
Abstract
Police officers and emergency personnel are on the frontlines of the opioid crisis. This research examines police officer attitudes about naloxone administration, drug treatment, and their role in handling drug-related incidents through an online survey. Although officers view themselves as adequately trained in administering naloxone/Narcan, almost half (43%) believe there should be a limit on how often someone who overdoses receives Narcan and the majority (83%) view naloxone/Narcan as providing an excuse to continue drug use. Officers also view drug treatment as ineffective. Negative attitudes differed as a function of frequency of overdose responses; officers who responded to more overdose calls and administered naloxone more frequently demonstrate more pessimistic attitudes toward drug treatment and the use of naloxone/Narcan. Officers more frequently exposed to drug overdoses need education and training about drug addiction issues to decrease stigma and elicit greater empathy toward people struggling with addiction.
Introduction
The opioid overdose death rate in the United States continues to be a major national issue. In 2019, research showed that, for the first time in history, the likelihood of dying from an accidental opioid overdose was higher than for dying in a car accident (National Safety Council, 2019). Deaths from opioids is also a major contributor to declining life expectancy in the United States (Centers for Disease Control and Prevention, 2019). Because of the dramatic increase in opioid-related deaths, President Trump declared opioid abuse and related deaths to be a public health emergency in 2017. Similarly, many of the most-effected states have also declared their own statewide emergencies in an effort to reduce opioid overdose deaths. In 2017, the states with the highest death rates for drug overdoses were found in West Virginia (57.8), Ohio (46.3), and Pennsylvania (PA; 44.3).
One policy response to this crisis has been an increase in the availability and use of naloxone (Narcan), an overdose-reversing drug. By 2017, every state passed legislation increasing access to naloxone (NCSL, 2017; Parker et al., 2018). In addition, most states have passed “Good Samaritan” laws preventing arrest for possession and other low-level drug offenses during an overdose call (NCSL, 2017). These policies have been linked to reduced death rates from opioid overdoses (Abouk et al., 2019; Rando et al., 2015; Rees et al., 2017). Still, little research has examined police attitudes toward the administration of naloxone and their views of drug addiction and treatment. Given that they are often the first responders to drug overdose calls, police officers can serve as a positive referral source for someone to enter drug treatment (Formica et al., 2018; Schiff et al., 2017). However, if they feel overwhelmed by overdoses in their community, or hold stigmatizing views toward people who use drugs, police officers may have negative interactions with them or may not want to engage with people who need treatment. The current study explores police officers’ attitudes toward the use of naloxone, their role in the opioid crisis, and how they view drug addiction and drug treatment. It also investigates the extent to which exposure to overdose incidents might affect these attitudes.
Attitudes Toward Naloxone (Narcan)
It has become much more common for police officers and other first responders to carry naloxone in the last few years (Lurigio et al., 2018). In many areas, community residents can also obtain naloxone at no cost and, often, anonymously (Wheeler et al., 2015). There is widespread public support for naloxone expansion (Rudski, 2016), and police chiefs have shown support for carrying naloxone (Smyser & Lubin, 2018). Still, the increasing availability of naloxone is not without controversy, and people who hold stigmatizing views toward opioid users may be less likely to support nonprescription naloxone access (Calabrese & Bell, 2019).
Because this is a relatively new development in policing, there is not much research on police officers’ attitudes about responding to overdose calls and using naloxone. A 2013 study examined police knowledge and attitudes about the Good Samaritan law in Washington State, finding that only 16% of police respondents knew about the law, which had been in effect for over a year (Banta-Green et al., 2013). The same survey found that police officers were more likely to have negative views of the immunity component of the law. About 22% of officers also viewed naloxone as enabling drug use. Similarly, Green et al. (2013) conducted interviews with 143 officers in two states and found officers often felt a sense of ineffectiveness and helplessness and a loss of empathy for individuals who overdose. Other researchers have found police officers often feel as though naloxone/Narcan provides a free pass and enables drug users to continue their use (Beletsky et al., 2005; Burris et al., 2009; Green et al., 2013) or engage in riskier drug use (Reichert et al., 2019; Saunders et al., 2019).
Overdose training and training on the use of naloxone for first responders and law enforcement has shown much success in increasing knowledge about opioid overdose and addressing concerns about naloxone administration, as well as improving self-efficacy in responding to overdose calls (Crocker et al., 2019; Dahlem et al., 2017; Khorasheh et al., 2019; Kitch & Portela, 2016; Purviance et al., 2017; Ray et al., 2015; Saucier et al., 2016; Simmons et al., 2016; Wagner et al., 2016). However, research that examines police officers’ training and attitudes about naloxone has rarely also included an examination of their attitudes toward people who use drugs, and none have assessed their knowledge about addiction. This study attempts to bridge these areas of previous research to better understand how stigma can play a role in police officers’ views of the opioid crisis.
Stigma and Drug Addiction
A growing body of research reveals significant public stigma toward people who use drugs and people with substance use disorders. Research on stigma toward people who have a substance use disorder typically use measures of social distance and perceived dangerousness as the primary indicators of stigma (e.g., Barry et al., 2014). Some of the items that social distance scales include are how comfortable the respondent is with a person with a drug addiction marrying into their family, living near them, or closely working with them. Perceived dangerousness scales attempt to measure negative labels toward people, fear, and distrust (Link et al., 1987). Other stigma measures include questions about the acceptability of discrimination toward people who use drugs and respondents’ attitudes toward drug treatment (Barry et al., 2014). Research studies, utilizing multiple measures of stigma, show that there is a great deal of public stigma toward people who use drugs, especially toward those who inject drugs (Barry et al., 2014; Calabrese & Bell, 2019; Corrigan et al., 2009; Crandall et al., 2002; Luoma et al., 2007). Recent research finds similar public stigma toward people who misuse opioid prescriptions, with respondents largely viewing these individuals as responsible for their problem and endorsing measures of social distance and dangerousness (Cooper & Nielsen, 2017; Kennedy-Hendricks et al., 2017).
Research also shows that people often view drug addiction more negatively than mental illness. For example, Barry et al. (2014) used a national web-based survey to compare attitudes toward people with mental illness and people with a drug addiction and found that 90% of the sample indicated they would be unwilling to have a person with a drug addiction marry into their family (compared with 59% who indicated the same measure of social distance toward someone with a mental illness). Corrigan et al. (2009), through a random web-based survey, also found higher stigma toward people with drug addiction compared with those with mental illness or a physical disability. The same study found that 64% of respondents felt that employers should be allowed to deny employment to persons with drug addiction and 54% thought landlords should be allowed to deny housing to a person with a drug addiction.
Although few studies have examined stigma among police officers explicitly, research shows that they also can hold stigmatizing views of people who use drugs. Wagner et al (2016), in an evaluation study of naloxone training among San Diego police officers, showed officers having high levels of agreement with statements like “People who overdose are to blame for their own overdose” and no improvement in attitudes toward overdose victims was found at post training. In a qualitative study of police officers in an urban area, Beletsky et al. (2005)’s interviews revealed police officers showed some empathy with drug users’ experiences but also felt that people who used drugs were to blame for their problems. In an exploratory study of post-overdose outreach programs in Massachusetts, Formica et al. (2018) found that police officer stigma was the most common barrier to implementing programs where law enforcement officers are supposed to help overdose survivors connect to treatment programs.
Related to this stigma are the increased feelings of burnout, pessimism, and exhaustion that can result from interacting with people who overdose. For example, Green et al. (2013) interviewed police officers who discussed losing empathy for people who use drugs in the context of the opioid crisis. Similarly, Saunders et al. (2019) found that emergency responders in New Hampshire, including police officers, expressed feelings of fatigue, burnout, and helplessness after increased exposure to overdoses. Gnann (2019) also found stigma among police officers, who expressed frustration when the same person received naloxone multiple times and viewed naloxone as enabling drug users. Haug et al. (2016), however, in an analysis of Twitter postings about administering naloxone, found police officers to have low levels of these attitudes. These studies are useful for illustrating how police officers view people who use drugs and naloxone policies, but they are all, apart from Wagner et al.’s. (2016), qualitative studies with very small sample sizes. More research is needed to see how widespread these stigmatizing attitudes are among police officers and how they are impacted by the use of naloxone.
On a positive note, various training programs have had success in reducing police officer stigma, most notably in the area of mental illness. The police-based “Crisis Intervention Team (CIT)” model has been implemented in many police departments across the United States and has shown improved knowledge on mental illness and reduced stigma among officers who have completed the 40-hr training (Bahora et al., 2008; Compton et al., 2014; Hanafi et al., 2008). In addition, police officers tend to view the program positively (Schaefer Morabito et al., 2013). One study found that officers who completed the CIT training also showed reduced stigma toward people with cocaine or alcohol use disorders (Bahora et al., 2008).
Reducing stigma is an important step in addressing the opioid crisis because stigma has been cited as a barrier to accessing treatment and can lead to poor retention in drug treatment and other negative outcomes for mental and physical health (Cooper & Nielsen, 2017; Fischer et al., 2002; Keyes et al., 2010; Latkin et al., 2013; Link et al., 1997; Luoma et al., 2007; Murphy, 2015; Semple et al., 2005).
Given police officers’ role in responding to overdoses, assessing their attitudes about drug treatment, use of naloxone, and stigma levels is important (Saloner et al., 2018). This study measured stigma levels and attitudes toward people who use drugs, along with naloxone experience, among local police officers in PA. PA enacted Act 139 in 2014, which enabled first responders, including police officers, to administer naloxone while also providing immunity to those reporting overdoses. As a result, police officers complete a mandatory online training about opioids and naloxone use. This Act has led to widespread use of naloxone by law enforcement, with a recent survey of PA police reporting 91% of officers statewide having access to naloxone (Jacoby et al., 2020). That same survey also had police officers indicate that in over 73% of overdose calls, police officers were the first to respond.
Despite the widespread use of naloxone by law enforcement, there has been little to no research that has examined whether officers with greater exposure to overdose and administration of naloxone/Narcan would lead to more negative attitudes toward drug treatment and utilization of naloxone/Narcan. Given the results found in previous studies of police officers’ attitudes toward naloxone use (Gnann, 2019; Green et al., 2013; Saunders et al., 2019), we suspected that the greater the exposure to overdoses, the less likely they would believe in the effectiveness of drug treatment programs and policies. Similarly, we suspected that officers who had less exposure to overdoses and administering naloxone/Narcan would be more positive about its use and have less stigma toward individuals with drug addiction. In fact, it is possible that the number of times responding to overdose incidents and administering naloxone/Narcan may have additive effects toward individuals with drug problems. This article explores these effects to not only understand officer attitudes toward drug treatment and the use of naloxone/Narcan, but to determine whether greater exposure to overdoses and the use of effective overdose-reversing methods function to create more negative attitudes toward drug policies and procedures.
Method
Procedures and Participants
Survey data were collected between December 2018 and March 2019. Seven counties in PA were targeted because of their varying overdose death rates, as publicized by 2016 Coroner and Medical Examiner reports. One of the objectives of the study was to examine responses in the context of overdose deaths, so we wanted to include counties that showed the range of low to high overdose deaths occurring in PA. The county with the lowest death rate had 13.0 while the highest was 43.6.
We attempted to reach via email or phone every police chief in these seven counties, informing them about the research and asking them to forward the survey link to their officers. In addition, three of the counties’ district attorneys assisted in survey recruitment by sending the survey out to police chiefs in their county. We also attempted to locate email addresses for police officers in the targeted counties; we sent a description of the study and a link to the survey to the ones we could locate.
A total of 618 police officers from 21 counties in PA completed the survey, with 523 from the targeted counties (85% of the sample). Based on the number of officers in each of the targeted counties, we estimate a response rate of about 19% in the targeted counties. Full-time and part-time officers were eligible to complete the survey. The additional officers were from PA counties that were not targeted. The online survey link was likely shared via email to officers in nearby counties through social and professional networks. All surveys are included in this analysis. For confidentiality purposes, we do not report the names of the specific counties.
Respondents included 515 males (93.5%) and 29 females (5.3%) and seven identifying as nonbinary or self-described (1.2%). Sixty-seven officers did not provide demographic information. The average age of respondents was 41.36 (SD = 10.06) years and they were overwhelmingly White (n = 501, 91.6%). A small percentage identified as Latino/Hispanic (n = 22, 4.0%), Black/African American (n = 8, 1.5%), Asian American (n = 2, .4%), and “other” (n=14, 2.6%). Seventy-one participants did not include a response for race. Most officers held a bachelor’s degree (n = 260, 46.9%), some college experience (n = 120, 21.7%), an associate’s degree (n = 101, 18.2%), a master’s degree (n = 9.6%), high school (n = 16, 2.9%), or doctoral degree (n = 4, .7%). More than half of the officers reported having a family member who had problems with drug/alcohol (n = 327, 58.9%) or a close friend that has had problems with a drug/alcohol (n = 305, 54.9%). Only 15 officers (2.4% of the sample) indicated that they had personally ever had a problem with alcohol and/or drug use.
Measures
Independent variables: Overdose experiences
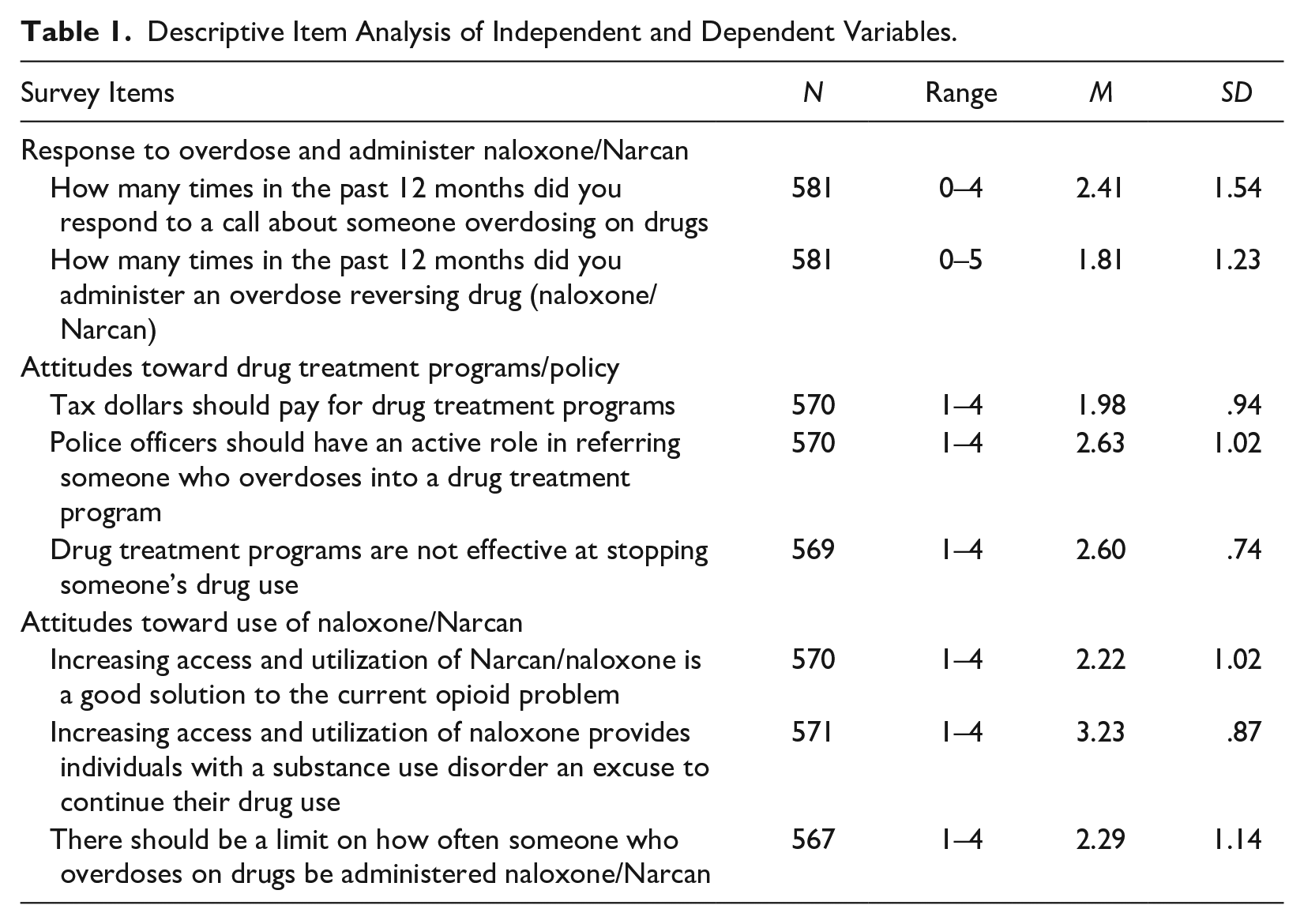
Several items measured the officer’s experience with overdose calls and administering naloxone. One question asked how many times in the past 12 months they responded to an overdose-related call, with categories of response from Never to More than 5 times. The same response categories were used for measuring how many times in the past 12 months the officer administered naloxone/Narcan. Preliminary analysis of the independent variables showed that the mean score for “How many times in the past 12 months have you responded to a call of someone overdosing on drugs” was M = 2.41 (SD =1.54) and a median of 3.00 (4–5 times). The mean and median for “How many times in the past 12 months did you administer the overdose reversing drug naloxone/Narcan to someone who had overdosed” were (M = 1.83, SD = 1.23) and median score of 1.00 (never). For the purposes of placing these variables into a multivariate analysis of variance to examine higher and lower levels of exposure to these variables, we utilized a median split (1 = less than or equal to one and 2 = greater than one) for independent variables of interest.
Attitudes toward drug treatment
Three items were used to measure officer attitudes about drug treatment and policy “Tax dollars should pay for drug treatment”; “Police officers should have an active role in referring someone who overdoses into a drug treatment program”; and “Drug treatment programs are not effective at stopping drug someone’s use.” All responses were recorded on a 4-point scale from strongly disagree to strongly agree.
Attitudes toward use of Naloxone/Narcan
Three items were used to assess officer attitudes about the use of naloxone/Narcan (e.g., “Increasing access and utilization of Narcan is a good solution to the opioid problem,” “Increasing access and utilization of Narcan provides individuals with a substance use disorder an excuse to continue their drug use,” and “There should be a limit on how often someone who overdoses be administered Narcan.” All responses were recorded on a 4-point scale, from strongly disagree to strongly agree.
Stigma
For the purpose of this study, we used a variation of the Perceived Dangerousness Scale, developed by Link et al. (1987), to examine negative labeling of mental illness. The scale was revised by the authors to refer to people who use opioids specifically. Because the vast majority of drug overdoses are now opioid-related (Hedegaard et al., 2018), we felt that the measure should refer to people who use opioids. Respondents were given five statements that they responded to on a 7-point scale measuring agreement/disagreement. Statements related to issues of trust and fear of people addicted to opioids. Cronbach’s α = .62. 1
Demographic (covariate) questions
Questions measured demographics of the officer, including race, gender, education, and age. Responses regarding their workplace included how long they had been a police officer, how long they worked in their current department, and whether they had any training about drug addiction or administering naloxone. Additional questions asked if they had any close friends or family members with drug/alcohol problems. To account for overdose variation across counties, we coded the 2016 overdose death rate for the county where the officer worked.
Results
Preliminary Analyses
We selected two sets of three items as the primary dependent variables for analysis: the three variables measuring attitudes toward drug treatment and the three items for attitudes toward naloxone. Table 1 describes the number of responses, range, and mean scores for each independent and dependent variable. Police officers have rather pessimistic attitudes toward the efficacy of drug treatment. The majority perceived drug treatment programs as not effective (56%) and only 33% agreed that tax dollars should pay for treatment. Still, nearly 62% agreed that police officers should have an active role in referring someone who overdosed into drug treatment, indicating that police officers are comfortable with that role. Police officers also have mixed views of the use of Narcan. Although almost all officers agree that their department provides adequate training on administering Narcan and they would willingly administer Narcan, a sizable proportion (43%) agreed that there should be a limit on its use. In addition, most respondents (83%) believed Narcan provides individuals with a substance use disorder an excuse to continue using drugs.
Descriptive Item Analysis of Independent and Dependent Variables.
A series of Pearson product moment correlations were performed to assess relationships between independent variables (number of times responding to an overdose and number of times administering Narcan) and dependent variables including: tax dollars should pay for drug treatment; police should play an active role in referring someone who’s overdosed into treatment; drug treatment programs are not effective. All dependent variables of interest were significantly correlated ranging from .20 to −.31. Dependent variables were also significantly correlated with independent variables of interest, number of times responding to overdose, and number of times administering naloxone/Narcan (see Table 2).
Correlations of Treatment Attitudes, Independent Variables, and Control Variables.
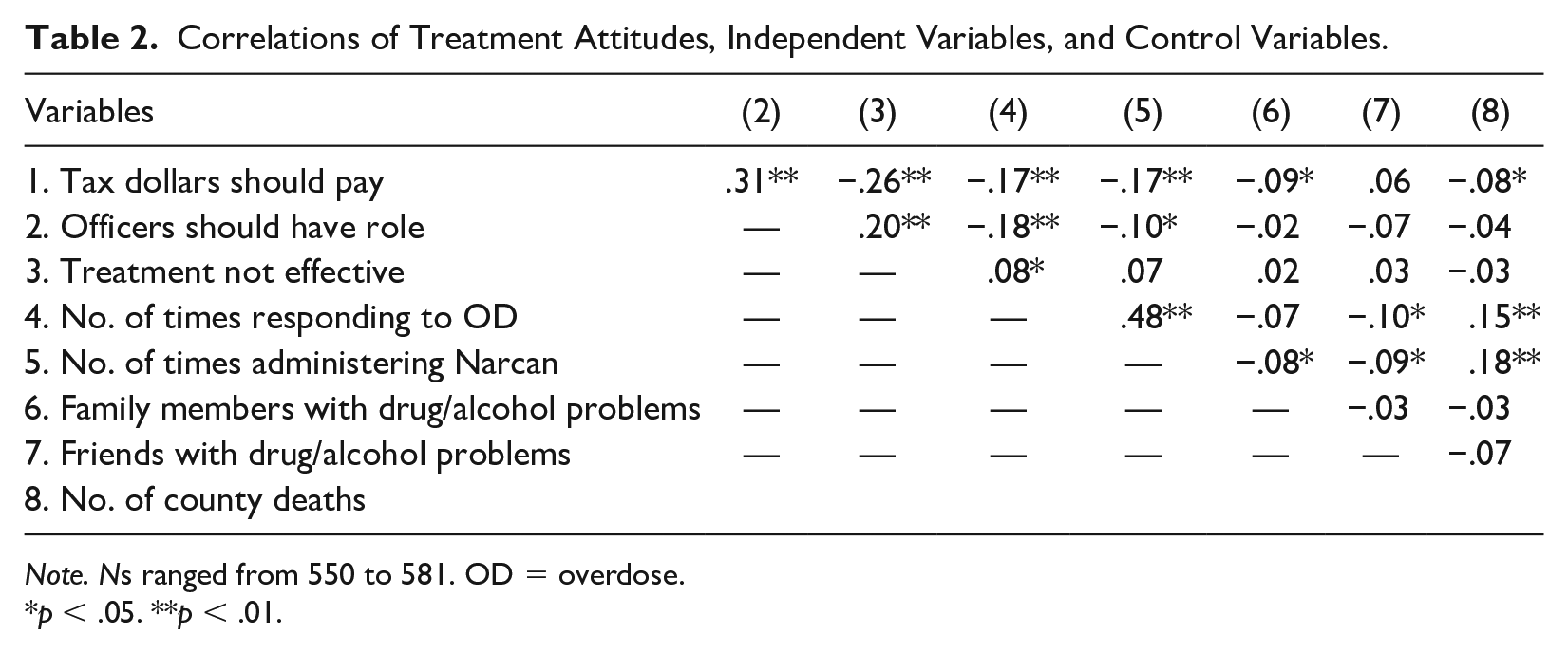
Note. Ns ranged from 550 to 581. OD = overdose.
p < .05. **p < .01.
A second Pearson product moment correlation was conducted including independent variables (number of times responding to an overdose and number of times administering Narcan and dependent variables including: limiting the use of Narcan; increasing access and utilization of naloxone/Narcan is a good solution; increasing access and utilization of naloxone/Narcan provides an excuse to continue drug use; and there should be a limit on the number of times naloxone/Narcan is administered). All dependent variables of interest were significantly correlated to each other ranging from −.44 to −.35. Dependent variables were also significantly correlated to independent variables except for endorsing limits on the use of naloxone/Narcan and how many times administering naloxone/Narcan (see Table 3).
Correlations of Narcan Attitudes, Independent, and Control Variables.
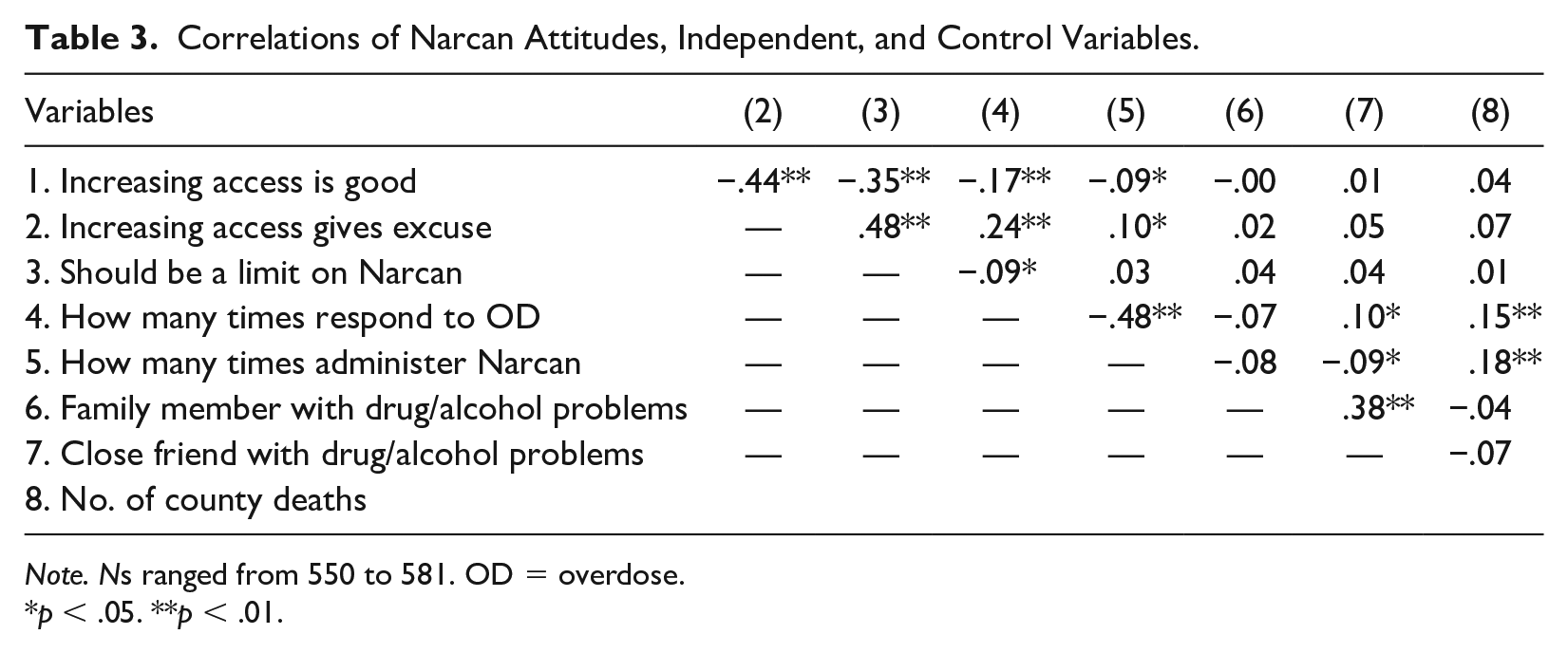
Note. Ns ranged from 550 to 581. OD = overdose.
p < .05. **p < .01.
Control variables were also added for each set of dependent variables, including officer age, gender, race, number of years of experience, education, and number of county deaths, and family member with a drug problem and friend with a drug problem. Preliminary results showed that none of the control variables were correlated to the dependent variables of interest, apart from having a friend or family member with a drug/alcohol problem. Officer experience, education, age, gender, and race were not significantly correlated to any of the variables of interest and eliminated from analyses. Having a family member with a drug/alcohol problem was related to support for using tax dollars for drug treatment, r(553) = −.09, p = .02, and having a close friend with a drug/alcohol problem was related to number of times responding to an overdose, r(552) = −.10, p = .01, and administering Narcan r(551) = −.09, p = .03. The use of tax dollars for drug treatment was related to having a family member with a drug/alcohol problem r(563) = −.08, p = .04, and number of deaths per county, r(563) = −.08, p = .04 (see Table 2). Having a close friend or family member with a drug problem and number of deaths per county were then used as covariates in subsequent multivariate analyses.
Correlational results for questions pertaining to attitudes about use of naloxone/Narcan showed none of the control variables were significantly related to the dependent variables. However, there were small but significant relationships found for number of times responding to overdose and number of times administering naloxone/Narcan and having close friends with a drug/alcohol problem and number of deaths in the county (see Table 3). Therefore, these variables will be used as covariates in multivariate analyses.
Officer Perceptions of Attitudes Toward Drug Treatment as a Function of Overdose Response and Administration of Naloxone/Narcan
The first analysis consisted of a 2 (Low/High Number of Times Responding to Overdose) × 2 (Low/High Number of Times Administering Narcan) multivariate analysis of covariance with the three dependent variables that represent general attitudes on drug treatment (tax dollars should pay for drug treatment, police should play an active role, and drug treatment programs are not effective) and having a close friend with a drug/alcohol problem, having a family member with a drug alcohol problem and number of county deaths as the covariates.
Results showed a significant multivariate main effect for how often officers responded to overdoses, F(3, 527) = 4.07, p = .007,
Results showed a marginally significant multivariate main effects for number of times administering naloxone/Narcan, F(3, 527) = 2.41, p = .06,
Mean Scores of Multivariate Main Effect for Number of Times Respond to Overdose.
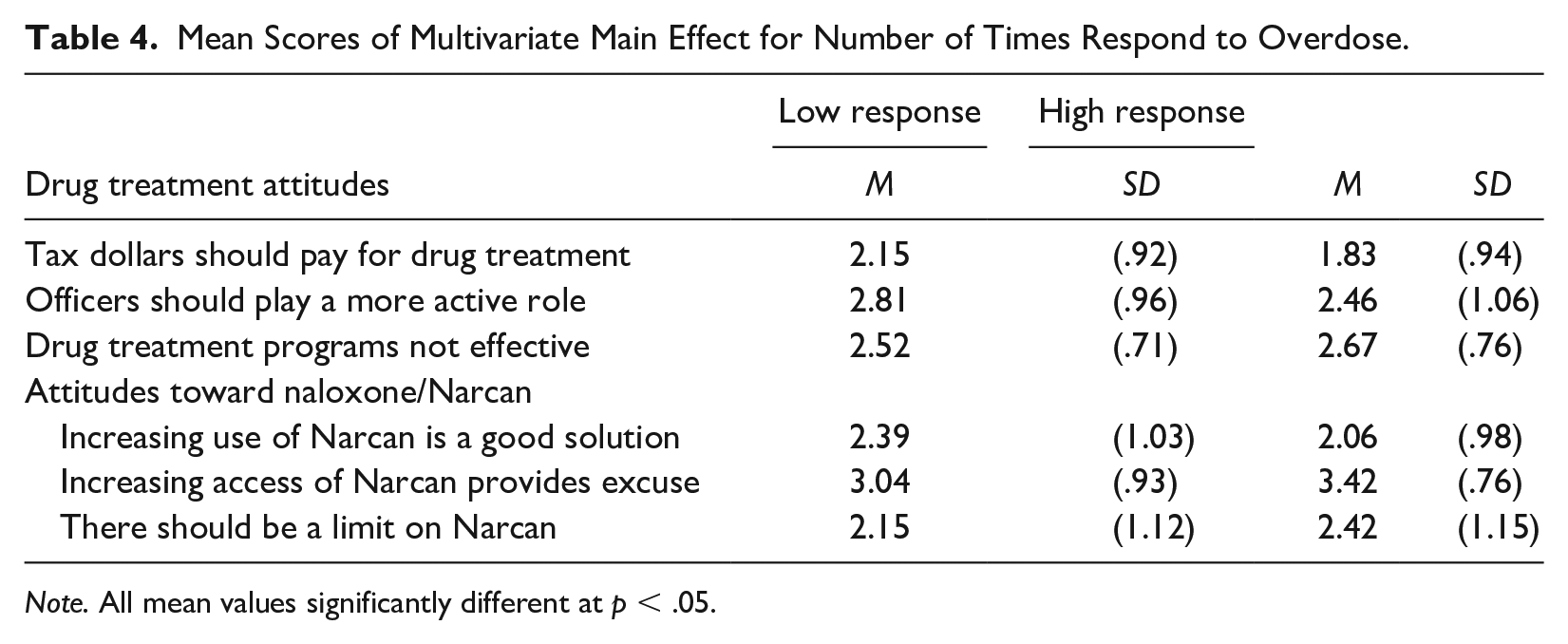
Note. All mean values significantly different at p < .05.
Officer Perceptions of Attitudes Toward Use of Narcan as a Function of Overdose Response and Administration of Naloxone/Narcan
Second, a 2 (Low/High Number of Times Responding to Overdose) × 2 (Low/High Number of Times Administering Narcan) multivariate analysis of covariance using the three dependent variables that represent attitudes about the use naloxone/Narcan was conducted (i.e., increasing access and utilization of Narcan is a good solution to the current opioid problem, increasing access and utilization of naloxone provides individuals with a substance use disorder an excuse to continue their drug use, and there should be a limit on how often someone who overdoses on drugs be administered Narcan), while variables including having a close friend with a drug/alcohol problem; having a family member with a drug alcohol problem; and number of county deaths were used as the covariates.
A significant Multivariate main effect was found for number of times responding to an overdose, F(3, 551) = 5.79, p = .001,
Preliminary Analyses of Perceived Dangerousness
Preliminary analyses were computed using two separate Pearson product moment correlations to determine relationships between each set of independent and dependent variables and control variables including officer age, experience, race, gender, education, having a family member with drug/alcohol problem, a close friend with a drug/alcohol problem, number of years of experience, and number of deaths per county.
The first set of correlations we included attitudes toward drug treatment variables, number of times responding to overdoses, number of times administering naloxone/Narcan and possible covariates. Results (see Table 5) showed no significant relationships between officer experience, gender, age, education, having a friend or family member with a drug or alcohol problem. However, number of deaths per county was the only significant relationship, r(545) = .08, p = .04 with perceived dangerousness and included in the regression model. In addition, Table 5 also shows there was no significant relationship between number of times administering naloxone/Narcan and perceived dangerousness and was removed from the regression model.
Correlations with Perceived Dangerousness and Attitudes Toward Drug Treatment.
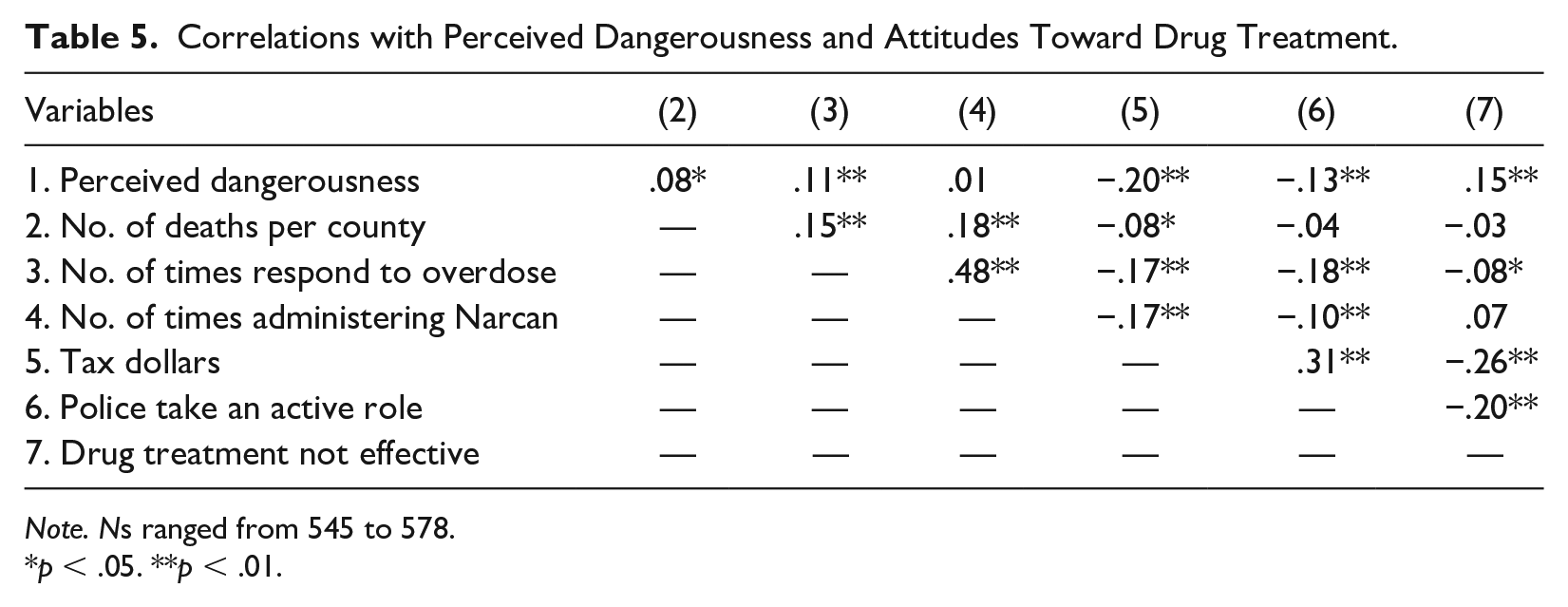
Note. Ns ranged from 545 to 578.
p < .05. **p < .01.
Predictors of Perceived Dangerousness and Attitudes Toward Drug Treatment
A multiple regression was computed using the enter method. The model included all three items assessing drug treatment attitudes and included number of times responding to overdose and number of county deaths. Results revealed the linear combination of variables was significantly related to perceived dangerousness, R2 = .11, F(5, 536) = 13.05, p < .0001. All three attitudinal variables were predictive of perceived dangerousness. The strongest predictor was the belief that drug treatment programs were not effective at stopping someone’s drug use, followed by tax dollars should pay for drug treatment programs and police officers should have an active role (see Table 6).
Regression Results for Perceived Dangerousness and Attitudes Toward Drug Treatment.
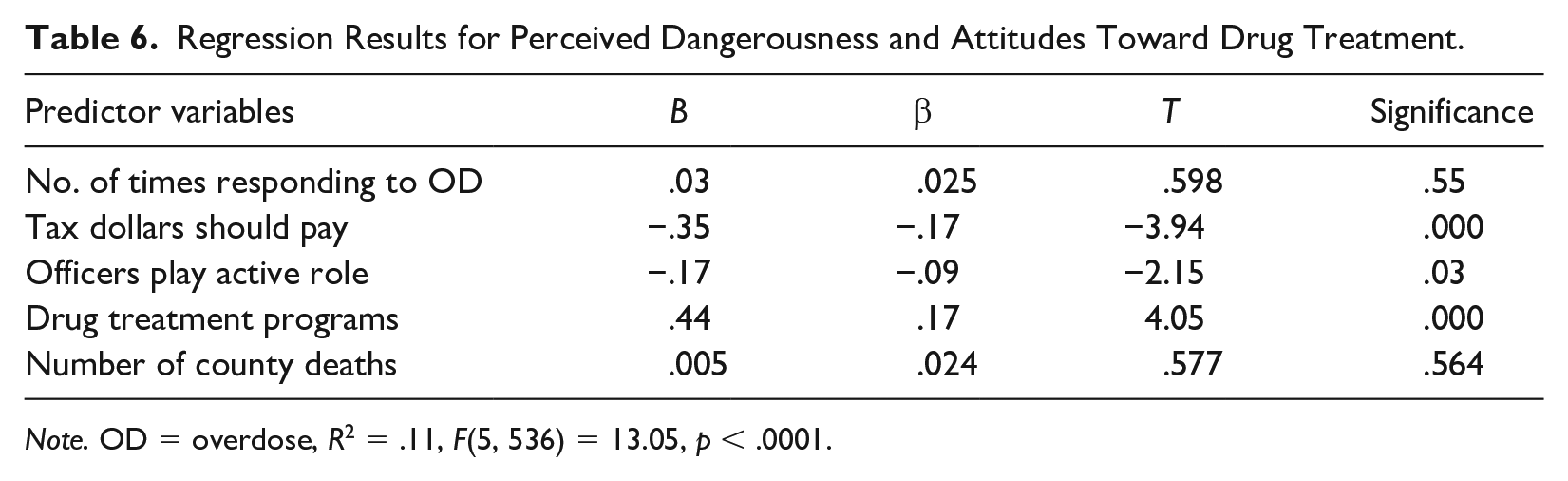
Note. OD = overdose, R2 = .11, F(5, 536) = 13.05, p < .0001.
Predictors of Perceived Dangerousness and Attitudes Toward Naloxone/Narcan
We then conducted Pearson product moment correlations to examine relationships between the set of three attitudinal variables relating to the use of naloxone/Narcan and all previous covariates. Results showed no significant relationship between administration of naloxone/Narcan and perceived dangerousness and therefore were not included in regression analyses. There were no relationships to any covariate except for county deaths, which was included in the analysis (see Table 7).
Correlations with Perceived Dangerousness and Attitudes Toward Use of Naloxone/Narcan.
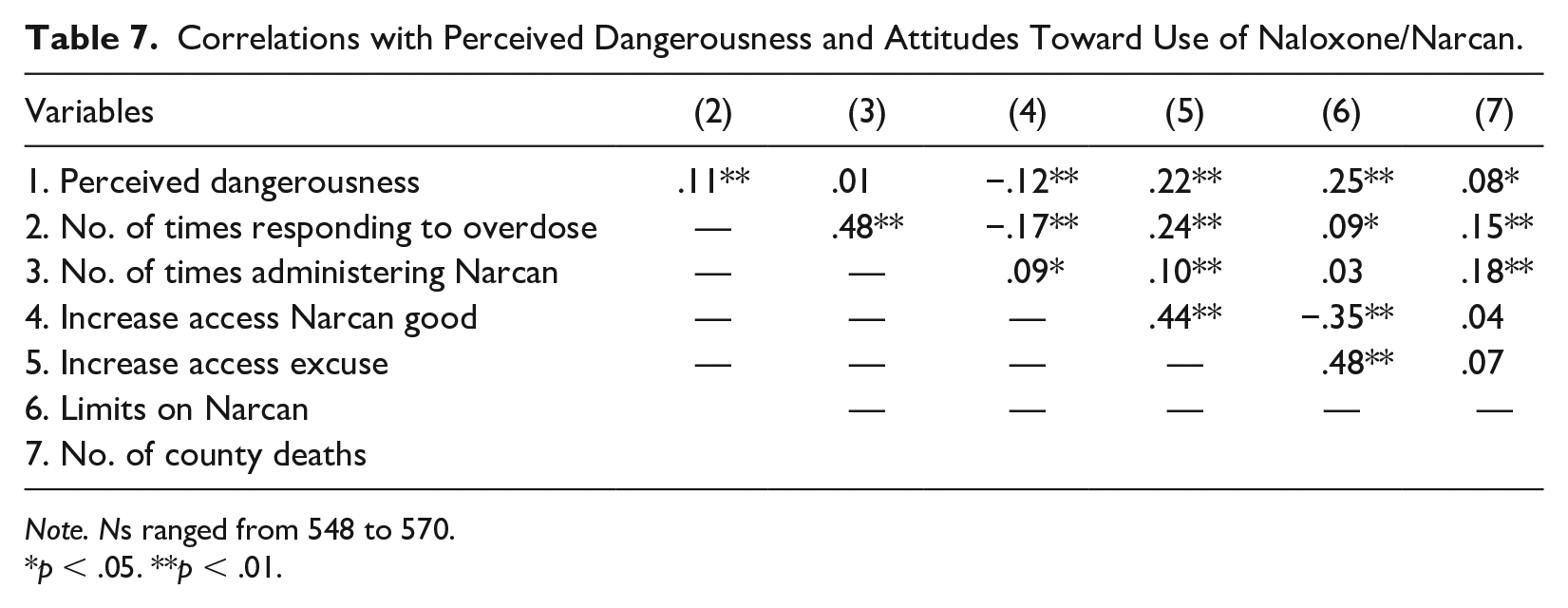
Note. Ns ranged from 548 to 570.
p < .05. **p < .01.
A second regression examined the attitudinal variables associated with the use of naloxone/Narcan. Predictor variables included number of deaths per county, how many times respond to overdoses, increasing access and utilization of naloxone/Narcan is a good solution to the current opioid problem; increasing access and utilization of naloxone provides individuals with a substance use disorder an excuse to continue their drug use; and there should be a limit on how often someone who overdoses should be administered naloxone/Narcan. Results showed the model was significant, and accounted for a significant amount of variability in perceived dangerousness, R2 = .08, F(5, 530) = 9.13, p = .000. Significant predictor variables included only two variables, increasing access and utilization of Narcan provides individuals an excuse to continue their drug use and there should be a limit on how often someone who overdoses be administered naloxone/Narcan (see Table 8).
Regression Results for Perceived Dangerousness and Attitudes Toward Use of Naloxone/Narcan.
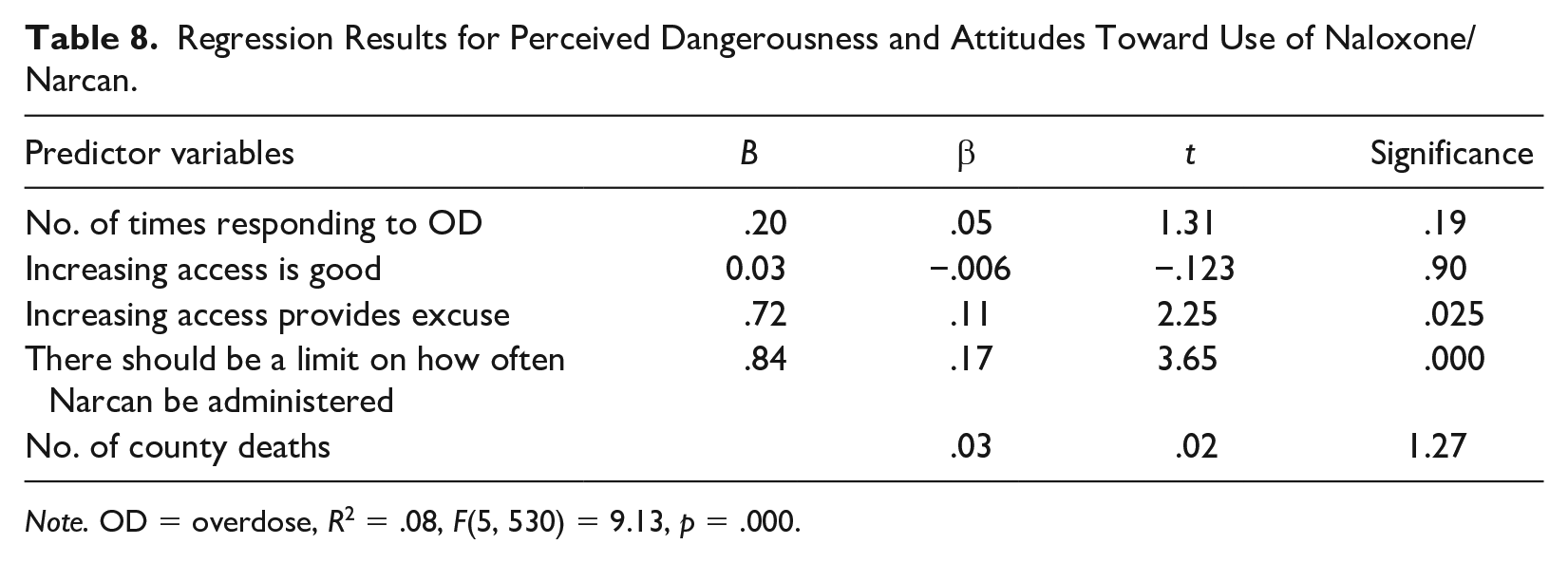
Note. OD = overdose, R2 = .08, F(5, 530) = 9.13, p = .000.
Discussion
This study sought to obtain a greater understanding of police officer’s attitudes toward drug treatment and the utilization of naloxone/Narcan. Given that police officers in PA are often the first responders to an overdose call (Jacoby et al., 2020), it is important to assess their attitudes toward the use of naloxone and their role in the opioid crisis. Like previous research, we found that police have complex views of naloxone and drug treatment. On one hand, police feel adequately trained in using naloxone and are willing to use it when needed, findings that have been shown in other studies of police trainings on naloxone (Crocker et al., 2019; Dahlem et al., 2017; Khorasheh et al., 2019; Kitch & Portela, 2016; Purviance et al., 2017; Ray et al., 2015; Saucier et al., 2016; Simmons et al., 2016; Wagner et al., 2016). Police in this study also largely agree that they have an important role in dealing with the opioid crisis. We found that they are even willing to help people access drug treatment, which is important in thinking about efforts that could better integrate law enforcement into the referral process. Two of the targeted counties in our study have recently implemented programs where police officers visit overdose victims with a certified recovery specialist and offer them assistance in accessing drug treatment. Given the results of our study, other counties should consider implementing similar programs. It may be one way for police officers to feel like they are contributing in a positive way to dealing with the opioid crisis.
On the other hand, police officers in our study still showed high levels of stigma toward people who use drugs and negative views of drug treatment. Most saw treatment programs as ineffective. Almost half agreed that there should be some limit on the use of naloxone and more than 80% believed that Narcan gives people who use drugs an excuse to continue using drugs.
The above attitudes were related to an officer’s exposure to overdoses and administering naloxone. Results of the study demonstrated the more officers responded to overdose incidents, the less likely they were to endorse using tax dollars for drug treatment, less likely to believe officers should play a role in referring drug users to treatment and less likely to believe drug treatment is effective. Although the number of times administering naloxone/Narcan to those who overdosed was only marginally significant, mean differences suggested the more officers administered overdose-reversing methods, the less likely they were to endorse the use of tax dollars for drug treatment. Surprisingly, our results showed no interaction effects, suggesting there were no additive effects, but simply the number of times responding to overdose incidents affected officer attitudes. Predictors of stigma (perceived dangerousness) included only using tax dollars for treatment and the belief that drug treatment programs were not effective. Because this study did not examine cause and effect of stigma, it is difficult to say whether officers developed greater stigma as a function of responding to overdoses. Still, the results demonstrate how stigma affects officers’ views.
Effects were also found for officer attitudes toward the utilization of naloxone/Narcan. The current study revealed those officers with less exposure responding to overdoses were more likely to believe that utilization of naloxone/Narcan is a good solution to the drug problem, while officers with more exposure to overdoses were less likely to believe it was a good solution. Previous research (Beletsky et al., 2005; Burris, et al., 2009; Green et al., 2013; Saunders et al., 2019) found that officer attitudes toward responding to overdose was often accompanied by a sense of futility, helplessness, loss of empathy, and the belief that naloxone/Narcan provided an excuse for future drug use. The current study found officers with greater exposure were more likely to believe increasing access to naloxone/Narcan provides an excuse for further drug use and its use should be limited.
We examined the use of covariates for drug treatment attitudes and utilization of naloxone/Narcan. We found only having a friend or family member with a drug problem and rates of community deaths were significantly related to attitudes, however their effects were very small and were not significant in the multicovariate analyses.
We suspected that officers who had less exposure to overdoses and administering naloxone/Narcan would have more positive attitudes about using Narcan and have less stigma toward individuals with drug addiction. Attitudes about placing limits on the use of Narcan and the belief that naloxone/Narcan provides an excuse for further drug use were the only significant predictors for stigma. The number of times administering naloxone/Narcan was not related to stigma. However, there was a small but significant correlation between stigma and number of times responding to an overdose, yet it did not contribute to the prediction of officer stigma. This may suggest that stigma, as measured by the Perceived Dangerousness Scale (Link et al., 1987), was independent of how often an officer responded to overdoses and/or the number of times they administered naloxone/Narcan. It should also be noted that these effects maybe be limited by the low scale reliability. Future research should utilize alternative methods to understand stigma to determine whether these effects are generalizable.
Given that exposure to overdoses was related to attitudes toward treatment and naloxone use, it appears that negative attitudes could be the result of compassion fatigue, especially considering that PA has the third highest overdose death rate in the country. Although police feel adequately trained to administer naloxone, they appear to lose empathy for people suffering from addiction as they respond to more overdose calls. Police departments should consider mandatory training and education programs about the science of addiction, where police officers can become better informed about the reality of drug addiction, including the role that relapse plays in the recovery process. Departments should also consider programs where police officers have open dialogues with people in recovery, especially people who have been revived by naloxone. This may offer a positive outcome of naloxone use that police typically do not see as part of their job. Other initiatives could also help improve police burnout, such as increasing participation in the Overdose Detection Mapping Application Program (http://www.odmap.org/), where overdoses are recorded in real time and data are used to create a more cohesive response to overdoses. PA is not currently participating in this program, but it could be another way to involve police in efforts that show positive results and, as an extension, may improve attitudes toward naloxone use.
Research on interventions designed to educate police officers about mental illness have shown that such interventions and training have been successful in changing police officers’ attitudes toward people with mental illness (Bahora et al., 2008; Compton et al., 2014; Ellis, 2014; Hanafi et al., 2008; Ritter et al., 2010). Training programs are also important in educating police officers about the intricacy of drug policies; a training program for police officers in Tijuana, Mexico showed positive results for increasing police officer knowledge of drug laws (Arredondo et al., 2017). A similarly structured training for police officers about the disease of addiction could also show positive results and lead to more referrals of people who overdose into drug treatment programs. Although some counties and states have implemented programs where police officers help overdose survivors access drug treatment, they are not widespread (Formica et al., 2018; Schiff et al., 2017). Engagement in drug treatment can reduce future opioid use and prevent overdose deaths. A systematic review of interventions designed to decrease stigma related to substance use disorders found that the majority of studies showed improved attitudes, reduced social distance, and increased levels of comfort among participants (Livingston et al., 2012). Such research shows that stigma toward people who use drugs can be decreased through educational programming.
Although this study provided a great deal of insight into how response to overdose affects attitudes, there are several limitations. First, some responses showed little variability and many correlations and effect sizes were small. Additional research is needed to explore whether these findings can be generalized across samples and populations. Similarly, the percent of variance accounted for in stigma were significant, but low, even after accounting for possible control variables. This suggests there are additional variables that should be identified and investigated to better explain stigma.
Conclusion
Police officers serve an important role in dealing with the current opioid crisis. Their increasing role as a first responder to overdose calls places them in a unique position to be a positive influence on whether the person who overdosed seeks drug treatment. In addition, they are often involved in drug education programs, especially in schools, putting them at the forefront of the current drug crisis. However, police can also inadvertently serve as a negative influence if they hold stigmatizing views of people who use drugs and communicate inaccurate information about drugs. Combatting the stigma around drug addiction is a crucial component of fighting the opioid epidemic and reduced stigma will lead to greater access to drug treatment for those who need it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.