
Abstract
This study examined associations among cannabis use disorder (CUD), 12-step program participation, and cannabis and other drug use at baseline and 3- and 6-month follow-ups. Participants were age 50 or older in a study of veterans receiving medical management of alcohol and/or opioid withdrawal (N = 171). Generalized estimating equations examined the extent to which time point, 12-step program participation, and CUD were associated with change in number of cannabis and non-cannabis drug use days. Also examined was whether having CUD was associated with 12-step program participation. From baseline through the 6-month follow-up, 12-step program participation increased, non-cannabis drug use decreased, and cannabis use remained stable. Twelve-step program participation at baseline was associated with better outcomes at follow-ups. Participants with CUD reported less 12-step program participation and more cannabis use days at follow-ups. Older adults with CUD may need other types of psychosocial treatments due to low participation in 12-step programs.
Use of cannabis among older adults is increasing, particularly among those ages 50 to 64 (Han et al., 2016). Use of cannabis within the past year among older adults is associated with higher psychological distress and use of other substances, including illicit drugs and binge drinking (Choi, DiNitto, Marti, & Choi, 2016). Despite higher psychological distress among older adults who use cannabis, these individuals are unlikely to attribute their problems to cannabis use, and therefore may not seek out treatment (DiNitto & Choi, 2011). The goal of the current study was to examine participation in 12-step programs and drug use outcomes among older adults with cannabis use disorder (CUD) over a 6-month period. Consistent with existing research on cannabis and other substance use, older adults were defined as 50 years old or older (Choi et al., 2018; DiNitto & Choi, 2011; Holland et al., 2016; Wu & Blazer, 2011).
Cannabis Use Disorder
The legalization of cannabis in some U.S. states has increased the availability of cannabis and the public’s favorable attitudes toward cannabis (Felson et al., 2019). Along with increased access to cannabis, the prevalence of CUD has increased (Hasin et al., 2016). Treatment rates and rates of long-term abstinence are low for CUD. For example, Hasin et al. (2016) found that only 13.2% of people with lifetime CUD sought treatment or participated in 12-step programs. Sherman & McRae-Clark (2016) found that psychological treatments reduced the frequency and quantity of cannabis use. Even so, abstinence rates were low following treatment and decreased even further long-term (Sherman & McRae-Clark, 2016). In support of this, a systematic review by Lee et al. (2019) found that the efficacy of CUD interventions is modest and very few individuals seek treatment. Wu et al. (2017) found that 92% of adults with CUD did not access cannabis-specific treatment at any point in the past year and 88% had not accessed any type of substance use treatment in the past year. Although novel approaches have been examined, such as individualized assessment and treatment focused on coping skills (Litt et al., 2020), abstinence is difficult to obtain. Much of the research on prevalence and outcomes of CUD is not focused specifically on older adults.
Older Adults and Cannabis Use
Among adults over age 50, cannabis is the most commonly used drug (Lloyd & Striley, 2018). Older adults who use cannabis are more likely than those who do not to report use of other substances within the past year, including alcohol and illicit drugs, as well as misuse of prescription drugs (Lloyd & Striley, 2018). Although substance use generally declines with age, substance use occurring within the past month doubled between 2002 and 2012 for adults ages 50 to 64 (Kuerbis et al., 2014). Among adults over age 50 who used cannabis within the past year, 23% reported cannabis use on at least half the days of the past year (DiNitto & Choi, 2011).
Negative Consequences of Cannabis Use Among Older Adults
The negative effects of using cannabis, including increased heart rate, impairments in short-term memory, and increase in the risk for heart attack, may be particularly pronounced among older adults who already have compromised cognitive status or cardiovascular functioning (Kuerbis et al., 2014). Adults over age 50 are more likely to report that they use cannabis to manage chronic medical conditions, compared with younger age groups (Haug et al., 2017). Increased rates of injury that result in emergency room visits have also been reported among adults age 50 and older who use cannabis (Lloyd & Striley, 2018).
In a study of adults age 50 and over, cannabis use within the past year was associated with increased odds of a major depressive episode. Among those with depression, increased frequency of cannabis use was associated with increased likelihood of suicidal ideation (Choi, DiNitto, Marti, & Choi, 2016). Adults age 50 and over who use cannabis are more likely to report stressful life events and lower social support than those who do not (Lloyd & Striley, 2018). Taken together, regular cannabis use among older adults is associated with significant medical and mental health problems that may lead to a need to seek out treatment or 12-step participation.
Twelve-Step Program Participation and Drug Use Outcomes Among People Who Use Cannabis
Broadly, 12-step programs such as Alcoholics Anonymous (AA) are effective in increasing long-term drug and alcohol abstinence rates (Majer et al., 2013; Witbrodt et al., 2012). There are many ways in which individuals can participate in 12-step programs, and individuals choose to be more or less involved. In a 1-year study of a 12-step facilitation intervention, involvement via meeting attendance and having a sponsor were most consistently associated with abstinence (Zemore et al., 2013). For drug-dependent individuals, ongoing participation in Narcotics Anonymous (NA) is also associated with abstinence and increases in psychological well-being (DeLucia et al., 2016). Participation in AA is beneficial for individuals with drug, not only alcohol, disorders, suggesting that referral to AA is appropriate for people who use drugs (Kelly et al., 2014).
Individuals who use cannabis may not identify as having a drug problem, and therefore may not self-refer to 12-step programs. This may be increasingly true with the legalization of cannabis in some states of the United States. However, participation in 12-step programs is beneficial among people who use cannabis. In a 5-year study of people who used cannabis, more attendance at 12-step meetings in the 3 months prior to each follow-up (1, 2, and 5 years) was associated with higher rates of abstinence from cannabis (Bonn-Miller et al., 2011). In addition, 12-step program participation at the 1-year follow-up was associated with higher abstinence rates at the 5-year follow-up. These findings suggest that 12-step program participation is associated with both short- and long-term rates of cannabis abstinence.
Older Adults’ Use of 12-Step Programs
The majority of research on older adults’ use of 12-step programs has focused on alcohol use rather than use of cannabis or illicit drugs. In a 9-year study of patterns of AA use, participants over age 40 with drug and alcohol problems were more likely than younger participants to discontinue use early or decrease use of AA over time, and were less likely to have consistently high participation or increased use of AA over time (Witbrodt et al., 2012). In a qualitative study, Holland et al. (2016) found that adults age 50 and older with a history of substance use were concerned about attending treatment group settings that potentially included a wide age range of patients. This suggests that some 12-step programs may not be seen as a good fit by older adults due to the heterogeneity of group members’ ages. However, when older adults do attend 12-step programs, they appear to benefit from participation. In a 20-year study of adults ages 55 to 65 with alcohol problems, obtaining help from 12-step programs was associated with improved alcohol outcomes at 10- and 20-year follow-ups (Moos et al., 2010).
Current Study
Although research suggests that participation in 12-step programs is beneficial for people who use cannabis (Bonn-Miller et al., 2011), and that adults 50 and older benefit from participation in 12-step programs (Moos et al., 2010), research is needed to determine whether these findings hold for older adults with CUD. The current study analyzed 12-step program participation and drug use outcomes among older adults with CUD over the course of a 6-month study of patients who received medical management of their alcohol and/or opioid withdrawal. Multiple aspects of participation in 12-step programs were examined including readiness to attend meetings, number of meetings attended, number of steps worked, and an index of overall involvement. CUD was focused on in this sample given the increased legalization and acceptance of cannabis, and the rising use of cannabis among older adults. Understanding whether and how older adults with CUD engage in 12-step programs, and the extent to which they benefit from doing so, is important for service providers.
The study’s primary questions were whether (a) 12-step program participation and CUD at baseline were associated with cannabis and other drug use at follow-ups, (b) 12-step program participation changed from baseline to the 6-month follow-up, and (c) participants with or without CUD differed on changes in cannabis and drug use, and 12-step program participation, over the 6-month follow-up. Specific hypotheses were not formulated due to the limited guidance from research on these questions.
Method
Participants
The current study analyzed data from a study of Veterans Affairs (VA) patients who received medical management for alcohol and/or opioid use withdrawal and were randomized to receive enhanced telephone monitoring or usual care post-discharge (Timko et al., 2019). The current study was of the older adult participants, defined as age 50 or older (n = 171). Participants were assessed at baseline (at entrance to the treatment episode) and at 3 and 6 months post-baseline. To be eligible for the study, participants were able to correctly answer the Orientation section of the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005), had access to a cell or land line telephone following discharge, and provided the name of at least one person who would know their whereabouts after discharge. Participants’ demographic characteristics at baseline are presented in Table 1.
Baseline Demographics for Older Adult Sample (Age 50 or Older) and by Diagnostic Group.
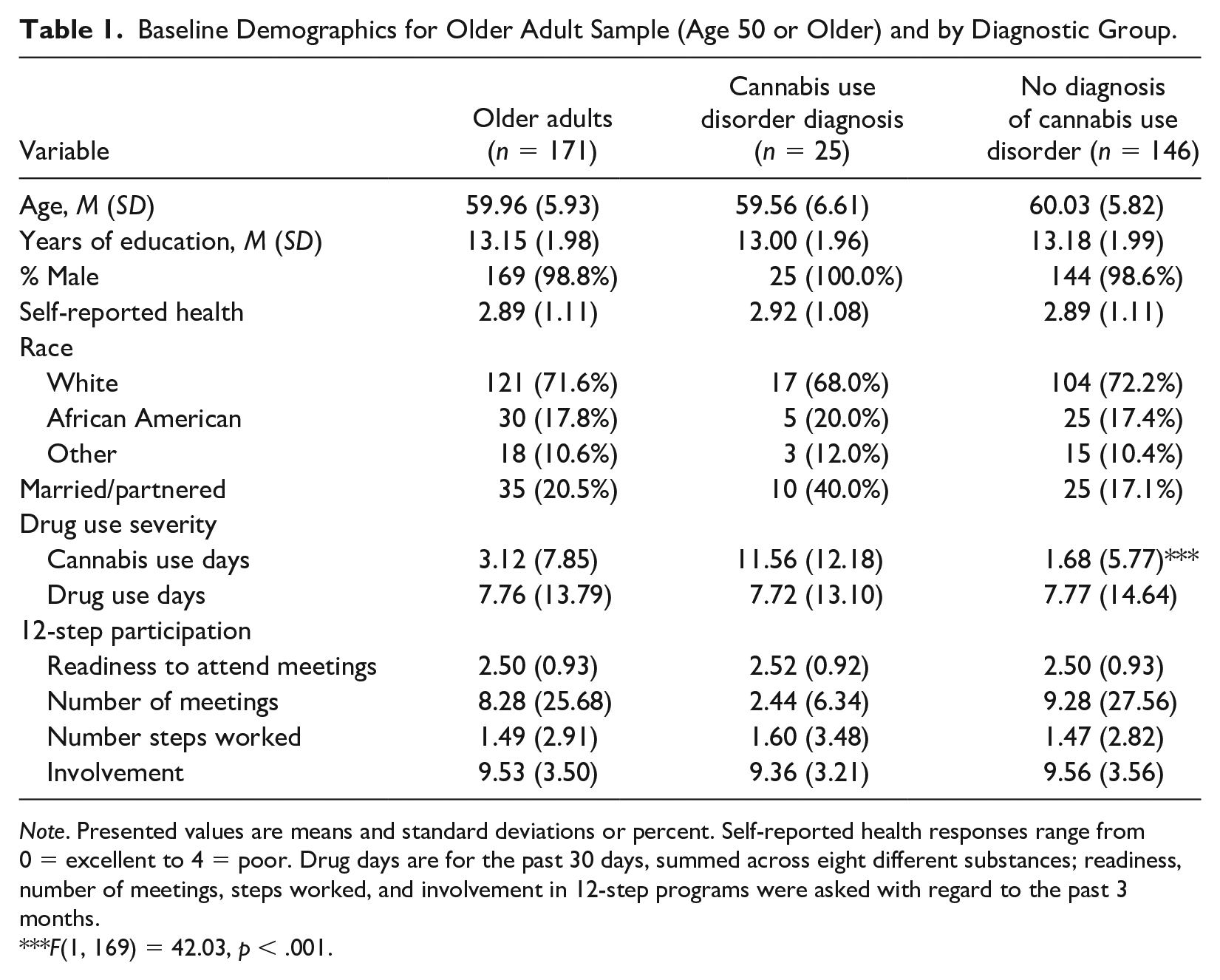
Note. Presented values are means and standard deviations or percent. Self-reported health responses range from0 = excellent to 4 = poor. Drug days are for the past 30 days, summed across eight different substances; readiness, number of meetings, steps worked, and involvement in 12-step programs were asked with regard to the past 3 months.
F(1, 169) = 42.03, p < .001.
Procedure
All study procedures were approved by the VA Central Institutional Review Board. After receiving an introduction to the study, eligible participants who agreed signed an informed consent form. Patients who provided informed consent completed the baseline interview. For the follow-up assessments, a research assistant collected self-report data from patients by telephone at 3 and 6 months post-baseline. Regarding retention rates, 157 participants were followed at 3 months (91.8% of those still alive and not incapacitated) and 158 participants were followed at 6 months (92.4% of those still alive and not incapacitated). Baseline comparisons on demographic characteristics of patients followed or not followed at 3 and 6 months post-baseline found no significant differences.
Measures
Demographic information
Demographic information was collected at baseline and at each follow-up interview.
Drug use
Drug use was assessed at baseline and both follow-ups using items from the Addiction Severity Index (ASI; McLellan et al., 2006; Table 1): (a) number of days in the past 30 that the participant used cannabis (termed “cannabis use days”) and (b) the sum of the number of days in the past 30 that the participant used eight substances, not including cannabis (e.g., sedatives; termed “drug use days”). Diagnosis of CUD was determined at baseline by medical chart review.
Twelve-step program participation
At baseline and all follow-ups, 12-step program participation was measured with items adapted from the Alcoholics Anonymous Involvement scale (AAI; Tonigan et al., 1996) and the Alcoholics Anonymous Affiliation Scale (Humphreys et al., 1998). Questions asked about number of 12-step meetings attended in the past 3 months, readiness to attend 12-step meetings at least once a week for the next 3 months (1 = “Not ready to do” to 4 = “Already doing”), total number of steps worked (out of 12), and involvement (see Table 1). Specifically, the total involvement score was the sum of 12 yes (=1) or no (=0) items about engaging in 12-step practices (e.g., read 12-step literature, had a sponsor, shared honestly at meetings).
Analysis Plan
The primary independent variable was the presence of CUD at baseline. The dependent variables were cannabis and drug use days, and four indices related to 12-step participation (readiness to attend meetings, number of meetings in the past 3 months, number of steps worked, and involvement) at follow-ups.
First examined was whether the diagnostic groups (CUD vs. no CUD) differed significantly on the dependent variables at baseline or on any key demographic variables. One-way ANOVAs were used for this analysis. Next examined was whether 12-step program participation and diagnostic group at baseline (CUD vs. no CUD) were associated with cannabis use days and drug use days at follow-ups. Generalized estimating equations (GEEs) were conducted with the independent variables of 12-step participation, diagnostic group, and time point (baseline and 3- and 6-month follow-up), statistically adjusting for condition (i.e., usual care or enhanced telephone monitoring), and race (White vs. non-White). Race was included as a covariate due to its significant association with substance use outcomes (Evans et al., 2017). Dependent variables were cannabis and drug use days. 12-step participation included the clinically meaningful indicators of number of meetings attended and overall involvement. All four indices of 12-step participation could not be included in the GEE analysis due to their high multicollinearity.
The next set of analyses examined whether diagnostic group at baseline was associated with 12-step participation at follow-ups. GEEs were conducted with the independent variables of diagnostic group and time (baseline and 3- and 6-month follow-up), statistically adjusting for condition and race. Dependent variables were the four indices of 12-step participation (readiness, number of meetings, total number of steps worked, and overall involvement).
An autoregressive correlation structure was specified in the GEEs, which assumes that measurements are less correlated the farther apart they are in time. The models included a continuous time variable that specified when each data point was collected; specifically, time was operationalized as 1 to 3, corresponding to the baseline interview and the two follow-ups, respectively. SPSS was used for all analyses and results are reported in Tables 1, 2, and 3.
Results of GEEs: Association of Cannabis Use Disorder and 12-Step Participation With Cannabis and Drug Use Days.
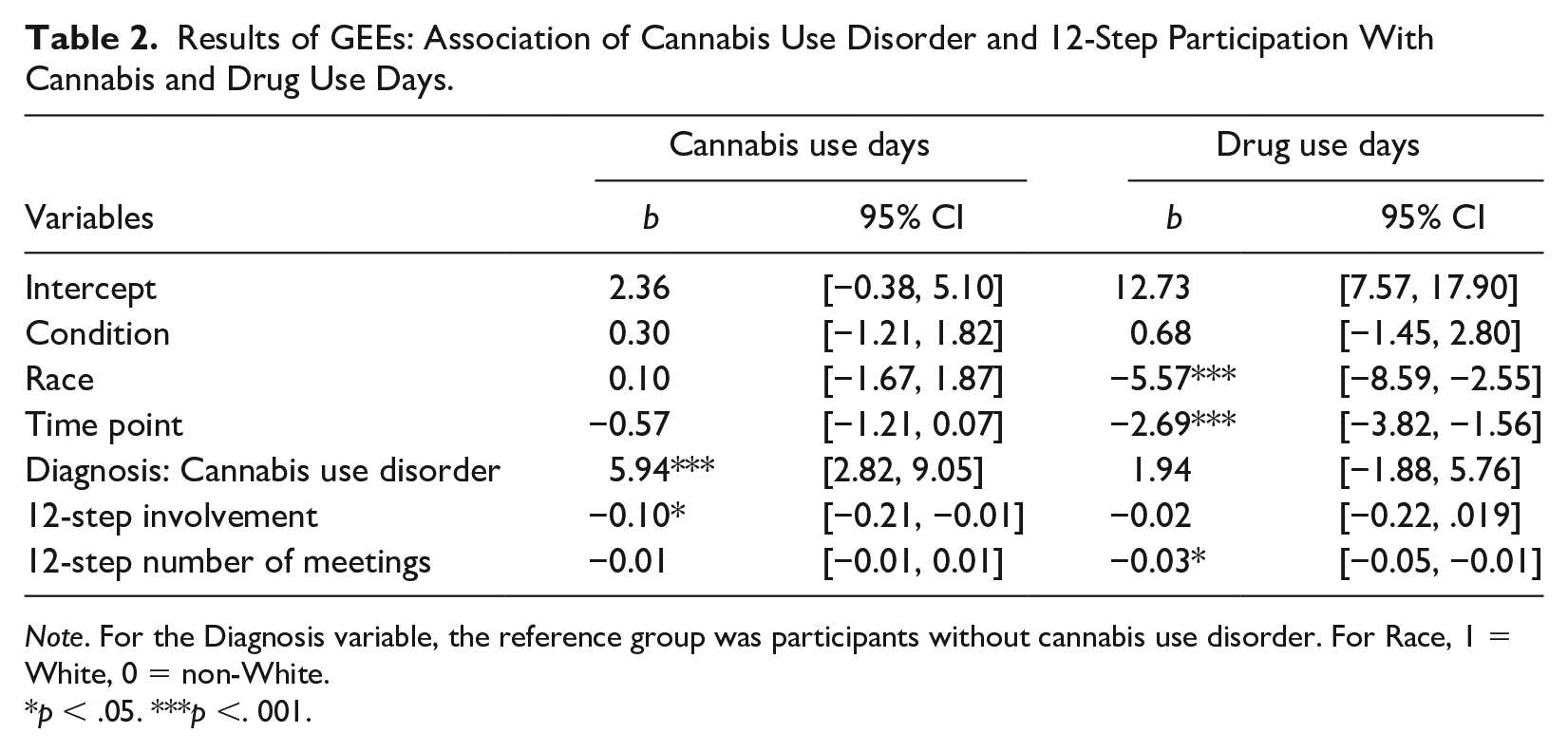
Note. For the Diagnosis variable, the reference group was participants without cannabis use disorder. For Race, 1 = White, 0 = non-White.
p < .05. ***p <. 001.
Results of GEEs: Association of Cannabis Use Disorder With 12-Step Participation Outcomes.
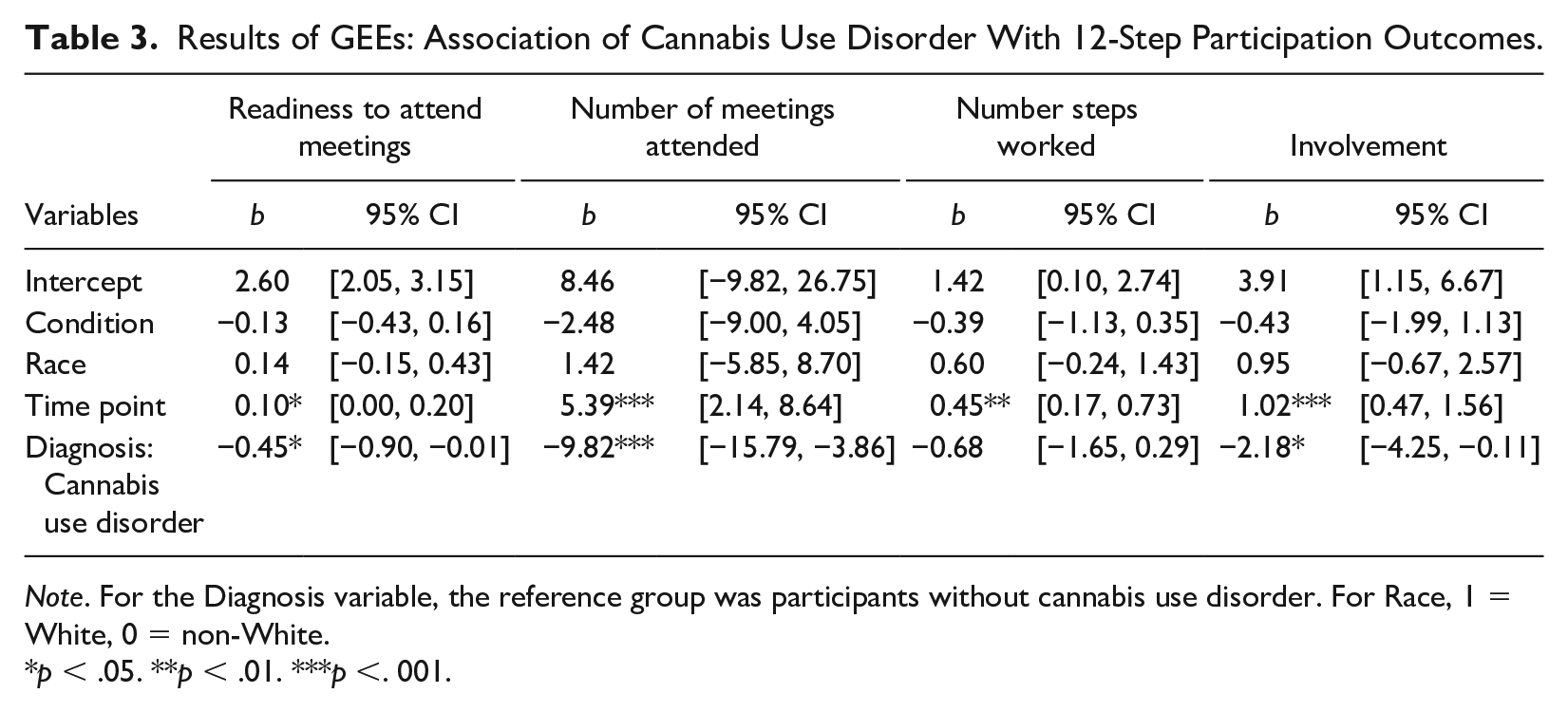
Note. For the Diagnosis variable, the reference group was participants without cannabis use disorder. For Race, 1 = White, 0 = non-White.
p < .05. **p < .01. ***p <. 001.
Results
Baseline Characteristics
As expected, at baseline, participants with CUD reported significantly more days of cannabis use in the past month (Table 1) than the group that was not diagnosed with CUD. The diagnostic groups did not differ significantly on any baseline demographic characteristics, 12-step program participation, or drug use days.
Associations of Diagnostic Group and 12-Step Program Participation With Cannabis and Drug Use
First examined was whether diagnostic group (CUD vs. no CUD) and 12-step program participation were associated with the outcome of cannabis use days while also considering time point, participant race, and condition. The nonsignificant effect for time point on cannabis use days showed that cannabis use days in the past month did not change from baseline through the 6-month follow-up (Table 2). Compared with participants without CUD, participants with CUD reported having used cannabis on more days in the past month from baseline through the 6-month follow-up. More 12-step involvement was associated with fewer cannabis use days from baseline through the 6-month follow-up.
Next examined was the outcome of drug use days, with results also noted in Table 2. For the covariate of race, participants who were not White reported more drug use days than White participants. The effect for time point was significant, showing that drug use days decreased from baseline through the 6-month follow-up. Participants with CUD did not differ on drug use days from those without CUD. Attending more 12-step meetings was associated with fewer drug use days from baseline through the 6-month follow-up.
Association of Diagnostic Group With 12-Step Participation
GEE analyses also examined whether diagnostic group was associated with four indices of 12-step participation (Table 3). For readiness to attend meetings, time point was significant such that readiness to attend meetings increased from baseline through the 6-month follow-up. Participants with CUD at baseline reported lower readiness to attend meetings from baseline through the 6-month follow-up than those without CUD.
For number of meetings, time point was significant such that number of meetings attended increased from baseline through the 6-month follow-up. Participants with CUD at baseline reported attending fewer meetings from baseline through 6 months than those without CUD.
For number of steps worked, time point was a significant predictor, indicating that participants reported an increase in the number of steps they worked from baseline through the 6-month follow-up. The effect of diagnostic group on number of steps worked was not significant.
For the outcome of involvement, time point was significant such that involvement in 12-step programs increased from baseline through the 6-month follow-up. In addition, participants with CUD reported less involvement in 12-step groups from baseline through the 6-month follow-up than those without CUD.
Discussion
The current study found that, among a sample of patients age 50 and older who received medical management of substance use withdrawal, participation in 12-step programs generally increased from baseline to the 6-month follow-up, drug use days decreased, and cannabis use remained stable. More 12-step program participation was associated with fewer cannabis and drug use days. Patients with CUD at baseline attended fewer 12-step program meetings, reported less readiness to attend 12-step meetings, and had lower involvement in 12-step programs at follow-ups, compared with patients who did not have CUD at baseline. It is particularly useful to service providers to identify groups at increased risk of negative outcomes. The results from the current study suggest that participants benefited from 12-step participation, but that older adults with CUD may need either additional facilitation to attend 12-step programs or alternative treatment options as they were less likely to attend 12-step programs than those without a CUD diagnosis.
Longitudinal Results
The finding that cannabis use did not change significantly for the sample overall is consistent with existing research on adult populations that found low abstinence rates for cannabis following treatment (Sherman & McRae-Clark, 2016). The finding may also reflect the increasing acceptance of cannabis and the perception that it is not a “hard” drug, which may lead to fewer efforts to reduce cannabis use. It is interesting to note that, in this study of adults age 50 and over, participation in 12-step programs increased significantly over the 6 months after withdrawal management services were received. Increased use of 12-step programs could be related to participants’ relatively high-severity substance use at baseline. However, the increase in 12-step program participation also suggests that older adults will engage with 12-step programs and become involved beyond simply attending meetings. This is an important finding, as older adults have reported reservations about mixed-age treatment settings and tend to participate less in 12-step programs compared with other age groups (Holland et al., 2016; Sacco et al., 2013; Witbrodt et al., 2012).
Participation in 12-step programs was beneficial in reducing cannabis and other drug use over the 6 months of follow-up. Research on the active ingredients of 12-step programs suggests that facilitation of adaptive social network changes is one of the primary mechanisms of reduced substance use, as well as improved ability to manage negative affect without using drugs (Kelly, 2017). Although the current study asked specifically about 12-step programs, other mutual-help group options (e.g., LifeRing, SMART Recovery) are available and may be helpful for individuals who are reluctant to attend 12-step programs due to their abstinence-based goals and spiritual focus (Zemore et al., 2017, 2018). For those older adults who are not yet ready to engage in a mutual-help group, brief motivational approaches may be appropriate (Barry & Blow, 2016).
Results by Diagnostic Category
A CUD diagnosis was associated with more cannabis use days and less 12-step program participation. These results suggest that older adults who have CUD are a high-risk group, in that they are less likely to participate in 12-step programs, and have higher cannabis use, than those without CUD, even after having recently completed a detoxification program. Older adults who have CUD may not seek out services because they tend to use cannabis to manage medical conditions (Haug et al., 2017). Because cannabis is considered a benign drug with higher social acceptability, there is not a clear consensus on whether treatment goals should be focused on abstinence or harm reduction, especially because most people who use cannabis are more likely to have reduction goals than abstinence goals (Hughes et al., 2016). This has led to an increase in studies on harm-reduction approaches to cannabis use (Askew, 2016; Lau et al., 2015a). In a study of older adults who used cannabis, several harm-reduction strategies were noted, such as changing the route of administration and controlling cannabis use through smaller doses and lower frequency (Lau et al., 2015b).
Considering the wide availability of 12-step programs, and the generally positive outcomes seen among attendees, service providers should consider facilitating attendance at 12-step programs for older adults who have CUD. However, it is also possible that different treatment modalities need to be offered to this age group beyond 12-step programs. Psychological treatments for CUD focus on behavioral therapies such as contingency management, relapse prevention, motivational interviewing, and other cognitive-behavioral techniques (Davis et al., 2015). In a meta-analysis of behavioral treatments for CUD, participants who received behavioral treatments had better drug use outcomes (lower frequency and severity) than participants in control conditions (Davis et al., 2015). Although the results of psychological interventions for CUD are promising, there is a need for studies on interventions for older adults who use cannabis.
Limitations
One limitation of the current study was that participants were all veterans, mostly male and White, and from one health care system, the VA. Systematic reviews indicate that VA-provided health care is similar to that provided in non-VA settings (Anhang Price et al., 2018; O’Hanlon et al., 2017) but studies of older persons using cannabis, including those diagnosed with CUD, should be conducted in other health care systems. The findings may not generalize to studies in which older adults are identified using other age requirements than the one used in this and other studies of substance use; for example, age 65 is a common age cutoff used to identify older adults in other fields of research (American Psychological Association, 2014). Furthermore, in the present study, substance use was based on self-report. Although substance use was assessed by trained staff using valid and reliable procedures and instruments to minimize bias and help recall, and the validity of substance use self-reports has been supported (Napper et al., 2010), additional sources of information on patients’ substance use, such as collateral reports, could be helpful.
Conclusions
In this 6-month study of older adults treated for alcohol and/or opioid dependence, 12-step program participation was beneficial in reducing cannabis and other drug use. However, participants with CUD reported higher use of cannabis and lower participation in 12-step programs. Although cannabis use is becoming more accepted, treatment rates for CUD are low and cannabis use continues to be associated with negative medical, mental health, and psychosocial outcomes among older adults (Choi et al., 2018; Choi, DiNitto, & Marti, 2016; Lee et al., 2019; Volkow et al., 2016). In light of the findings, older adults with CUD should be identified as a high-risk group in need of targeted and personalized treatment approaches. Tailored approaches that facilitate 12-step participation or treat cannabis use may be needed for older adults with CUDs. Effective psychosocial treatments for CUD include a combination of cognitive-behavioral therapy, motivational enhancement therapy, and contingency management. Although these treatments have not been examined specifically among older adults, a modular and individualized approach to CUD treatment among older adults may assist in improving treatment outcomes for this group, particularly in light of their low use of 12-step programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Department of Veterans Affairs (VA), Health Services Research and Development (HSR&D) Service (CRE 12-010 and RCS 00-001 to Dr. Timko).