
Abstract
Given the rapidly changing U.S. cannabis legislation landscape, the aim of this article is to describe individuals who self-reported growing cannabis in the past year by selected characteristics and geographical location. Using data from 2010 to 2014 National Survey on Drug Use and Health, we conducted bivariate chi-square tests and ran a multivariable logistic regression model to examine the indicators associated with growing cannabis. Approximately, 484,000 individuals aged 12+ self-reported growing cannabis in the past year (1.6% of marijuana users). Predictors of growing cannabis included being male and self-reported reporting using cannabis for a greater number of days. Data showed differences in the proportion of cannabis growers by the state of residence. Obtaining a baseline estimate of cannabis growing practices prior to recreational cannabis markets emerging (2014) is important because such practices may undermine efforts to discourage diversion to youth. Tracking these acquisition patterns will better inform content for public health messaging and prevention education, particularly those targeting youth.
Introduction
Since 1996, 32 U.S. states and the District of Columbia have allowed the use of cannabis for medical reasons (Law Atlas Project, Temple University Beasley School of Law, 2017; National Conference of State Legislatures, 2019). Although many scholars have considered the impact of these policies in terms of their potential benefits and harms (Anderson et al., 2013; Caulkins et al., 2015, 2016; Cerdá et al., 2020; Kilmer, 2019; McGinty et al., 2016; Sabia & Nguyen, 2018; Shover & Humphreys, 2019), one area receiving considerably less attention is the impact of these liberalization policies on personal cannabis cultivation. Personal cannabis cultivation could be valuable as an alternative source of supply for some individuals and/or patients, as it enables consumers to avoid paying higher prices for these products and allows consumers to generate strains and/or oils with unique mixes of natural cannabinoids well-suited for their purposes. Moreover, home cultivation when adopted as the sole supply strategy (as in Washington D.C. and Vermont) helps limit the role of a commercialized industry trying to market its products to would-be consumers. Taxes in such a market could still be obtained if based on the seedlings and/or plants sold to individuals for their home cultivation (similar to the way people buy seeds or seedlings from the nursery to grow tomatoes). There are potential downsides to home cultivation, however, as it might facilitate direct access to minors in the home and enable diversion to black markets, particularly if large quantities of cannabis plants are allowed to be grown at home. In addition, home cultivation may have unregulated standards compared to those in the commercialized industry.
As of February 2017, 15 U.S. states provided legal protection to patients who cultivate their own cannabis for medicinal purposes (Klieger et al., 2017). With legalization of recreational or nonmedical use of cannabis in nine U.S. states, further permissions to cultivate cannabis for individual use were granted to all adult residents in nearly every legalizing state (National Conference of State Legislatures, 2019). Washington State is the only legalizing state that limits nonmedical cannabis growing to licensed cultivation businesses. Despite the increasing prevalence of legal permissions granted to residents in these states, very little is known about the extent to which people rely on cannabis self-growing practices. Data from the Substance Abuse and Mental Health Services Administration’s (n.d.) National Survey on Drug Use and Health (NSDUH) show that the prevalence of individuals aged 12 and older self-reporting growing cannabis increased from 0.6% in 2002 to 2.4% in 2013, before dropping back to 1.2% or approximately 400,000 individuals in 2014 (Azofeifa et al., 2016). Thus, cannabis cultivation for self-use clearly remained a relatively infrequent event during a period when state laws only allowed it for medicinal purposes but it rose dramatically until retail stores began to open in 2014.
At the end of the 1980’s, there were an estimated 250,000 individuals in the United States involved in the commercial cultivation of cannabis (Weisheit, 1992), but since then only a few web-based surveys drawing on convenience samples through social media have been used to generate information about cannabis cultivation among commercial growers (Potter et al., 2015) and/or regular cannabis users (Borodovsky & Budney, 2017; Caulkins et al., 2020). While these web-based surveys are valuable, it is unclear the extent to which the populations captured in these web surveys are hidden from general households that are surveyed more regularly.
In this article, we examine the characteristics of individuals who report using cannabis in the past year and growing it themselves from 2010 to 2014 NSDUH. In doing so, we identify the characteristics of individuals who are engaging in self-growing practices and, therefore, provide the first description of self-identified cannabis growers in households and thus are able to look at geographic differences in growing propensities across states. These data were selected deliberately to provide important baseline estimates, pre-legalization time period of recreational cannabis sales in the United States (2014), to understand future changes in the U.S. self-growing cannabis market.
Materials and Method
Data Source: NSDUH
NSDUH collects annual information about the use of illicit drugs, alcohol, and tobacco among the noninstitutionalized U.S. civilian population aged 12 and older via household face-to-face interviews, using a computer-assisted personal interviewing system (Center for Behavioral Health Statistics and Quality [CBHSQ], 2014b). NSDUH uses a multistage area probability sample design for each of the 50 states and the District of Columbia that allows the production of representative national and state-level estimates. NSDUH data are protected under the Confidential Information Protection and Statistical Efficiency Act of 2002, which ensures that all data are used for statistical purposes only and cannot be used for any other purposes. Detailed information regarding NSDUH methodology and questionnaires is available elsewhere (CBHSQ, 2014a, 2014b). The present study used combined data from NSDUH’s from years 2010 to 2014 to produce annual average estimates of pre-legalization time period of recreational cannabis use and cultivation among the U.S. household population.
Sample
The analytic sample includes respondents aged 12 years and older who self-reported using marijuana in the past year. The term “marijuana” is used in this section only to reflect NSDUH’s original terminology. Otherwise, the term “cannabis” will be used throughout this report. From 2010 to 2014, NSDUH data were collected from approximately 62,100 individual respondent interviews per year (unweighted), with this analysis focusing on those who self-reported using marijuana in the past year. The analytic weighted sample of past-year marijuana users was approximately 25% aged 12 to 20 (7,692,000) and 75% aged 21 or older (23,430,000), and 60% male (18,828,000) and 40% (12,294,000) female (data not shown). Respondents with unknown information on whether they grew marijuana in the past 12 months were excluded from the analyses (approximately 2.4% [unweighted] or 1.9% [weighted]). This sample was weighted to provide the nationally representative estimates of the national household population.
Measures
Marijuana use was defined in NSDUH as a self-report of using marijuana (“pot” or “grass”) or hashish (“hash”) within the past 12 months preceding the date of the interview. The sequence of NSDUH’s questions began with “How long has it been since you last used marijuana or hashish?” Among those who reported past-year use of marijuana, respondents were then asked: “Now think about the last time you used marijuana. How did you get this marijuana?” Response categories were bought it, traded something else for it, got it for free or shared someone else’s, grew it yourself. Participants who self-reported that they grew marijuana themselves during the last year were considered “marijuana (cannabis) growers” for this analysis. Note that as only past-year marijuana users answered the question regarding cultivation, these responses cannot be viewed as representative of cannabis cultivators. They instead represent a very large sample of individuals who most likely grow for their own purposes.
Demographic Variables
Demographic characteristics assessed included sex, age, race/ethnicity, annual household income, county type, current employment status, and level of education obtained. Selected behavioral characteristics included the number of days the respondent used marijuana in the past year, and meeting Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for marijuana dependence. The full list of NSDUH questions can be found elsewhere (CBHSQ, 2014a).
Statistical Analyses
Statistical analyses were performed using SAS Version 9.4 and SUDAAN Version 11.0.1 (RTI International). Population weights were calibrated through a model-based procedure to adjust for state, age group, sex, and race/ethnicity groupings, and variances were calculated accounting for the complex NSDUH survey design.
Analysis
The percentage of past-year users who self-reported growing marijuana for each category of the selected variables was examined. Tabular distributions of the sociodemographic and selected behavioral characteristics of marijuana users were contrasted by growing status (yes/no) using chi-square tests at α = .05 (Table 1). Next, all the characteristics of interest were included in a multivariable logistic regression model to identify the predictors of having reported growing marijuana at least once among past-year marijuana users, while controlling for the effects of other variables in the model (Table 2). We ran separate models for underage (12–20 years) and adults (21 and older) to understand unlawful practices among minors. Adjusted odds ratios (AOR) greater than one indicated that the indicator was associated with an increased likelihood of growing marijuana relative to the reference group, and an AOR less than one indicated that the indicator was associated with a decreased likelihood of growing marijuana relative to the reference group. We present the 95% confidence interval (CI) for each AOR estimate. We also described the number (in 1,000s) and percentage of those reporting past-year marijuana use for whom marijuana was recommended by a doctor from selected and available survey years from 2013 to 2014 (Table 3).
Percentage of Past-Year Cannabis Users Aged 12 and Older Who Self-Reported Growing Cannabis By Selected Demographic Characteristics—National Survey on Drug Use and Health, United States, 2010–2014.
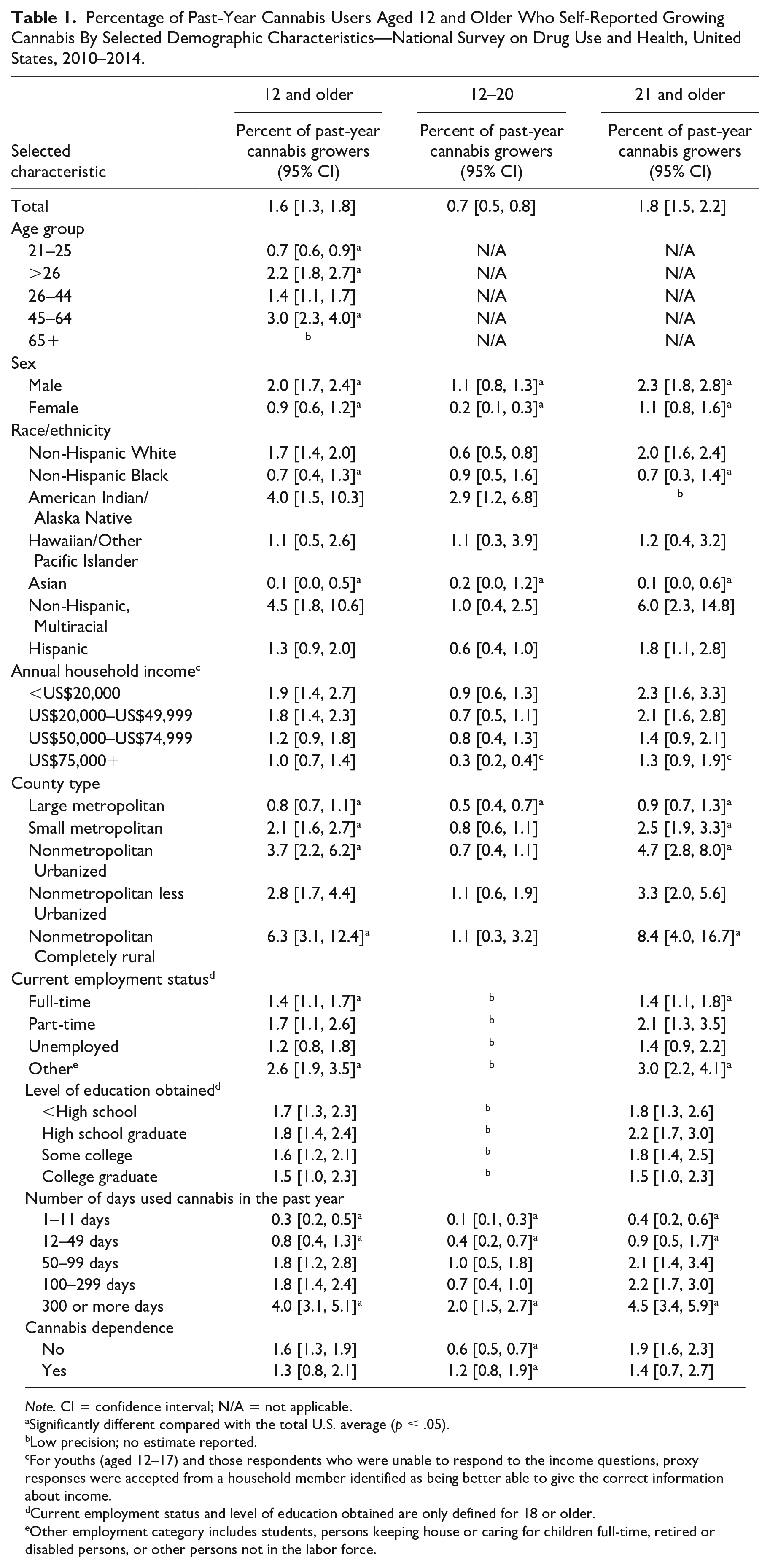
Note. CI = confidence interval; N/A = not applicable.
Significantly different compared with the total U.S. average (p ≤ .05).
Low precision; no estimate reported.
For youths (aged 12–17) and those respondents who were unable to respond to the income questions, proxy responses were accepted from a household member identified as being better able to give the correct information about income.
Current employment status and level of education obtained are only defined for 18 or older.
Other employment category includes students, persons keeping house or caring for children full-time, retired or disabled persons, or other persons not in the labor force.
Adjusted Odds Ratios Predicting Growing Cannabis Among Past-Year Cannabis Users Aged 12 and Older by Selected Demographic Characteristics—National Survey on Drug Use and Health, United States, 2010–2014.
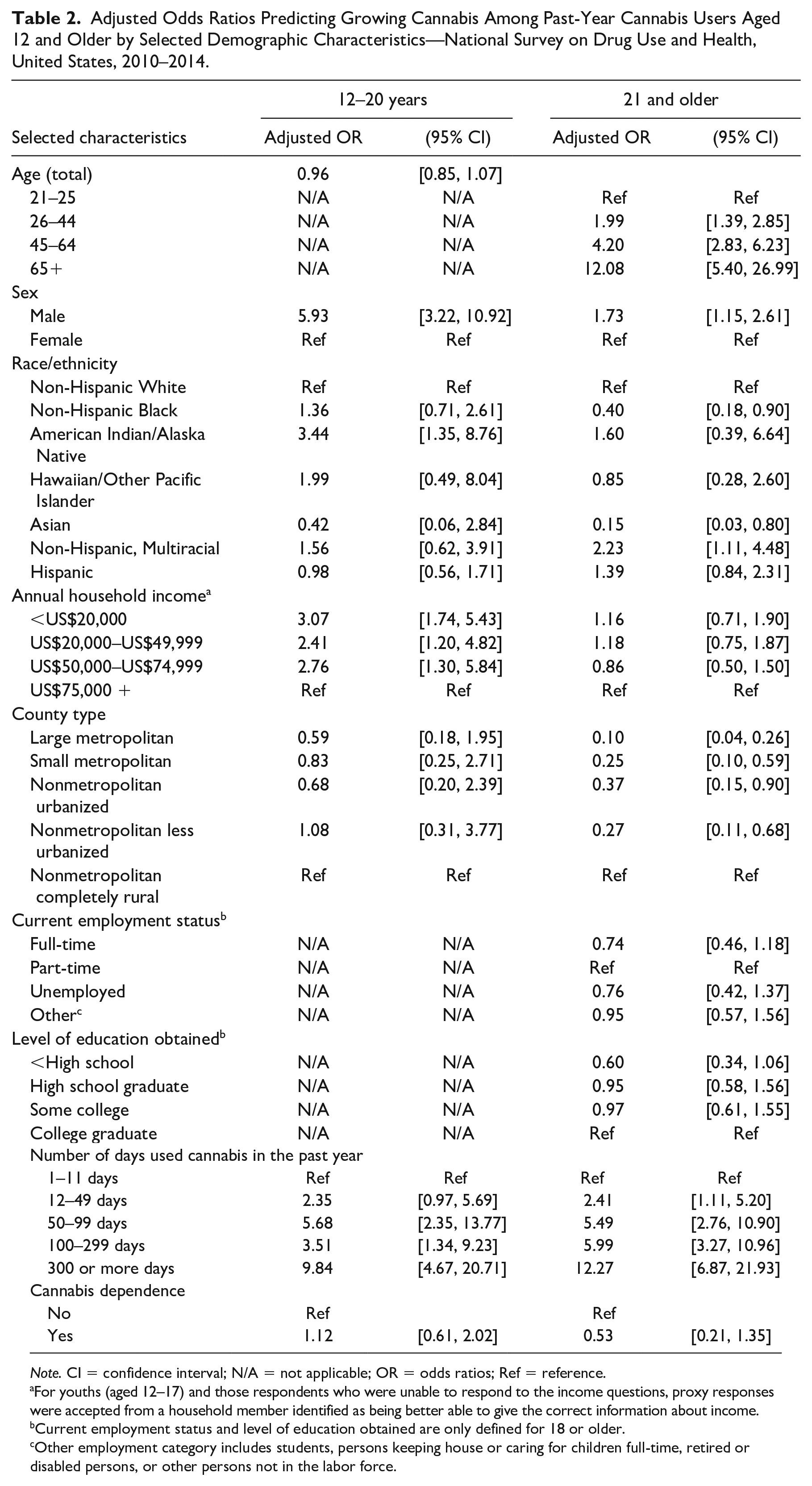
Note. CI = confidence interval; N/A = not applicable; OR = odds ratios; Ref = reference.
For youths (aged 12–17) and those respondents who were unable to respond to the income questions, proxy responses were accepted from a household member identified as being better able to give the correct information about income.
Current employment status and level of education obtained are only defined for 18 or older.
Other employment category includes students, persons keeping house or caring for children full-time, retired or disabled persons, or other persons not in the labor force.
Number (in 1,000s) and Percentage of Past-Year Cannabis Users aged 12 and Older Who Self-Reported Any or All of Past-Year Marijuana Use Being Recommended by a Doctor by Source of Last Marijuana Use—National Survey on Drug Use and Health, United States, 2013–2014.
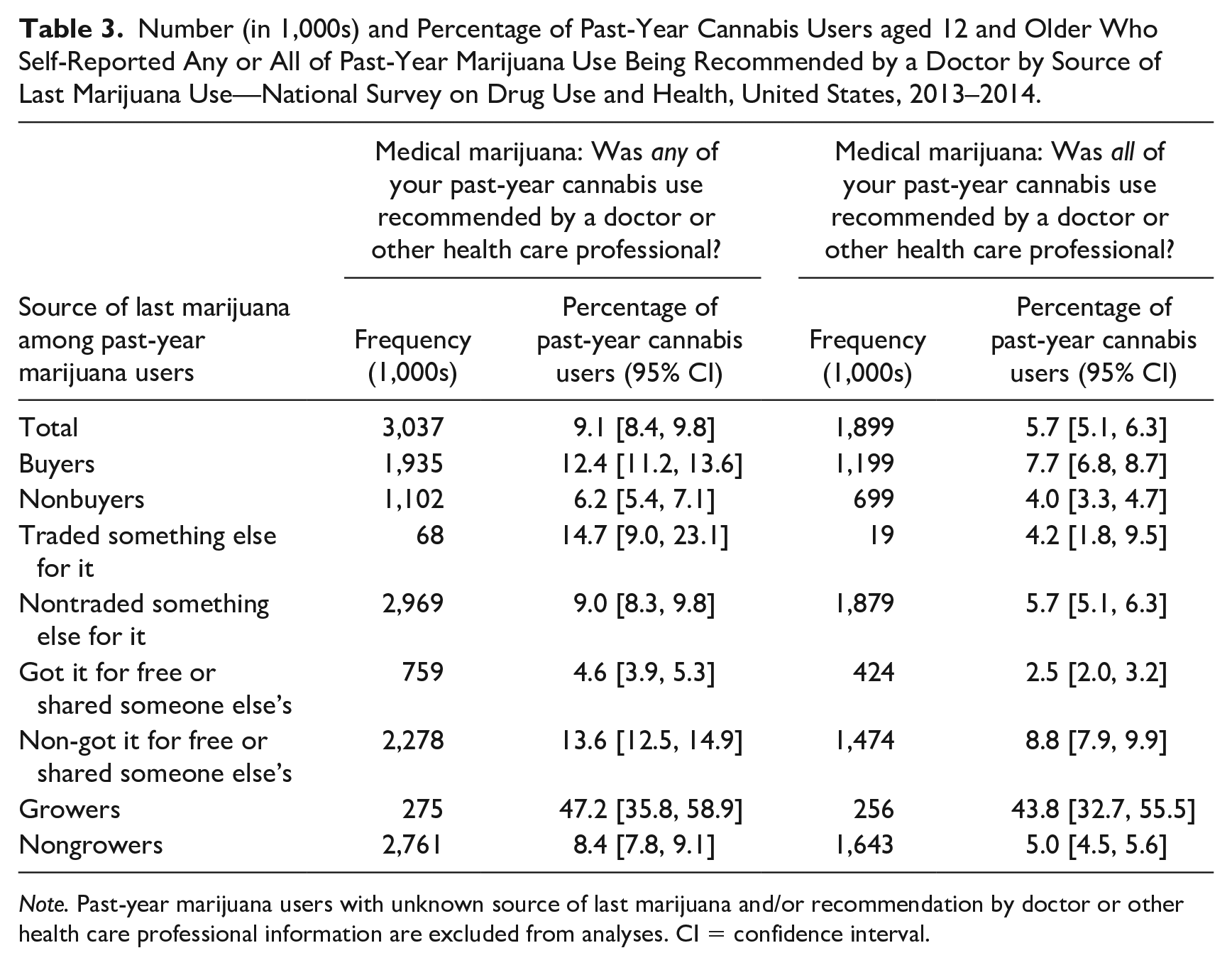
Note. Past-year marijuana users with unknown source of last marijuana and/or recommendation by doctor or other health care professional information are excluded from analyses. CI = confidence interval.
Finally, we produced state estimates to quantify the percentage of all people aged 12 and older, who self-reported growing marijuana in the past year among marijuana users by state of residence (Figure 1). State-level estimates were compared with the U.S. national average (1.6%) using α = .05 level as a cutoff to determine statistical significance. States were ordered by the existing or effective (pre, during, or none) state medical cannabis law as described in Law Atlas Project, Temple University Beasley School of Law (2017).
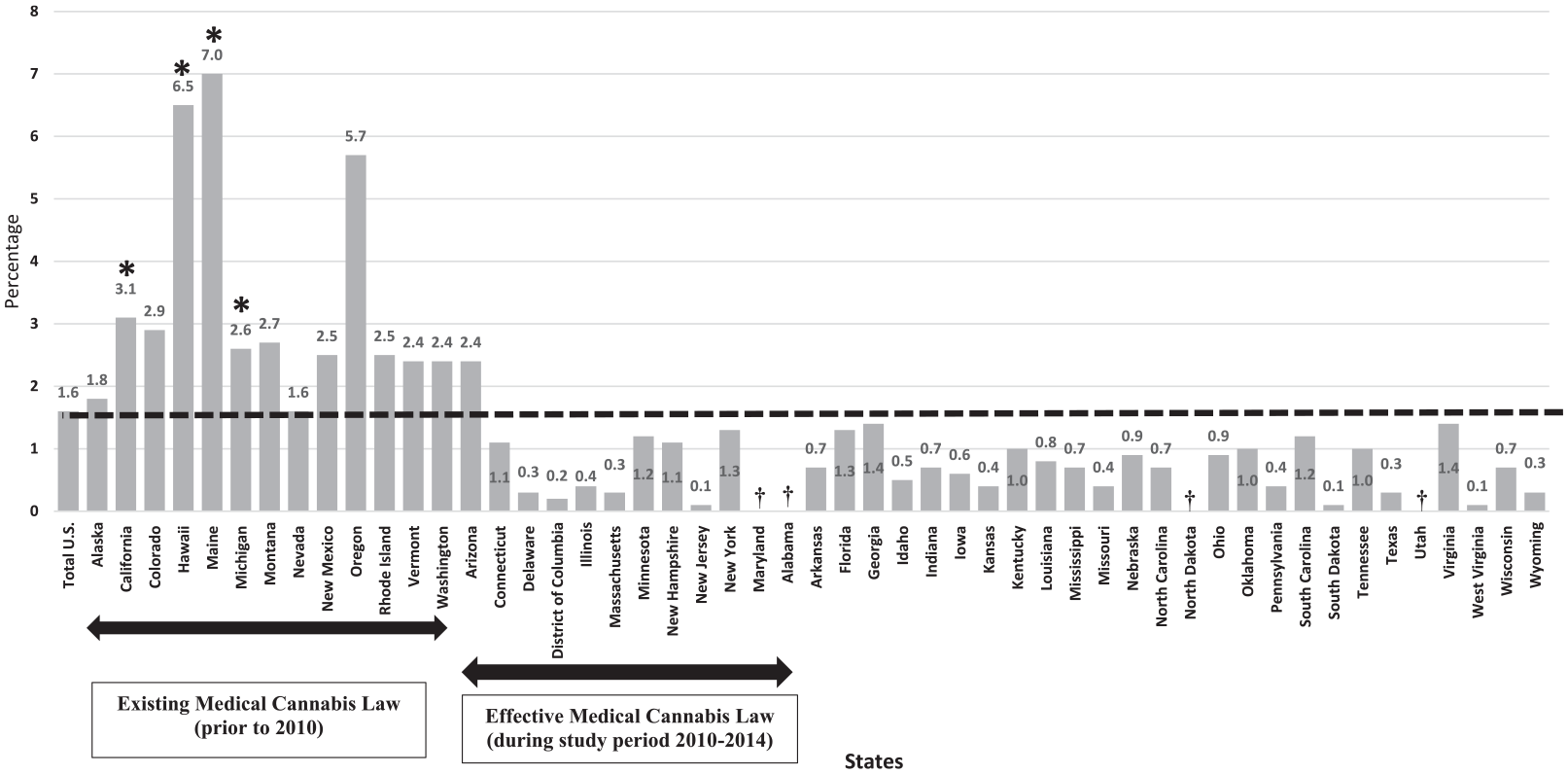
Percentage of past-year cannabis users who self-reported growing cannabis among persons aged 12 and older by state of residence and ordered by the existing or effective state medical cannabis law—National Survey on Drug Use and Health, United States, 2010–2014.
Results
National-Level Results
During 2010–2014, there was a total estimate of approximately 484,000 past-year cannabis users aged 12 and older (1.6%) who self-reported growing cannabis, which includes an estimated 51,000 (0.7%) individuals aged 12 to 20 and an estimated 433,000 (1.8%) individuals aged 21 and older. Table 1 depicts the selected demographic characteristics and behavioral indicators of cannabis users who reported growing cannabis in the past year and indicates self-reports of growing cannabis was significantly higher (p ≤ .05) among males (2.0%, CI = [1.7, 2.4]), individuals aged 45 to 64 (3.0%, CI = [2.3, 4.0]), those who reside in rural areas (6.3%, CI = [3.1, 12.4]), those who reported having “other” employment status (2.6%, CI = [1.9, 3.5]), and among those who reported using cannabis for >300 days in the past year (4.0%, CI = [3.1, 5.1]) compared with the national average (1.6%, CI = [1.3–1.8]). Indicators for the level of education attained and cannabis dependence were not significantly associated with reporting self-growing cannabis among past-year cannabis users.
Individual-Level Results
Table 2 shows the multivariable correlates of self-reported growing cannabis in the past year among cannabis users aged 12 to 20 years and 21 and older. Among those aged 12 to 20 years, predictors of growing cannabis included, being male (AOR = 5.93, CI = [3.22, 10.92]), being American Indian/Alaskan Native (AOR = 3.44, CI = [1.35, 8.76]), living in a household with an income less US$20,000 (AOR = 3.07, CI = [1.74, 5.43]), and using cannabis for a greater number of days in the past year (e.g., those who reported 300 or more days used in past year [AOR = 9.84, CI = [4.67, 20.71]]).
Among those aged 21 or older, predictors of growing marijuana included being male (AOR = 1.73, CI = [1.15, 2.61]), being an adult aged 65 and older (AOR = 12.08, CI = [5.40, 26.99]), being a non-Hispanic, multiracial ethnicity (AOR = 2.23, CI = [1.11, 4.48]), and using marijuana for a greater number of days in the past year (e.g., those who reported 300 or more days used in past year [AOR = 12.27, CI = [6.87, 21.93]]).
State-Level Results
Figure 1 illustrates the state-level percentages of cannabis users aged 12 and older who self-reported growing cannabis in the past year. States are organized from left to right based on the following: (a) whether the state had a pre-existing medical cannabis law prior to our evaluation period (2010–2014), (b) whether the state had adopted a medical cannabis law during our evaluation period, and (c) whether the state had not adopted a medical cannabis law at all (e.g., Georgia, Iowa, Louisiana, and Kansas) or did so after our evaluation period (e.g., Arkansas, Florida, Pennsylvania, and Ohio). These cannabis state law allocations were based on the existing online databases (Law Atlas Project, Temple University Beasley School of Law, 2017). Four states had a significantly (p < .05) higher percentage of cannabis growers compared with the U.S. average (1.6%): Maine (7.0%, CI = [4.4, 11.1]) with approximately 13,000 individuals, Hawaii (6.5%, CI 4.1–10.3) with approximately 9,000 individuals, California (3.1%, CI = [2.1, 4.6]) with approximately 140,000 individuals and Michigan (2.6%, CI = [1.8, 3.7]) with approximately 31,000 individuals. All four of these states had medical cannabis laws allowing patient cultivation of cannabis that were adopted prior to our evaluation period. Other states with the existing medical cannabis laws also allowing patient cultivation of cannabis (e.g., Alaska, Colorado, Nevada, and New Mexico) did not exhibit significantly higher rates of self-reported growing in our samples.
Discussion
This is the first study providing baseline information, pre-legalization time period of recreational cannabis sales (2014), on cultivation or growing patterns of cannabis among a nationally representative household sample in the United States. Data from this study show that after two decades of state medical cannabis liberalization policies in the United States, cultivation of cannabis nationally remained relatively low, with only 1.6% of self-reported past-year cannabis users (less than half of a million individuals) aged 12 and older self-reporting growing their own cannabis by 2014; however, this national number hides important differences across demographic groups and states.
We found in the NSDUH household survey data that self-reported cultivation rates were lower in virtually all states without a medical cannabis law by 2014 than the national average. States that adopted medical cannabis policies prior to our sample period (2010–2014) generally were found to have self-reported growing prevalence rates above the national average, although only four (California, Hawaii, Maine, and Michigan) were statistically significantly higher than the national average. This finding is consistent with findings from a study that recruited its sample of 1,813 cannabis users online via social media platform—Facebook (Borodovsky & Budney, 2017). Even in these medical cannabis states, rates of home cultivation were in the single digits, suggesting that self-cultivation among cannabis users was just not a very common method of acquisition prior to the adoption of adult-use laws. There are two possible explanations for this. First, medical cannabis users, despite having legal protections to grow their own cannabis, prefer not to do so. Second, medical cannabis users make up a very small proportion of all cannabis users, a finding that has been supported in earlier work using the NSDUH data (Compton et al., 2017).
This study also found that people who chose to grow their own cannabis were more likely to have the following characteristics: male gender, aged 45 to 64, resided in rural areas, and reported using cannabis for >300 days in the past year. While survey methodology and targeted populations differ between NSDUH’s household sample and that of the web-based survey of cannabis users, selected characteristics (e.g., gender, age, cannabis use) were consistent (Potter et al., 2015). Many of these same characteristics held as key predictors of self-reporting growing cannabis in multivariate regressions as well, although it was found in the multivariate analysis that lower annual household income and being of American Indian/Alaskan native descent were positively correlated with youth cultivation (those aged <21), while among adults, it was those from non-Hispanic, multiracial backgrounds that were more likely to report growing their own cannabis.
These data provide an important baseline for understanding the extent to which more recent state policy changes pertaining to recreational cannabis influence the market and cannabis cultivation. In places like Washington D.C. and Vermont, where retail dispensaries for recreational cannabis are not currently allowed, cannabis cultivation represents the only way for nonmedical users to obtain their cannabis outside of black markets. Thus, trends in self-reported cannabis cultivation among residents in these jurisdictions may have risen or are rising following the legalization of nonmedical cannabis (in 2014 for D.C., and 2018 for Vermont). In other states, like California, Colorado, and Maine, it is unclear what to expect with legalization, as recreational users in these states have or will have the option to grow their own or purchase from retail outlets. Purchases from retail outlets will be subject to taxation, however, which may lead some to choose to grow their own cannabis (at a perceived lower cost).
It will be particularly important to continue monitoring the extent to which youth (individuals younger than 21 years of age) engage in cannabis cultivation for personal consumption. The data show that there is a very small group of underage past-year cannabis users (approximately 51,000 individuals) who were already engaging in cannabis cultivation prior to the nonmedical legalization of cannabis in any of these states. Although some of these individuals may have state-issued medical cards, there is no reason to expect that group to grow over time, particularly as more medical cannabis states adopt dispensary systems. Cannabis cultivation by minors may be an important avenue by which youth circumvent policies reducing their access to nonmedical cannabis and thus represents a very important metric to track as states continue to experiment with recreational cannabis laws. Although not done at the national scale, patterns of youth participation in cannabis cultivation have been studied elsewhere (Bouchard et al., 2009; Nguyen & Bouchard, 2010). States that allow adults to grow at home for recreational purposes may make it more feasible for youth to do the same (as it is more difficult to enforce laws pertaining to underage home cultivation than it is to enforce laws pertaining to underage purchases). State public health authorities may want to consider public education campaigns for parents or guardians who grow cannabis in their household to prevent access by youth.
In addition to youth access, monitoring the extent of cannabis cultivation and characterizing cannabis growers is also important to public health, as the products resulting from such growers are unregulated and untested. They may contain contaminants that present household or other exposure issues or may be manufactured into products at home that are high potency (e.g., edibles or concentrates), as described elsewhere (Borodovsky & Budney, 2017; Lenton et al., 2018). Knowledge of who is growing cannabis can provide public health professionals with an idea of who to target for prevention and educational campaigns to protect public health and safety.
Limitations
The findings in this report are subject to several limitations. First, data are self-reported and are subject recall bias for experiences during the past 12 months as well as social desirability bias. Second, NSDUH did not include a question for medical use of cannabis for all survey years; nonetheless, a subset analysis for the years 2013–2014 (Table 3) was included for individuals aged 12 and older. Future NSDUH analyses, when available, will be able to compare U.S. cannabis growers for medical or nonmedical reasons with more robust sample size. Third, NSDUH does not allow us to distinguish lawful and unlawful cannabis growers, or between cannabis home growers versus commercial cannabis growers, which could limit the interpretation of the data. Fourth, given the complexity and heterogeneous nature of the specifics of state cannabis legislation, correlation of cannabis growing patterns by the state was not done in this study. Fifth, the authors could not assess if individuals grew their cannabis indoors or outdoors, limiting our analysis and interpretation of the data. To strengthen future U.S.cannabis growers’ studies, researchers may learn from other industrialized countries’ experiences in conducting alternative methodologies to reach this targeted population (Barratt et al., 2012; Barratt & Lenton, 2015; Barratt et al., 2015).
Conclusion
Despite these limitations, this the first U.S. study describing national estimates for individuals who self-reported growing cannabis in the past year by selected characteristics and U.S. geographical location. These results show that less than half a million Americans aged 12 and older self-reported growing cannabis in the past year and that cannabis growers were more likely to be male, living in a household with an income less than US$20,000, and reported using cannabis for >300 days in the past year. These findings are broadly consistent with the findings obtained from web-based surveys targeting more regular cannabis users (Potter et al., 2015), which suggests that in the case of cannabis, household populations may be useful for understanding cultivation behavior.
These data are important because they establish a baseline before many states allowed cannabis retail sales (2014), which will enable public health authorities to understand future changes in the U.S.growing cannabis market. Given the existing and evolving changes in use, state-level cannabis laws and policies, and the growth in the U.S. cannabis market (Azofeifa et al., 2016; Caulkins et al., 2016; Lin et al., 2016; National Conference of State Legislatures, 2019), continued monitoring on modes of acquisition such as growing and buying patterns is vital to understand how this market gains or loses cannabis users. In addition, it will be valuable to track these patterns to understand the effects of cannabis state legislation and to better inform public health messaging and prevention education.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the College of Health and Human Services, Western Michigan University and the Price School of Public Policy and Schaeffer Center for Health Policy and Economics, University of Southern California.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Participation Protection
The National Survey on Drug Use and Health (NSDUH) data are protected under the Confidential Information Protection and Statistical Efficiency Act of 2002 (PL 107-347), which ensures that all data are used for statistical purposes only and cannot be used for any other purposes. NSDUH was reviewed and approved by RTI International’s Institutional Review Board (Protocol ID Number 13961, Project Number 0213986).