
Abstract
Disruptions in opioid treatment programs (OTPs) are common after major disasters. Highly regulated OTPs confront challenges when responding to extended closures following disaster. Following Hurricane Sandy in 2012, an OTP located at the Manhattan Veteran Affairs Medical Center (VAMC) closed for 5 months. Semistructured interviews were conducted with clinicians and administrators who participated in the evacuation of the Manhattan VAMC, including the co-located OTP program. The Manhattan OTP preemptively dispensed emergency take-home methadone doses. Following closure, emergency guest-dosing arrangements were made for approximately 100 Veterans with Veterans Affairs (VA) and non-VA OTPs throughout New York City. Fortuitously, a retired VA OTP at another facility was reopened and accredited expeditiously. OTPs must improve contingencies for emergency response. However, disruptions in methadone delivery and threats to patient safety are likely to continue until agencies with oversight authority of OTPs describe specifications for emergency alternate care sites during long-term disaster recovery.
Keywords
Introduction
For decades, methadone maintenance treatment has been used for the treatment of opioid use disorder. Layers of federal, state, and local laws and regulations are in place to assure the safe delivery of care and to prevent diversion and misuse of this controlled substance (Rettig & Yarmolinsky, 1995). Federal regulations (CFR §8.11) and responsibility for their enforcement span multiple agencies. Within the U.S. Department of Health and Human Services, the Substance Abuse and Mental Health Services Administration (SAMHSA) oversees certification requirements and accreditation standards for opioid treatment programs (OTPs) (42 CFR §8.12), while the Food and Drug Administration (FDA) assures the safety of methadone for purposes of opioid maintenance treatment. The movement of methadone as a controlled substance is policed by the Drug Enforcement Administration (DEA), an agency of the U.S. Department of Justice. The DEA is also responsible for granting special permission to qualified physicians to dispense methadone in a certified OTP. In addition, State Opioid Treatment Authorities (SOTA) and local government entities at the county and municipal levels govern zoning, licensing, and day-to-day issues regarding methadone delivery from accredited OTP programs.
Following a major disaster that lasts a prolonged period, the layers of regulations designed to ensure the safe delivery of methadone also make it difficult to maintain continuity of care (Bloodworth, Kevorkian, Rumbaut, & Chiou-Tan, 2007; Elliott, Benoit, Matusow, & Rosenblum, 2017; Frank, Dewart, Schmeidler, & Demirjian, 2006; “Hurricane Sandy and Daily,” 2012; Matusow, Benoit, Elliott, Dunlap, & Rosenblum, 2018; Maxwell, Pullum, & Tannert, 2005; McClure, Mendoza, Duncan, Rotrosen, & Hansen, 2014; Rutkow, Vernick, Mojtabai, Rodman, & Kaufmann, 2012). Disasters can happen with little or no notice, last longer than several days, and disrupt communications systems and coordination of care. At stake is unintended withdrawal for methadone patients, which can begin within hours of the first missed dose (Bloodworth et al., 2007; Carlisle Maxwell, Podus, & Walsh, 2009; Matusow et al., 2017). The symptoms of withdrawal are profound (Gossop & Strang, 1991; Mattick & Hall, 1996; Sigmon, 2014) and can lead to relapse (Bart, 2012; Center for Substance Abuse Treatment, 2005; Saxon, Hser, Woody, & Ling, 2013; Volkow & McLellan, 2016). Moreover, abstinence from methadone can lead to relapse and overdose, which is often fatal (Diaper, Law, & Melichar, 2013; Schuckit, 2016; Sordo et al., 2017; Volkow & McLellan, 2016).
There is evidence to support both an increase in deaths from opioid overdose and a growing number of Americans affected by opioid dependence (Jones, Campopiano, Baldwin, & McCance-Katz, 2015; Madras, 2017; Rudd, Seth, David, & Scholl, 2016). In parallel, there is proof that the treatment system is already functioning at capacity (Jones et al., 2015). When disasters destroy the infrastructure needed to comply with strict OTP requirements, this already fragile system is very likely to collapse. This presents a crisis within a crisis.
September 11, 2011, was one of the first no-notice disasters to shed light on the consequences of disruptions in methadone dispensing. Many methadone patients were scattered throughout the city when the attacks occurred (Frank et al., 2006). Communication disruptions made it difficult to provide dose verification to guest programs (Frank et al., 2006; McArthur, Demirjian, Harmon, Hayashi, & Fogash, 2005). Consequently, some patients resorted to illicit drug use when they could not tolerate withdrawal symptoms (Frank et al., 2006; Weiss et al., 2002). OTP providers reported an increase in positive urine toxicology for illicit drug use for those who returned when the OTP reopened (Frank et al., 2006).
Hurricane Katrina (August 23-31, 2005) is another example of the consequences of a short notice event on methadone patients. Evacuated patients arrived in other states without personal identification, proof of enrollment, or dosing regimens (Bloodworth et al., 2007; Carlisle Maxwell et al., 2009; McClure et al., 2014). Many were beginning to experience symptoms of withdrawal when they arrived in the Houston Astrodome and were mistakenly quarantined as their symptoms (e.g., diarrhea) mimicked an infectious disease (Carlisle Maxwell et al., 2009). Local OTPs reported being completely unprepared for the number of patients they were forced to absorb given the federal prohibition against dispensing methadone from the shelter setting (Bloodworth et al., 2007; Carlisle Maxwell et al., 2009; McClure et al., 2014; Rutkow et al., 2012). Clinicians were challenged to know how to structure their treatment given the absence of dose information (Carlisle Maxwell et al., 2009; Rutkow et al., 2012; SAMHSA, 2015), and were often forced to wait for patients to exhibit withdrawal symptoms to reestablish the baseline dosages required to eliminate withdrawal (Carlisle Maxwell et al., 2009). SAMHSA responded to clinicians from guest programs who were concerned about dosing unknown patients and issued clinical guidance to the State Methadone Authorities (SMA) and OTPs in the states directly affected by Hurricane Katrina to guide short- and long-term treatments (Bloodworth et al., 2007; Rutkow et al., 2012).
In the aftermath of Hurricane Sandy (October 22-November 2, 2012), difficulties with maintaining continuity of care for methadone patients surfaced again. There were reports of patients using illicit drugs and resorting to high-risk injection practices to alleviate the symptoms of withdrawal (Matusow et al., 2017; “Hurricane Sandy and Daily,” 2012; Pouget, Sandoval, Nikolopoulos, & Friedman, 2015). Public transportation and roadways were not in service, and patients, especially those with physical disabilities, struggled to get to guest-dosing programs (Matusow et al., 2017; “Hurricane Sandy and Daily,” 2012). Verifying patients and communicating dosing information were again issues (Matusow et al., 2017; McClure et al., 2014). OTP providers complained about poor communication with regulatory agencies, confusion about the emergency dosing rules, and a lack of flexibility by DEA enforcement (McClure et al., 2014). They stated that permission from regulatory agencies to release take-home doses prior to the storm was not communicated to them and there was a lack of clarity about when the emergency dosing rule started and stopped (McClure et al., 2014). Had the communication occurred, the OTPs could have released doses to carry their patients through the course of the storm (McClure et al., 2014). There was wide interpretation of the emergency dosing rules across various programs (Matusow et al., 2017). Large numbers of patients desperately crowded into emergency departments where some were turned away or given methadone dosages that were much higher than their usual treatment doses, putting them at risk for fatal methadone overdose (McClure et al., 2014). Unfortunately the emergency dosing period lapsed during the disaster period and regulatory agencies ordered some providers to cease guest dosing (McClure et al., 2014). Some administrators and pharmacists felt an obligation to bend the rules to continue dosing patients, and then worried about their own legal exposure (McClure et al., 2014).
Examples of successful methadone continuity after major disasters are difficult to find in the literature. Emergent care for 68 patients who were receiving daily methadone from an OTP destroyed by the 2011 Joplin tornado was facilitated by an electronic health record shared between two treatment facilities, one located in Joplin and the other in Springfield, Missouri (Abir, Mostashari, Atwal, & Lurie, 2012). Each facility had separate databases with security provisions that allowed need-to-know access for the other to facilitate a regular request for guest dosing or guest dosing in the event of a disaster. Because the data for each were stored at a central location in Texas, dosing information for the patients from Joplin was preserved and accessible to the Springfield treatment facility, facilitating the latter’s ability to provide guest dosing (Abir et al., 2012).
Very little is known about how OTP emergency preparedness planning contributed to the disruptions experienced following previous disasters. Elliott et al. (2017) underscored the need for OTPs to have emergency plans in place regarding continuity of operations, communications, transportation, staffing, and guest and take-home dosing (Elliott et al., 2017). Their findings indicate that emergency plans vary widely, are not exercised, and tend to be out of date or incomplete (Elliott et al., 2017; Frank et al., 2006; Matusow et al., 2017). They generated a set of recommendations after interviewing OTP patients, staff, and directors from disaster-prone states. Their suggestions for improving OTP preparedness plans are consistent with the suggestions made by others, and include activities such as maintaining up-to-date contact information for patients and clinic staff, conducting disaster drills, and establishing memoranda of agreement with neighboring OTPs (Carlisle Maxwell et al., 2009; Frank et al., 2006; Tofighi et al., 2014). Their findings were then presented to SOTAs from these states, as well as representatives of DEA and SAMHSA. The authors articulated strategies for improving disaster preparedness planning, the SOTAs’ role, and interagency cooperation (Elliott et al., 2017).
When Hurricane Sandy made landfall in New York City in 2012, the Manhattan Veterans Affairs (VA) OTP was serving approximately 100 Veterans on methadone maintenance therapy. This facility, which was co-located at the Manhattan VA Medical Center (VAMC), was one of only two VA OTPs in the region and the only OTP program within the VA New York Harbor Health Care System (NYHHS). The temporary, hurricane-related closure of the Manhattan VA OTP provides another opportunity to learn from the experiences of an OTP that closed, with little notice, for an extended period.
Method
Three months after Hurricane Sandy, we conducted 31 semistructured interviews with executive managers, senior clinicians, and administrators who participated in the evacuation of the Manhattan VAMC, including the co-located OTP, 1 day prior to Hurricane Sandy. Due to damage from the storm, outpatient services remained closed for 5 months and inpatient services remained closed for 8 months.
The interview guide was developed based on an instrument from a prior study examining VA nursing home evacuations after Hurricanes Katrina and Rita (Claver, Dobalian, Fickel, Ricci, & Mallers, 2013), a hospital evacuation tool (Schultz, Koenig, Auf der Heide, & Olson, 2005), and the hospital evacuation literature (Bagaria, Heggie, Abrahams, & Murray, 2009; Chavez & Binder, 1996; Gray & Hebert, 2007; Sternberg, Lee, & Huard, 2004). Topic areas included prior disaster response experience, participation in disaster preparedness planning and exercises, preparations and planning in the days leading up to evacuation, the evacuation decision process, and operations and logistics of evacuation. Open-ended questions were constructed to elicit responses in a conversational style and to encourage participants to expand on experiences, such as the challenges to maintain methadone treatment (Ricci, Griffin, Heslin, Kranke, & Dobalian, 2015).
All interviews were audio recorded and transcribed. The Atlas.ti software program (Version 7.1.6, Scientific Software Development GmbH, Berlin, Germany) was used to manage the analysis of the transcripts. The first author read and coded the first five interviews using an initial list of a priori codes based on the interview guide and hospital evacuation literature. To establish reliability, three other members of the research team read the same five interviews and reviewed the assigned codes. Discussions and reconciliation resulted in a master code list that was used to recode the first five and remaining interviews. This study was approved by the VA Greater Los Angeles Healthcare System’s Institutional Review Board (Los Angeles, California USA).
Results
With the impending threat of Hurricane Sandy, approximately 100 patients enrolled in the NYHHS VA OTP were asked to come in on Friday (October 26, 2012) to receive several emergency take-home doses of methadone that were anticipated to last for the duration of the storm and its immediate aftermath. The entire Manhattan VA campus was evacuated on Sunday (October 28, 2012), the day before Hurricane Sandy made landfall. The evacuation included a VA hospital and a broad range of outpatient clinics including a VA OTP. Only a small team of emergency clinicians, engineers, security staff, and administrators stayed behind to protect the campus.
The following morning, an OTP nurse and pharmacist joined the team at the facility to assist any OTP patients who might show up for dosing. Some methadone patients did show up, and were dispensed doses to last them into the following week. These patients were reminded about neighboring OTPs where they could go to receive guest dosing should the campus not reopen within several days.
There were a number of patients that came in and [the pharmacist] was able to give them [emergency doses of medication]—still not thinking it was going to be so long—a few days to get them covered. . .
The OTP staff gathered what written documentation they could from their electronic medical record (EMR) prior to losing power. This documentation could facilitate NYHHS OTP patients who needed to seek guest dosing from non-VA OTPs or VA OTPs not within the NYHHS network.
Getting information that we need to have in our hands because it’s all computerized to say yes to another clinic. [The care is] legitimate. These patients are in our program.
As predicted, the storm arrived that evening (October 29, 2012). A six-foot wall of salt water rushed into the Manhattan VAMC facility, causing widespread devastation. Within hours of the storm surge, it became apparent that it would take months to repair the extensive damage to the Manhattan facility.
Although the medical center evacuation was deemed a success, a group of clinicians and administrators recognized that a new emergency was unfolding. Specifically, OTP patients would need to resume their regular doses almost immediately; methadone dosing arrangements rose to be a top priority for Manhattan VAMC staff within the first 24 hr.
That was actually a big problem. That was a huge problem. That was our most immediate problem, . . .making sure that they were getting dosed. That was the most time-sensitive issue because within 24 hours we had to address that . . . . when Sandy hit, we had no facility to take care of those [methadone] patients.
A senior clinician reported that approximately half of the patients were directed to the closest VA OTP, located in the Bronx, but which was outside the VA NYHHS. The remaining patients were absorbed into non-VA OTPs throughout New York City, including facilities at Beth Israel and Cabrini, even though many of those facilities were also in the storm impact area.
A lot of other facilities took emergency care of our patients because they can’t go for too many days without Methadone.
Nevertheless, a senior clinician reported that the effort to arrange guest dosing and provide dose verification was challenging because the computers were down and service for satellites, landlines, cell phones, and texting was sporadic. While the VA uses an EMR, it was not capable of transmitting dose information to the non-VA OTPs. Moreover, because the Bronx VA OTP was not part of the VA NYHHS, patient records from the Manhattan VA were not accessible to Bronx VA clinicians. Fortunately, VA OTP staff had printed dose verification records from the EMR several days before the storm.
It’s a requirement for methadone programs that they have contingency plans [describing] how to dose patients, so-called courtesy dosing. Patients have resources how to find out what their neighborhood nearby methadone programs are [and] the programs could verify and courtesy dose. But, that’s something you think about lasting a day or two. . . This was a longer-term problem.
The surge of patients experienced by the Bronx VA OTP was reported to be overwhelming. Fortunately, the VA deployed several counselors and a physician to assist this OTP with order verification and dispensing of medication.
The Bronx started getting a little panicky because they were being overwhelmed in terms of the number of patients. They asked if we would provide staff. So, that’s when we started sending several counselors up, and even had a physician for a while helping them with their orders.
Despite the successful transfer of OTP patients to other facilities, the emergency dosing period passed quickly and a long-term solution was still needed. Coincidently, the NYHHS had a previous OTP on the Brooklyn VA campus. The OTP had closed a few years prior, but the OTP unit environment remained intact. Reopening the Brooklyn OTP would still require that it meet regulatory requirements and complete the accreditation process.
Then it became apparent that we needed, after we were getting beyond the envelope of what constituted the emergency, we then needed to set up an opiate treatment program. Then it gets a little bit dicey because then it starts getting into regulatory issues with the DEA. You can’t just willy-nilly open-up a program.
Fortunately, the Brooklyn VA site was approved within 1 week, an uncharacteristically short length of time. As reported by interviewees, It was serendipitous that a methadone clinic at another [NYHHS] facility had been closed, but it was still equipped with all the proper locks, alarms and physical layout. Within three days, the DEA had approved the new unit. It’s because we literally had this thing that had been mothballed. Otherwise, we never would have been able to open-up a methadone clinic. We would have had to [contract out for care] or otherwise come up with alternative sites to provide care to our opiate treatment patients.
This fortunate situation would not likely be the case for most OTPs.
Discussion
Hurricane Sandy provided sufficient warning for the Manhattan VA OTP staff to implement emergency take-home dosing to cover daily methadone during the storm period. Staff reported for duty the day after the evacuation to gather vital documents in case they needed to verify patients to guest programs. Despite these efforts and having an EMR, staff still had to transmit dosing information to both VA and non-VA programs during the storm recovery period. The Manhattan patients overwhelmed the Bronx VA OTP, and extra staff had to be sent to accommodate the surge. It was only because the VA could restore a mothballed methadone clinic that an alternative OTP site could open quickly. The scenario for this VA is not the norm for most OTPs, whether VA or non-VA, following disasters. Without the retired OTP, the Manhattan VAMC would have had to create a new program and go through the entire accreditation process, which typically requires many months before approval is obtained.
One year prior to Hurricane Sandy, the same Manhattan VA OTP evacuated prior to the arrival of Hurricane Irene (August 2011), but in contrast to Hurricane Sandy, the damage caused by Hurricane Irene was not extensive and services were restored within 3 days. If Hurricane Sandy had played out like Hurricane Irene, dispensing emergency take-home doses of methadone for several days would have been sufficient. Instead, the damaging storm surge caused by Hurricane Sandy led to a closure that exceeded the typical timeline for emergency take-home dosing and emergency guest dosing. While the existing provisions for guest dosing provided an immediate solution in the aftermath of the disaster, the timeframe was insufficient because of the long-term damage caused by Hurricane Sandy.
Moreover, OTP services cannot be easily relocated. Each OTP has its own unique accreditation which cannot be transferred to another location. Operations must cease if a damaged OTP cannot reopen by the time provisions for emergency guest dosing expire. Reopening from a new location would require the fulfillment of all federal, state, and local laws, and regulations as for any other new facility.
Further complicating care after a long-term disaster, OTP patients cannot easily move from one OTP to another. Rules and mechanisms are in place to confine patients to one, home OTP where patients must present daily, in person to receive a carefully titrated dose of methadone. This dosage could be vastly different from the dose another patient receives.
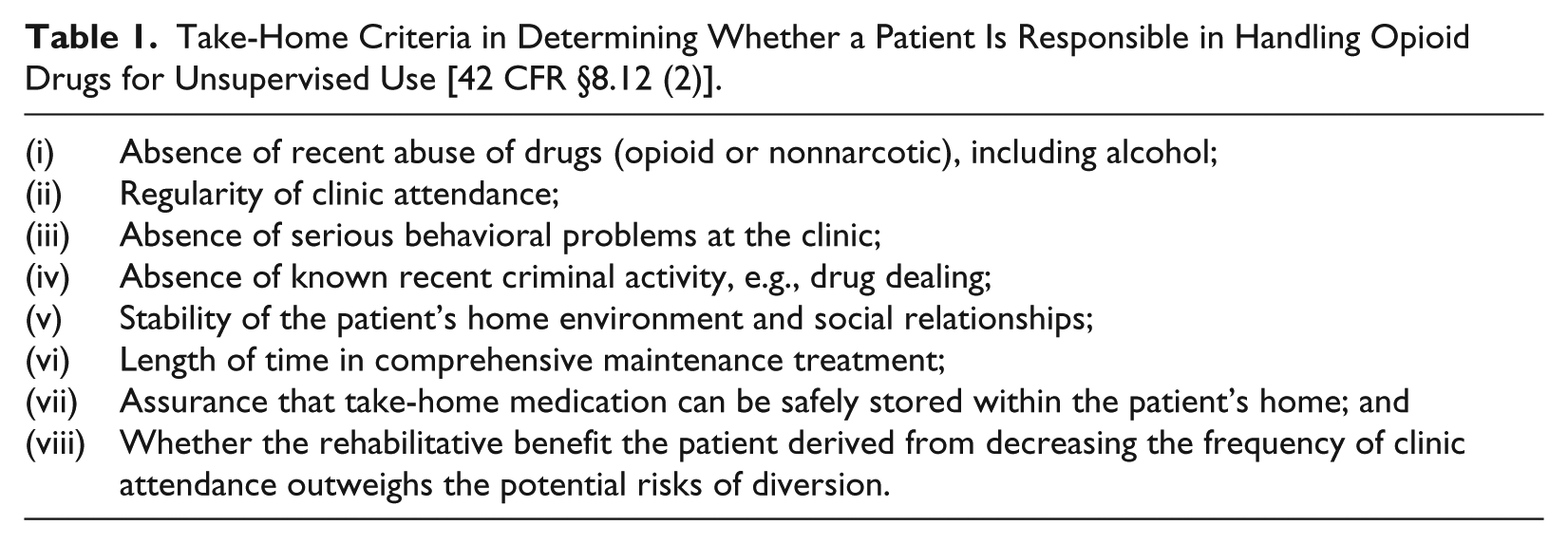
Under normal nonemergent circumstances, the opportunity for the unsupervised use of methadone away from the home OTP is highly restricted. Patients must be enrolled in comprehensive maintenance therapy and meet strict criteria for handling unsupervised dosing (see Table 1). For those who are eligible, the weekly take-home allowance is extremely conservative—one dose, which can be increased by one dose every 90 days thereafter for the duration of 1 year, after which the regulations further relax after a year of compliance. Guest dosing to accommodate travel for a personal emergency is also for a short period, and requires a record of justification and request for exception from SAMHSA (2015).
Take-Home Criteria in Determining Whether a Patient Is Responsible in Handling Opioid Drugs for Unsupervised Use [42 CFR §8.12 (2)].
Authorizing emergency take-home doses or emergency guest dosing privileges following disaster, even if for only several days, represents a stark contrast to the strict rules normally governing unsupervised use. Despite what could be perceived as a very lenient provision, it is an insufficient solution to meet patient needs after a major disaster when clinics require weeks or months to resume operations.
OTP regulations stipulate that every patient should be educated about emergency procedures and given an identification card that includes information about their medication regimen. Emergency plans should include the availability of staff to retrieve and transmit current dosing information to guest dosing programs that have been predetermined and established to be in good standing with accreditation and DEA requirements.
SAMHSA provides guidelines for OTPs to create a continuity of operations plan in the event of a disaster (Elliott et al., 2017). In response to the issue of dose verification, the agency promoted the development of technologies and standards to enable the exchange of behavioral health data, but logistical issues redirected those efforts. Currently, the National Council for Behavioral Health, funded by SAMHSA and Health Resources and Services Administration (HRSA), has established a Center for Integrated Health Solutions (CIHS) to provide training and a health information exchange that includes mental health and substance use policy and IT solutions. Resources collected from five states are now available to guide other states on topics such as amending state legislation, and exchanging behavioral health and physical health information between treatment facilities (Elliott et al., 2017).
Nonetheless, the fundamental question remains unanswered regarding how highly regulated OTPs can respond to extended closures in the wake of major disasters and ensure continuity of care for their at-risk patients. The continued challenges faced by the strict and sometimes rigid regulation of OTPs endanger an increasing number of Americans affected by opioid dependence. Despite numerous lessons learned following previous disasters, Hurricane Sandy again demonstrated that this same issue has not yet been adequately addressed.
Conclusion
The challenges faced by the Manhattan VA OTP during Hurricane Sandy were consistent with the experiences of other OTPs during other major emergencies. Strict accreditation standards, statutes, and regulations are designed to ensure the safety of methadone delivery and prevent its diversion and misuse. However, they also markedly complicate methadone delivery when OTPs are forced to close for more than a few days. Unlike most OTPs, the Manhattan VAMC was extremely fortunate in that it was able to reestablish a closed OTP site. This would not be the norm for most OTPs during disasters, including other VA OTPs. OTPs must maximize their contingencies for emergency response. However, disruptions in methadone delivery and threats to patient safety are likely to continue until agencies with oversight authority of OTPs describe specifications for emergency alternate care sites during long-term disaster recovery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.