
Abstract
With the ongoing opioid epidemic, evidence-based interventions are needed to prevent and respond to opioid-related overdoses. Overdose prevention sites (OPS) have been operating effectively internationally since the 1980s. In the United States, despite unprecedented numbers of overdose-related deaths, only two sites operate in New York City. California, generally a beacon of progressive policy, has been unable to implement a sanctioned facility. Using two waves of survey data (2017 and 2022), this paper seeks to answer the following research questions: (1) Do CA voters support overdose prevention sites? (2) How has support changed over time? And, (3) What factors contribute to the support and opposition of these programs? Results reveal that most respondents would support an OPS in California, despite the recent veto of such measures by California Governor Newsom. Further analyses examine factors that contribute to both support and opposition, as well as exploring potential avenues for reform.
On August 22, 2022, California (CA) Governor Gavin Newson vetoed SB57, a CA Senate Bill that would have legalized overdose prevention sites in three cities in CA: San Francisco, Oakland, and Los Angeles. This was four years after then Governor Brown vetoed a similar 2018 bill that would have sanctioned these sites. Overdose prevention sites, also referred to as drug consumption sites or safe injection sites, are spaces where individuals can self-administer substances, either licit or illicit, under the supervision of trained medical staff (Kreit, 2019). These sites have been implemented all over the world since the 1980s and have had a demonstrable positive effect on overdose rates, engagement with services, crime reduction, and admittance into drug treatment programs (Kerr et al., 2017; Potier et al., 2014). Specifically, these sites reduce drug-related overdose, infection, and disease and increase access to quality-of-life services and drug treatment (Lofaro & Miller, 2021). Overall, they reduce public health and public safety concerns related to substance use (Wenger et al., 2011). San Francisco, Oakland, and Los Angeles would have been the first sanctioned sites in the United States.
Social activists have a long history of impacting politics (Amenta, 2010; Levy & Mattsson, 2023). President Obama in 2015 was the first U.S. President to advocate for harm reduction, citing the Harm Reduction Coalition and other harm reduction activism groups (Nadelmann & LaSalle, 2017; The White House, 2015). Overdose prevention sites entered the discourse among United States 1 legislators by harm reduction activist groups who offered potential solutions to the opioid epidemic and its high overdose rates. In 2021, New York City became the first city in the United States, and the second in North America (following Canada’s first site in 2003), to authorize safe injection sites in both the Washington Heights and East Harlem neighborhoods (Mays & Newman, 2021). Other cities, like San Francisco, Los Angeles, and Philadelphia have been working towards opening similar sites but have been met with pushback and legal challenges, including Newsom’s veto of SB57. But, the question remains, do the legislators of CA (SB57) best represent the voters or do voters more align with Newsom?
While the literature has sufficiently demonstrated the efficacy of safe injection sites (e.g., Hathaway & Tousaw, 2008; Kappel et al., 2016; Ng et al., 2017; Pitpitan et al., 2016) and some studies have examined the legal and political challenges (e.g., Oliver et al., 2011; Whitford & Yates, 2009; Winstanley et al., 2016), very few studies have examined public perceptions (see Lange & Bach-Mortensen, 2019; Parham, 2018). Politicians have made unilateral decisions about the implementation of these programs in their respective states, without a clear understanding of public perceptions. The public could provide an alternative pathway to reform. Using two waves of California voter survey data, this paper fills that gap and provides a comparative quantitative analysis revealing changes in public attitudes in favor of implementing safe injection facilities in CA. These data show overall CA voters support these programs, and Gov. Newsom’s veto did not align with public opinion.
This paper starts by situating our study within a historical overview of overdose prevention sites both internationally and in the United States and briefly explores the legal and political barriers to implementing these programs in the United States. Studies on public perceptions of harm reduction measures and drug policy are included in this discussion. We then describe the methods, analyses, and results, and end with implications and future avenues of research.
Harm Reduction Programs
Harm reduction measures in the United States, while controversial, are not new. Harm reduction is a practical approach to drug use that aims to reduce the potential negative consequences, such as overdose, infection, and the transmission of blood-borne diseases. It primarily operates in opposition to abstention – although abstention can be defined as one method of harm reduction (Riley & O’Hare, 2000). The earliest form of harm reduction in practice occurred in New York City in the 1960s. Following a rise in overdose deaths in New York City at the time, physicians began prescribing methadone as opioid-replacement therapy to prevent overdoses (Green et al., 2004; Payte, 1991). A few decades later, harm reduction in the United States expanded during the AIDS epidemic in the 1980s. With the rise of HIV/AIDS primarily affecting men who have sex with men (MSM) and those who inject drugs, grassroots activists sought tools to reduce transmission and drug-related mortality. Advocacy and education around ways to transmit as well as harm reduction measures, such as condom distribution and syringe exchange programs, developed.
Syringe exchange programs (SEPs) provide sterile syringes and injection equipment, such as cotton, sterile water, cookers, and tourniquets to people who inject drugs (PWID) to prevent needle and equipment sharing and the potential transmission of blood borne diseases. Some SEPs have also begun to provide safe smoking equipment, such as glass pipes, foil, and filters, providing a safer avenue for people who smoke drugs (PWSD). These were the first harm reduction programs to be implemented in the United States and remain the only harm reduction measure currently legalized by state and federal governments.
Drug Consumption Sites
Drug consumption sites advance the philosophies, goals, and practices of syringe exchange programs. They provide safe injection and smoking equipment to participants, while also providing a space for people to consume their substances under the supervision of trained medical staff (Kent, 2001). These sites have rooms and private areas where individuals can smoke, inject, or otherwise ingest their substances. In the United States, the substances must be procured outside of the space and brought inside for use. Individuals can receive education and support in safe ingestion practices from staff members, such as finding veins and vein care, and overdose prevention tactics. Drug consumption sites prevent the transmission of blood borne disease and reduce infection rates (Kappel et al., 2016; Ng et al., 2017). A randomized controlled trial that examined injection risk intervention further supports these findings (Pitpitan et al., 2016).
One of the primary goals of these sites that sets them apart from SEPs is the focus on overdose prevention and reversal. By allowing individuals to use their substance under the supervision of medical staff, the risk of overdose is drastically reduced (Dupree et al., 2021; Hathaway & Tousaw, 2008; Kapel et al., 2016; Ng et al., 2017). Insite, the safe injection site in Vancouver, Canada, has had zero overdose deaths since their opening in 2003 (Vancouver Coastal Health, 2022).
In addition to decreased morbidity and mortality for people who use drugs (PWUDs), drug consumption sites have a net positive effect on public safety. Similar to SEPs, drug consumption sites reduce needle litter in their communities and have been documented to reduce public use and crime (Bayoumi & Zaric, 2008; Beletsky et al., 2008). This well-documented efficacy is also cost-effective (Bayoumi & Zaric, 2008; Dupree et al., 2021).
Despite this evidence, these sites are rare in North America and primarily operate in Europe, Australia, and Canada. Insite in Vancouver, Canada was the only safe injection site operating in North America for nearly 20 years. Bern, Switzerland opened the first safe injection site in 1986 (Kreit, 2019; Peters & Wittenberg, 2020), and similar sites have been operating successfully since. Various groups have attempted to open drug consumption sites in the United States – Los Angeles, San Francisco, Philadelphia, and even Minnesota, but only New York City has been successful so far (Kreit, 2019). The Minnesota state legislature recently approved $14 million for opiate overdose prevention and response (MN HF 2847, 2023), potentially including an overdose prevention site (OPS), though one has yet to be realized. In 2021, Rhode Island Governor McKee signed legislation permitting an OPS, and the Rhode Island Department of Health is currently working to open their first site (Rhode Island Department of Health, 2022). Still, the U.S. is quite behind – 40 years behind.
Barriers and Legal Challenges to Harm Reduction
Harm reduction programs have had well-documented success since their inception. They reduce morbidity associated with drug use, overdose deaths, needle litter, public use, and public nuisance. They also decrease crime and increase access to drug treatment, while costing less than traditional drug prevention and prohibition efforts. Why, then, are these programs not more widely implemented in the United States? The crux of this response lies in U.S. federal and state politicians’ staunch commitment to the War on Drugs, their federal legislative actions (Consolidated Appropriations Act of 2018, Anti-Drug Abuse Act of 1986), and funding policies and practices. Those efforts in addition to the stigma associated with drug use (Kreit, 2019), hegemonic abstinence-only view of both treatment and recovery, local law enforcement procedures, and public fear of PWUDs have historically impeded harm reduction programs in the U.S.
Political Opposition and War on Drugs
The opposition to harm reduction programs like overdose prevention sites dates as far back as the 1960s. Since Richard Nixon’s presidency, politicians have relied on the War on Drugs as a platform when running for office (Whitford & Yates, 2009). An analysis of presidential State of the Union addresses from 1946–2010 found that drug policy was a primary discussion point in most of the addresses, with spikes in focus during Nixon, Reagan, and George W. Bush (Oliver et al., 2011). Being tough on crime (i.e., promoting drug enforcement) and vehemently anti-drug (i.e., opposing funds for treatment or harm reduction) has generally been required for a successful election campaign and a favorable public opinion of a sitting president.
Even as public opinion shifts, politicians may still disfavor harm reduction policies because of special interest groups and political risk aversion. Jacobs and Shapiro (2000) argue that political leaders prioritize manipulating public opinion rather than responding to it (see also Barbera et al., 2019). Essentially, politicians set the agenda, often based on the needs of elite stakeholders and special interest groups (Bryson, 2004; Disch, 2012). As a result, federal and state politicians have enacted legislation that expand the War on Drugs and, in effect, bar the creation of, and federal funding for, harm reduction programs. Legislation on SEPs is prime example.
Federal Funding
While SEPs are sanctioned by their respective counties and states, resistance to harm reduction remains at the federal level. In 1988, Congress enacted section 300ee-5 of the Public Health and Welfare Act preventing federal funding for syringe exchange programs (42 U.S.C. 300ee-5, 1988). The law was renewed in 1990 as the Ryan White Care Act. While President Obama revised the law in the 2018 Consolidated Appropriations Act, federal funds can only be used for staff and operation costs. These funds cannot be used to purchase syringes or safe injection equipment to avoid inconsistencies with drug prohibition and enforcement (Consolidated Appropriations Act H.R. 1625, 2018). SCSs came next.
In March of 2022, Congresswoman Herrera Beutler (R-WA) introduced H.R. 7029, the Stop Injection Sites for Illegal Drugs Act of 2022. This law could cement the federal ban on SCSs by prohibiting federal funds to be provided to states that operate an unlawful injection site. While the language of the bill is non-specific, it implies any federal funding would be proscribed except for that which is used for criminal legal system programs (e.g., Community Oriented Policing Services grant and Byrne grant). Beutler’s bill argues that SCSs are in violation of the Crack House Statute, 2 which is part of 1986 federal legislation enacted at the height of the drug war.
Legislation: Crack House Statute
As part of the Anti-Drug Abuse Act of 1986, Congress passed 21 U.S.C. S856, colloquially referred to as the Crack House Statute. This statute prohibits the maintenance of premises where drugs are manufactured, sold, and most critically for safe consumption sites, used. Although staff members of drug consumption sites would not possess or distribute the drugs, operating a space that allows drug use inside is a direct violation of this statute. President Trump’s Department of Justice filed the lawsuit against a Philadelphia non-profit in 2019 for attempting to open a supervised injection facility in their community (Leonard, 2019) based on this statute. The DOJ won.
Despite approval from state legislative bodies, both CA Governors Newsom and Brown vetoed bills that would have sanctioned safe injection facilities. Similarly in Vermont in 2022, where overdose rates continue to increase dramatically, Governor Phil Scott vetoed House Bill 728. This bill would have allowed an Overdose Prevention Site Working Group to begin research on overdose prevention sites and move toward the implementation of one. In May of 2023, the Pennsylvania Senate approved a ban on safe injection facilities (McGoldrick & Whelan, 2023). It will be signed by PA Governor Shapiro who stated his opposition to safe injection sites on the record (Whelan, 2022). These legislators are praised by local groups, colloquially referred to as NIMBYs, who oppose the implementation of similar facilities in their local communities.
NIMBYism
NIMBYism, or “not in my backyard”, is a colloquial reference to the socio-spatial stigmatizing of marginalized groups based on real fears of residents living in affected areas (Tempalski et al., 2007). NIMBYism is prevalent when discussing facilities for people who are unhoused, with mental health disorders, with HIV/AIDS, or with a history (no matter how short or long) of criminal activity (see Dear et al., 1997; Law, 2003; Law & Takahashi, 2000; Lyon-Callo, 2001). Facilities for PWUDs – particularly those that provide harm reduction services – have also been blocked or shut down by local NIMBYists (Daker-White, 1997; Tempalski et al., 2007). The Orange County Needle Exchange Program (OCNEP), the only needle exchange operating in Orange County, CA, is one example.
The OCNEP was shut down in 2018 after only two years of operation, despite support from the California Department of Public Health (OCNEP, 2023). While opponents cited increased needle litter as the reason for the injunction – a legitimate concern – the driving force was negative public opinion (OCNEP, 2023). Now, PWUD in Orange County, CA can no longer access services in their county. OCNEP is currently attempting to get their approval from the California Department of Public Health reinstated – however – public pushback there is strong. OCNEP will need to garner support from stakeholders and other constituencies.
Support of Harm Reduction
Harm reduction programs, including overdose prevention sites (OPS), have garnered support from a diverse range of stakeholders, reflecting the growing recognition of their effectiveness in addressing substance use-related harms. Public health experts, community organizations, and affected populations alike have voiced their support for these initiatives. In both a Philadelphia (Javadi et al., 2022) and a general public (Bonar & Rosenberg, 2010) study, substance use professionals had widespread support of harm reduction strategies. Another Philadelphia study, where an overdose prevention site was proposed, also found overwhelming support for the initiative, especially among residents experiencing unstable housing and those with a history of substance use (Roth et al., 2019).
Public support for harm reduction typically varies based on demographic identities and political ideologies. For example, public support for federal funding of harm reduction strategies was strong among older individuals, males, those with liberal political ideologies, and those who advocate for help rather than punishment for PWID based on a nationwide survey of U.S. adults by Kulesza et al. (2015). Queer individuals have been at the forefront of harm reduction advocacy since the AIDS epidemic, continuing to be strong supporters of harm reduction initiatives (Hassan, 2022). Their early engagement with harm reduction reflects a commitment to compassionate and evidence-based approaches to addressing substance use-related harms. This is in contrast to those who are less knowledgeable about the efficacy of harm reduction efforts. One study on community perspectives of harm reduction programs in San Francisco’s Tenderloin district showed many were concerned about program effectiveness and the potential for public disorder (Wenger et al., 2011). And yet, they were open to a dialogue on the benefits of safe injection sites, showing the potential for swaying public opinion.
Public Opinion and Drug Policy Reform
Shifting public opinion has been the driving force for drug policy reforms for decades (VanderWaal et al., 2006). Cannabis medicalization and legalization in the U.S. are prime examples (Schaeffer, 2023). California was the first to legalize medical cannabis in 1996, which only occurred because of a shift in public attitudes toward marijuana (Goldberg, 1996; Grossman, 2019). Prior to the legalization of medical cannabis through the Compassionate Use Act in 1996, Governor Pete Wilson twice vetoed similar legislation introduced by the California Legislature that would have legalized medical marijuana (Grossman, 2019). Following this veto, the public collected signatures to put the Compassionate Use Act on the ballot and ultimately won (Grossman, 2019). Since then, public perception of cannabis has continued to shift and liberalize, ultimately leading to the legalization of recreational use in California in 2016 through the passage of Proposition 64. Since, 22 other states, plus Washington D.C., Guam, Northern Mariana Islands, and the U.S. Virgin Islands have legalized cannabis for recreation use. Cannabis legalization in CA evidences the power of public opinion in shifting public policy in CA (Bonner, 2023).
Thus far, in cities debating the legalization of OPS, public opinion is mixed. Local business owners in San Francisco’s Tenderloin district in 2011 (over a decade ago) worried a site would exacerbate public disorder (Wenger et al., 2011). A 2021 study of business owners in Baltimore had similar findings, stressing the potential for public disorder and lack of efficacy (Dupree et al., 2021). Philadelphia was the only city that showed support for OPS (Roth et al., 2019), which was contingent on the success of the OPS in reducing overdoses and promoting public safety. None of these cities have been able to assess the impact of OPSs, as each still do not have a legally sanctioned OPS. In states with referendum systems, public opinion may significantly influence this complex landscape.
Present Study
Public opinion can institutionalize or block harm reduction programs, regardless of the documented successes of harm reduction programs internationally and within the United States. Given this, the present study seeks to answer the following research questions: (1) Do CA voters support overdose prevention sites? (2) How has support changed over time? And (3) What factors contribute to the support and opposition of these programs? Based on the relevant literature, we hypothesize that (1) CA voters will support overdose prevention sites; (2) Support will have increased over time; (3) Support will be strongest among Democratic voters and older individuals.
Data and Methods
The current study uses data from California Speaks Opinion Research (CALSPEAKS), a non-profit survey research institute at California State University, Sacramento (Barker et al., 2017). Data from two surveys administered across the state of California were used for analysis. The first survey took place in 2017 and the second in 2022. Both surveys were part of a larger panel design using probability-based sampling methods (CALSPEAKS, 2019).
The sample size for the 2017 survey was 815 respondents (representing 7,824,145 Californians when weighted), while the 2022 survey included 1057 respondents (representing 30,452,632 Californians when weighted). Both datasets were used to examine the first two research questions (“Do CA voters support…” & “How has support changed over time?”), but only the 2022 data were used to analyze factors that contribute to the support or opposition of the programs.
Description of Variables
Public perception of drug consumption sites was measured using a dichotomous variable that asked the respondent if they would support or oppose such facilities. The 2017 survey stated safe consumption/injection facilities/overdose prevention sites provide a space for drug users to consume/inject drugs under the supervision of medical staff. Proponents argue that these facilities reduce overdose-related deaths, infections, and the spread of diseases, and connect users to treatment programs. Opponents argue that these facilities enable drug use and fail to reduce crime.
It then asked, “Would you support/oppose a law allowing safe consumption/injection facilities in CA?” The 2022 survey asked, Overdose prevention sites provide a space for drug users to use drugs under the supervision of medical staff. Would you support/oppose a law allowing sites like these in California?
In both waves of data collection, the questions were differentially presented on various surveys to control for potential response style errors from survey respondents. For example, some surveys asked, “Would you support…” while others phrased the question “Would you oppose….” Thus, respondents were asked one of the following questions: 1) “Overdose prevention sites provide a space for drug users to use drugs under the supervision of medical staff. Would you SUPPORT a law allowing sites like these in California?” or 2) “Overdose prevention sites provide a space for drug users to use drugs under the supervision of medical staff. Would you OPPOSE a law allowing sites like these in California?” Respondents could respond ‘yes’ or ‘no’ to the question they were presented. All responses were then recoded into a single dichotomous variable (1 = support; 0 = don’t support) for the purpose of analysis. The survey changed the language in the 2022 survey to overdose prevention site to reflect the language being used in CA SB 57 and similar legislation.
Demographic, Drug Use, Trust in Government, & Political Party Affiliation Variables (2022 Data).
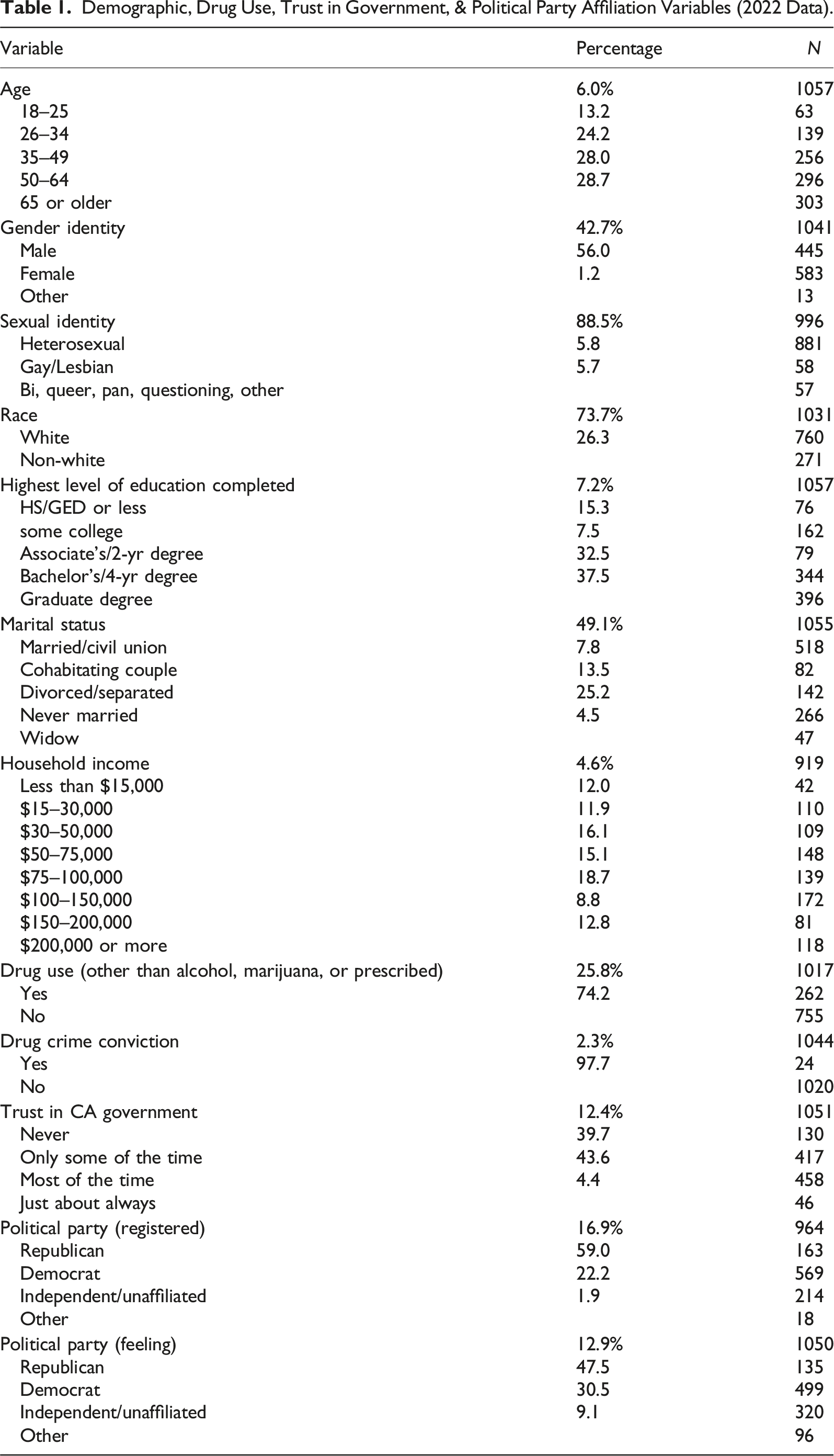
Sample Characteristics
The 2022 sample was primarily White (73.7%), heterosexual (88.5%), and reported low levels of drug use (25.8%) or drug-related criminal convictions [2.3% (see Table 1)]. A slight majority of respondents were 50 years or older (56.7%), and a similar percentage were female (56.0%). Almost half of the sample was married or currently in a civil union (49.0%). The sample was also relatively well educated, with 70% of respondents having earned a bachelor’s degree and/or graduate degree, while less than 10% of the sample had only earned a high school diploma or less. There was a good deal of variation in both household income and trust in California’s government. Finally, the largest political group represented in the sample was the Democratic Party (59.0% registered; 47.5% identifying).
The demographic characteristics of the 2022 sample were compared to the 2017 sample, and the two sets of respondents were quite similar. The 2022 sample was a bit older (56.7% aged 50 or older vs. 50.7% in 2017), with a higher percentage of White respondents (73.7% vs. 64.7%), fewer registered Republicans (16.9% vs. 27.6%). and more education (70% with at least a bachelor’s degree vs. 57%).
Methods of Analysis
The sample characteristics and support for safe consumption sites were analysed statistically using SPSS software. The results include descriptive statistics, an independent samples proportions test, bivariate chi-square tests, and a series of multivariate logistic regression models.
Results
Support for Drug Consumption Sites
Support for Drug Consumption Sites.

Bivariate Associations
Demographic Characteristics
Bivariate Associations Between Demographic Variables and Drug Consumption Site Opinion (2022 Data).
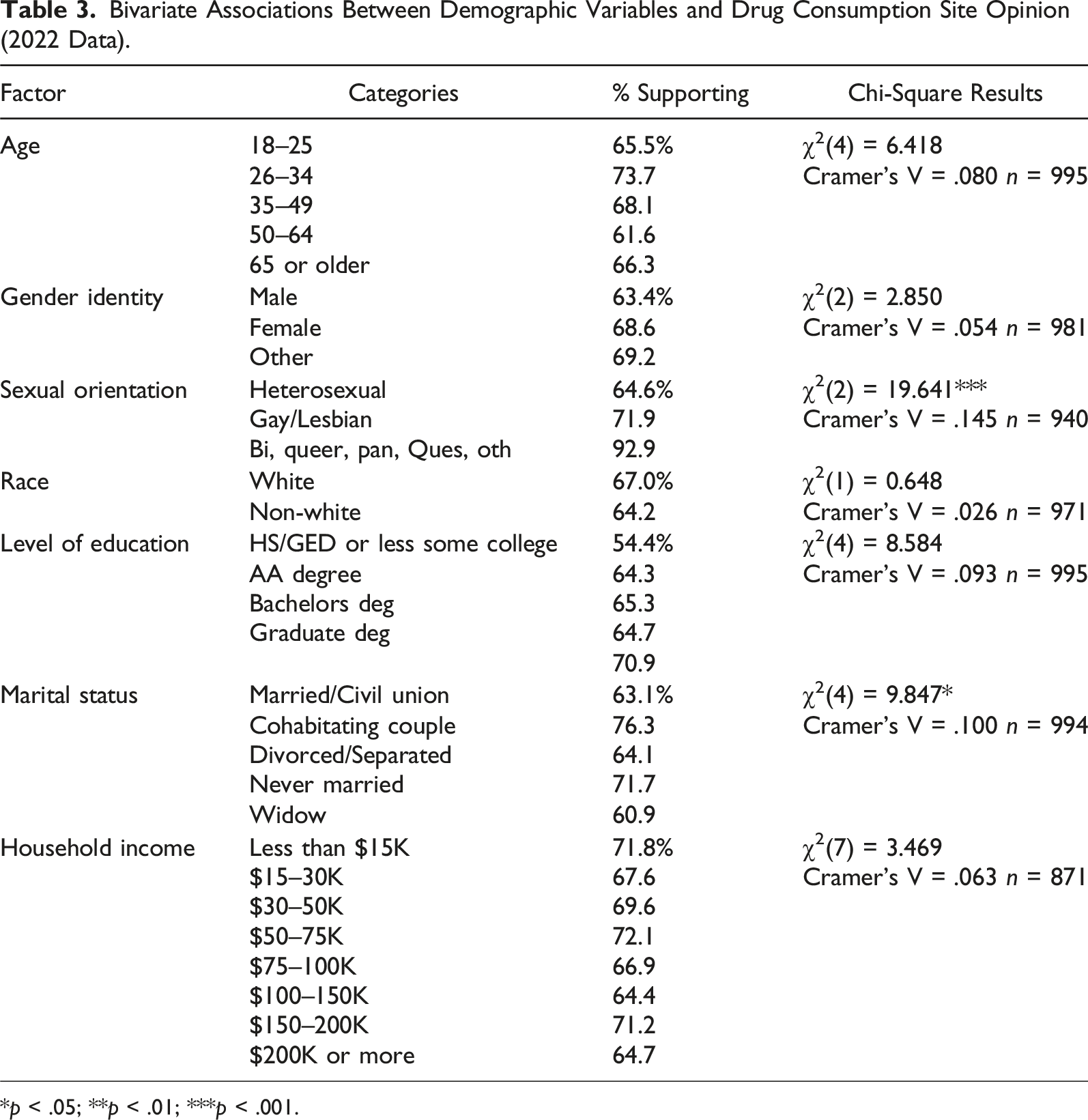
*p < .05; **p < .01; ***p < .001.
Drug Use
Bivariate Associations Between Drug Variables and Drug Consumption Site Opinion (2022 Data).
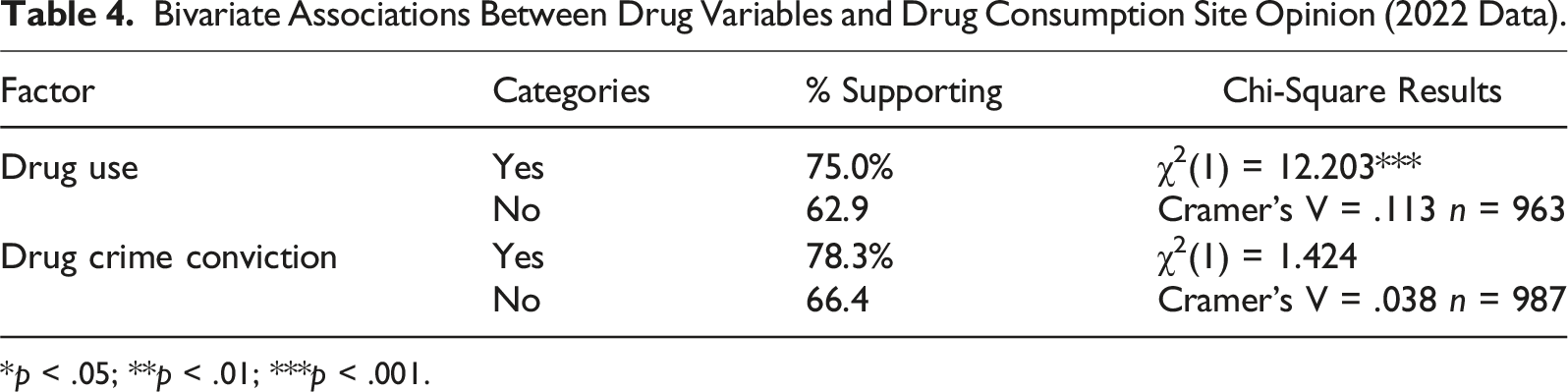
*p < .05; **p < .01; ***p < .001.
Trust in California’s Government
Bivariate Association Between Trust in California’s Government and Drug Consumption Site Opinion (2022 Data).
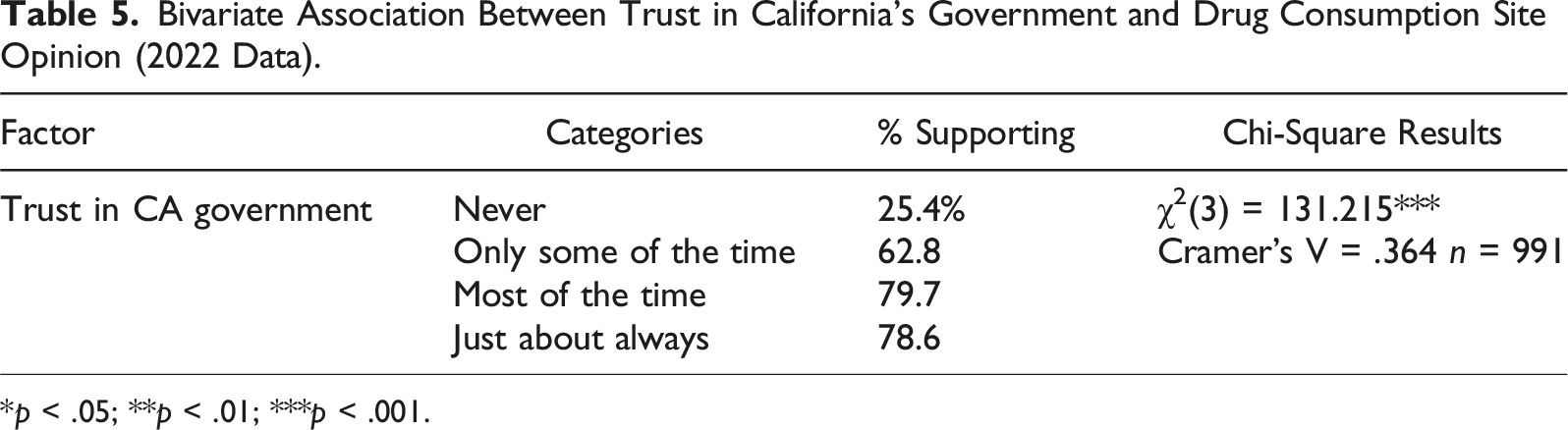
*p < .05; **p < .01; ***p < .001.
Political Party Affiliation
Bivariate Associations Between Political Party Affiliation and Drug Consumption Site Opinion (2022 Data).
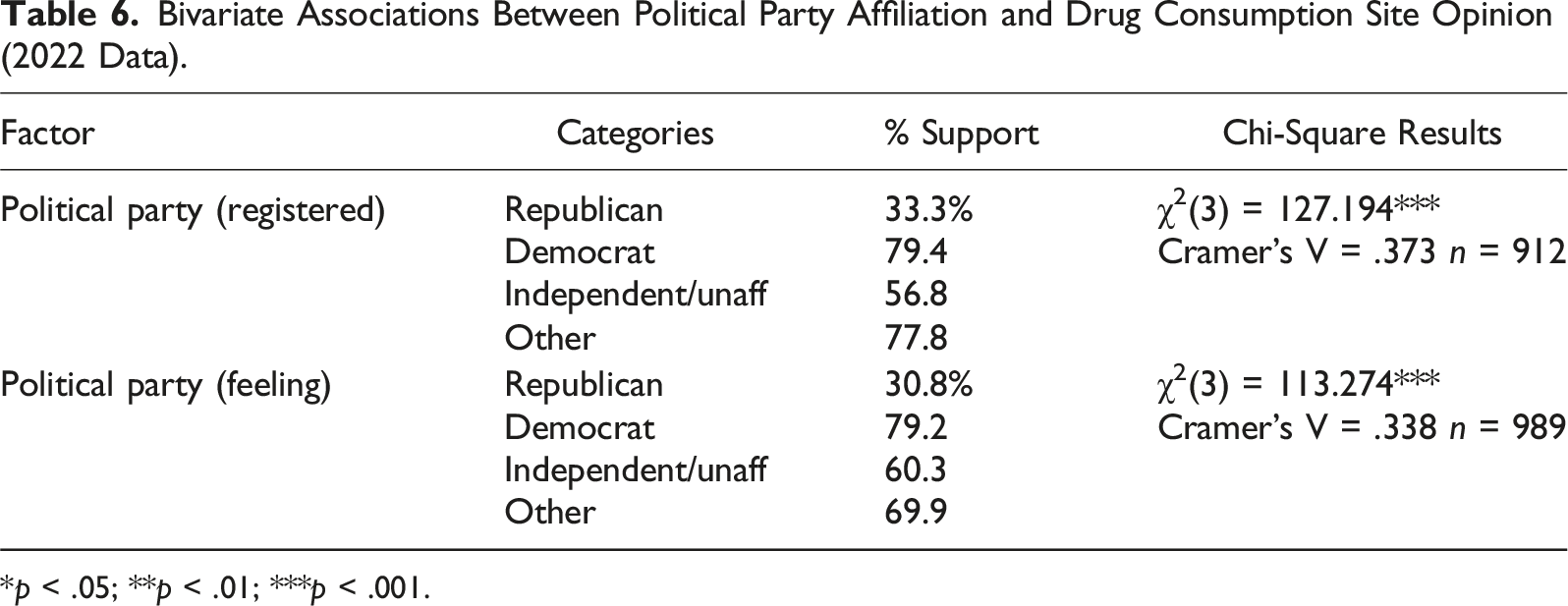
*p < .05; **p < .01; ***p < .001.
Multivariate Models
Multivariate Logistic Regression Models Predicting Drug Consumption Site Opinion (2022 Data).
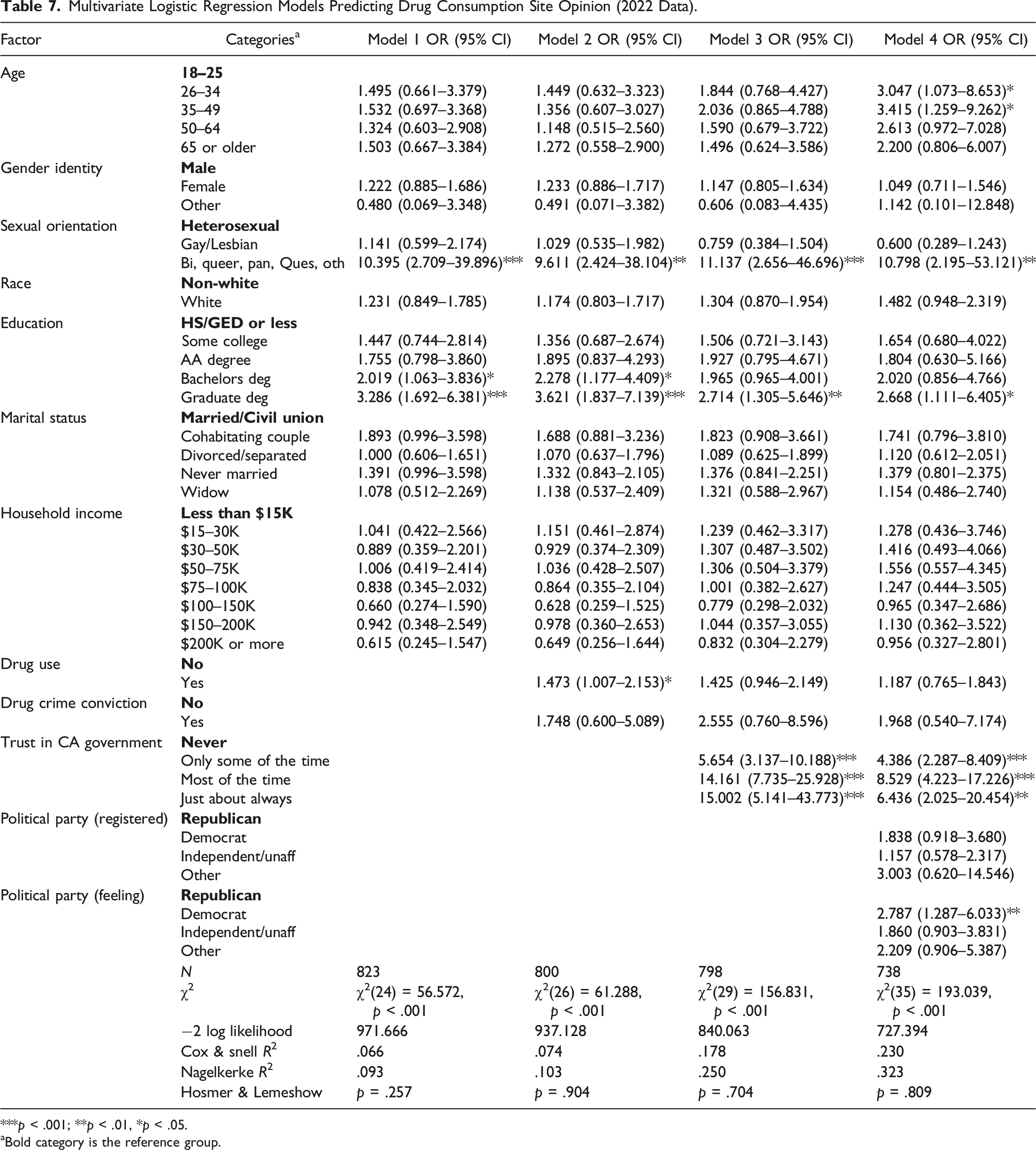
***p < .001; **p < .01, *p < .05.
aBold category is the reference group.
In our first multivariate logistic regression model, we only entered the demographic variables as covariates. In the subsequent models, we entered one group of variables at a time, starting with the drug variables, followed by trust in California’s government, and finally, political affiliation variables. This allowed us to examine changes in the significance and impact of individual predictors as other covariates were added to the model.
Model 1 revealed only two demographic factors that were significantly associated with the dependent variable. These variables were sexual orientation and level of education. Individuals who identified as bisexual, queer, pansexual, questioning, or other were approximately ten times more likely to support overdose prevention sites than heterosexual individuals. They were also significantly more likely to support these sites than gay or lesbian individuals. For education, individuals, who had earned a bachelor’s or graduate degree were two to three times more likely to support overdose prevention sites than individuals whose highest level of education was a high school education or less (i.e., HS diploma, GED, never finished high school).
Model 2 introduced the drug variables along with the demographic variables from Model 1. Both sexual orientation and level of education remained statistically significant. The prior drug use variable also displayed statistical significance, with individuals who had reported prior drug use being approximately one and a half times more likely to support overdose prevention sites than individuals with no reported prior drug use.
Model 3 introduced trust in California’s government to the model. With the introduction of this new covariate, sexual orientation and level of education remained statistically significant, but prior drug use was no longer significant. The newly introduced trust in government variable was statistically significant. Specifically, individuals who reported ‘never’ trusting California’s government were five times or more less likely to support overdose prevention sites than individuals who report trusting California’s government ‘only some of the time,’ ‘most of the time,’ or ‘just about always.’
Model 4 was the final model, and it introduced the two political affiliation variables. With the addition of these two new covariates, sexual orientation, level of education, and trust in government remained statistically significant. The age variable also became significant, with individuals between the ages of 26 and 49 being significantly more likely to support overdose prevention sites than individuals aged 18 to 25. For political affiliation, individuals who personally thought of themselves as Democrats (regardless of official registration status) were over two and a half times more likely to support overdose prevention sites than those who identified as Republicans. Interestingly, an individual’s registered political party was not significantly associated with support or opposition to overdose prevention sites.
The variables that displayed the most consistent associations with opinions about drug consumption sites, even after controlling for other covariates, were sexual orientation, level of education, trust in California’s government, and political affiliation. BPQ + individuals (i.e., those identifying as bisexual, queer, pansexual, questioning, or other) were more likely to support overdose prevention sites than heterosexuals. Individuals with higher levels of education, specifically those with graduate degrees, were also more likely to support overdose prevention programs than individuals with a high school diploma or less. Those who have at least ‘some trust’ in California’s government to do ‘what is right’ were significantly more likely to support these sites than individuals with no trust in the government. Finally, Democrats were significantly more likely to support sites than Republicans.
Although age and drug use were significant in some of the models, the findings were not consistent across all models. The fact that age displayed significance in the largest model (#4), suggests age may play a role in influencing opinions once other factors have been controlled for, with adults between the ages of 26 and 49 reporting the highest levels of support. This variable warrants further investigation. On the other hand, the significance of drug use in one of the earlier models disappeared once other covariates were entered, thus suggesting that variable does not have a unique impact on support levels.
Discussion
The data illustrate that California voters support implementing overdose prevention sites, aligning with the CA legislature yet conflicting with the current and previous CA governors’ vetoes. CA voters are more supportive of safe consumption spaces in 2022 than they were in 2017. Those least supportive of these sites are between 18 and 25 years of age, identify as heterosexual, have no college education, express no trust in California’s government, and consider themselves Republican. While the data suggest that a ballot measure has a likelihood of being approved now, additional educational campaigns about safe consumption sites and harm reduction more generally should target these groups. Local educational efforts would also be needed in areas where OPSs are implemented to avoid the potential overturning of these sites due to NIMBYism (similar to that which happened to OCNEP in Orange County, CA). These data further suggest that a ballot measure, rather than a legislative bill, is needed for OPS to be approved. Our study also supports the assertion made by Disch (2012) that political power can be disconnected from public opinion. This is especially true for the War on Drugs and related drug policies. Despite the persistence of ineffective and harsh drug criminalization, public polling shows a desire to shift from criminalization to a public health approach (ACLU, 2021). Just like with both medical and recreational marijuana use, political action is detached from the public desire to sanction OPS in California.
California is a decades long leader in progressive politics and policy reform and can serve as a litmus test for perceptions among less progressive demographics. Although these data are from California specifically, the findings demonstrating voter support for OPS despite past political action are relevant to those seeking similar policy reforms in other states and at the federal level. For example, ballot measures or legislative bills are not likely to pass in deep red states, where populations overwhelmingly identify as Republican and have less trust in government. Deep red states, like Louisiana, Kentucky, Tennessee, and West Virginia also have some of the highest overdose death rates in the United States (CDC, 2023) and could greatly benefit from OPSs. Significant educational efforts on the value and effectiveness of OPSs would be needed to build support and push the needle in those states. Educational campaigns have been shown to be effective at changing perceptions and influencing behavior (see Maibach et al., 2008; Noar, 2006; Snyder & LaCroix, 2013; Wakefield et al., 2003). While staunch moral beliefs may pose a barrier to the efficacy of these campaigns, Felson et al.’s (2019) analysis of cannabis legalization suggest public health campaigns and media framing can impact perceptions of once polarizing issues.
Avenues for Future Research
Future research on public perception at the state level and local level is needed to understand when and how OPSs and other harm reduction measures may be implemented. While there is statewide support in CA, this may vary when examined on a smaller geographic scale. Moreover, similar research is needed in states other than California. As many states have grappled with the implementation of OPS, through funding, legislation, and grassroots efforts, an understanding of general public perception of OPS and similar harm reduction measures is needed, and a qualitative assessment of voter perceptions would help clarify correlations between certain voter characteristics, such as LGBTQ identities, marital status, and governmental trust, and public support of or opposition to OPS discovered in this study.
An important area of inquiry raised by the study is the constituency paradox raised by Disch (2012) and supported by these data. How can the disconnect between political actions and public opinion be explained? Why do political decisions so often diverge from the evidence? While this study explores this query between Governor Newsom’s veto of SB57 and the public approval of OPS, further studies can explore this failure of democracy.
Conclusion
OPS is an evidence-based solution to the opioid epidemic. OPSs have been shown to reduce overdoses and subsequent overdose-related mortality, the transmission of blood-borne disease, infection, crime, public drug use, public needle litter, and overall public nuisance (Kerr et al., 2017; Lofaro & Miller, 2021; Potier et al., 2014; Wenger et al., 2011). Moreover, through comparative quantitative analysis of voter data from 2017 and 2022, this study revealed that CA voters would support the implementation of an OPS in their state. Given this, Governor Newsom’s veto of SB57 represents a disconnect between his policies and the will of those he governs.
Drug policy and harm reduction reform efforts may be best served from a bottom-up approach. Similar to the legalization of medical marijuana in 1996 and the subsequent legalization of recreational marijuana in 2016, ballot measures, rather than legislative efforts, may be needed to sanction overdose prevention sites. It is time to give the people what they want, and give those who use drugs what they need, overdose prevention sites.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (November 2024):
This article has been updated to include minor style corrections in Table 7 since its original publication.