
Abstract
Nitrous oxide (N2O) is a popular recreational intoxicant and associated paraphernalia are increasingly being found at road traffic accident scenes in the Netherlands, suggesting that N2O intoxication causally contributes to the occurrence of a significant number of road traffic accidents. However, information on the pharmacodynamics- and kinetic characteristics of recreational N2O use is limited, impeding policy making and enforcement. This investigation aimed to determine a representative dosing method for recreational N2O use and establish a relevant timeframe for assessing psychomotoric functioning in future research. Online survey responses of 511 N2O users revealed that the majority inhaled N2O from party balloons filled with 4–14 L of N2O. Inhalation typically involved a repetitive “rebreathing” technique with 20–30 second breaks every six cycles, or without breaks, for approximately 12 cycles in total. 10.3% of respondents admitted to have inhaled N2O during driving in the past. Driving departure within 1 hour of inhalation was common, providing a relevant timeframe for the investigation of psychomotoric effects of recreational N2O use in future research.
Introduction
Nitrous oxide (N2O) is a gaseous anesthetic drug that has been in use in clinical practice for preoperative and procedural anesthesia since the middle of the 19th century (Robinson & Toledo, 2012). It is therefore one of the oldest anesthetic gases. Nitrous oxide acts, among other things, as an N-Methyl-
The recreational use of N2O is associated with risk of harmful outcomes, although the potential harms do not appear to be generally appreciated among users (Allan et al., 2022). Apart from the potentially severe health consequences of excessive use, that is, vitamin B12-deficiency-induced neuropathy (Winstock & Ferris, 2020), risk of asphyxiation (Wagner et al., 1992) and frost bite injuries (Hwang et al., 1996), the acute state of dissociation and ataxia that accompanies N2O intoxication introduces a risk of injuries due to accidents (van Amsterdam et al., 2015). It is therefore ill advised and in violation of traffic law in most jurisdictions to use N2O while operating a vehicle in traffic or while operating heavy machinery. Nevertheless, various recent reports regarding recreational N2O in the Netherlands highlight an especially concerning trend of recreational users consuming N2O while driving. From January 2019 to October 2021, the Dutch police reported nearly 1800 traffic accidents in which N2O use was suspected to play a role (van Hulzen, 2021). The total number of incidents (accidents or routine traffic stops) reported by the Dutch police where evidence of N2O use was available, appears to be steadily rising, with 60 incidents reported in 2016, to 960 incidents counted in 2019 (van Hulzen, 2019). A recent survey study among 209 recreational N2O users found that 35% of the respondents admitted to having operated a motor vehicle directly after or while inhaling N2O (van Meer, 2020).
The increasing prevalence of N2O use in traffic in the Netherlands, and possibly elsewhere (Vinckenbosch et al., 2023), warrants more research into the effects and detectability of recreational N2O use (i.e., magnitude and duration), in car drivers. These effects of recreational N2O use are expected to differ conceivably from those of medical administration due to its shorter exposure time and higher concentrations. An investigation of an internet forum for recreational N2O users by Mclean et al. (2022) shows that there are various ways for recreationally inhaling N2O. However, what a “typical” recreational dose of N2O entails is not clear. In their review, van Amsterdam et al. (2015) mentioned that a typical recreational dose of N2O consists of a party balloon filled with ≈3 – 5 L (normobaric) N2O. However, the authors also acknowledge that it is difficult to determine the exact dose typically inhaled from the balloons because users inhale a number of small and imprecise volumes from the balloons. Indeed, how N2O is typically inhaled (e.g., number of inhalations) has not been investigated. Also, recreational N2O users often use multiple subsequent doses in one session. Prior research reported that the majority of N2O users (≈80%) use at most 10 doses per occasion (van Amsterdam et al., 2015). The typical time interval between subsequent doses has not been documented. A more detailed understanding of recreational N2O dosing and administration is essential for selecting a representative dosing method in future experimental studies into this phenomenon.
Apart from being used on the road, N2O appears to be frequently used in parked vehicles (Hamans & Peters, 2019). It is of concern that the diffusion of N2O within the confined space of a passenger car could result in intoxicating air concentrations of N2O. This concern arises from the fact that, N2O is mainly excreted respiration without undergoing significant metabolic changes (Banks & Hardman, 2005). Hence, it is conceivable that departing after using N2O in a car without properly ventilating could unintentionally result in intoxicated driving because of the presence of residual N2O within the vehicle, especially if multiple occupants have been using nitrous oxide in the same vehicle (Wagner et al., 1992). Furthermore, regardless of whether proper ventilation is observed or not, it is unclear whether the impairing effects of a typical dose of N2O use have completely subsided after the subjective high has waned, and if not, for how long those persist. A study by Moyes et al. (1979) found that the number of errors during simulated driving was significantly increased up to 30 minutes after a 15-min exposure to 50% or 70% N2O. It can, therefore, not be ascertained that it is safe to participate in traffic soon after a typical recreational dose of N2O was inhaled. Whether recreational N2O users take care of proper ventilation in confined spaces like a car, or how long they usually wait until they start driving after N2O use has not been investigated.
The survey presented in this article was conducted as an exploratory investigation leading up to an experimental study [EudraCT Number: 2021–003,242–20] into the effects of N2O on psychomotor function related to driving performance and its detectability in breath samples, blood, and saliva. Hence, the primary objective of the current survey was to identify a representative dosing and administration method (volume, inhalation medium, number of inhalations, inhalation technique, single or multiple dosing, duration between subsequent doses, etc.) for recreational N2O use. A secondary goal was to investigate the prevalence of N2O use while or shortly before driving, and to determine how long drivers usually wait before departing after N2O use. This information will help to decide on the required duration of measurements after N2O administration in the aforementioned experimental project. A third, minor objective was to investigate whether proper ventilation of N2O use in vehicles was generally observed to support the relevance of future research into the intoxicating potential of N2O in confined spaces such as passenger cars.
Methods
Survey Structure
An online survey was constructed using the Qualtrics®XM survey building software. The survey was divided into four blocks containing questions centered around (1) respondent demographics, (2) frequency of N2O use, (3) dosing and method of administration, and (4) recreational N2O use in relation to traffic participation, in that order. Survey flow logic was introduced in the design so that different follow-up questions were displayed to respondents depending on their prior answers. For an overview of the survey flow, questions (originally in Dutch, English translations included for demonstrative purposes), and answer options, the reader is referred to the supplementary materials. The survey was designed to take approximately 10 minutes.
Survey Distribution and Incentives
A link to the online survey was published in July 2021 as a paid advertisement on Facebook® and Instagram®, using the Meta® business suite. The selected target population was aged 18 – 64 years, residing in the Netherlands and having used N2O recreationally at least once in the last 5 years. Despite having the lowest prevalence of recreational N2O use compared to the other age groups, the advertisement disproportionally reached people from the age group of 45–64 years (65.4% of people reached according to Meta® Business suite provided estimates). Therefore, an identical advertisement was published targeting the age group of 18–44 years, 11 days after publishing the initial advertisement. The advertisements were exclusively published in Dutch, hence the targeted population consisted solely of Dutch speakers. The first advertisement remained online for 43 days, while the second was online for 32 days. Both advertisements and the survey itself were taken offline after 500 complete survey responses were recorded. This sample size was selected based on the available budget for incentives, which consisted of a €25 voucher that was raffled for every 50 surveys completed.
Validity Check
Several validity checks were performed in order to identify invalid, nonsensical, or untruthful responses, and cases were excluded if they were judged invalid after closer inspection. Firstly, respondents who reported to have last used N2O more than five years ago in either item 1 or item 7 (see supplementary materials) were excluded, as this is inconsistent with the a priori-determined cutoff for last use (i.e., <5 years ago). Secondly, only respondents who, at a minimum, completed block 1 (demographics) and 2 (frequency of use) were included for the final analysis. Thirdly, answers to questions 9 and 13 were pooled in a new item listing the reported total number of doses used in a typical single day where N2O was used. The answers to this pooled item were compared to that of item 33 (doses/balloons per occasion). It was deemed plausible that the total number of doses used per day of where N2O was used could exceed the number of doses per occasion, if multiple occasions occur per day. However, it appears inconsistent to state that more doses are used per occasion than are used per day of recreational N2O use. Since the respective items included a slide button, which might not be as easily controlled on a mobile device, a difference of at most five doses was allowed, assuming that these respondents intended to indicate the same number of doses in both items. Fourthly, it was checked whether respondents who indicated to have changed their habitual N2O use since the start of the sars-cov-2 pandemic on item 14 provided consistent answers in items 15 to 20. Fifthly, respondents who indicated to have used N2O in the previous year on item 7 but then indicated to have used N2O less than once during the previous year on item 8 were excluded. Lastly, the recorded time spent filling in the survey was inspected with respect to total percentage completed. Outliers (>1.5 IQR) on the low end (fast answering) were considered suspicious and inspected for irregularities.
Results
Metadata and Validity Checks
A total of 825 responses to the questionnaire were recorded, of which 500 were registered as complete. A total of 147 responses were removed because the responses indicated that the last use of N2O dated from more than 5 years ago. Another 89 responses were excluded because they did not make it through block 2 and therefore only contained demographics. In addition, 19 responses were excluded because the respondents indicated using at least 5 doses of N2O or more per occasion than per day of use, which was considered improbable and likely to be the result of an entry error. Next, 52 responses were excluded because the respondent indicated having changed their pattern of N2O use since the start of the sars-cov-2 pandemic while providing inconsistent answers in the follow-up questions on frequency and number of doses. Finally, 6 responses were excluded because of inconsistent answers to items 7 and 8. No responses were excluded based on completion time. Hereafter, one additional partial response was deleted because the respondent indicated to be aged 100 years. This was deemed hardly plausible or due to entry error, resulting in exclusion of the response. Hence, the final number of responses included for analysis was 511, of which 392 (76.7%) were complete and 119 (23.3%) were partial responses. Because of the inclusion of partial responses and the occasional presence of invalid/uninformative answers (e.g. reporting the weekly use of “one tank” without specifying volume), the sample size will differ throughout this paper, but will be explicitly mentioned for each item discussed. Summary of included and excluded responses.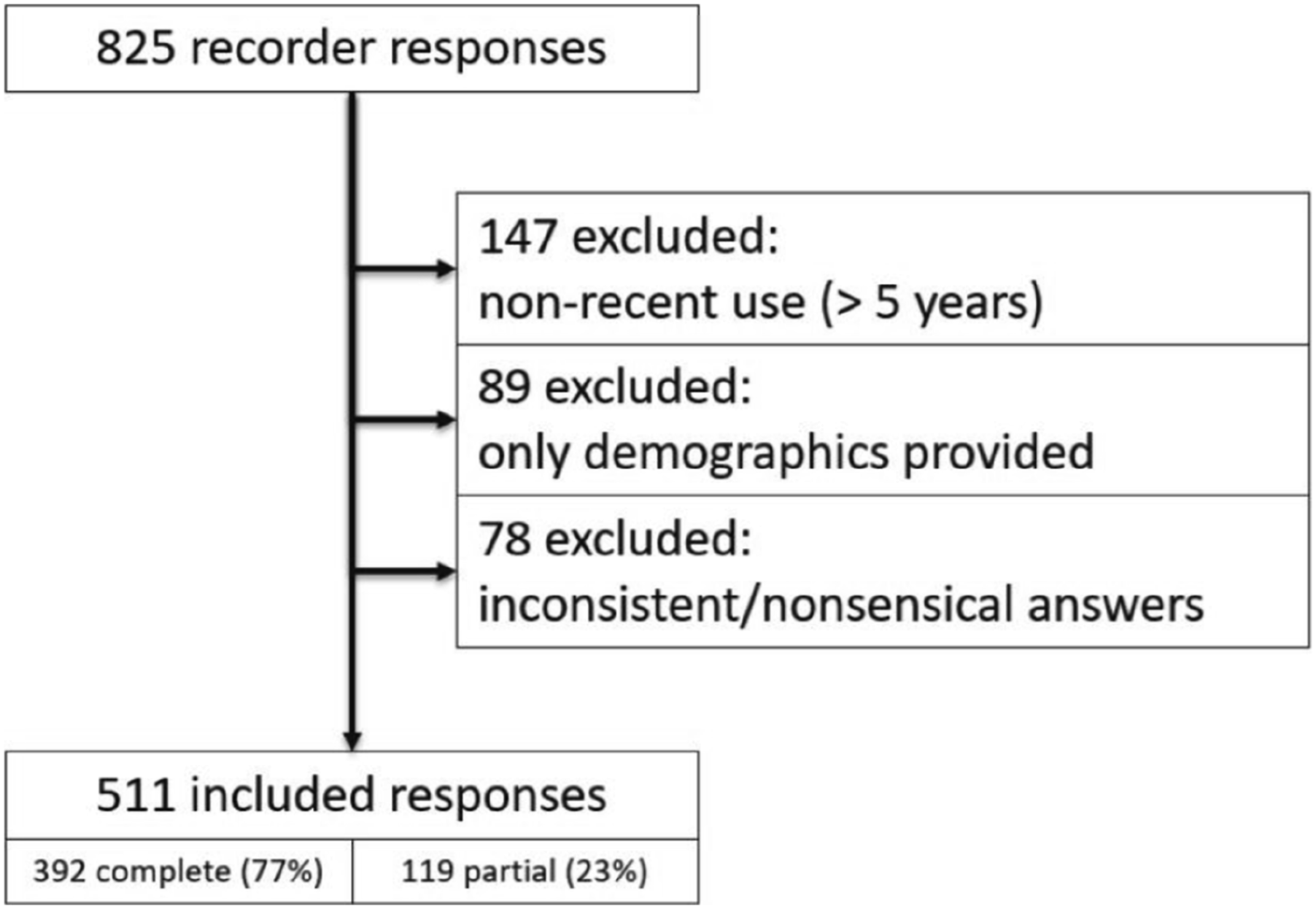
Respondent Demographics and Frequency of Recreational N2O Use
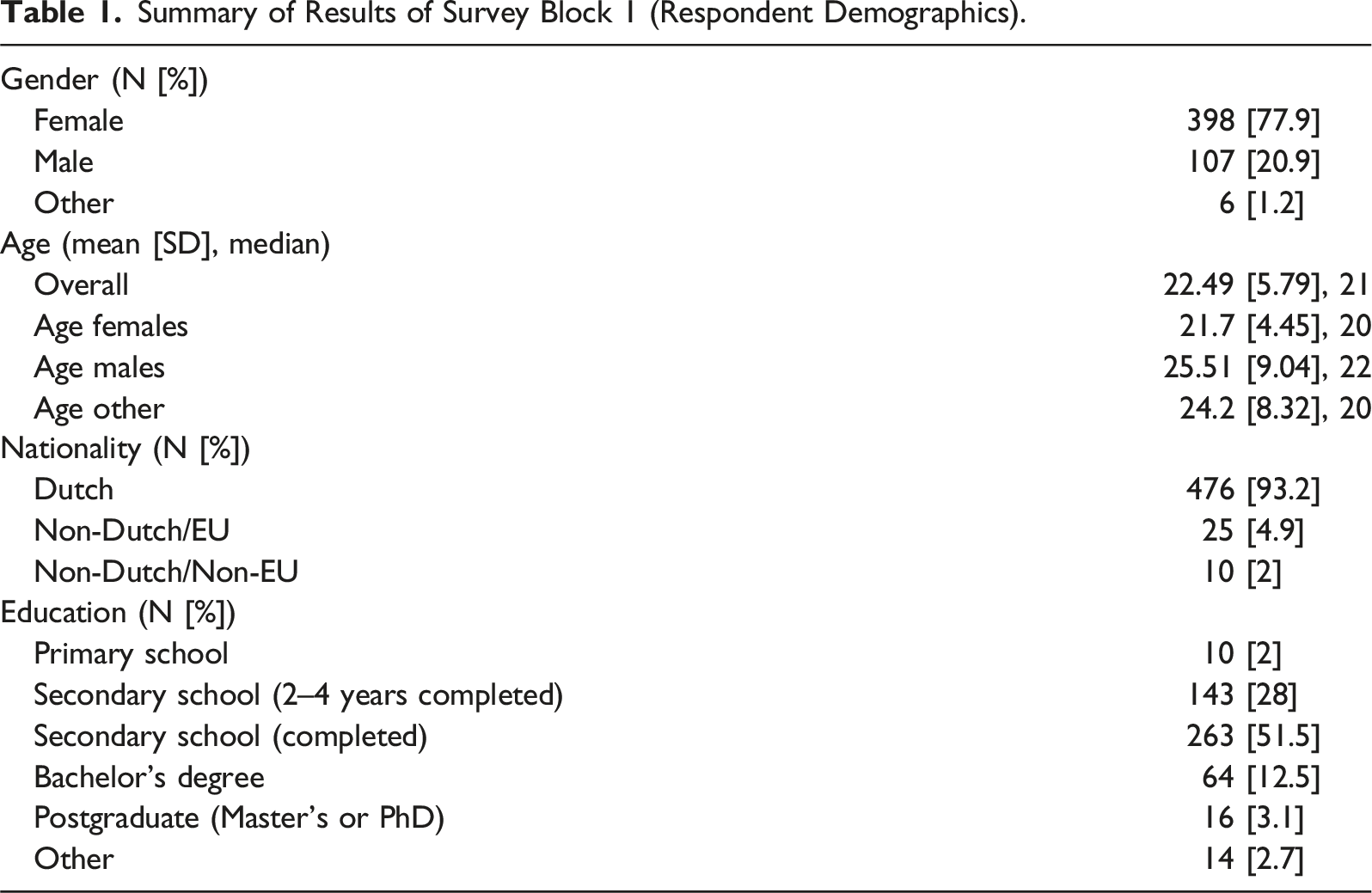
Summary of Results of Survey Block 1 (Respondent Demographics).
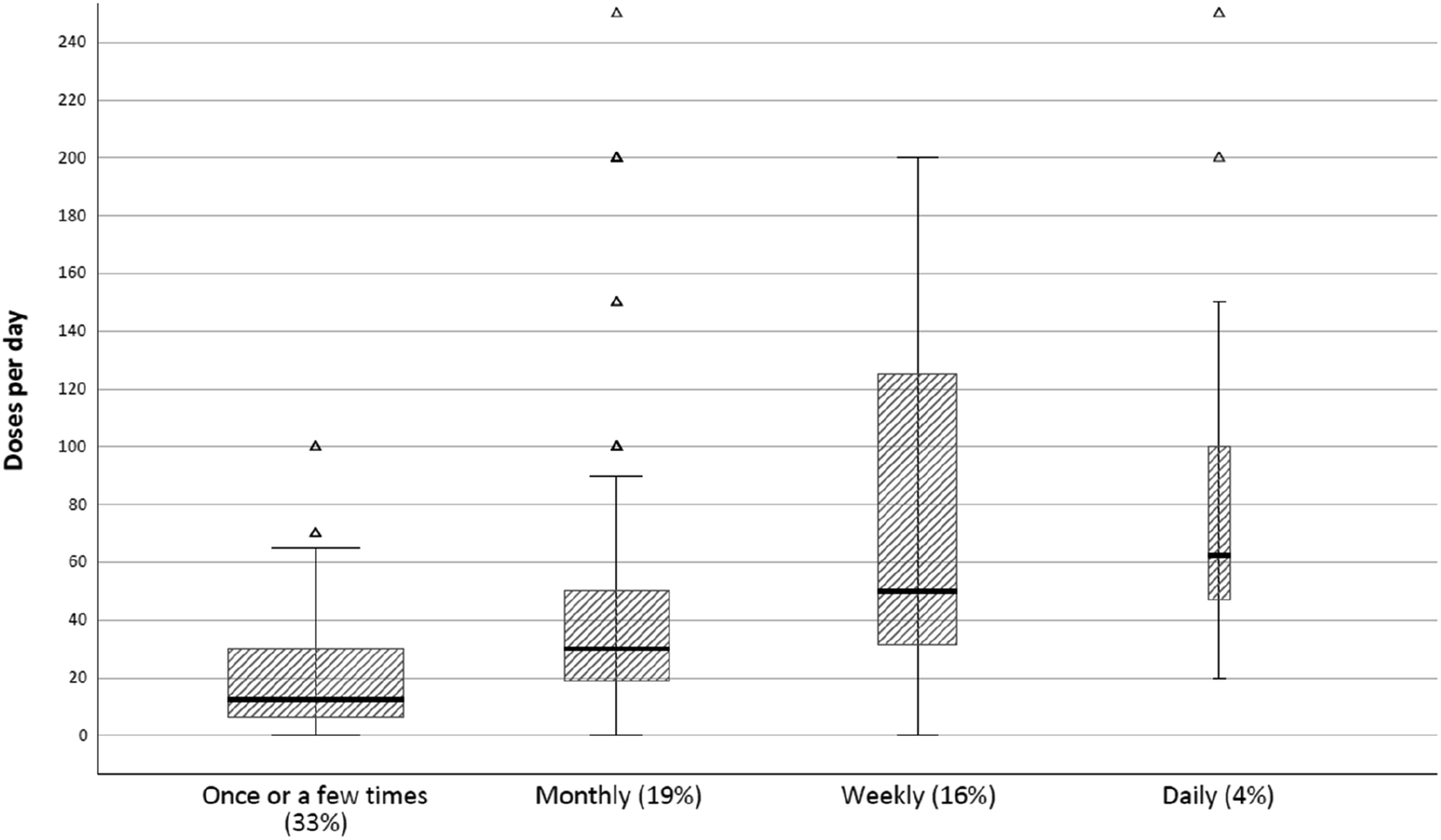
Number of N2O doses/balloon/trips (irrespective of volume) reported to be used per day of recreational N2O use by frequency of use (during previous year). The proportion of respondents in each frequency group is listed underneath the x-axis and is further illustrated by the width of the respective boxplot. Participants who did not use N2O during previous year are not included since they were not presented with item 13 (i.e. doses per day of use), hence total in figure does not amount to 100%.
Regarding education (item 4), the generally young age of the sample implies that many respondents were too young (i.e. < 21 years) to have completed a higher education. A Chi-square test revealed no significant difference in the completion of higher education (i.e., bachelor’s or postgraduate degree) between male and female respondents aged 21 years or older (χ2 (2, N = 266) = 0.08, p = .78). Likewise, there was no significant difference in the number of respondents who completed their secondary education by age 19 between males and females (χ2 (2, N = 171) = 1.82, p = .17).
Overall, the majority of respondents (N = 369, 72.2%) indicated to have used N2O in the previous year, while the rest (N = 142, 27.8%) indicated to have done so more than 1 year but less than 5 years ago (item 7). One hundred sixty-six respondents (32.5%) indicated to have used N2O only once or a few times during the previous year. In addition, 99 (19.4%), 80 (15.7%), and 22 (4.3%) respondents indicated to use N2O on a monthly, weekly, or daily basis, respectively (item 8) Figure 1.
Overall, the number of doses per day of use was severely right skewed because of several extreme outliers. Daily users reported using a median of 62.5 doses, irrespective of volume, per day (M = 96, SD = 74.79, N = 20; item 9). Weekly users reported using a median of 50 doses per day on which N2O was used recreationally (M = 161.06, SD = 325.48, N = 75; item 13), and a mean of 2.03 days of use per week (SD = 0.98, N = 80; item 10). Monthly users reported a mean of 4.33 days (SD = 4.45, N = 99; item 11) of N2O use per month, with a median of 30 doses per day of recreational N2O use (M = 50.07, SD = 58.18, N = 97; item 13). Finally, occasional users (once or a few times during the previous year) reported an average of 9.96 days of N2O per year (SD = 11.85, N = 164; item 12). During each day of N2O use, these users reported to consume a median of 12.5 doses of N2O (M = 20.86, SD = 19.62, N = 164) per day of recreational N2O use (item 13). Number of doses used per day of N2O use and number of days of N2O use were not documented for respondents who indicated not to have used N2O during the last year as they were directly forwarded to item 14. Figure 2 illustrates the number of N2O doses reported per day on which recreational N2O was used per frequency group.
Overall, the mean number of days of N2O use per year, derived from number of days per week, month, and year, was 63.69 days (SD = 92.35, median = 24, N = 365). On each day, the average reported number of doses (volume not defined) used was 59.92 (SD = 150.65, median = 29.5, N = 356). There was a significant correlation between the frequency of N2O use and the number of N2O doses used per day of use (r (353) = .57, p < .001). This suggests that when N2O use habits escalate, they do so both in frequency of use as well as in volume of N2O used per occasion Figure 3.
An independent samples t test did not provide evidence for a difference in number of days of N2O use per year between female (M = 1.39, SD = 0.65) and male respondents (M = 1.33, SD = .61, t (348) = 0.632, p = .53), nor regarding number of doses used per day of N2O use between males (M = 1.35, SD = 0.61) and females (M = 1.43, SD = 0.51, t (348) = 1.107, p = .27).
Next, potential differences in days of N2O use per year and doses per day of use across education levels were examined. Because of the small number of respondents who only completed primary school education (N = 10) or a postgraduate degree (N = 16), these groups were joined with the group who completed the first 2–4 years of secondary school (N = 143) and people who obtained a bachelor’s degree (N = 64), respectively. Respondents who’s educational status was unknown (N = 15) were excluded from an ANOVA which did not provide statistical evidence for a mean difference across education level in number of days of N2O use per year (log transformed) (F (2,353) = 2.3, p = .10), or regarding number of doses per day of N2O use (F (2,344) = 1.07, p = .35).
When asked whether their N2O use had changed since the start of the coronavirus pandemic (i.e., March 2020; item 14), 247 (48.3%) respondents indicated that they did not change their N2O use, 104 (20.3%) indicated to use less N2O, and 160 (31.3%) indicated to use more N2O than before. On average, respondents who reduced their N2O use since the start of the pandemic, reported a decrease of 2.56 days of use per year (SD = 38.55, median = 4, N = 104) and a mean reduction of 16 doses (volume not specified) per day of use (SD = 57.72, median = 2, N = 103). Respondents who increased N2O use since the start of the pandemic reported an average increase of 80.18 days of use per year (SD = 106.61, median = 38, N = 143) and an increase of 56.28 doses (SD = 176.63, median = 20, N = 157) per day of use.
Dosing and Method of Administration
The vast majority of respondents (N = 490, 95.9%) indicated to inhale N2O from a balloon as their most frequent method of inhalation (item 21). An additional 5 respondents (1%) indicated to use nitrous oxide from a whipped cream dispenser (i.e. usually a metal flask in which an 8 g canister N2O is released to pressurize). The final 16 respondents (3.1%) indicated to use N2O in a different way, however did not provide particularly informative descriptions of their alternative method (e.g., “in all possible ways”). (a) Boxplots illustrating the number of inhalations from a N2O filled balloon by inhalation technique. The proportion of respondents reporting to mainly use the respective technique is reported under the x-axis and is further illustrated by the width of the respective boxplot. Triangles indicate outliers according to 1.5 x IQR criterium. (b) Histogram displaying the reported total number of inhalation repetitions from a N2O filled balloon (irrespective of volume) over all inhalation techniques. The median (black) and mean (red) with 95% confidence interval (dotted lines) are visualized in the graph. (c) Histogram of the reported estimates of the duration of the breaks for respondents indicating to use the intermittent rebreathing technique The median (black) and mean (red) with 95% confidence interval (dotted lines) are visualized in the graph. (d) Histogram of the number of cycles reported to be completed before taking a break by respondents indicating to use the intermittent rebreathing technique. The median (black) and mean (red) with 95% confidence interval (dotted lines) are visualized in the graph.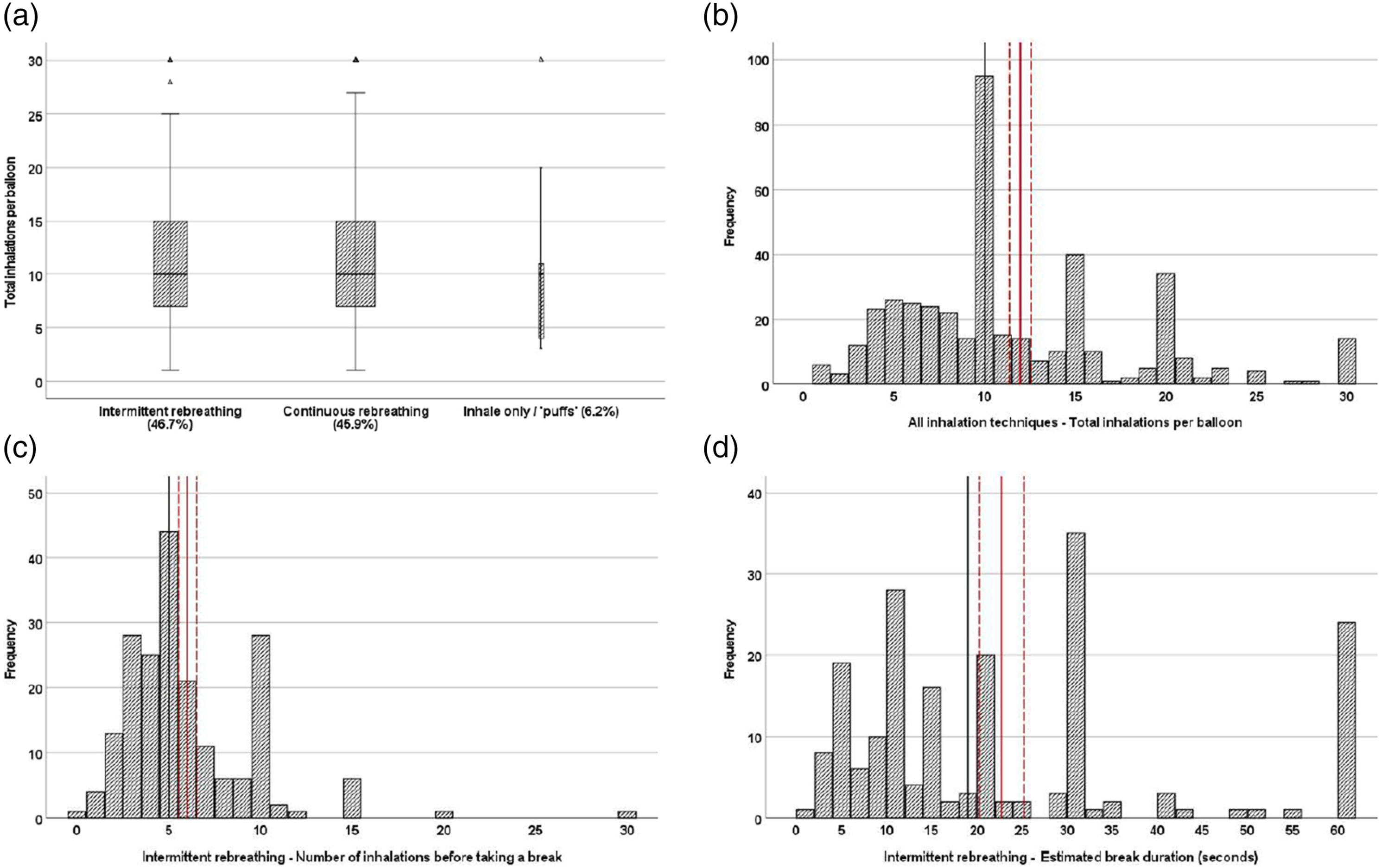
Of the respondents who indicated to inhale N2O from a balloon, most (46.7%) said they use an inhalation technique which involves repeatedly inhaling from a balloon followed by exhaling back into the balloon (hence “rebreathing” exhaled air; item 22) taking a break every 6 cycles (SD = 3.65, median = 5, N = 198) (1 cycle = 1 inhalation and 1 exhalation; item 23) for an estimated average duration of 22.75 seconds (SD = 17.53, median = 19, N = 193; item 24) before continuing to inhale N2O from the balloon. This group of respondents reported to complete an average of 12.11 cycles (SD = 6.51, median = 10, N = 210) in total per balloon (item 25). In addition, 45.9% of respondents who answered to mainly inhale N2O from a balloon, indicated to use the same “rebreathing” technique but without taking breaks (item 22). This group estimated to complete an average of 11.25 cycles (SD = 6.29, median = 10, N = 185) per balloon (item 25). Another 6.2% indicated to take puffs, without exhaling back into the balloon (item 22), with an estimated average of 9.61 puffs (SD = 5.92, median = 10, N = 28) per balloon (item 26). A final 6 participants (1.2%) responded that they used a different inhalation method (item 22), further specifying that they either used various methods (N = 2), they only used N2O once and can’t remember exactly (N = 1), only inhale once (N = 2), or inhale from the balloon via the mouth but exhale through the nose (N = 1).
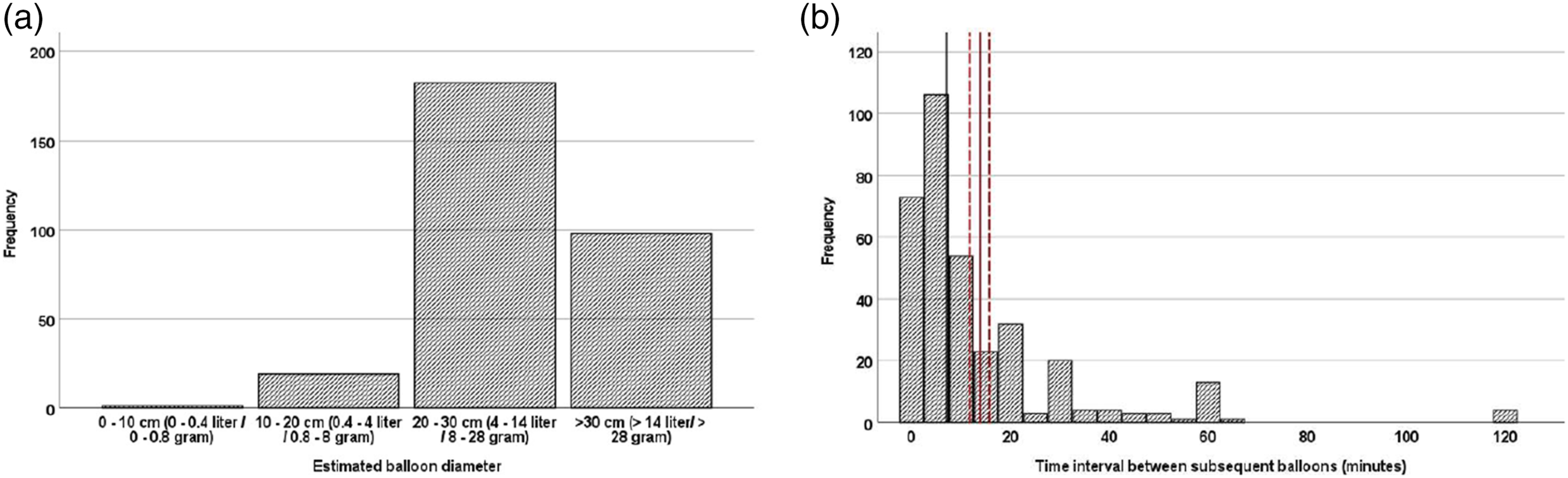
Most respondents inhaling from balloons indicated to continue until they noticed any (light) subjective intoxicating effects (32.5%) or moderate to strong effects (35.8%; item 32). Another 16.6% said to continue inhaling until they were unable to continue the process and/or because of being unable to stand or sit upright. A minority (3%) of respondents indicated to continue until they lost consciousness. Seven percent of respondents said to stop after a fixed number of inhalations (M = 4.53, SD = 2.11). A final 5% selected the “different” option and specified to continue until the balloon was empty, or provided an uninformative answer (e.g. “until I am out of the space”). Bar chart illustrating the proportions of chosen point of discontinuation of N2O inhalation by preferred inhalation technique. Of note is that continuous rebreathers appear to prefer higher levels of intoxication before discontinuing inhalation. (a) Estimates of N2O volumes in inhaled balloons based on reported estimates of balloon diameter. Estimates made based on conception of balloon as an orb, disregarding its elastic properties and under normobaric (sea-level air pressure) circumstances. (b) Histogram of the reported time usually left between subsequent N2O balloons in minutes. The median (black) and mean (red) with 95% confidence interval (dotted lines) are visualized in the graph.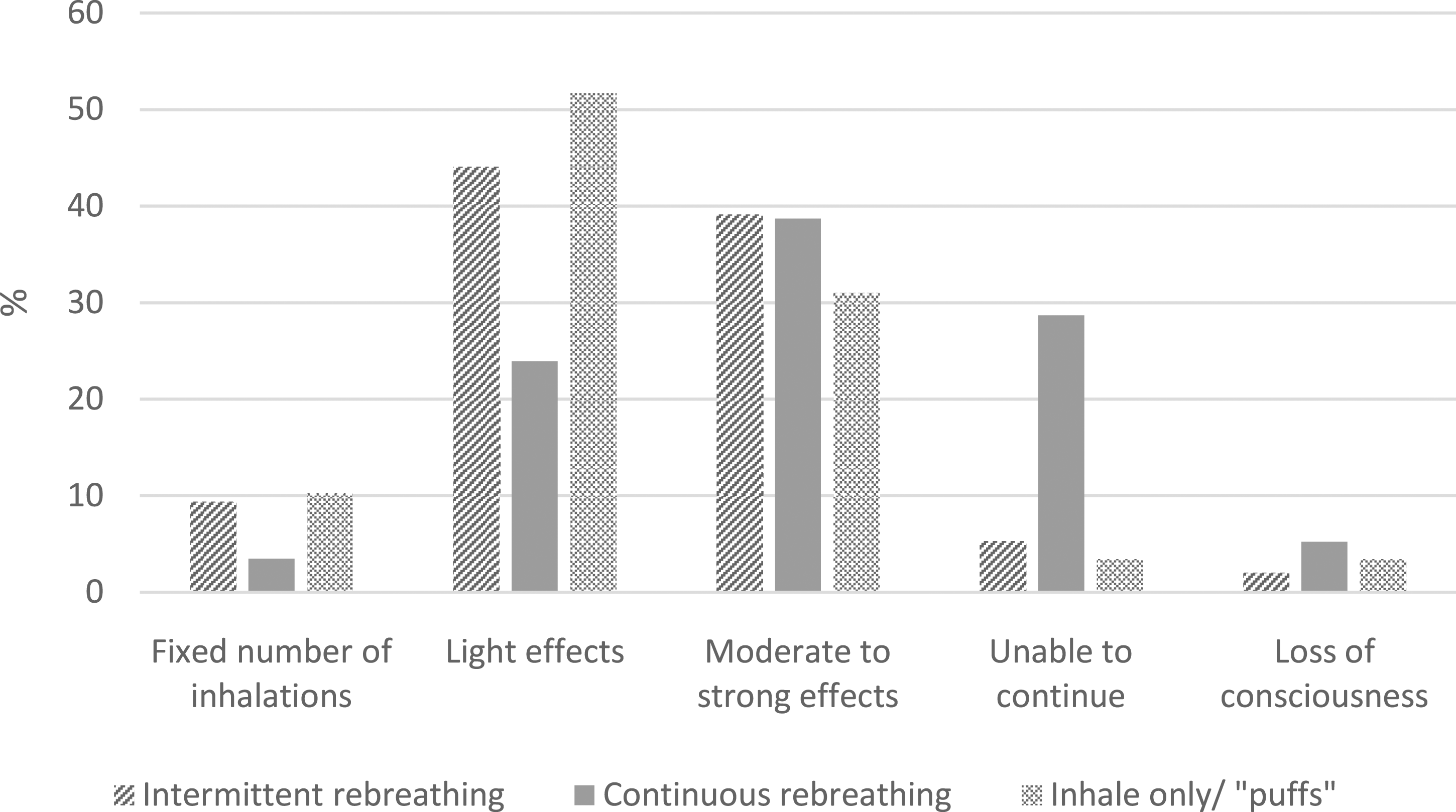
A comparison of the preferred point of discontinuation of inhalation (item 32) per inhalation method (item 22) uncovered a statistically significant association between these variables (χ2 (8, N = 437) = 73.62, p < .001). Specifically, it appears that users applying the “continuous rebreathing” technique more often continue until they notice moderate to strong effects, or until they are no longer physically able to continue compared to users applying the “intermittent rebreathing” technique or those taking “puffs”.
When asked about the medium used for filling a balloon with N2O, 82.9% (N = 353) answered that balloons were generally filled by directly fitting a balloon to a large cylindrical container (item 27). Of these respondents, 73.9% stated to estimate the volume of the balloon on sight (item 29), 4.5% claimed to have a precise method to determine the volume, and 2.5% indicated they had another way. A closer inspection of the open answers to item 29 of the latter two groups revealed that neither had a precise method for volume determination, but also estimated the volume on sight. However, in contrast to the first group, the latter two appeared to attempt to fill the balloon as much as possible (e.g. “until it nearly bursts”), as deducted from the answers of the former two groups to item 30 (i.e. estimated size of balloon).
Together with respondents who indicated uncertainty about how the balloons they inhaled from were generally filled (e.g. filled by another person, N = 28), the respondents who indicated to fill their balloon from a large cylinder were asked to estimate the diameter of the balloons they generally inhaled from (item 30). In total, 344 respondents answered this item, with about 0.6% indicating that their balloons usually had a diameter of 0–10 cm, which would roughly correspond to a volume of up to 0.5 L of N20 under normobaric circumstances (conceiving a balloon as an orb and disregarding slightly higher pressure inside balloon due to elastic properties). Another 6.1% of the respondents estimated their balloons to be 10 – 20 cm in diameter (0.5 L–4L of N20). The majority of respondents (61.6%) estimated their balloons to have a diameter between 20 – 30 cm (4 L–14 L). A final 31.7% estimated their balloons to generally have a diameter larger than 30 cm.
Apart from filling balloons from a large cylinder, 8.4% (N = 36) indicated to use small metal canisters (a.k.a. “Whippits” or “nangs”) to inflate their balloons with N2O. Each canister contains about 4L of N2O when released (van Amsterdam et al., 2015). Of these respondents, 21 (58.3%) indicated to only use one canister per balloon, while 11 respondents (30.5%) stated to use two canisters per balloon (item 28). Three more participants (8.3%) said to use 4 canisters per balloon. One answer was missing.
Answers to the question (N = 489) of how many doses (i.e. balloons) were typically used per sitting yielded a right skewed distribution. The upper limit was set at 50 doses. About 21.6% of the respondents indicated to use 50 doses per sitting. Because the follow-up option to specify how many doses were used was not displayed properly to the respondents, it is unclear whether these participants used more than 50 doses but indicated the highest possible option, or generally use around 50 doses per sitting. The 25th, 50th, and 75th percentiles indicated to use ≤6, ≤18, and ≤40 doses per sitting respectively.
Only 19 out of 489 respondents who answered item 33 (doses/balloons per occasion), stated to use only one dosing of N2O per sitting. Hence, the vast majority of users use multiple balloons per sitting. The follow-up item, that is item34, asking for the time between subsequent doses was answered by 461 respondents of which 90% stated they usually inhaled a second dose within 2 hours after the previous one. More specifically, the average time between subsequent doses in this group was 13.53 minutes (SD = 17.74, median = 7, N = 392).
Recreational N2O Use in Relation to Traffic Participation
Of the 463 respondents who completed block 4, 177 stated not possessing a valid driver’s license and 286 said they did (item 36). Of the latter, 26.9% said to have their license for less than 2 years, 42.7% for 2–5 years, and 30% for more than 5 years (item 37). Interestingly, more respondents (N = 298) reported to regularly drive a car than those stating to be in possession of a valid driver’s license. Three respondents clarified that they drove a car during their driving lessons; the rest did not provide an explanation about the circumstances under which they regularly drive without a valid license. The majority of respondents (N = 238, 79.9%) indicated to drive on a daily basis, 46 (15.4%) weekly, 10 (3.4%) monthly, and 1 participant indicated to drive only a few times per year (item 38). Participants who answered to never drive (N = 157, mainly respondents without a valid driver’s license) were hereafter directed to the end of the questionnaire Figure 4. (a) Probability estimates and 95% confidence intervals of admitting to having inhaled N2O while driving on a public road by gender. (b) Probability estimates and 95% confidence intervals of admitting to having inhaled N2O while driving on a public road by frequency of use.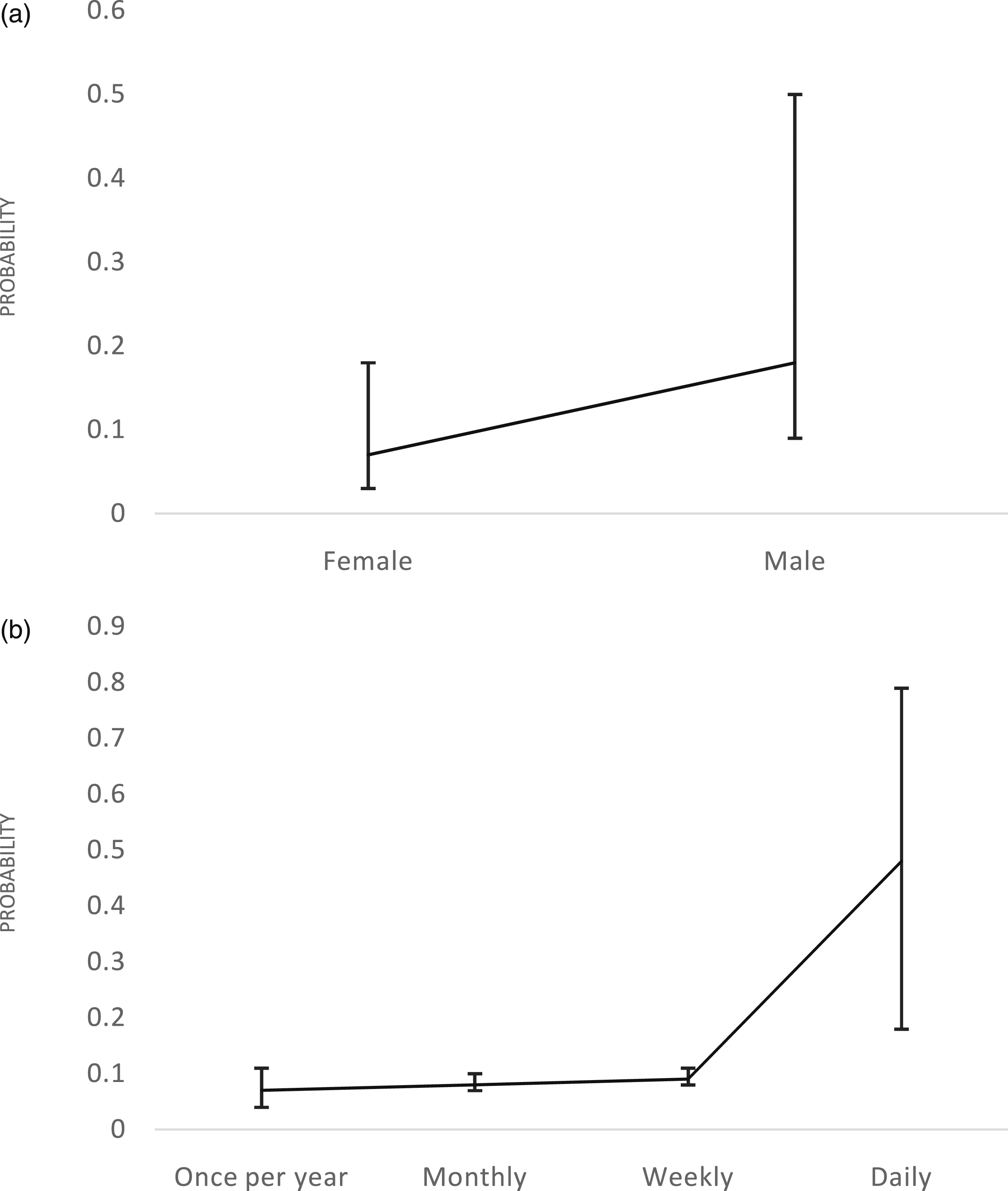
Of the remaining respondents 290 answered item 39, asking whether they ever operated a vehicle on a public road while using nitrous oxide, 30 (10.3%) admitted to have done so in the past. Of these respondents, 7 claimed to do so daily, 2 weekly, 2 monthly, 2 a few times per year, and 14 claimed to not do this regularly but to have done so in the past (ranging from 1 to 7 times; item 40). Nineteen respondents stated that the last instance occurred less than one year ago, and 8 said to have done so more than one year ago (item 41). A subsequent binary logistic regression showed that days of use per year (B = 0.006, SE = 0.002, Wald = 12.827, p < .001), sex (B = 1.129, SE = 0.424, Wald = 7.088, p = .008), but not educational level (B = −0.06, SE = 0.216, Wald = 0.078, p = .781) significantly predicted previous instances of driving while using N2O (χ2 = 17.719, df = 3, p = .001). The odds of male respondents for admitting to have used N2O while driving was estimated to be three times greater than those of female respondents (OR = 3.093, 95%CI [1.347, 7.103]. The odds ratio associated with days of N2O use per year was 1.006 (95%CI [1.003, 1.010], indicating that self-reported frequency of N2O use is significantly and positively associated with self-reported driving under the influence of N2O. Figure 5 depicts the estimated probability of admitting to having used N2O while driving for the predictors sex and frequency of use. Histogram of the reported time (minutes) between last N2O inhalation and driving departure for those respondents who stated to sometimes use N2O less than 2 hours before driving. The median (black) and mean (red) with 95% confidence interval (dotted lines) are visualized in the graph.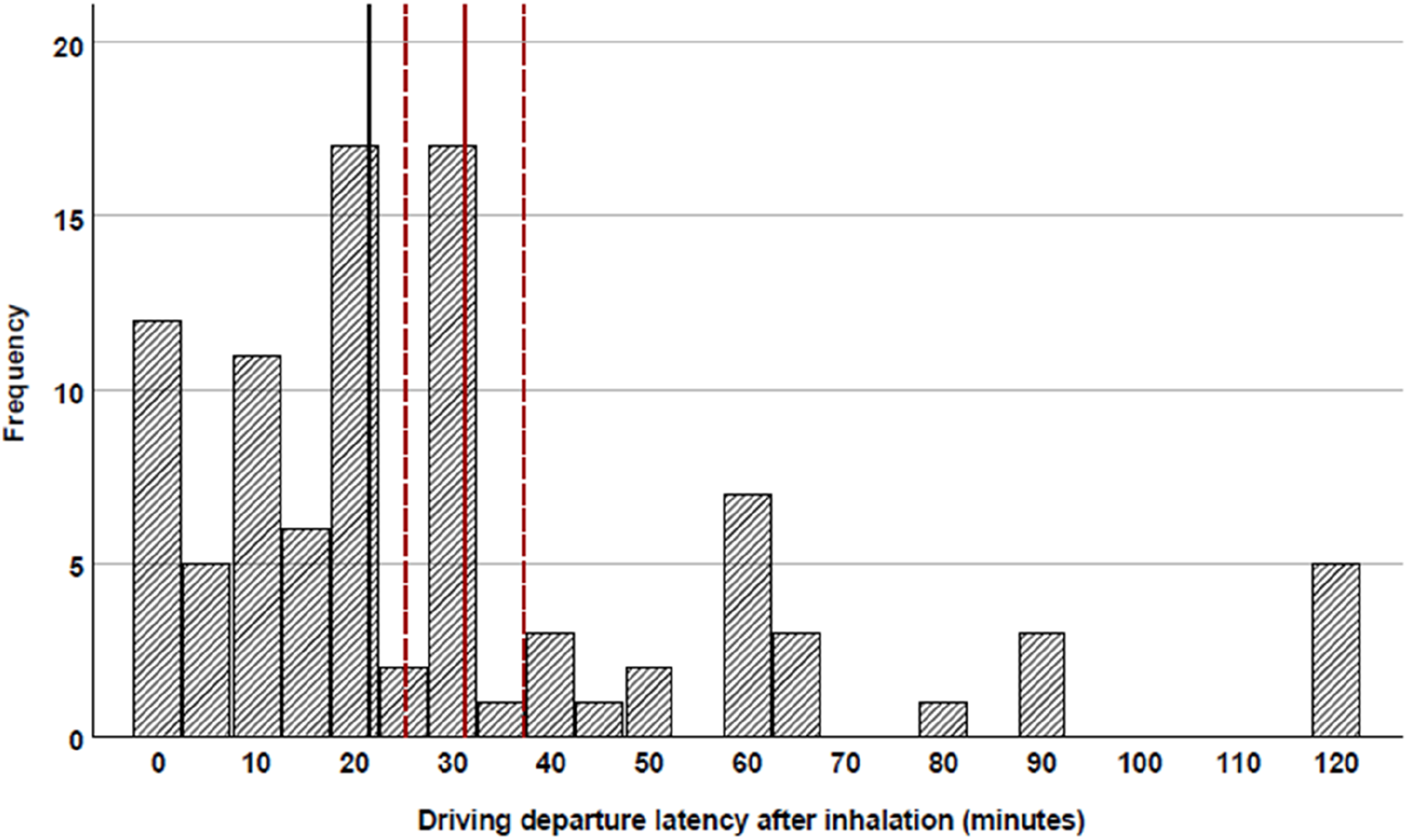
One-hundred eight out of 295 respondents (36.6%) indicated that they sometimes used N2O less than 2 hours before driving (item 42). The average reported time between inhalation and departure was 29.64 minutes (SD = 29.11, median = 21; item 43). It is clear from Figure 6 that the majority of respondents to this item (85.4%) estimate to wait for about an hour or less before departing after N2O use. Twenty-five of the 107 respondents (23.4%) to item 44 stated to use N2O mainly in a car. Over half of these respondents (N = 15) said they always or mostly did so with others (item 46). Only 2 respondents who reported to mainly use N2O in their car stated to always or usually open the windows of the vehicle while doing so (item 45) Figure 7.
Finally, 87 of the 292 respondents (29.8%) to item 47 indicated that their passengers sometimes use N2O shortly before (<2 hours) or while they were driving, without the respondents joining in the use. Of these respondents, only 19 (21.8%) stated to always or most often open a window when this occurred (item 48).
Discussion
The primary objective of the presented survey was to identify the most common dosing and administration methods of recreational N2O use. The results show that the vast majority of recreational N2O users inhale the gas from an N2O-filled balloon. These balloons are usually filled by fitting a balloon to a metal cylinder containing up to several kilograms of compressed N20. Dosing was never reported to be done in a precise way. Instead, the volume of the balloon was mainly reported to be estimated on sight. The usual diameter of the N2O filled balloons was estimated to be between 20 to 30 cm. Conceiving a balloon as an orb and disregarding its elastic properties, this diameter roughly corresponds to a volume of 4–14 L of N2O, which approximately corresponds to the content of 1–4 nitrous oxide containing metal canisters (a.k.a. whippits/bulbs/nangs). Most users reported inhaling multiple doses per sitting, ranging from 2 balloons to more than 50, although most people reported to use less than 50 balloons, and about half of the respondents indicated to use 18 balloons or less per sitting. About 90% of the respondents reported to leave less than 2 hours between two subsequent balloons, with an average break of 13.5 minutes (median of 7 minutes).
Most respondents indicated to use an inhalation technique which involves continuously inhaling from the balloon followed by exhaling back into the balloon, hence recycling their exhaled breath. About half of these respondents did so by taking a short break, with an average estimated duration of approximately 23 seconds, every 6 cycles (1 inhalation +1 exhalation = 1 cycle), completing an average total of 12 cycles. The other half continuously in- and exhaled from the balloon without breaks for an average of 11 cycles. Approximately one third of the respondents stopped inhaling whenever they felt any intoxicating effects. Another one-third continued until they perceived these effects as moderate to strong. A sizable minority, approximately one fifth, continued until they could no longer continue (due to signs of ataxia or shortness of breath), or until loss of consciousness.
Compared to previous reports (Hamans & Peters, 2019; van Amsterdam et al., 2015; Winstock et al., 2015), the prevalence of at-least-weekly users was significantly higher in the current sample (≈20% vs. 3%–4%). Also, the number of balloons per session was observed to be significantly higher than previous findings (Kaar et al., 2016; van Amsterdam et al., 2015; Winstock et al., 2015). Furthermore, the frequency of N2O use was found to positively correlate with number of balloons used per session, further confirming that the currently presented sample had a higher proportion of heavy N2O users instead of more frequent users of modest amounts of N2O per instance of use. These descripancies could be explained by sampling differences, that is large international sample (Kaar et al., 2016; Winstock et al., 2015) versus mostly Dutch sample in the current study, and 29% minors (Hamans & Peters, 2019) versus exclusively respondents aged 18+ to the current survey (albeit not verified other self-reported age). However, the possibility remains that heavy N2O use has increased in the Netherlands since these respective papers have been published. Indeed, an analysis of information inquiries made to the Dutch poison control center regarding N2O poisoning and/or N2O-abuse-induced peripheral neuropathy, showed an exponential increase in these inquiries starting from 2015 (van Riel et al., 2022). Also, in comparison to earlier reports, small metal canisters do no longer appear to be the most common source of recreational N2O. Instead, users now mostly inflate their balloons using larger cylindrical containers. The use of N2O containing cylinders has been assumed to be associated with heavier N2O use (van Amsterdam et al., 2015; van Riel et al., 2022).
The secondary objective of the present survey was to investigate the prevalence of recreational N2O use while driving on a public road, or shortly before. In the latter case, the goal was to map the average duration between inhalation and departure. Despite being in violation of Dutch traffic laws about impaired driving, about 1 in 10 of the respondents who indicated driving a car on a regular basis admitted to having used N2O while driving on a public road, of which one-third claimed to do so at least once a month. Seven out of these 30 respondents even stated to do so on a daily basis. In comparison to earlier findings (van Meer, 2020), the proportion respondents who admitted to have driven under the influence of N2O was found to be substantially lower (10% vs. 35%). A possible explanation for this discrepancy is that the survey by van Meer (2020) asked respondents about the use of N2O during “or” shortly before departure, while the current survey specifically asked about N2O use “during” driving. Another discrepancy with these prior findings is that gender was a significant predictor for driving while using N2O. Arguably, the same difference in phrasing, that is “during or shortly before driving” versus “during driving”, might have diluted the effect of sex in the survey by van Meer (2020). Overall, male drivers are consistently found to be more likely than females to drive under the influence of alcohol or other drugs (Lloyd et al., 2020; Navas et al., 2019; Robertson et al., 2017). Arguably, there is no apparent reason to assume that this general notion would not hold for driving under the influence of N2O. Under the assumption that males are indeed more likely to drive under the influence of N2O and provided that our sample consisted mainly (≈80%) of female respondents, the observed proportion of respondents who admitted to having used N2O while driving is arguably an underestimation. On the other hand, it should be noted that non-probability sampling methods employed in the current and aforementioned studies can lead to inflated prevalence estimates, which are not generalizable to the general population (Ganesh et al., 2017). Regardless, the sizable proportion that was found provides support the hypothesis that N2O contributes to the occurrence of road traffic accidents, as opposed to being mostly a coincidental finding at traffic accident sites.
One third of the drivers in the sample indicated to sometimes drive within 2 hours after having used N2O, with a mean delay of 29 minutes. One in four of these respondents indicated that in those instances they used N2O inside of a car. Unfortunately, the phrasing of the item does not allow specifying whether this happened in a driving or parked vehicle. Using N2O in a (parked) vehicle often occurs together with other users. Overall, the respondents did not appear concerned with ventilating the vehicle, as only two indicated to mostly or always open a windows or doors while using N2O in the vehicle. Also when the driver indicated not to use N2O themselves, but their passengers did, proper ventilation was generally not observed. Whether this practice can result in passive or prolonged intoxication remains to be investigated, however, this is not inconceivable within the confined space of a passenger car.
Conclusion
In the Netherlands, nitrous oxide is frequently used while or shortly before driving a car on a public road. These findings illustrate the relevance of further research into this phenomenon. Although the acute state of N2O intoxication is undoubtedly not reconcilable with the practice of safe and responsible driving, it remains to be determined if starting to drive a car soon after is still subject to impaired driving. Future research is needed to investigate these effects for up to at least 60 minutes after N2O administration.
Based on the current findings, it is advised that experimental administration of N2O, aimed at simulating recreational use, should involve inhalation of undiluted N2O from a party balloon filled with 4–14 L. Participants should apply an inhalation technique which involves inhaling from the balloon and exhaling again into the balloon (re-inflate), before repeating. After ±6 cycles, participants should take a 20 – 30 seconds break before continuing inhalation. It is advisable to allow inhalation to continue for at least 12 cycles or until the desired subjective effects are experienced.
The results of this survey show that N2O is frequently inhaled inside parked vehicles. Furthermore, the obtained responses do not indicate that proper ventilation is a common concern for the occupants. Future research should elucidate whether this practice can lead to the accumulation of N2O within the confined space of the vehicle to the point where intoxicating or functionally impairing effects become apparent.
Footnotes
Acknowledgments
The authors would like to thank Trimbos Institute and TeamAlert for their valuable comments during the conceptual phase of the survey construction.
Author Contributions
All authors contributed significantly to the conception, execution, analysis, and/or writing of the presented study and the current manuscript. All authors consent with the publication of the manuscript in its current, submitted form.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the department of neuropsychology and psychopharmacology of the faculty of psychology and neuroscience of Maastricht University, the Netherlands.
Ethical Approval
Ethical review and approval for the study in the present manuscript was provided by Ethics Review Committee Psychology and Neuroscience (ERCPN) of the faculty of psychology and neuroscience of Maastricht University, the Netherlands (protocol: ERCPN 239_104_06_2021). All participants gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki.
Data Availability Statement
The data presented and discussed in the current manuscript are obtainable upon reasonable request to the corresponding author.