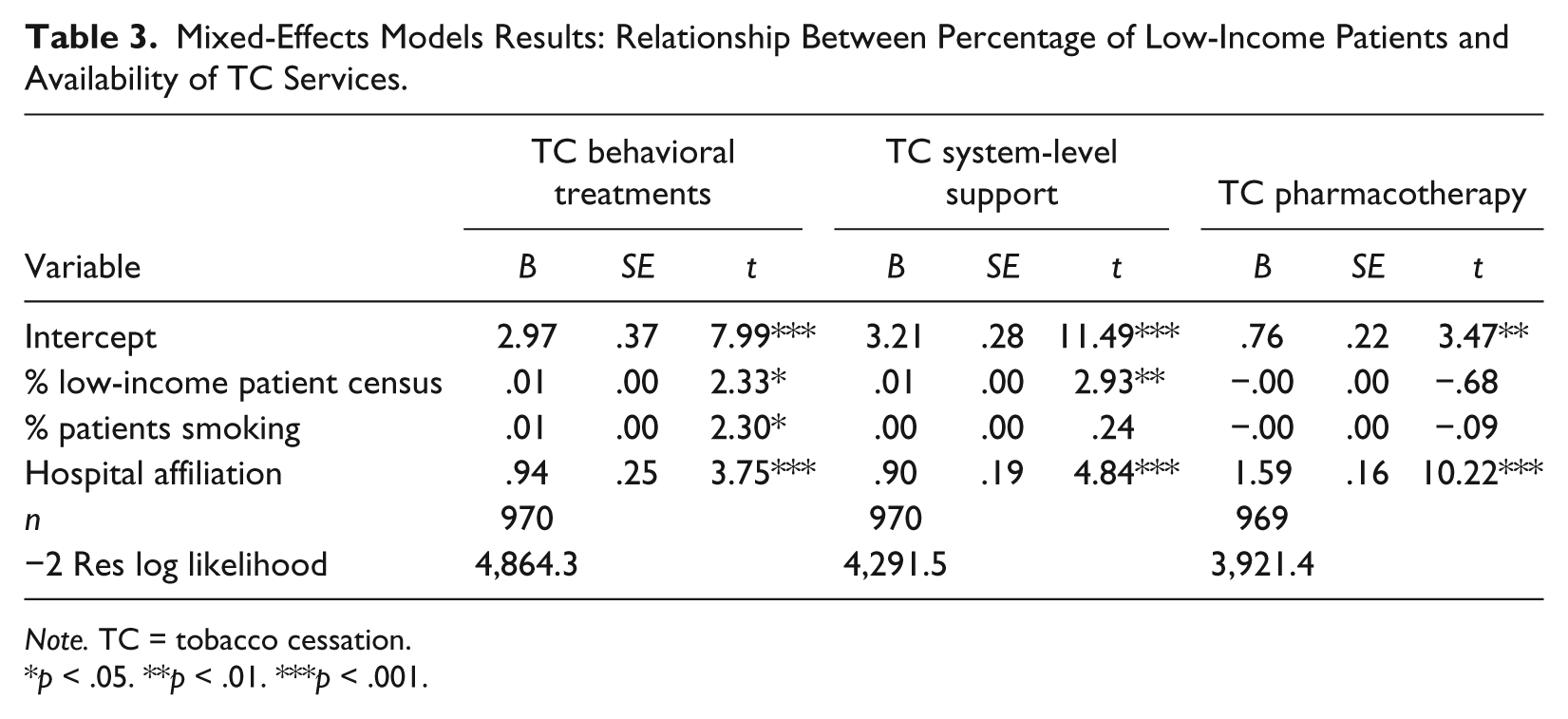
Note. TC = tobacco cessation.
p < .05. **p < .01. ***p < .001.
Results
Sample Description
As shown in Table 1, program administrators held diverse job titles including director (64.31%), manager/supervisor (15.41%), and owner/president/vice president/chief executive officer (8.35%). The majority of administrators were Caucasian (79.68%), licensed and/or certified as SUD professionals (76%), held at least a master’s degree (66.07%), and were women (55.38%). Almost half of them carried a caseload (43.08%). According to program administrators, the majority of treatment programs offered outpatient-only treatment (57.93%), followed by residential-only treatment (20.74%), and a mixture of both outpatient and residential treatment (21.34%). Almost half of the programs were accredited (48.21%). Programs employed a mean of 2.29 (SD = 3.17) clinical supervisors and 9.27 (SD = 12.93) counselors.
Descriptive Statistics and Correlations Among All Study Variables
According to program administrator reports and as shown in Table 2, treatment programs reported an average of four TC behavioral treatments (range = 0-11), four TC system-level support (range = 0-9), and one TC pharmacotherapy (range = 0-9). Treatment programs reported that 19.76% of their patients were low-income and an average of 70.47% patients smoked. Approximately 17% of treatment programs were affiliated with a hospital or medical facility. Also displayed in Table 1 are the relationships among all study variables, which did not indicate multicollinearity concerns.
Relationship Between Low-Income Patient Census and TCS Availability
Table 3 shows that the percentage of low-income patient census was significantly positively associated with the availability of TC behavioral treatments (B = .01) and the availability of TC system-level support (B = .01). In contrast, there was no significant relationship between the percentage of low-income patients and the availability of TC pharmacotherapy. Regarding the control variables, the percentage of patients who smoke was significantly positively related with the availability of TC behavioral treatments (B = .01), and hospital affiliation was significantly positively associated with the availability of all three TCS (B = .94 for behavioral treatments, B = .90 for system-level support, B = 1.59 for pharmacotherapy). No other significant relationships were found.
Discussion
Findings from our study show that SUD treatment programs with a greater low-income patient census offer more TC behavioral treatments and more TC system-level support, but not more TC pharmacotherapy. These are important findings considering that low-income Medicaid enrollees are more likely to smoke than other adults (American Lung Association, 2011), and low-income adults tend to have less access to TC treatment in general (American Legacy, 2010). SUD programs with a higher census of low-income patients may integrate behavioral treatments and system-level support more into usual care due to greater need for assistance. For example, low-income smokers may need more individual and group counseling as well as more counseling sessions to help them quit smoking. They may also require more intense training in problem solving skills pertaining to their TC attempts as well as greater TC support and encouragement. Low-income patients also tend to have greater need for diverse services such as help with employment, housing, nutrition, and health care (e.g., Adler & Newman, 2002). In contrast, TC pharmacotherapy may not require as much integration with existing treatment protocols, resulting in no differences on this TC service.
However, it is important to bear in mind that the availability of the three TCS is not widespread overall. These findings are similar to previous research on the adoption of diverse TCS in SUD treatment programs (e.g., de Tormes Eby & Laschober, 2013; Friedmann et al., 2008; Guydish et al., 2012; Knudsen & Studts, 2010; Knudsen et al., 2012; Rothrauff & Eby, 2010). Thus, although low-income patients may not be at a particular disadvantage in terms of access to TCS in general compared with other patients, they may not have extensive access to the full range of EBTs to aid their TC attempts. The lack of TCS availability is a major public health concern considering the greater prevalence of smoking among low-income patients (CDC, 2012; Moreno & Houston, 2012) and the demand for TCS in SUD treatment programs (Richter et al., 2001; Rohsendow et al., 2003).
Implications for Policy, Research, and Practice
With the establishment of the Affordable Care Act (ACA), Medicaid benefits now include mandatory coverage for TC programs, including TC pharmacotherapies in 2014 (American Lung Association, 2012). Moreover, those who are uninsured will be eligible for TC benefits through the State Health Insurance Exchange (American Lung Association, 2012). This may increase the opportunity for SUD clinicians and other health care providers to implement or enhance TC programs for patients during SUD treatment. When these policies go into effect, this may increase access to care for those who are most in need of TCS.
Future research should investigate why disparities exist for low-income patients if this population may in some cases have greater accessibility to certain TCS. Yet, challenges continue to exist for low-income patients in all three prevention layers: primary, secondary, and tertiary. Implementation of primary prevention programs, screenings, and treatment for tobacco-related illnesses are a challenge for mental health care professionals. These challenges are further complicated by the traditional health care issues that impact low-income individuals such as generally less access to TCS (American Legacy, 2010). Moreover, when EBTs are available, this population is less likely to use them and is less likely to quit smoking (Virdrine, Reitzel, & Wetter, 2009).
Low-income smokers are also less likely to live and work in smoke-free environments, in both public and private areas. For instance, lower socioeconomic home environments are more likely to have current smokers and fewer smoking bans in the household (Muilenburg et al., 2009; Zhang, Martinez-Donate, Kuo, Jones, & Palmersheim, 2012). There is also increased smoking and less likelihood of TC in community and public environments that are considered lower income areas (Cohen, Sonderman, Mumma, Signorello, & Blot, 2011; Turrell, Hewitt, & Miller, 2012). In addition to environmental and social exposure to tobacco, there is also greater access to tobacco products in these low-income areas (Loomis, Kim, Goetz, & Juster, 2013). Overall, there is a lack of primary prevention efforts that reach lower income individuals and an overall need to have culturally and socially relevant primary prevention programs for TC (Unger, Sun, & Johnson, 2007).
Limitations and Conclusions
Several limitations warrant mention. First, we used the percentage of patients whose treatment is paid by Medicaid and Federal Block grants as a proxy for low-income status. Although SAMHSA (2007, 2014) reports indicate a similar percentage (13% of admissions in 2005 were expected to be paid primarily by Medicaid and Medicaid was the most frequently reported insurance by adults at admission at 21.3% in 2011), the relationship between low-income patients and availability of TCS may be different when low-income status is calculated through other means (e.g., patients’ self-reported income, W2s, unemployment benefits). This should be examined in future studies. Second, findings are based on SUD program administrator reports and may not reflect clinicians’ experiences regarding the availability of TCS. This represents an avenue for future research and may provide a unique perspective regarding the actual use of TCS with low-income patients. Third, although our findings are based on a nationally random sample, they are limited to community-based SUD treatment programs and may not generalize to programs with similar low-income patient census. Studies are needed that focus on military-based programs, prison-based programs, DUI educational programs, and Veteran’s Health Administration programs to gain a better understanding of the availability of TCS for low-income patients being served in these settings.
Even with these limitations, this study provides a better understanding of TCS availability for low-income patients in SUD treatment programs. Our findings suggest that low-income patients seeking treatment for SUDs have equal access to TC pharmacotherapy and more access to behavioral treatments and system-level support for TC than other patients. However, availability of TCS is generally not extensive, which warrants further investigation into whether low-income patients are receiving optimal TCS in SUD treatment to address their high smoking rates.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not represent the official views of the National Institute on Drug Abuse (NIDA) or the National Institutes of Health (NIH).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Award Number R01 DA028188 from the National Institute on Drug Abuse (NIDA) awarded to Jessica L. Muilenburg and Lillian T. Eby (multiple principal investigators).