
Abstract
Painful life events have been highlighted as being instrumental in promoting change during drug addiction recovery. This paper attempts to integrate the ‘pains of desistance’ approach into a recovery capital framework. It explores the life courses of 30 people in drug addiction recovery who had previously had a problem with an illicit substance to explore the role of the pains of recovery (potential push factors) alongside different forms of recovery capital (pull factors) at key turning points of change during recovery. Findings demonstrate that pull factors linked to CHIME were significant in promoting positive changes. Turning points acted as antidotes to pains experienced in early recovery. Three antidotes appeared to be gender specific. Implications highlight the need for greater access to community capital pathways. It advocates the need to dispel the myth for a rock bottom moment and for a more macro conceptualisation of drug addiction recovery.
Introduction
Drug addiction recovery is a dynamic process involving long-term, personal, complex processes of change and key life transitions (Best, Ghufran, Day, Ray, & Loaring, 2008; Hser, Longshore, & Anglin, 2007; Martinelli et al, 2020). It incorporates shifts to identity, behaviour and lifestyle, as well as increases in well-being, human growth and active participation in society (Betty Ford Institute Consensus Group, 2007; UK Drug Policy Commission, 2008). Despite this, there has been a tendency amongst studies to focus on the timeframe for recovery or the proportion of people who will recover) (Dennis, Scott, & Laudet, 2014; Kelly, Bergman, Hoeppner, Vilsaint, & White, 2017). However, what remains an under researched area is the exploration of turning points during processes of change when moving from addictive patterns of substance use into drug addiction recovery, and the ongoing transitions and motivations needed to sustain recovery (Addison et al., 2020; Best & Hennessy, 2021).
Drug Addiction Recovery and Recovery Capital
The notion of drug addiction recovery as a complex process of change is key to understanding the journey involved from addiction to recovery (Cloud & Granfield, 2008). The Recovery Science Research Collaborative define recovery as ‘an individualized, intentional, dynamic, and relational process involving sustained efforts to improve wellness’ (Ashford et al., 2019, p. 5). Definitions of drug recovery have evolved over time with earlier definitions of recovery tending to have a greater focus on abstinence, whereas more recent definitions, such as those advocated here, incorporate notions of increased control over substance use, growth and improvements in well-being and in a range of life domains (Martinelli et al., 2020).
Within the drug addiction recovery journey, the person in recovery accrues recovery capital over time (Betty Ford Institute Consensus Panel, 2007). Cloud and Granfield (2008, p. 1972) defined recovery capital as ‘the sum total of one’s resources that can be brought to bear on the initiation and maintenance of substance misuse cessation’. However, the dynamics of recovery and the levels of recovery capital change at different stages of recovery (Best, 2022; Patton et al., 2022). The Betty Ford Institute Consensus Panel (2007) identified that a person moves through different stages or phases during drug recovery. They highlighted how the stability of recovery improves over time. The three key stages are early recovery (which refers to the first year of recovery), sustained recovery (refers to years 1–5 of recovery), and stable recovery (refers to 5 or more years of recovery). Other studies also indicate that the likelihood of stable recovery is greatly improved with longer periods of abstinence (Hser et al., 2007; Schutte, Byrne, Brennan, & Moos, 2001; Shah, Galai, Celentano, Vlahov, & Strathdee, 2006; Vaillant, 2012). Further, Dennis et al. (2014) has found that it takes around 5 years before recovery can be considered ‘self-sustaining’.
Recovery capital increases as a person in recovery makes positive progress along their journey (Cloud & Granfield, 2008). Best and Laudet (2010) see recovery capital as consisting of three domains – personal, social and community (or collective) capital. Recovery capital refers to more than an individual’s internal qualities or resources such as their self-esteem, mental health etc. It also incorporates positive social identity, relational supports and networks, as well as the capacity to access, participate in and contribute to a range of resources in the community. The three domains help bridge together the agentic (personal) and structural (community) factors involved in drug recovery. Whether or not a turning point or a rock bottom moment is utilised as a positive motivation for change may be due to a unique combination of agentic and structural factors faced by the individual.
The recovery journey and the accrual of recovery capital is not a linear or wholly positive experience, and setbacks and barriers are experienced along the way (Best et al., 2021). Research has shown that there are many similarities between the complex processes of desistance and drug recovery (Kay & Monaghan, 2019) including the experience of pains and barriers (Nugent & Schinkel, 2016; Patton & Farrall, 2021). Numerous pains of desistance have been identified, including the pains of goal failure, disappointment and hopelessness, isolation, stigma and exclusion, criminal justice policy and leading a limited life (Farrall, Hunter, Sharpe, & Calverley, 2014; Shapland & Bottoms, 2011; Standing, 2011). Cloud and Granfield’s (2008) conceptualisation of negative recovery capital links to this by showing that recovery capital exists on a positive and negative continuum. Negative forms of recovery capital (usually in the form of negative events, factors, experiences, forces) include things such as criminal justice involvement, age, poor physical and mental health. This body of research suggests that negative factors and forces act as obstacles that slow down or derail recovery progress. This view contrasts with motivations for change studies which suggest that rock bottom moments provide a push momentum that creates positive change.
Motivations for Change: Hitting Rock Bottom
The motivations for change based literature has identified that turning points and rock bottom moments are key to creating change. These studies have identified that a person conducts a cost/benefit analysis (akin to utilitarian theories of deterrence), which can then promote entry into drug recovery from addiction, or from one phase of drug recovery to the next (Betty Ford Institute Consensus Panel, 2007; Brookfield, Fitzgerald, Selvey, & Maher, 2019; Hutchison, 2019; McIntosh & McKeganey, 2001; Teruya & Hser, 2010). Excessive costs or pain(s) are posited as a necessary motivational push factor for change.
Experiencing a rock bottom moment is highlighted as a key explanation for positive change in drug addiction recovery (McIntosh & McKeganey, 2001). A rock bottom moment has been described as a defining moment where an individual feels that they cannot continue with their drug use any longer due to experiencing a crisis, painful event(s), dire life circumstances or loss of hope (Kirouac, Frohe, & Witkiewitz, 2015; Klingemann, 2011). Rock bottom moments represent key milestones in the recovery process, for example, to begin seeking drug treatment or asking for other types of help (Kirouac et al., 2015). Examples of rock bottom moments include a suicide attempt, potential imprisonment, violent threats by a romantic partner, a significant negative health outcome communicated by a doctor; physical degradation; threats of being cut off relationally by a loved one; and becoming pregnant or a potential loss of custody of a child (Addison et al., 2020; Hser et al., 2007; McIntosh & McKeganey, 2001). McIntosh and McKeganey (2001) found that rock bottom moments are more potent than other types of turning points as they are imbued with greater levels of motivation and conviction due to the perception that there is now no alternative but to stop use.
Motivations for Change: Turning Points
Turning points are heterogenous in nature, and Clausen (1995) distinguishes four different types of turning points: a change in a specific role a person embodies, a change in perspective or outlook, a change in life direction or goals, or a change in self-concept. Turning points can be produced by a single event, abrupt change or short-term situation (e.g., an adverse drug effect, being sent to prison, a sudden change to health). Turning points can also be produced by a series of incremental changes over time and long-term, dynamic situations or events (e.g. changes within a significant romantic or familial relationship) (Brookfield et al., 2019; Hser et al., 2007; Hutchison, 2019; Teruya & Hser, 2010). Turning points may also occur due to a positive experience or event (e.g., the news of pregnancy, gaining employment). They do not always have to be the result of a negative experience or event (e.g., a bereavement, loss of employment etc.). Increased awareness may also produce turning points and key decisive shifts in behaviour or help to cultivate an envisioned future and/or identity (Addison et al., 2020; Teruya & Hser, 2010). Turning points are bi-directional, they can entrench dire life circumstances and drug use or can lead to positive progression towards increased well-being and human flourishing. Regardless of the resultant direction produced, it is a dynamic, complex and nuanced process of change, infused with layers of meaning and interpretation (Schinkel, 2019). Whether or not something becomes a turning point is determined by the individual and the meaning they (as well as potentially others) apply to it (Teruya & Hser, 2010).
Turning points can also act as key facilitators to identity change (Biernacki, 1986; McIntosh & McKeganey, 2001). Biernacki (1986) found that the decision to stop using drugs can often occur when there is a conflict of identities because of the event or experience relating to the turning point. McIntosh and McKeganey (2001) highlighted the need to repair a ‘spoiled identity’ that contained characteristics that someone comes to regard as unacceptable to themselves and others. They went on to add that this was rarely sufficient by itself but needed to be accompanied by a vision of a renewed future. These studies highlight the significant role identity plays as a potent mechanism for behavioural change.
Patton et al. (2022) recently explored the role of push and pull factors in promoting change in drug addiction recovery. In contrast to much of the motivations for change based literature, they found that a range of pull factors were most effective in promoting positive turning points and changes from early to stable recovery phases. They identified a range of pull factors and forces that helped promote positive identity and behavioural changes related to the CHIME model; CHIME stands for Connectedness; Hope; Identity; Meaning and Empowerment (Leamy, Bird, Le Boutillier, Williams, & Slade, 2011). The model relates to positive social capital and connections to the community, a sense of hope and vision about the future, the development of new and positive identities, a sense of agency and empowerment through the discovery of meaning and purpose and community service. These factors and forces pulled a person forward in their journey towards well-being, human development, and flourishing. Push factors on the other hand, related to a range of pains of recovery or barriers which, rather than acting as a turning point to move away from negative experiences, instead thwarted recovery.
Rationale
Painful life events and negative life circumstances have been highlighted as being instrumental for change in drug recovery. Therefore, this paper attempts to integrate the ‘pains of desistance’ approach (Nugent & Schinkel, 2016) into a recovery capital framework to highlight those aspects of the recovery journey that are negative, painful and act as barriers thwarting recovery.
The ‘pains’ of recovery are negative factors and forces that act as barriers that impede a person’s capacity to accrue recovery capital (Patton et al., 2022). A pain of recovery is translated into a push factor when the pain of recovery is transformed from a being a barrier to recovery into a motivational force for positive change. Pull factors and forces are strengths, assets and resources or forms of recovery capital that help propel, accelerate, or pull a person forward on their recovery journey. They oftentimes relate to the CHIME model demonstrating that discovery of purpose, constructing replacement identities, creating a vision for the future life desired and being engaged in meaningful relationships and activities are key to positive change.
Whilst both recovery capital and forms of negative recovery capital or barriers to recovery have been explored, they have not been explored as push and pull factors for change. Further, the tendency within studies has been to examine these separately, with some recent exceptions (Best et al., 2021; Patton et al., 2022). To attempt addressing some of these gaps, we use the life-narratives of those in recovery to explore both the pains of recovery (potential push factors) alongside different forms of recovery capital (pull factors) at key stages or points of change in the recovery journey. This will permit a more comprehensive insight into the recovery journey and greater understanding of how push and pull factors act as motivators, facilitators or obstacles for positive change.
We will firstly identify which pains of recovery (potential push factors) are present and which strengths, resources, and assets (pull factors) are present, within the three domains of personal, social and community recovery capital, at key points of change. These key points of change are the getting started in early recovery phase and key turning points in the recovery journey. Secondly, we will explore whether and how the pains of recovery act as push motivational factors, and whether and how pull factors act as pull motivational factors for positive change.
Methods
The paper uses a life narrative approach to the analysis of 30 people in recovery. A stratified sample of 15 males and 15 females (n = 30) was gained from the English and Scottish participants of the REC-PATH study. The REC-PATH European study included participants from England, Scotland, Belgium and the Netherlands. It explored drug recovery pathways using mixed methods (see Best et al. 2018, for a full methodological outline of the REC-PATH study). 28 respondents had participated in a baseline and follow-up assessment survey as part of the REC-PATH study (the remaining two participants completed either the baseline or the follow-up assessment survey) and were invited to participate in a follow up interview. The REC-PATH study had as an inclusion criterion that participants had previously had a problem with an illicit substance but now regarded themselves to in recovery or recovered from their illicit substance problems in line with the view that ‘you are in recovery if you say you are’ (Valentine, 2010). It was very important that we allowed our participants to use their own definition of substance use problems (i.e., we specified that the study focused on illicit drugs and those who identified problems with alcohol or prescribed drugs only were excluded). We made no attempt to test or verify the extent of these problems or whether they would meet diagnostic criteria as the focus was on the individual’s own understanding and definition of recovery.
The respondents were mainly White (27 were White, 2 were Asian and 1 was Black). 29 respondents were in the stable recovery phase and 1 respondent was regarded to be in the sustained recovery phase (Betty Ford Institute Consensus Panel, 2007). The sample ranged in age, with 2 respondents aged 30–39, 17 respondents aged 40–49, 8 respondents aged 50–59 and 3 respondents aged 60–69). Heroin (22 respondents), Alcohol (21 respondents), Cocaine/Crack (13 respondents, 8 and 5 respondents respectively) and prescription medications (5 respondents) were the substances that were highlighted as resulting in addictive patterns of substance use and behaviours. The respondents reported use of several different mechanisms of recovery support during their recovery journeys. 12-step mutual aid groups were most commonly utilised at some point during their recovery journey and were used by 17 respondents; other peer-based recovery support services were used by 6 respondents; community-based treatment (including substitute prescribing) was used by 11 respondents; residential treatment (including residence in a Therapeutic Community) 15 respondents; and natural recovery was used by 1 respondent.
A life narrative approach was used throughout the interviews to allow an exploration of trajectories, transitions and turning points in the life course (Hser et al., 2007). This approach permits the embodied lived experience of the individual to be shared, including the meanings of events at different stages and phases of their life course (Squire et al., 2014), whilst also understanding the socio-historical and cultural contexts in they are occurring (Striano, 2012). A semi-structured interview was used in which participants were asked to describe key events and turning points around key stages of their life: 1. 2. 3. 4. 5. 6.
The interviews permitted an exploration of the participant’s journey to recovery, their experiences of professional and peer support, and their understanding of the key components that supported their recovery or acted as barriers to achieving their goals. The interviews were conducted by telephone by the second author between September 2019 to March 2020 and lasted between 45 and 75 min. The interviewer typed up their responses during the interview.
Push and Pull Factors as Motivations for Change.
Results: Motivations for Change During the Recovery Journey
The results presented below uses the life-narratives of those in recovery at key points of change and transition in the ‘getting started’ in recovery phase and at key turning points in their recovery journey. The results present the lived experience of the pains of recovery (potential push factors) alongside different forms of recovery capital (pull factors) to permit a more comprehensive insight into the recovery journey. The results also present findings as to how push and pull factors and forces act as motivators, facilitators or as obstacles for positive change. (Patton et al. (2022) presented the push and pull findings for the current sample in early and stable recovery phases). It should be noted that pseudonyms have been used for all respondents in the quotations presented below. The results section begins with a discussion of the 10 themes as they relate to the ‘getting started’ in recovery phase. In section two of the results, the seven themes that relate to key turning points in the respondents recovery journey are discussed. Finally in section three, we begin to illustrate how the turning points appear to be antidotes to the pains of recovery experienced earlier in the ‘getting started’ phase of recovery.
‘Getting Started’ in Early Recovery
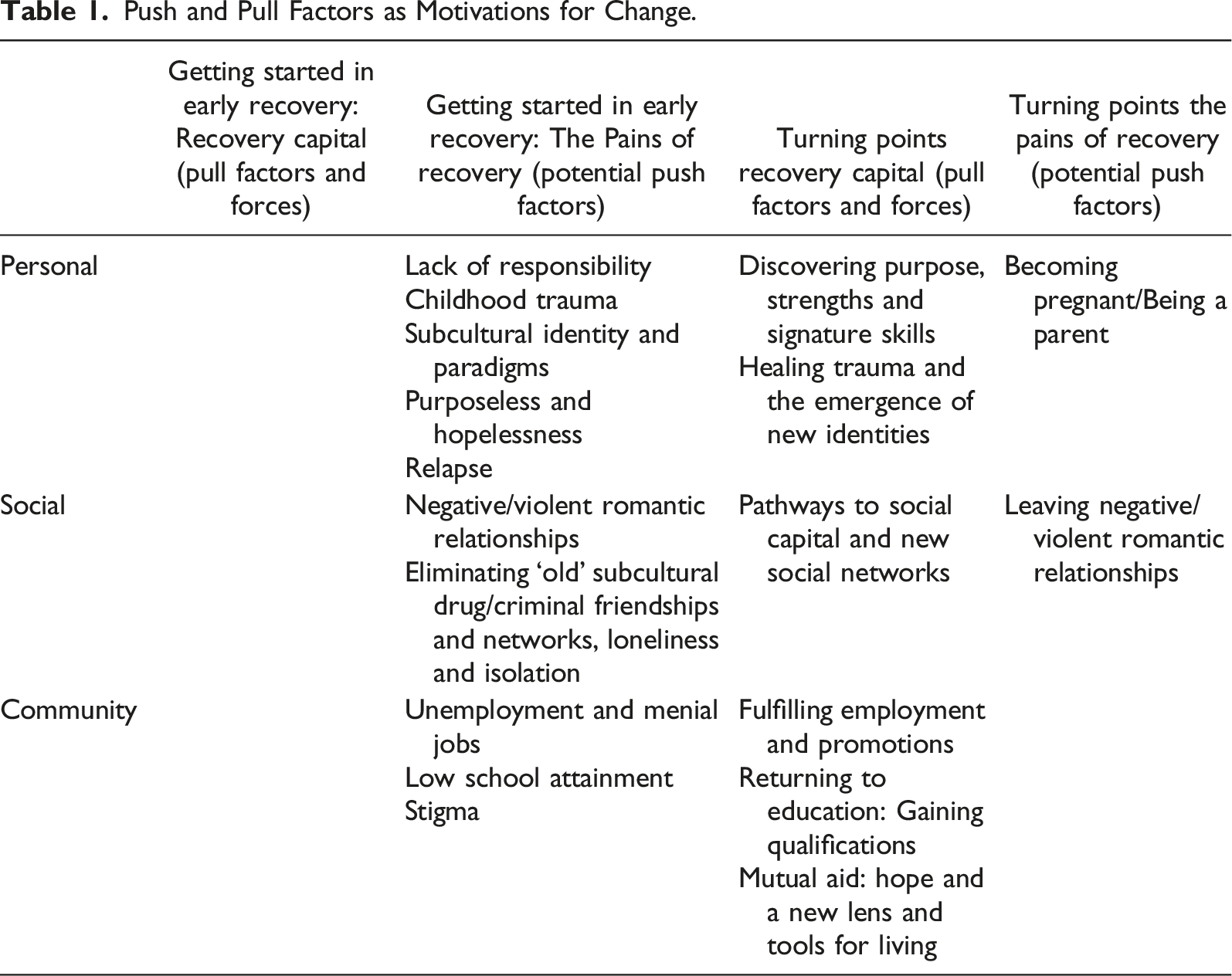
Table 1 presents an overview of all the pains of recovery, push and pull factors identified in the ‘getting started’ phase of recovery and also at turning points within the recovery journey using a recovery capital framework. The ‘getting started’ in the early recovery was a chaotic phase of life and a key time of transition and change in the respondent’s life course. Consequently, respondents did not identify any forms of recovery capital or pull factors in the ‘getting started’ in early recovery phase, and as a result, the first column in Table 1 is blank. This aligns with the finding elsewhere that recovery capital is very low at the start of recovery (Best et al., 2020). However, 10 pains of recovery were discussed by respondents in the ‘getting started’ phase.
The Pains of ‘Getting Started’ in Early Recovery
Personal Capital
The Pains of a Lack of Responsibility
Respondents shared about developing a self-centred existence due to their addictive patterns of drug use and reflected on having a more carefree existence around conventional responsibilities and of having no responsibilities. Dan reflected, ‘I thought I was in the Rolling Stones. I felt completely disconnected from life and I had no responsibility for anything.’ Similarly, Yuri stated, ‘I never paid bills, I never paid taxes, I was horrible.’ Anne described her outlook in the addiction phase, ‘I had nothing to live for…I had no responsibility and my using got worse.’ Overall, parental responsibilities or the envisioning of being a mum was a key antidote to their lack of purpose and responsibilities in the addiction phase. However, for the men, gaining responsibilities at work was the antidote to their lack of purpose and responsibilities in the addiction phase (as discussed below under community capital).
The Pains of Childhood Trauma
Childhood trauma was common amongst the respondents. Key turning points occurred as many of them began to deal with and heal their childhood trauma. Ray observed that ‘when the initial trauma happened as a child, I cut off all feelings, and nicotine as a drug assisted me in staying numb so did alcohol and all the drugs I used. Knowing this was freeing.’ For some the realisation of the connection between their drug addiction and the childhood trauma came during ‘a session one day, I was misbehaving in the group, and the facilitator asked why I had used every day for 25 years. I had no idea why…It kind of set me free and that maybe this wasn’t just my fault’ (Mark).
The Pains of Unemployment, Menial Jobs and Maintaining Existing Roles
Most of the sample in the getting started period of early recovery phase were unemployed or were in menial roles they disliked. Luke expressed how ‘there is a real challenge for getting meaningful work.’ Mark had, ‘been unemployed for a long time.’ Similarly, Anne, ‘wasn’t working at the time.’ Respondents also worked in menial jobs, Alice shared that she had, ‘a cleaning job through my neighbours, cleaning new buildings on a building site. I struggled with money and was on benefits.’
Being in recovery impacted upon respondents’ capacity to work at times. Amy explained that she ‘was still employed but signed off sick.’ Supportive managers and colleagues were instrumental in helping some respondents remain in existing employment roles. Ed explained that ‘I hung onto my job by a thread and would probably have been sacked if I had a different manager.’
Pains of Purposeless and Hopelessness
In addition to the pains of leading a life without conventional responsibilities (discussed above), a key feature of getting started in early recovery was a sense of hopelessness which had a profoundly debilitating and stagnating effect on personal and community capital. The lack of purpose resulted in a lack of vision which in turn created a sense of hopelessness about themselves and stymied a desire for something better. Yosef reflected that at that time he could not ‘recall a time where I experienced a sense of hope.’ Elizabeth felt that her ‘life had no meaning or purpose…I was just going through the motions of being alive’ and Amy recalled that she, ‘wanted to be dead’ as she felt she had no purpose or direction in life.
The Pains of Subcultural Paradigms of Life and Navigating a New Terrain
Personal recovery capital was low in early recovery as evidenced by subcultural understandings of living and their search for a new view of themselves, the world and how to navigate it, as they experienced sobriety. Mutual aid groups increased participants awareness of their ‘subcultural lens’ on life. Eric felt that he was an expert in drugs and how to use them ‘but I knew nothing about living without using drugs.’ Ellie further observed ‘I had to learn everything new.’ Sam reflected, he ‘had no reference point’ and did not know anyone who lived a ‘straight life’ and so questioned ‘What does a decent person do when faced with these circumstances? I was in the dark about what a straight person would do.’ The search for answers, and new ways of understanding and navigating life were apparent and a cause of pain, discomfort and vulnerability.
The Pains of Trying to Stop Drug Use
Relapse was a common feature, especially in early recovery. The road to sobriety was not a straight or simple one. Zoe observed that she could remain abstinent for a week but then ‘I would go on benders.’ Similarly, Emily remembered how ‘I would give myself any excuse to pick up again.’ Yuri also ‘tried to come off Class A but I did not have the tools to maintain any recovery.’ Most of the respondents tried drug treatment as part of their recovery. Yoel shared that ‘I found that treatment was often very rigid and did not often mirror the chaos of my lifestyle. If I turned up 15 min late, I would not be seen. If that happened 2-3 times I would have to restart.’ Yosef reflected on his initial relapses, ‘I had my first in-patient detox for alcohol and methadone, I think I lasted three days then self-discharged and went back to the community where I was dying, and I died a little bit more.’ Luke had attempted to give up heroin, ‘The first time I went into a clinical detox unit was when I was 32 but I only managed to stay relatively substance free for about 7 months.’ Some respondents recognised that they were not ready for drug treatment in this phase, Harriet explains, ‘When I went back into prison one of the options was rehab on a court order, I thought this was a good idea, and I thought I would treat this as a holiday and then go back out and use again. At that stage, I wasn’t emotionally mature enough to get a grasp.’ The pains of relapse impacted on the levels of hope the respondents had that they could ever make the changes they desired relating to their patterns of drug use and broader lifestyle changes.
Social Capital
The Pains of Romantic Relationships
Negative and violent relationships were a central feature of romantic relationships in the addiction phase and early recovery phase. Emily explained how her relationship progressed very quickly with violent repercussions, ‘I met a bloke and we left [rehabilitation]…it was a classic… but when he started using again, he became very violent.’ Similarly, Holly explained that her partner, ‘was a complete and utter twat, violent and nasty, he broke my ribs.’ Anne also shared that her partner ‘was very violent, very controlling and manipulative.’ In most cases the violent relationships lasted for many years and had a profound, traumatic and destabilising impact on their lives which also thwarted their capacity to make progress in drug recovery.
The Pains of Subcultural Networks, Loneliness, and Isolation
As respondents entered recovery, they began to reflect and reassess existing friendships and social networks. A key realisation was that their friendships largely consisted of others who used or sold drugs. Abbie realised how she ‘was always hanging out with people who used drugs.’ Holly reached a similar conclusion and ‘started to cut off. The only people that I had contact with was the dealers thinking they were my friends, but it was only making things worse. So, I started to delete their numbers and not go to those areas anymore.’
The process of re-evaluation was difficult for many and led to the pains of social isolation and loneliness. This required respondents to proactively act to create new social networks, new friendships and to reorient their lifestyle exploring new locations whilst also avoiding old relationships and places.
The Pains of Low School Attainment
Education had not always been a positive experience or outcome in terms of gaining qualifications for many in the sample. Harriet reflected that ‘I did a crap job with most of my school exams. I went to Grammar school…I did not do well at school. The only GCSE I got was in food tech and that was partly because my mum taught it.’ Subsequently a large number of respondents returned to education during their recovery to help acquire qualifications to help them gain employment, gain status and legitimate identities.
The Pains of Stigma in the Workplace
Another key motivator for the return to education was due to experiencing stigma in the workplace. Abbie shared that, ‘having worked in treatment for so long, I am tired of being patted on the head for being another ex-addict and that is why I am doing a PhD.’ Yosef shared the reason why he ‘did lots of qualifications, and was a bit of a training junkie’ was because he felt inferior to those he was working with at a senior level in his organisation.
Turning Points in the Recovery Journey
The seven themes that the respondents discussed as key turning points in their recovery journey are presented below using a recovery capital framework. Five of the turning points were regarded as pull factors, one was regarded as a pain of recovery (a push factor), and the remaining turning point was both a pull factor for some respondents, and a pain (push factor) for the others. Each heading also denotes if this factor was a push or pull factor or both at the end of the heading.
Personal Capital
Healing Trauma and the Emergence of New Identities (Pull Factor)
Lily stated that recovery had meant ‘healing and coming back to her true self.’ Isabel described how she ‘was broken down and then rebuilt. It was the worst and best experience of my life.’ Healing events in childhood was key for Amy who realised that ‘there was all this stuff I blocked out’ but went on to have ‘therapy to heal my childhood trauma.’ Harriet reflected on her journey and was able to create a new sense of self identity as a result, she said, ‘I created a separation from ‘that person’ that I used to be … There was a flip in my mindset about who I am.’ The healing process enabled respondents to create new identities and begin to create new lifestyle and behavioural changes that permitted recovery capital to be built upon.
Finding Purpose and Being Promoted (Pull Factor)
Employment provided a space for the discovery of purpose, a core skill set and the expression of strengths. Such discoveries acted as key turning points and were inextricably linked to advancements in the recovery journey and for stabilising abstinence. They also over time were linked to gaining promotions, finding fulfilling work, financial reward and climbing the career ladder. The male respondents in the sample were more likely to talk about the importance of discovering purpose. Recognition and increased levels of responsibility at work were key vehicles and validations sphere where the males in the sample.
Gaining a sense of purpose through employment was key for many. Dan shared how his workplace has been a key source of affirmation and provided him with his purpose following two successive promotions after returning to work following a long period of absence due to his recovery. He felt his work had ‘cemented my self-esteem…it has given me a real sense of purpose.’ Mark similarly discovered through his work ‘for the first time I had a real sense of purpose. I had a real sense of ownership and pride to me and to my self-esteem. It was the feeling that I can do something.’ Sam recalled a time at a drug recovery conference as a newly appointed Recovery Coach how, ‘It set the hairs on the back of my neck going…that was the first time it gave definition to what I wanted to do with my own life and what we were trying to set up.’
Becoming Pregnant and Being a Mother (Push and Pull Factor)
Parental responsibility was a key motivational reason to want to become abstinent and enter recovery amongst six of the females in the sample. For three of the mums (Holly, Abbie and Isobel) becoming pregnant and their conceptualisation of the mum that they wanted to be and the life they wanted to afford their child helped to pull them onwards into recovery. Whereas for the other three mums (Ellie, Amelia and Anne), their negative experiences and circumstances acted more as a rock bottom type moment that pushed them into recovery.
Becoming pregnant was a key motivator for change for Holly, ‘I was about 30 and I was in a violent relationship. He was using and weirdly I planned to have a child. I wanted to be clean myself if I wanted to be a mum. When I did get pregnant that was the motivation for me to stop.’ Similarly, for Abbie, ‘I found out I was pregnant…It was the straw that broke the camel’s back…I saw the life I was living through a child’s eyes, this is far too violent and dirty and horrible to be a childhood. …I did a 10-day DF detox, and my daughter was born in March 1998, and I never used again.’ For Isobel becoming pregnant also sparked other key transitions, “I fell pregnant, got a mortgage, and moved into my own house.’
Rock bottom moments acted as a push motivation for change for three of the six respondents related to this turning point. For Ellie the goal of abstinence was initially more of a struggle, ‘I was already 6 months pregnant when I found out I was pregnant…[social services] went straight for adoption. It was then that I had to stop. I was a heroin user and alcoholic…I tried to stop but I could not. I ended up in a hospital having my son and social services took him away from me. The solicitor said either you keep using and give up your son or you stop using and you keep him. This was the point I decided to change.’
Being a mother was also a key motivator for change after experiencing rock bottom moments for some. Amelia described a key turning point for her when she realised, she risked losing the relationship she had with her children, ‘I went into blackout and ruined the holiday, and when we came back my middle son came and sat on the side of the bed and said, ‘if you keep drinking, me and the brothers are going to cut you out of our lives.’ I knew that he meant it. For me that was my line in the sand.’ Anne shared her traumatic experiences, and ultimately it was the impact on her children that was the catalyst for change, ‘My life was at risk, my partner had kept me hostage for three days in the living room. He threatened to chop my head off and then kill himself. I could not live this life anymore. I did not want the kids to see their dad kill their mum, that was the lightbulb moment.’
Social Capital
Leaving Negative and Violent Relationships (Push Factor)
Being in a negative, dysfunctional relationship with incidents of domestic violence was commonplace amongst many of the female respondents at the start of their recovery journey. For some, their partner also influenced their use of drugs. The negative effects of such relationships over time became a turning point for the females affected by this to leave the relationship or break the pattern of having multiple partners who had been violent towards them.
The effects of leaving a negative, abusive, or violent relationship provided a level of safety and stability that the female respondents had not had previously. Anne shared how she ‘got into a really bad relationship. I got married after 6 weeks to someone who was an addict… My partner was quite controlling and was using it over me, he was building up my tolerance so I could not cut down…it was chaotic for 12/13 years until I left.’ Holly shared that she was with her partner, ‘for a couple of years, and it ended just after Christmas. After he raped me on Christmas morning’. In addition, separating from negative relationships also provided the opportunity to create new living environments and lifestyles and one where drugs were not present. Alice shared how she was able to enter recovery after separating from her partner, ‘My ex-husband went to jail…one month after separating from him I stopped using drugs and I do not think that’s just a coincidence, I do take responsibility for my own using but think I was vulnerable, and he influenced me. He introduced me to heroin.’ Zoe said that she ended the relationship due to her partners ongoing drug use, ‘I left him in the end…he still wanted to smoke crack and smoke week and I came home from work one day and the house was full of teenagers smoking weed. I just thought that I did not want this.’
Pathways to Social Capital and New Social Networks (Pull Factor)
Mutual aid groups were key in providing pathways to social capital and creating new social bonds and friends for life, especially amongst the female respondents. Harriet shared how she ‘made some really good friends that meant something to me’ at her meetings. For some, the relationships were stronger than just friendships, Harriet, shared that she felt she ‘had gained big brothers’, and similarly Laura shared how she gained ‘a brand-new family’ through her recovery groups. Abbie found that her participation in recovery groups helped her ‘start a social life and network, and I am still friends today with some of them.’ Nathaniel felt that ‘the support I got in the meetings filled the void of drugs.’
Returning to education during recovery was also a key turning point as it helped respondents gain new friendships and social networks. Noah observed that ‘my social life massively improved. I started making friends at the college who had never known me in my drinking and using days.’ Anne found that when she ‘went to college, I have a good group of friends from that, and I am still in contact with lots of them.’
The workplace also opened pathways to social capital by providing opportunities for new friendships and social networks. Lily shared that the way she socialises now, ‘is with work colleagues.’ Mark explained how his ‘social life was built around’ the recovery project he was leading. Eva shared that her work colleagues were there to lift her up and ‘the loudest cheer leaders when things go well.’
Community Capital
Returning to Education and Attaining Qualifications (Pull Factor)
Whilst gaining new qualifications wasn’t always easy for everyone, almost all of those who returned to education did attain a range of new qualifications. Amy utilised this second chance at education and gave it her all, she said ‘I did not go out of my flat, I studied and ate digestive biscuits, no drinking, no drugs and no life. Zoe also returned to education and ‘went to college and did an access course in sociology and I smashed it. And then I went to uni…I spoke to my dissertation supervisor, and he is now my PhD supervisor.’ Attaining qualifications boosted self-esteem and helped construct new legitimate identities. It also increased levels of community capital in relation to the employment roles and career pathways this opened as well as the increased status this afforded them within their workplace and local community.
Fulfilling Employment and Promotions (Pull Factor)
Discovering a sense of purpose and identifying strengths and signature skills often led to advancements in terms of promotions and seniority further down the timeline on the respondents journey. Yosef had a series of promotions once he discovered some of his core skills and strengths, he explained, ‘I was a trainee recovery coach. It became pretty clear that I had a talent for group facilitation, psychosocial interventions, care plans, working in a person-centred way, listening and I progressed really quickly to a full-time recovery coach and then a lead recovery coach.’ Nathaniel also noted how his discovery of purpose and skill set had led to a series of successive job progressions, he explained that ‘I got involved in the local group, then intergroup, then national, then international and I am now the national lead for the UK region. The one thing beyond that is joining the world board. I will certainly consider that in the next few years.’ Such discoveries resulted in respondents expressing a passion and fulfilment for their jobs, ‘I love what I do and the biggest part of that is that I feel useful, in a way I never have before.’ (Yosef), and Sam said that he ‘really loved the job’ that he was doing.
Mutual aid Groups: Hope and New Paradigms and Empowering Tools for Change (Pull Factor)
Mutual aid groups offered a fundamental turning point for many in the sample. Whilst respondents had spoken about having periods of abstinence, they described how they struggled to maintain this until they began doing work in a recovery group. Eric described his moment of entering a recovery group and ‘when people told me how to stay clean it was like dropping bombs… I was done with using drugs and I just needed someone to show me the way.’ Respondents described that they became equipped to maintain their recovery, Elizabeth described that the process of being equipped was key for her and that her recovery group provided her with a means to navigate life and that had provided her with ‘a manual for life.’ Similarly, Emily explained that ‘one of the key factors for me was being given this information about myself and about addiction, and what you can do about it.’ Ed reflected that he had, ‘No relapse or lapse since first entering the programme. This was down to doing the programme correctly and working hard.’
Meeting others in recovery who had made significant changes to their lifestyle including the elimination of drug use was key as it created a contagion of hope as it allowed those getting started in the early recovery phase to have hope that this change was and is possible. Yoel found that ‘In the early days, seeing other people with lived experience was a really useful thing to see people who had come out of the other end, who were happy and content with their lives.’ Noah also found hope in hearing people share that ‘they had not had a drink for months or for years and to me that seemed like a staggering achievement, and I just could not imagine at the time and it was those two things that kept me coming back. It was that sense of identification with people’s sense of hopelessness and that there were people there who had stopped.’ Similarly, for Nathaniel, ‘When I started meeting with other people in recovery, made me think how easy it was. From that day, I never relapsed and never picked up a drug.’
Turning Points as Antidotes to the Pains of ‘Getting Started’ in Recovery
Turning Points as the Antidotes to the Pains of Getting Started in Early Recovery.
Personal Capital Antidotes
Beginning to Heal: The Antidote to Childhood Trauma
There was an obvious link between experiencing trauma as a child, and then later as an adult, because of their recovery journey, entering some form of counselling, or therapeutic group. Consequently, the respondents began to heal their trauma and construct new replacement identities. The healing and positive replacement identities acted as an essential antidote to the pains of their childhood.
Discovering Purpose and Strengths: The Antidote to Hopelessness and Lack of Meaningful Direction
Discovering purpose, a core skill set, and a set of signature strengths through employment opportunities was one of the biggest turning points for many in the sample, especially the male respondents. This pull factor was the antidote to the pains of a lack of responsibility (discussed above), the pains of unemployment or menial jobs and the pains of purposelessness and hopelessness. This pull factor alone helped to accelerate progress in recovery as it also provided legitimate replacement identities, a sense of affirmation and acceptance. As well as increases to financial capital, it offered access and participation in new esteemed spaces within the work sphere and new self-perceptions and identities.
Parental Responsibility: The Antidote to Living for Oneself
The anticipated advent of a child acted as a pull factor for some, whilst the awareness of the potential loss of access/relationship to a child acted as a push factor for others. Both motivations provided an antidote to earlier pains of purposelessness and lack of responsibility. The mother child relationship provided the respondents with a clear sense of purpose and responsibility beyond themselves and links to the restoration or development of positive identities.
Social Capital Antidotes
Leaving Romantic Partners: The Antidote to Violent and Negative Relationships
The literal pains of living with a violent and controlling partner became too much for the females in the sample. As a result, such pains became the motivational push for them to finally leave the relationship and make a fresh start. This in turn provided a foundation on which to build a new life and identity and accrue recovery capital.
Social Networks in Mutual Aid, Education and Employment: The Antidote to Cutting off Subcultural Networks, Loneliness and Isolation
Friendships and social networks gained through mutual aid groups, education and employment provided the antidote to the pains of loneliness and isolation as a result of cutting off old drug using friends and subcultural networks in an attempt to sustain abstinence.
Community Capital Antidotes
Mutual aid Groups Providing a New Lens for Living: The Antidote to Subcultural Paradigms and Relapse
Mutual aid groups were not only important for access to new groups and social networks but provided new tools and paradigms for life which acted as a replacement to subcultural paradigms and lifestyles. This new lens for living was an antidote to low levels of personal capital as respondents prior to attending mutual aid groups did not have a paradigm of how to lead a ‘conventional lifestyle’. Further, mutual aid groups were key in eliminating or significantly reducing relapse amongst many within the sample.
Returning to Education and Gaining Qualifications: The Antidote to Under Achievement at School and Stigma
Returning to education was a key antidote for those who did not achieve qualifications earlier in life and helped some overcome stigma at work. Attaining qualifications provided much needed validation in the workplace, increased both personal and community capital through an increased sense of empowerment and identity change linked to CHIME. Engagement in education and later in employment provided much needed replacement identities both for themselves but also in the eyes of the other in the community and workplace etc.
Discussion
The paper contributes to our understanding of turning points in addiction to recovery careers by characterising the challenges in overcoming addictions and the role of push and pull factors in sustaining and building recovery pathways. Within the recovery capital framework, we were keen to observe the number and nature of both the pull factors and the pains of recovery as motivations for change, as well as the impact of the factors and forces for initiating and sustaining positive or negative changes in the recovery journey. Ten themes were identified as pains of recovery in the ‘getting started’ phase of recovery and no pull factors were identified by the respondents. The 10 pains were, lack of responsibility; childhood trauma; subcultural identity and paradigms; purposeless and hopelessness; relapse; negative/violent romantic relationships, eliminating ‘old’ subcultural drug/criminal friendships and networks, loneliness and isolation; unemployment and menial jobs; low school attainment; and stigma. Seven themes were identified as turning points. The majority of the turning points (five out of seven) were regarded as pull factors: discovering purpose, strengths and signature skills; healing trauma and the emergence of new identities; pathways to social capital and new social networks; fulfilling employment and promotions; returning to education and gaining qualifications; mutual aid, hope and a new lens and tools for living. One turning point was a push factor: leaving negative/violent relationships. One turning point was experienced as a push factor for some and a pull factor for others: becoming pregnant/being a parent. Overall, it was observed that pull factors exerted the most influence in creating positive changes which oftentimes had an ongoing positive ripple effect on other aspects of the recovery journey and domains of recovery capital.
The turning points characterised as pull factors showed the greatest positive impact in promoting advances in recovery. These pull factors related to the CHIME model (Leamy et al, 2011) and psychological capital in positive psychology (Youssef-Morgan & Luthans, 2013) with its emphasis on hope, efficacy, resilience and optimism. As an illustration, from the research carried out, we see an example of the significant positive impact of a CHIME-related pull factor in the area of employment, where this provided a space for the key turning point of discovery of purpose, a core skill set, empowerment and the expression of strengths. This in turn created an ongoing ripple effect of positive changes, and typically linked to advancements in a range of recovery capital domains such as an increased sense of empowerment, the achievement of goals, an increased sense of agency, increased recognition and levels of responsibility including promotions and financial rewards. It permitted the creation of new legitimate replacement identities akin to notions of secondary desistance (Farrall et al., 2014). Social capital increased as new friendships developed in the workplace and access to new pro-social networks emerged. It also provided increased access to community resources and opportunities and an increased sense of belonging akin to tertiary desistance (Anderson & McNeill, 2019).
Access to meaningful employment is often cited as a barrier for many in recovery (Best et al., 2021). The findings here reveal a different perspective of how the positive ripple effects of gaining meaningful employment highlight that it is so much more than simply gaining employment or an income. The reason why gaining meaningful employment and discovery of purpose and signature skills as a turning point was so potent as a pull factor was due to earlier deficits during the addiction phase and the pains of getting started in recovery. Specifically, the pains of purposeless and hopelessness, the pains of lack of responsibility and the pains of unemployment and menial jobs. Once pull factors are introduced into a respondent’s life, they help to rebalance these life domains from being on the negative side of the recovery capital continuum to moving to the positive side of the recovery capital. They act as an accelerator for change including promoting positive ripple effects which impact multiple areas of life (Best & DeAlwis, 2017; Cloud & Granfield, 2008).
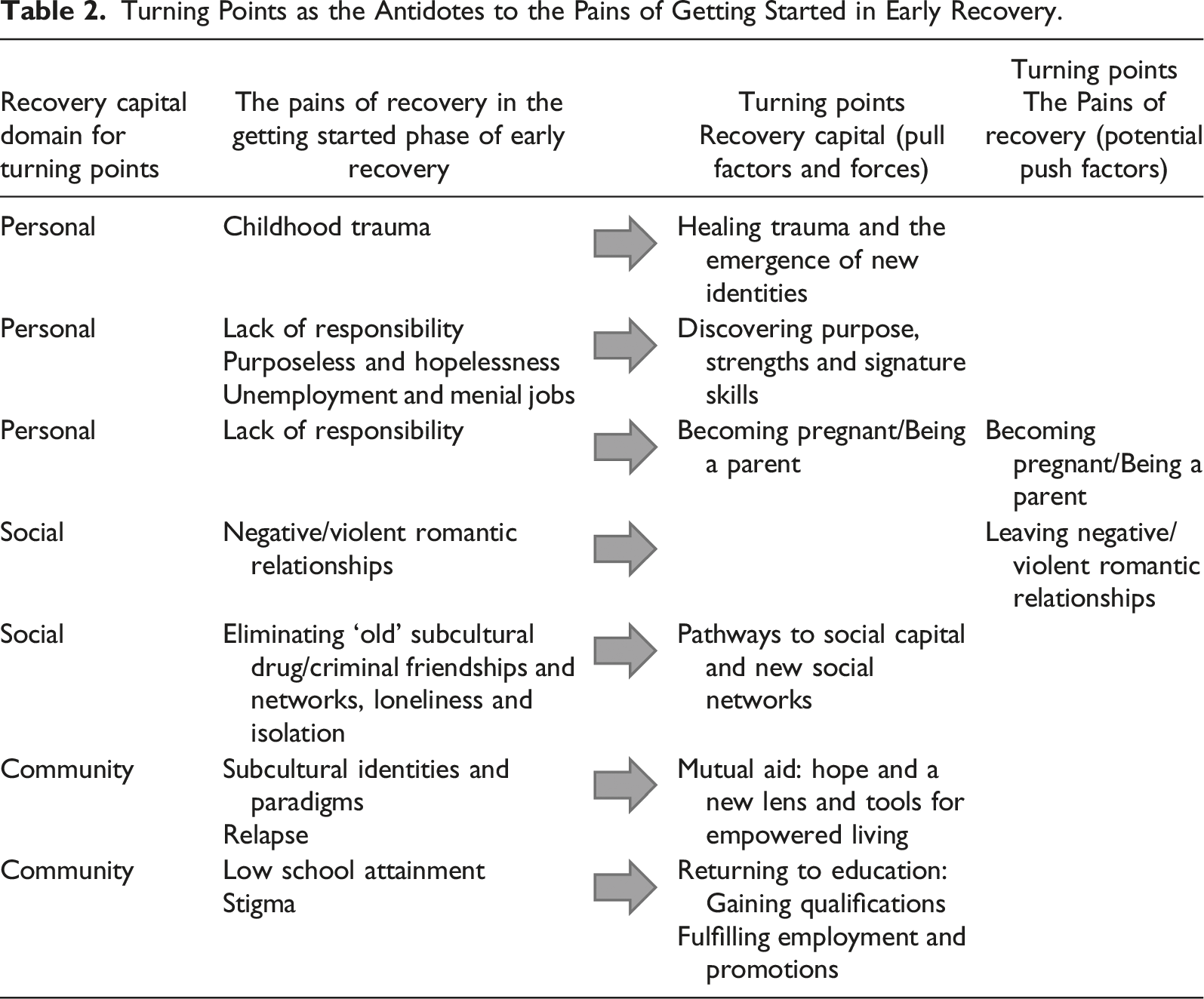
The pull factors and forces expressed through the turning points were typically preceded by one or more related pains of recovery in the ‘getting started’ stage. Each turning point acted as a sort of antidote to the pains of recovery previously experienced. The pains of recovery remained a negative, limiting, or painful event/experience which thwarted advances in recovery capital accrual and human flourishing until it was met by a pull factor. For example, childhood trauma remains debilitating until opportunities for healing are presented through counselling, therapy, or mutual aid support; pains of loneliness and isolation persisted as a result of respondents cutting off ‘old’ drug using and criminal networks until they were greeted with new social networks and opportunities for friendships through the workplace, education and mutual aid groups. The pull factors present a sort of ‘doorway’ to new pathways and modes of being and doing in the world that allows the respondents to move forward, beyond the pains and barriers experienced. In this sense, there is a dynamic interaction occurring at different time points between push and pull factors and forces. Further, respondents experienced multiple turning points at different stages of the recovery journey to initiate and sustain the recovery process. The potency of pull factors and forces as the positive means through which the accrual of recovery capital is gained, is potentially due, at least in part, to the deficits caused by the pains of recovery and further highlights why a deficit approach to recovery or behaviour change will not prove to be effective. Rather a more comprehensive understanding is needed of the dynamic tensions and relationships between pains, deficits, barriers, push factors, strengths, assets and pull factors and forces.
Negative or painful turning points and rock bottom moments were heralded in the literature as demonstrating a potency for positive identity or behavioural change. However, push factors in the form of turning points or rock bottom moments generally did not act as motivational push factors that created positive change. Two main exceptions to this were found; two push factors provided the motivation to make positive changes, and these highlight a possible gendered effect operating. Firstly, fleeing a violent and abusive romantic relationship was the strongest push factor for many of the females in the sample. This provided the safety and stability for these respondents to begin to accrue and build recovery capital in different life domains. Secondly, for mothers, the threat of losing custody of a child, including becoming pregnant with the threat of losing custody of the baby once it was born, became the push factor that led to positive changes.
A third gendered effect was found but this time amongst the male respondents in the sample, who were far more likely than the females to talk about the importance of discovering purpose, strengths and meaningful employment and how this led to a succession of promotions as well as other advances in their recovery capital domains. The females rarely mentioned this as a significant theme and therefore this represents a third potential gendered effect operating within the findings albeit this time with a pull factor.
What has emerged is that the same turning point is not always experienced in the same way. Purpose was key to both males and females. The turning point of discovery of purpose came through the form of motherhood for many of the females in the sample and through employment and career for many of the males. The complexity of turning points is further highlighted through the finding that the same turning point, for example motherhood, can also operate as both a push factor for some and yet a pull factor for others. Similarly, the complexity in understanding turning points is highlighted through the potential transformation of a pain of recovery, and whether it remains as such, or becomes a motivational push factor for change. What is potentially occurring with this sample is, as Schinkel’s (2019, p. 366) work highlights “how aspects of life which have been positioned as ‘turning points’ in the desistance and criminal careers literature are not ‘points’ at all, but complex processes incorporating a multitude of subjective meanings and experiences, with a number of effects on offending trajectories and beyond.” What may appear to be a single turning point is part of a larger, more complex, nuanced and dynamic interplay of push and pull factors, interlaced with differential levels of individual agency, situated choices and meanings, recovery capital, hope, and structural location within society.
The qualitative life course data has uncovered rich insights. These insights reveal complex nuances in the dynamic interactions between push and pull factors and forces during the recovery journey, using a recovery capital framework, that would not have been possible with quantitative data alone. Qualitative research has a much-needed role to play in helping to illuminate the intricacies of these interactive and dynamic recovery capital pathways. An even greater number of qualitative studies in this field would be welcomed to advance understandings in the science of recovery. The turning points data presented here has revealed that at any one time, especially in the ‘getting started’ period of early recovery, the individual is having to grapple with multiple, complex, and at times competing life circumstances and narratives regarding their identity and recovery. Factors such as the physiological effects of substances are also compounded by experiences of marginalisation, stigmatization, abuse, and interpersonal violence.
Based on the findings, there are numerous implications for policy and practice. The pains and antidotes of drug recovery revealed a wide range of life domains where support is needed to prevent the development of illicit drug addiction behaviours or to help assist create stable recovery. The areas highlighted by those with lived experience of recovery are family support services, child welfare services to help with childhood abuse and trauma and recovery from such experiences, as well as education services, employment and housing to provide the pull factors necessary for recovery. Drug policies which inflict further pains onto an already over-burdened individual with excessive pains in the addiction or early phase of recovery are unlikely to be effective yet are financially costly. The findings here relating to the supplanting of new paradigms and lifestyle practices through mutual aid groups, support the policy recommendation provided in the recent Dame Carol Black review (2021) in England and Wales for the creation of a Recovery-Orientated System of Care (ROSC) to include people with lived experience of drug dependence working as recovery champions and recovery coaches, to provide networks of peer-based recovery support and establish communities of recovery and mutual aid groups.
In relation to implications for practice, there is a need to raise awareness about the myths of the potency or effectiveness of rock bottom moments. Dispelling the belief in the need for a ‘rock bottom’ moment as a necessary or qualifying event before being able to commence recovery could be key for some, who might otherwise elongate the addiction phase unnecessarily by waiting for such an event which is ultimately likely to be ineffective (Klingemann, 2011). At the crux of many of the antidotes to recovery discovered here, is the need to provide access to community capital (employment, recovery, professional and wider community services) that creates opportunities for new social networks and new role models. Developing structures and systems that permit access to pathways and help facilitate this process will prove effective in promoting change. The research findings here could help to inform recovery care plans by mapping out various pains, push and pull factors at different phases of recovery and potential relationships and dynamics between them to help increase the likelihood of accruing recovery capital. The recovery care plans should also consider some of the three gendered effects found here.
A number of potential limitations exist with the current research. This article has examined each turning point as a single or isolated turning point as expressed by the research participant. However, life is rarely as compartmentalised as this, so we acknowledge the likely interconnectedness of a range of factors that may have contributed to interactions between turning points or rock bottom events. Further, each turning point or rock bottom moment has been explored as a driver or obstacle to recovery progress and in this sense has been made subservient to this process which may not have been the respondents view of the particular event or crises etc. Finally, the findings here rely on retrospective recall of life course events, so aspects of the respondent’s life course accounts may not be fully accurate. However, turning points only make sense as a retrospective interpretation of lived and living experience.
The implications for recovery research are that conceptually it needs to incorporate more macro understandings of the causes of addiction and the processes of recovery. Inherent within definitions of recovery and recovery capital as a framework for overcoming addiction, is the acknowledgement that the causes of addiction and the pathways out through drug recovery go beyond the individual and are also linked to structural and systemic factors and forces as well as social relationships and notions of belonging and participation in society. The pains of recovery (akin to the pains of desistance) are not necessarily pains experienced as a result of these processes but rather have origins that pre-date entry into either process. In a sense therefore, the pains of addiction and drug recovery should perhaps more accurately be described as the pains of personal, systemic, structural and societal ills. Pull factors, expressed through a turning point, act as the antidote to the pains experienced. It is proposed here that the practices and science of recovery being developed is in effect a kind of antidote or antibody to drug addiction. At present, the emphasis remains inaccurately on the individual and their personal process. The pains described by the sample here are of course personal and relate at the individual level, but they are also shared and collective. Therefore, the systems, structures and societal ills need to recover also.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Health Research, grant number PR-ST-0217-10001.