
Abstract
The impact of COVID-19 on Driving Under the Influence (DUI) treatment is unknown. This study examined changes in the number of DUI program enrollments and enrollees’ characteristics by COVID stage. We conducted secondary analyses of routine data collected from a sample of 3309 consecutive clients enrolling in a large DUI treatment program Pre-COVID-19, Early-COVID-19 during lockdown, and Late-COVID-19 after lockdown lifted. Enrollments declined in Early-COVID (n = 643) compared to Pre-COVID (n = 1416), but rebounded in Late-COVID (n = 1250). Early-COVID enrollees tended to be unemployed, first conviction offenders, and have only minimal depression, non-hazardous alcohol use, lower alcohol levels at arrest, and lower drug use compared to their Pre-COVID counterparts. Compared to Pre-COVID, Late-COVID was generally characterized by the same characteristics as Early-COVID, as well as greater numbers of Latinos. Findings demonstrate extraordinary enrollment reductions and changes in sociodemographic and clinical features among DUI treatment enrollees during stages of COVID-19.
Introduction
The Coronavirus has been considered the greatest socioeconomic and public health disaster of the 21st century (Naseer et al., 2023; Raphael & Schneider, 2013). A plethora of emerging research has demonstrated the unparalleled burden COVID-19 placed on individuals, healthcare providers, and organizations, the effects of which still linger (Czeisler et al., 2020; Whaley et al., 2020). While lockdown measures were implemented to curb COVID-19 transmission, such measures had unintended public health and safety consequences. Emotional dysregulation and maladaptive coping behaviors are psychological responses to pandemics (Taylor, 2019), and as such, substance use, mental health, trauma-related symptoms, serious consideration of suicide, and drug overdose deaths increased during the COVID-19 pandemic, indicating a greater need for expanded treatment infrastructure and access (Ahmad et al., 2022; Czeisler et al., 2020; Rodriguez et al., 2020; Twenge & Joiner, 2020). Further, despite fewer vehicles on the road secondary to lockdown and stay-at-home measures, the U.S. experienced a notable 14.3% increase in Driving Under the Influence (DUI)-related fatalities, from 10,196 in 2019 to 11,654 in 2020 (National Center for Statistics and Analysis, 2022).
While increasing pandemic-related public health and safety problems emerged, COVID-19 illuminated deep structural problems in the healthcare system which have been associated with health disparities stemming from inequalities in determinants external to the healthcare system (Blumenthal et al., 2020). COVID-19 ushered in unprecedented healthcare system challenges characterized by lower utilization of services, significant revenue losses (particularly in fee-for-service markets, such as DUI), and diminished human resource capital (Ambrosetti et al., 2021; Blumenthal et al., 2020; Doleman et al., 2023; Mark, Gibbons, et al., 2021; Raphael & Schneider, 2013). Prior research reported declines in healthcare utilization ranging from minimal (e.g., non-elective procedures and prescriptions) to very large reductions (e.g., elective, preventive procedures) (Whaley et al., 2020). There were also notable reductions in behavioral health service utilization, including reductions in psychiatric admissions during the COVID-19 lockdown and a rebound effect after the lockdown was lifted (Ambrosetti et al., 2021). Similarly, despite increases in drug-related overdose deaths, addiction treatment admissions declined both nationally (Cantor et al., 2022), and in California (Mark, Gibbons, et al., 2021). However, these reductions were based on studies of publicly-funded, typically voluntary, substance use treatment programs, unlike the California fee-for-service DUI treatment system.
The California DUI treatment system represents a critical intersection between public health and criminal justice, providing early intervention to those potentially vulnerable criminal justice-involved individuals mandated to treatment. While research has explored COVID-19 impacts on substance use treatment, focusing on access, program-level impacts, and Telehealth services (Green et al., 2020; Mark, Treiman, et al., 2021; Pagano et al., 2021), there is a notable research gap specific to the DUI treatment system context, which this study served to address.
While we anticipated COVID-19 would be associated with a reduction in DUI treatment enrollments, the magnitude remained unclear and obscured by unique DUI treatment contextual factors. Specifically, while the California Department of Health Care Services (DHCS) loosened regulations to allow for virtual remote services and expand DUI treatment access, not only did DUI treatment programs close temporarily during Early-COVID, but between August 2019 and April 2022, there was a 16% permanent reduction in licensed DUI programs, from 290 to 245, including the largest program located in the County in which this study was conducted (DHCS, 2020).
COVID-19 also deeply affected California Courts which play an integral role in the DUI treatment process. Courts also temporarily closed during the Early-COVID-19 period (San Diego Superior Court California DUI FAQ after Coronavirus COVID-19 Pandemic Reopening, 2020). Adjudication of criminal cases nearly ceased, and dockets were extended while stay-at-home orders were in place (Harris, 2023). Locally, arraignments were scheduled out for months (>120 days) compared to the usual 30-45 days Pre-COVID (Harris, 2023). When Courts reopened, an array of policies to reduce COVID-19 transmission were implemented, and many DUI offenders were diverted out of criminal Court, given alternative sentencing or extensions (Harris, 2023). Court backlogs, delays, and policy changes (e.g., virtual hearings) potentially affected conviction rates (Harris, 2023). The breadth of such dynamic contextual factors, coupled with the lack of estimates of declines in DUI treatment contributed to our need to examine the magnitude of change in DUI treatment enrollments during Early- and Late-COVID-19 periods compared to the Pre-COVID period.
It was also important to examine whether those enrolling during Early- and Late-COVID-19 differed by sociodemographic, program-level, and clinical characteristics compared to their Pre-COVID counterparts. While DUI treatment is considered ‘early intervention’ for those with substance-related problems and its risk factors (Hohman et al., 2017), the DUI population is one characterized by high rates of substance use disorders (SUDs), co-morbid psychiatric conditions, trauma backgrounds, and socioeconomic disparities, which may have been amplified during COVID-19 (Barker et al., 2023; Hohman et al., 2017). COVID-19 exacerbated pre-existing socioeconomic disparities in health and disrupted services to meet marginalized clients’ needs (Cruden et al., 2021). The shift to a virtual service modality draws attention to potential disparities in service utilization (Vakkalanka et al., 2024); thus, it was important to examine COVID impacts in the DUI treatment context and the longer term changes following the Early-COVID lockdown period (Brandizzi et al., 2022).
This study served to bridge these critical research gaps by examining changes in the number of DUI treatment program enrollments by COVID stage (Pre-, Early- and Late-COVID), and assessing changes in enrollees’ sociodemographic, program-related (e.g., first or multiple conviction), and clinical characteristics (e.g., alcohol/drug use and depression) by COVID stage. Our overarching assumption was that Early-COVID, during lockdown, had a significant impact on enrollments and enrollee characteristics compared to the Pre-COVID period (prior to lockdown), and Late-COVID (after lockdown lifted). Given the fee-for-service DUI structure, such impacts had serious implications for DUI treatment capacity and sustainability. We hypothesized there would be a significant decline in DUI treatment enrollments in Early-COVID compared to the Pre-COVID period with a significant rebound in Late-COVID and approximating Pre-COVID numbers. Using the 3-category COVID-19 stage as the dependent variable, we examined sociodemographic, program-level, and clinical characteristics, but made no hypotheses given the exploratory nature of this study and the lack of literature specific to the DUI context.
Methods
Setting and Participants
We conducted a retrospective, secondary analysis of data collected from 3,309 participants enrolling in a large Southern California DUI treatment program from mid-June 2019 to mid-March 2022. Participants were referred through the Department of Motor Vehicles (DMV) or the Courts following an alcohol and/or drug-related DUI offense. Figure 1 graphically depicts the DUI Offender Process once someone is convicted, with the DMV, Court, and DUIP program responsibilities depicted (CADTP, 2017). The DUI Offender Process (CADTP, 2017)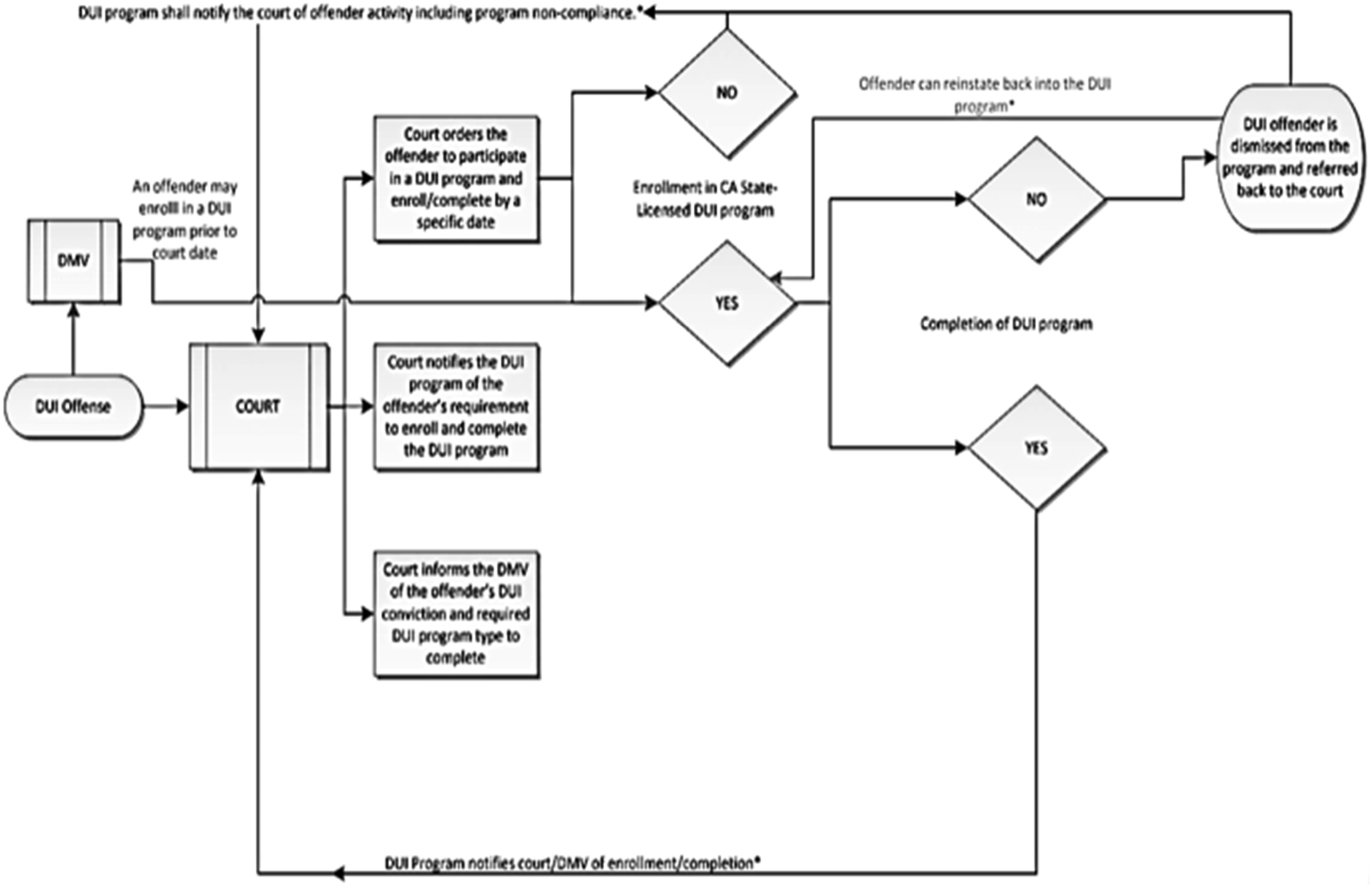
The present DUI program has been operational for 34 years. Prior to COVID, licensed DUI treatment programs were only authorized to provide in-person services. After a brief 2.5-month closure during Early-COVID, the program implemented Telehealth and commenced a hybrid of in-person and virtual remote services after COVID-19 lockdown measures were lifted. Services include psychoeducation, individual, and group counseling targeting problem recognition and strategies for reducing risk and implementing effective behavioral change (SAMHSA, 2006). The counseling staff are either registered/certified Alcohol and other Drug (AOD) counselors or master’s level clinicians. The program uses a standardized curriculum, The Paradigm Developmental Model of Treatment (PDMT) (DiStefano, 2012) and a case management framework for resource linkages (SAMHSA, 2000).
The program length is predicated on program type (i.e., first or repeat offense) and blood alcohol concentration (BAC) or breath alcohol concentration level (BrAC) in a driver’s system. The program length ranges from 6 weeks (i.e., DUI charge reduced to reckless driving) to 18 months (i.e., Multiple Conviction). There are two First Conviction Program lengths (three or nine months), with mandates for the enhanced 9-month program based on a BrAC
Data Collection and Samples
The DUI program collected participant-reported sociodemographic, program level, and clinical (i.e., AOD use and depression severity) cross-sectional data from n = 3,309 consecutively enrolling participants (n = 1,416 Pre-COVID, n = 643 Early-COVID, and n = 1,250 Late-COVID) during a routine intake process (Assessment of Participant’s Alcohol or Drug Problem, 2012). Most measures are based on current theory, research, and practice in the field. At Pre-COVID, tablet-based assessments were largely self-administered by participants, with help from program staff when needed. Early- and Late- COVID data were collected on tablets by staff conducting virtual interviews. All data were entered into a secure internal database and de-identified prior to analysis. Institutional Review Board approval was obtained.
Measures
The 3-category COVID Stage criterion variable included a Pre-COVID control period, defined as the time between June 15, 2019 to March 15, 2020. June 2019 marked the point at which the DUI program shifted to a web-based assessment tool using tablets, affording a standardized data collection strategy across the study. March 17, 2020 marked the implementation of lockdowns to prevent COVID transmission, at which point the program closed temporarily and re-opened in June 2020. For similarity with Pre-COVID in duration and season, we chose similar time frames for the Early-COVID stage, defined as June 15, 2020 to March 15, 2021 during lockdown, and the Late-COVID stage, defined as June 15, 2021 to March 15, 2022, after the lockdown lifted. Figure 2 shows the three COVID stages by month and year. Newly Enrolling Participants in the DUI Program by Month/COVID Stage: June 15, 2019 to March 15, 2022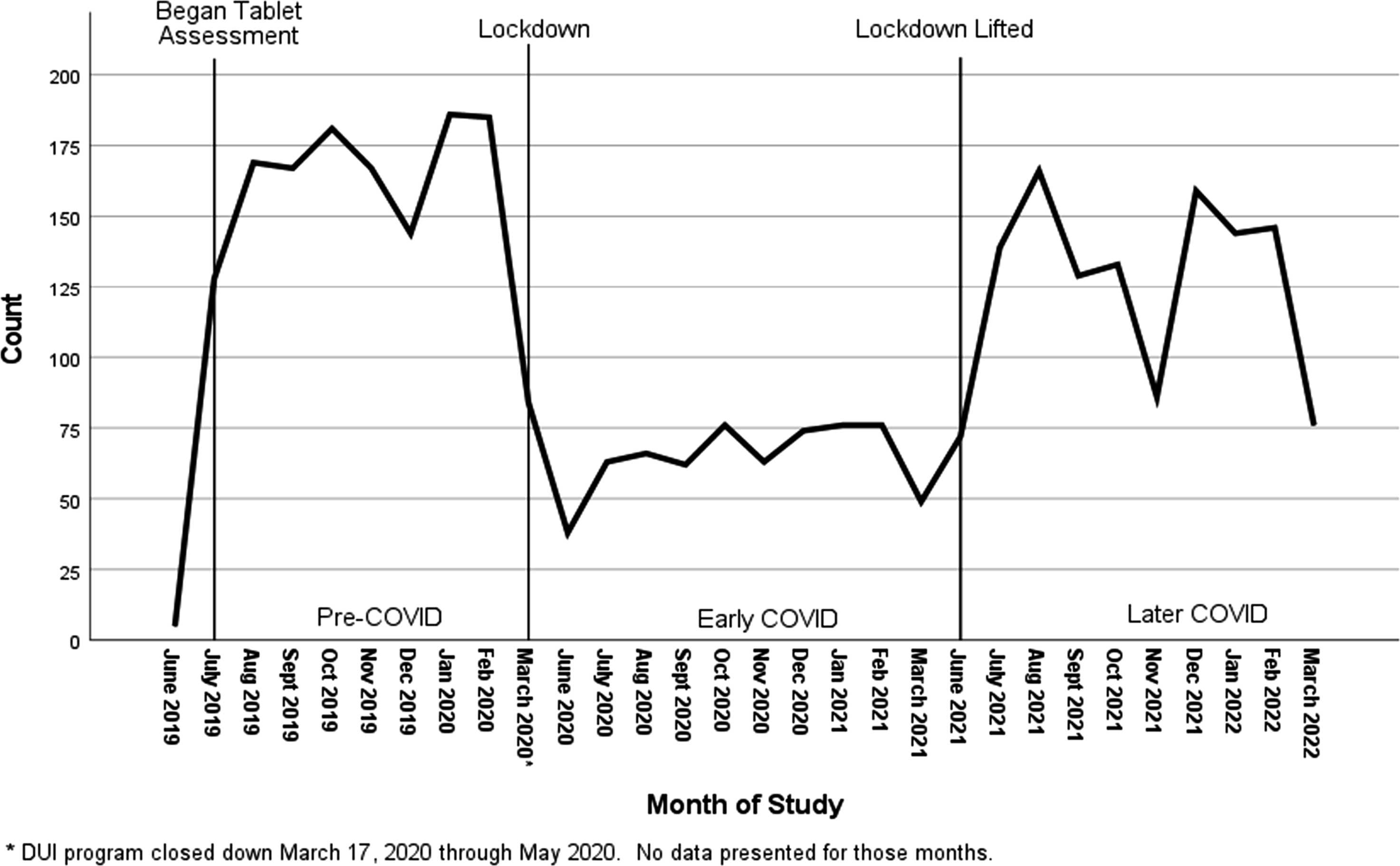
Sociodemographic variables included age at intake, gender (binary), race/ethnicity, language, marital and employment status, and military experience. Education and income were excluded because of unreliable or missing data. Program-level variables included DUI program type (i.e., First or Multiple Conviction) and resident district region (i.e., Central, East or North County, South Bay, or Out-of-County/State).
Clinical variables addressed alcohol, drug, and depression severity measures. Alcohol use severity was measured using the Alcohol Use Disorders Identification Test (AUDIT-10) and the AUDIT-C to assess hazardous alcohol use and alcohol use disorders (Higgins-Biddle & Babor, 2018). The AUDIT-10 assesses alcohol consumption, drinking behaviors, and alcohol-related consequences and is considered the gold standard for screening hazardous alcohol use in clinical settings (Babor et al., 2001). A visual depiction of standard drinks was provided to prompt responses. The AUDIT-10 is scored on a scale of 0-40 and typically recorded into categories: scores ranging from 0-7 indicate low risk alcohol use; 8-15 indicate risky use; 16-19 indicate hazardous use; and 20-40 indicate high risk alcohol use (Babor et al., 2001). For this study, Cronbach’s alpha for the AUDIT-10 ranged from 0.87- 0.91 by COVID stage. The AUDIT-C, an even briefer screener that consists of the first three AUDIT-10 questions, primarily addresses the amount and frequency of use and identifies gender-specific at-risk drinkers (i.e., binge drinking) who may not be alcohol-dependent. The AUDIT-C is scored 0-12, with a score of 0 reflecting no hazardous alcohol use. A score ≥ 4 for men and ≥ 3 for women is considered positive for hazardous alcohol use; therefore, the AUDIT-C is often used to create a hazardous/non-hazardous dichotomous categorical variable. In general, a higher score or category on both the AUDIT-10 and the AUDIT-C is indicative of problematic drinking (Dawson et al., 2005).
In addition to the legal consideration of BrAC for DUI arrest (i.e., legal limit of 0.08), higher BrAC concentrations are important measures of alcohol misuse because they are associated with greater risk for both DUI recidivism and alcohol related injury (Courchesne et al., 2018). BrAC is typically participant-reported for those referred through the DMV and is often confirmed by the Court. In this study, BrAC levels were self-reported and categorized into the following three meaningful categories, <0.08%, 0.08–0.19%, and ≥.20%.
The Drug Abuse Screening Test (DAST-10), a validated 10-item brief screening tool, was used to assess non-prescribed drug use and related consequences (Skinner, 1982). Items are scored one point for “yes” responses, with reverse scoring for one item. A score of 0 indicates no problems reported; 1-2 indicates low level risk; 3-5 moderate level; 6-8 substantial level; and 9-10 severe level (Skinner, 1982). In this study, moderate, substantial, and severe categories were combined due to small cell sizes, and Cronbach’s alpha ranged from 0.90-0.75 by COVID stage.
To screen for depression, the intake assessment used the first two items from the Patient Health Questionnaire (PHQ-2), which screens for the frequency of depressed mood and anhedonia in the past two weeks (Patient Health Questionnaire (PHQ-9 & PHQ-2), 2020). A positive response to either item prompted the PHQ-9 to screen whether the participant met criteria for a depressive disorder, using a 4-point Likert scale to score criteria from 0-3 (not at all to nearly every day). Total scores of 0-4 indicate no to minimal depression; 5-9 mild; 10-14 moderate; 15-19 moderately severe; and 20-27 severe depression In the present study, all categories of any depression (i.e., mild, moderate, moderately severe, and severe) were combined due to small cell sizes, and the Cronbach’s alpha ranged from 0.89-0.92 by COVID stage.
Statistical Analyses
Enrollment numbers were aggregated on a monthly basis and a Kruskal-Wallis nonparametric test assessed COVID stage differences in enrollments (Hollander et al., 2015). Differences by COVID stage in sociodemographic, program-related, alcohol, drug use, and depression severity measures for repeated cross-sectional data included bivariate tests (chi-square tests and one-way analysis of variance). Multinomial Logistic Regression (MLR) was then used to assess the independent association of DUI participants’ sociodemographic, program-related, and clinical variables with COVID stage (Petrucci, 2009). To select the set of independent variables (i.e., correlates) for the MLR, we included those associations from the bivariate analysis that were statistically significant at the .05 level and that also had effect sizes (Cramer’s V or Eta2) of 0.05 or greater (Mangiafico, 2016). A Forced Entry method in the MLR was used to determine the strength of association between COVID stage and independent variables.
Results
Participant Enrollments by COVID Stage
Figure 2 presents the monthly enrollment of new participants for the three COVID stages. For the Pre-COVID 9-month period, there were 1,416 new participants, with a mean of 156.78 new participants each month. The Early-COVID period during lockdown saw 643 new participants, or an average of 64.3 new participants per month, a 54.6% decrease from the pre-COVID period. During Late-COVID, once lockdown had been lifted, numbers rose to 1,250 (average of 125 per month), representing a 94% increase over Early-COVID but were still 11.7% below Pre-COVID numbers. A Kruskal-Wallace test showed that the Early- COVID period was significantly different from Pre- and Late-COVID, although Pre- and Late-COVID did not differ significantly from one another (χ2(2) = 19.39, p = .000).
Sociodemographic, Program-Level, and Clinical Characteristics of Enrollees by COVID Stage
Multinomial Logistic Regression Results Examining the Relationship Between Sociodemographic, Program Level, and Clinical Characteristics for Participants Enrolling Pre-COVID, Early-COVID and Late-COVID Periods
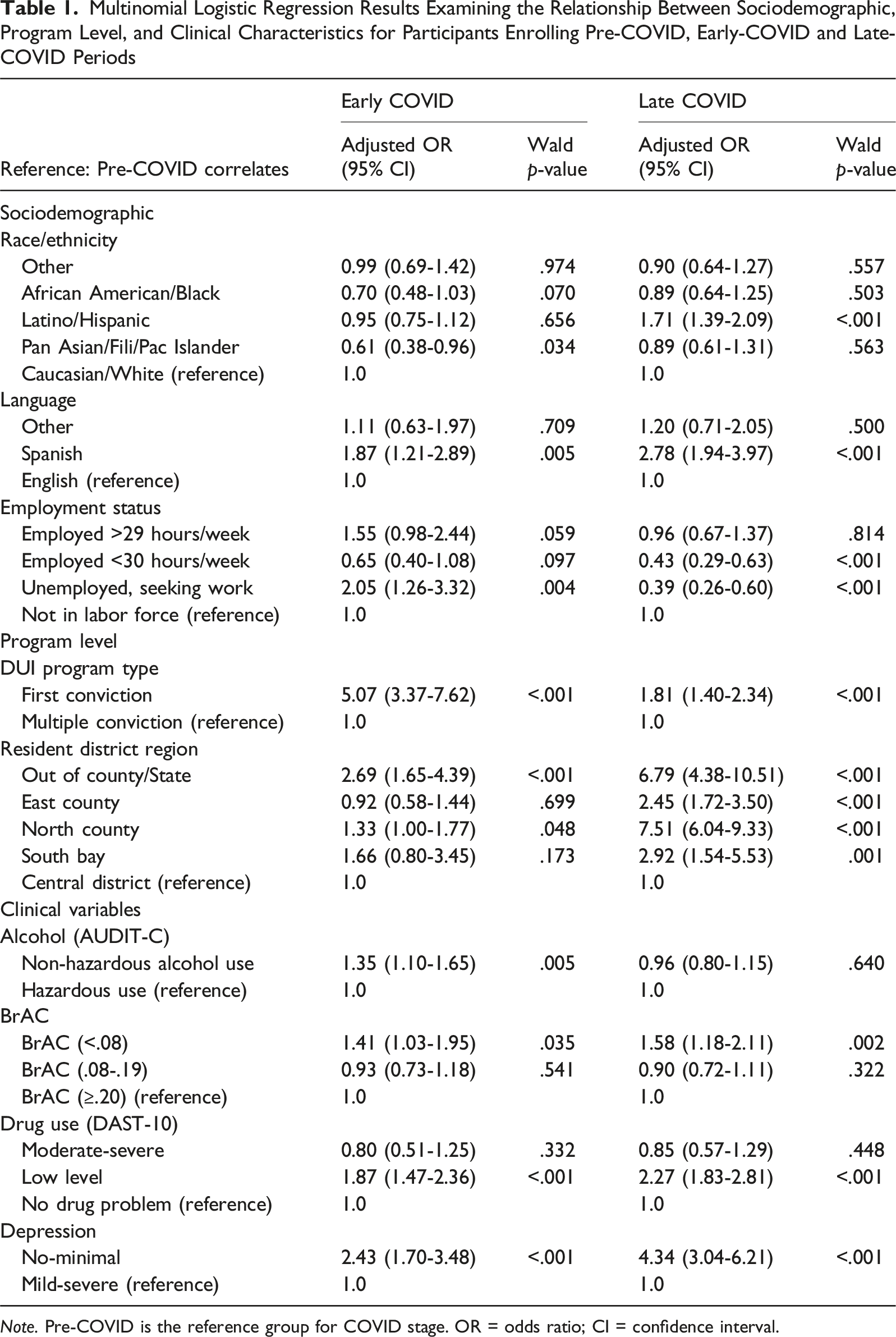
Note. Pre-COVID is the reference group for COVID stage. OR = odds ratio; CI = confidence interval.
Discussion
This study analyzed the longitudinal variations in the number of DUI enrollments by COVID stage, and changes in sociodemographic, program-level, and clinical features by COVID stage of those enrolling into a large Southern California DUI treatment program, by COVID stage. We found a significant reduction (54.6%) in enrollment numbers during Early-COVID, following lockdown, compared with the Pre-COVID period. During Late-COVID, once lockdown lifted, numbers increased 94% over Early-COVID, suggesting the impact of lockdown measures. Our Early-COVID reductions are somewhat consistent, although larger, than those reported in other studies, with a 23.5% average decline, from 2019 to 2020, in substance use treatment admissions reported across States (Cantor et al., 2022), and a 28.3% reduction in monthly treatment admissions (outpatient and inpatient) observed in California (Mark, Gibbons, et al., 2021). However, these comparison studies were based on publicly funded treatment programs, unlike California DUI treatment, which is legally structured as fee-for-service.
The Early-COVID enrollment reductions were likely due to multiple procedural, structural and behavioral changes during that time, including reduced vehicle miles traveled, changes in law enforcement priorities, the closing of bars and indoor restaurants, lower arrests, and Court discretion. California, a COVID “hotspot” (Gilson, 2020), swiftly implemented pandemic-response policy changes and was one of the first states to implement shelter-in-place orders (Jackson et al., 2022). When the COVID lockdown was applied in March 2020, California experienced one of the largest reductions in road traffic, thus a large reduction in DUIs was expected (Gilson, 2020). Evidence indicates that travel pattern changes associated with staying-at-home on any given day increased from 19% pre-COVID to 26% during COVID (Office of Behavioral Safety Research, 2021). Simultaneously, San Diego closed bars and indoor restaurants to contain COVID (Higgins-Dunn, 2020).
By April 2020, California DUI arrests had dropped dramatically (Rees et al., 2023). In addition to policies that lowered police-public encounters during Early- COVID, law enforcement procedural changes may have diminished DUI arrests; DUI checkpoints were halted and law enforcement shifted focus toward COVID public safety and social order (Jennings & Perez, 2020). Police made fewer traffic stops for minor violations which would have previously resulted in a DUI (Gilson, 2020). Regional law enforcement staffing challenges plagued the area (Handy & Hargrove, 2023), exacerbated by the unpopular vaccine mandate resulting in a high volume of officer resignations (Garrick, 2022; Hodgson, 2022).
While miles driven and DUI arrests decreased during COVID, evidence suggests U.S. drivers had higher percentages of self-reported high-risk driving behaviors, with 7.6% reporting the likelihood of engaging in DUI behavior during COVID, compared to Pre-COVID, vis-à-vis their Canadian counterparts (Vanlaar et al., 2021). Findings highlight pandemic-related attitudes in subsets of drivers who perhaps thought DUI behavior was more likely to go undetected during COVID. In California, another interesting pattern change in DUI arrests occurred; whereas DUI arrests prior to COVID typically occurred at night or early morning hours, during COVID DUI arrests often occurred during daytime hours (Hessedal, 2020). Should there be unique pandemic-related conditions under which DUI arrests occur, there may be changes in the characteristics of individuals enrolling in DUI treatment.
Our DUI program made several adaptations to implement Telehealth, such that by June 2020 services could be delivered to a reduced number (n = 1,553) of participants. Once the lockdown was lifted mid-June 2021, (i.e., Late COVID), there was an immediate uptick in enrollments, which coincided with a 50% increase in DUI program staffing compared to the prior year, as social distancing restrictions lifted. In November 2021, there was a brief interruption in the recovery pattern where we experienced a large enrollment dip, most likely due to concerns over the Delta and newly identified Omicron variants (Hoeven, 2021).
In addition to COVID’s impact on the DUI program’s quantity of utilization, we examined enrollees’ characteristics during each COVID stage. All nine variables tested in a multivariate model were independently related to COVID stage. Of the 22 statistically significant associations, 14 were consistent in Early- COVID and Late- COVID in terms of statistical significance and direction, although the magnitudes differed. For example, the odds of preferring Spanish increased in Early- and Late- COVID compared to Pre-COVID; although the magnitude was greater in Late-COVID than in Early- COVID (Adjusted OR = 2.78 and 1.87, respectively).
Employment status was associated with the odds of enrolling by COVID stage. More than twice as many of those unemployed/seeking work (compared to those not in the work force) enrolled Early-COVID, yet the unemployed were far less likely to enroll Late-COVID, which is understandable given California’s unprecedented COVID-driven labor crisis. In Early-COVID, unemployment climbed to 3 million statewide by May of 2020—45% of California workers had filed for unemployment by the end of 2020 (Bell, Hedin, Moghadam, et al., 2021). The San Diego metropolitan area followed this trend, reporting a 16% unemployment rate at the peak in April and May of 2020 (US Bureau of Labor Statistics, 2025). Yet, statewide and local re-employment recovery rose slowly through the Fall of 2020 and by the Spring of 2021, 57% of California and 55% San Diego workers who lost their jobs in Early-COVID were employed at least part time (Bell, Hedin, Mannino, et al., 2021; US Bureau of Labor Statistics, 2025). This timing of unemployment and recovery could account for the higher number of unemployed enrolling during Early-COVID. Several studies have reported that the unemployed were particularly likely to misuse alcohol (Weerakoon et al., 2021) and other drugs (Hunter & Nida, 2021) during the pandemic, so these individuals may have comprised a large proportion of those who received a DUI during Early-COVID. By Late-COVID, many previously unemployed had found work and so may have been less likely to be involved in a DUI.
By Late-COVID, part-time employees (<30 hours per week) were less likely to enroll compared to Pre-COVID. Historically, many part-time workers preferred full-time work, but the jobs were not there. COVID changed that by contributing to a tight labor market (many unfilled job vacancies), with many employers offering full time jobs to attract workers (Isadore, 2022). Thus, the number of part-time workers hit an all-time low by Summer 2022, making up just 2.2% of the overall US labor force (Isadore, 2022). To the degree that part-time workers moved into full-time jobs, particularly in Late-COVID, there simply may have been fewer of those categorized as part-time on the road.
The sociodemographic characteristic, race/ethnicity, differed by COVID stage. Compared to Pre-COVID, Asian/Filipino/Pacific Islanders were far less likely to enroll during Early-COVID, but by Late-COVID, that finding was no longer significant. Public perceptions regarding COVID-19 and adherence to mitigation strategies may account for the significant reduction among enrollees identifying as Asian/Filipino/Pacific Islander. Research suggests COVID-19 fear was highly correlated with anti-Asian attitudes and xenophobia during Early-COVID, particularly as it was framed in language associating the virus to China as its country of origin (Dhanani & Franz, 2021). Evidence also suggests Asians were more likely to adhere to COVID-19 mitigation strategies and vaccinating (Anand et al., 2023).
During Late-COVID, there was greater representation of those identifying as Latino or Hispanic and having Spanish language preference. Latino ethnicity and Spanish preference were not so highly correlated as to be problematic. Specifically, 37.8% of those with Spanish language preference identified as Caucasian, and 29% of those with English language preference identified as Latino/Hispanic. At least two prior studies reported more Hispanics compared to other ethnic subgroups had initiated or increased alcohol consumption during COVID (McKnight-Eily, 2021; Metz et al., 2022). However, it is more likely that the increased representation of Hispanics observed was secondary to the permanent closure of a large Southern California DUI program.
At the program level, enrollees during COVID were more likely to be First Conviction participants compared to Pre-COVID, although the magnitude of change diminished in Late-COVID, possibly indicating a rebound effect. The magnitude of change in resident district region also grew stronger in Late-COVID, with a greater number of those enrolling during COVID residing out-of-county or in North County, reflecting the changing catchment area.
The changing catchment area also partially accounted for changes in participant characteristics observed in Late-COVID, specifically the increase in Hispanic, Spanish-speaking participants residing in the North County region. Notably, Latino/Hispanic drivers have been overrepresented among California DUI arrestees for the past decade; in 2020 they comprised 37.3% of the population, but 53.6% of DUI arrestees (Rees et al., 2023), highlighting a disparity that merits further consideration.
The increased enrollments during COVID among those identifying as Hispanic and Spanish speaking illuminated the program’s need to increase bilingual, bicultural counseling staff to meet increased demand. Given the behavioral health shortage, this highlights a target area for building workforce capacity and the need to implement evidence-based interventions that have been adapted and tested for their acceptability among Latinos (Osilla et al., 2012). Further research may explore contributing socioeconomic, cultural, and structural factors potentially at play.
For Latinos, COVID-19 exacerbated socioeconomic disadvantages and economic consequences were barriers to seeking health care and adhering to mitigation strategies (Cervantes et al., 2021). A lack of culturally and linguistically tailored interventions may impede treatment access that could otherwise promote positive coping to address pandemic-related stressors (Cervantes et al., 2021). Tailored interventions have been shown to reduce shame and improve motivation, engagement, and outcomes (Barker et al., 2016; Osilla et al., 2012). Culturally-specific group interventions have been found to be four-times more effective than culturally-diverse group interventions, and those delivered in participants’ preferred language were twice as effective as those conducted in English (Griner & Smith, 2006). Current research suggests that tailored public health campaigns, outreach and education targeting Latino immigrants with messaging about health, mental health, substance use, and DUI laws may promote physical and economic health, while also reducing DUI risk (Cervantes et al., 2021; Ramirez, 2022). Expanding efforts to incorporate public health messaging through enhanced social media campaigns, Spanish-language television, radio, and billboards could serve to address attitudes regarding drinking and driving and reduce cultural and structural barriers to substance and mental health treatment in the future (Ramirez, 2022). Meanwhile, DUI programs need to better address culturally-specific needs for this group. While this DUI program had evidence-based Spanish-language curriculum Pre-COVID, the Telehealth service delivery needs to address on-going content development and technical and access challenges.
In terms of clinical variables, enrollees during COVID were more likely to have BrAC levels
A notable departure from Pre-COVID was an 87% increase in low-level drug problems during Early-COVID and more pronounced during Late-COVID, relative to no problems. Follow-on analyses explored the involvement of specific drugs for reason of arrest, however no drug use was evident for the low-level group upon arrest. Over 94% of their arrests were alcohol-related and no other specific drug played a large role. During COVID-19, individuals may have initiated drug use, or increased already very low use, out of boredom or to cope (Abramson, 2021), but this use did not seem to factor in their DUI arrest. Regardless, the concomitant problem of alcohol misuse and other drug use (even low-level drug use) requires the clinical capacity to assess an individual’s risk level, use severity, and functioning (Gastfriend & Mee-Lee, 2004). Brief Interventions targeting this type of use (i.e., hazardous alcohol use and low-level drug use) have been shown to be an inexpensive, cost-effective early intervention strategy to increase an individual’s motivation and efficacy to abstain or moderate use (Jhanjee, 2014). DUI treatment programs may reduce harms by disseminating information about the potential risks of combining alcohol with other substances (Chacon et al., 2021). Should low-level drug use continue to play a role in the DUI population over time, clinicians may use Brief Interventions to provide realistic feedback and facilitate referrals for psychotherapeutic and pharmacological treatment, when indicated (Jhanjee, 2014; Roman et al., 2011).
Another interesting finding was the no/minimal depression endorsed during COVID compared to Pre-COVID, with the magnitude greater in Late-COVID. Historically, both First and Multiple conviction DUI offenders have been shown to have high rates of co-occurring disorders, including depression, PTSD, and self-harm (Barker et al., 2023; Hohman et al., 2017). The changes observed in participant characteristics and less severe alcohol misuse may account for the significant reduction in depression among those enrolling during COVID. COVID possibly ushered in a different DUI client type, the needs of whom we do not fully understand. A critical question is whether these characteristic changes will be maintained long-term.
Findings show a clear pattern in which Early-COVID enrollees tended to be lower risk with minimal depression, more non-hazardous alcohol use, lower BrAC levels, and more first conviction seen, compared to Pre-COVID controls; this pattern was maintained to some degree at Late- COVID. It may be that higher risk individuals convicted of a DUI during COVID were more likely to take advantage of Court extensions for several reasons. Stigma experiences among people in SUD treatment are well documented and could have resulted in DUI treatment avoidance given the opportunity (Luoma et al., 2013; van Boekel et al., 2013). Prior studies suggest an inverse association between severity of alcohol problems and motivation to engage in mandated alcohol services (Gregoire & Burke, 2004; Luoma et al., 2013).
Criminal justice impacts and DUI program closures may have contributed to the significant demographic changes observed for those enrolling. In California, about one third of participants attending First Conviction programs will go on to become repeat offenders. Reduced recidivism has been attributed to sanctions coupled with rapid entry into DUI treatment (Rees et al., 2023). This raises the concern that systemic delays in DUI treatment program entry may result in increased DUI recidivism rates in the near future.
Limitations
While this repeated cross-sectional study has several strengths, including complete samples from a large DUI program, a liberal inclusion criterion, and the avoidance of nonparticipation and self-selection biases due to the nature of routine data collection from all program participants, it is not without limitations. While it was important to understand how sociodemographic, program level, and clinical characteristic correlates changed by COVID-19, the cross-sectional design precludes any causal inferences. With the exception of BrAC, no biological data were collected for confirmatory purposes of self-reported data. Biases due to self-report and recall may be in play, and generalizability to other DUI programs cannot be assumed.
Conclusions
California, deemed a COVID “hotspot,” experienced dramatic declines in substance use disorder treatment and the pandemic presented serious disruptions to the California DUI system infrastructure unlike any other public health or economic crisis to date. To our knowledge, this study is the first study to evaluate the impact of COVID on the quantity and characteristics of DUI treatment enrollments before, during, and after the lockdown. The study context is a unique one, as DUI treatment bridges the intersection of public health and safety; study participants represent a criminal justice involved, mandated segment of the treatment population. Findings demonstrate extraordinary reductions in monthly enrollments, and striking changes in sociodemographic and clinical features among enrollees during COVID compared to the Pre-COVID control period. Enrollees during COVID presented as primarily first conviction offenders with lower clinical risk profiles compared to their Pre-COVID counterparts, the reasons for such appear to be multifactorial. Study results have important implications for public policy and service delivery adaptations, such that the DUI system may be better prepared to respond to any future large scale public health crises without negative impact on reach.
The multiagency DUI system under pandemic conditions had limited guidance upon which to draw, and there are scant evidence-based guidelines to date. This study provides a good starting place to provide some strategic future directions for DUI programs. Future research is needed to: (1) examine the long-term COVID impacts on DUI treatment; and (2) evaluate policy and procedural changes on DUI outcomes; (3) explore COVID impacts on job demands, experiences and evaluation of work for providers across agencies; and (4) identify key determinants for future sustainability. Developing an integrated, interagency response within the DUI system (e.g., development of a central and open database) may be a critical success factor for future DUI system disaster preparedness (Jackson et al., 2022; Piquero, 2021).
Supplemental Material
Supplemental Material - A Secondary Analysis of Sociodemographic, Program Level, and Clinical Characteristics of Driving Under the Influence Treatment Enrollees Prior to, During, and after the COVID-19 Lockdown
Supplemental Material for A Secondary Analysis of Sociodemographic, Program Level, and Clinical Characteristics of Driving Under the Influence Treatment Enrollees Prior to, During, and after the COVID-19 Lockdown by Melanie A. Barker, Susan I. Woodruff, María Luisa Zúñiga, Jamila K. Stockman, Kiyomi Tsuyuki, and Eileen Pitpitan in Journal of Drug Issues.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.